
Adolescent Health Literacy and Neighbourhood Features: HBSC Findings from Czech Republic, Poland, and Slovakia

 ,
,  ,
,  ,
,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Health Literacy
2.3. Neighbourhood
2.4. Statistical Methods
3. Results
3.1. Level of HLSAC
3.2. Neighbourhood
3.3. School Effect
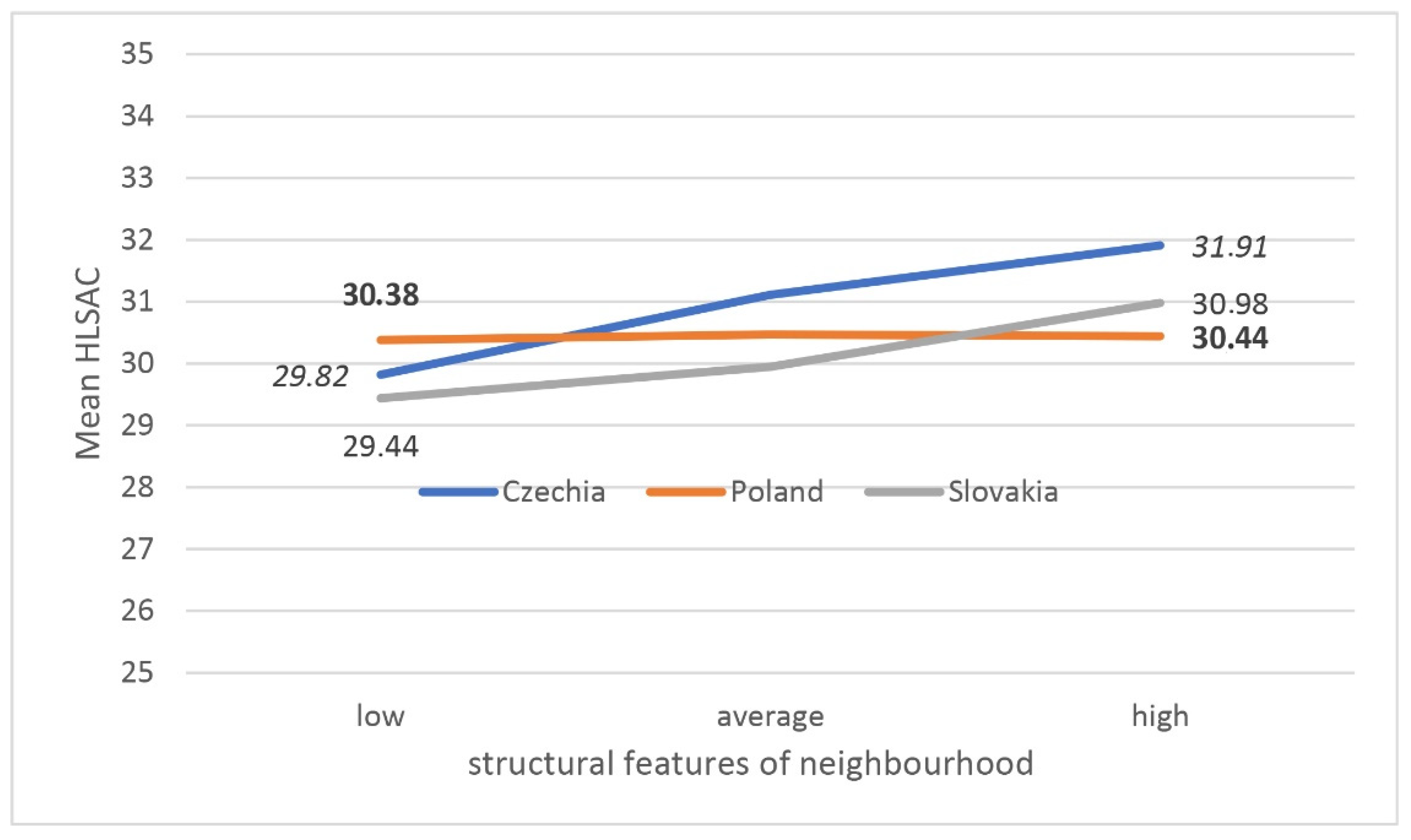
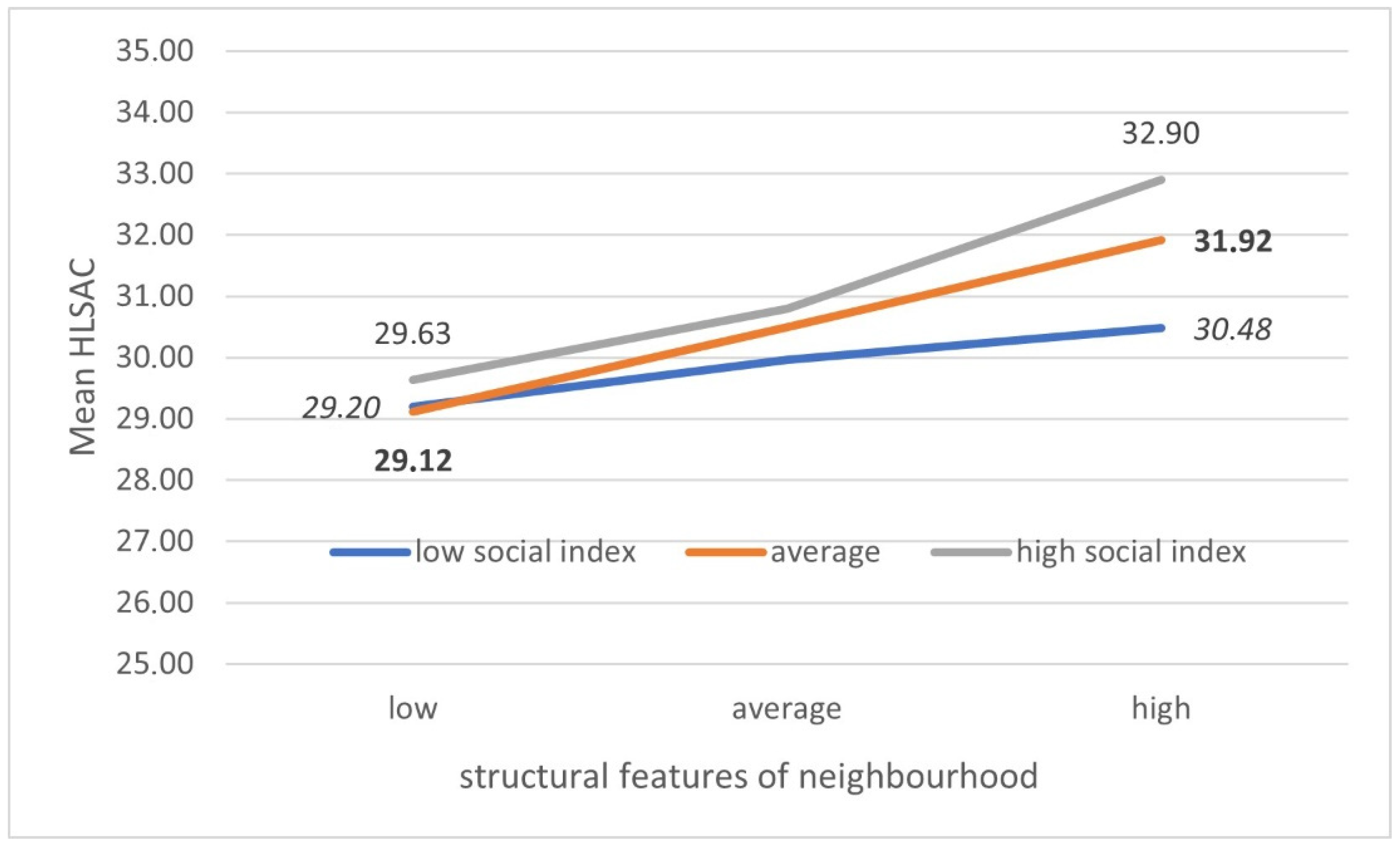
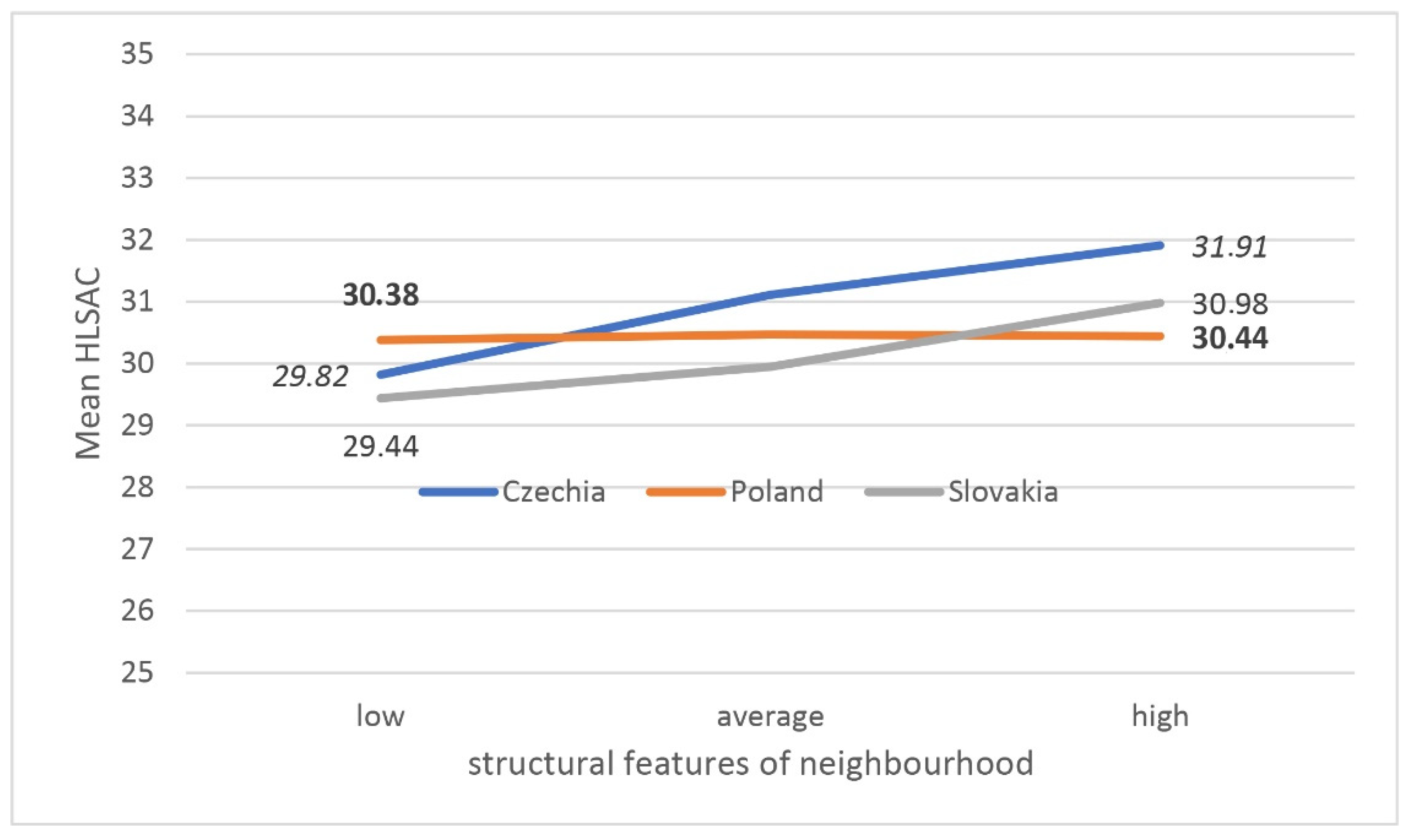
3.4. Multifactorial Analysis
4. Discussion
5. Strengths and Weaknesses of the Study
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- First International Conference on Health Promotion, Ottawa, 21 November 1986. Available online: https://www.who.int/teams/health-product-and-policy-standards/access-to-assistive-technology-medical-devices/health-promotion (accessed on 19 April 2021).
- Nutbeam, D. Health Promotion Glossary. Health Promot. Int. 1998, 13, 349–364. [Google Scholar] [CrossRef]
- Nutbeam, D. The Vital Role of Meaningful Community Engagement in Responding to the COVID-19 Pandemic. Public Health Res. Pract. 2021, 31. [Google Scholar] [CrossRef]
- Bronfenbrenner, U. The Ecology of Human Development: Experiments by Nature and Design; Harvard University Press: Cambridge, MA, USA, 2009. [Google Scholar]
- Inchley, J.; Currie, D.; Young, T.; Samdal, O.; Torsheim, T.; Augustson, L.; Barnekow, V. Growing Up Unequal: Gender and Socioeconomic Differences in Young People’s Health and Well-Being. Health Behaviour in School-Aged Children (HBSC) Study: International Report from the 2013/2014 Survey; WHO Regional Office for Europe: Copenhagen, Denmark, 2016. [Google Scholar]
- Boardman, J.D.; Onge, J.M.S. Neighborhoods and Adolescent Development. Child. Youth Environ. 2005, 15, 138. [Google Scholar] [PubMed]
- Kopcakova, J.; Dankulincova Veselska, Z.; Madarasova Geckova, A.; Bucksch, J.; Nalecz, H.; Sigmundova, D.; Van Dijk, J.P.; Reijneveld, S.A. Is a Perceived Activity-Friendly Environment Associated with More Physical Activity and Fewer Screen-Based Activities in Adolescents? Int. J. Environ. Res. Public. Health 2017, 14, 39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nieuwenhuis, J.; Hooimeijer, P. The Association between Neighbourhoods and Educational Achievement, a Systematic Review and Meta-Analysis. J. Hous. Built Environ. 2016, 31, 321–347. [Google Scholar] [CrossRef] [Green Version]
- Downey, D.B. How Schools Really Matter: Why Our Assumption about Schools and Inequality Is Mostly Wrong; University of Chicago Press: Chicago, IL, USA, 2020. [Google Scholar]
- Von Hippel, P.T.; Workman, J.; Downey, D.B. Inequality in Reading and Math Skills Forms Mainly before Kindergarten: A Replication, and Partial Correction, of Are Schools the Great Equalizer? Sociol. Educ. 2018, 91, 323–357. [Google Scholar] [CrossRef] [Green Version]
- Downey, D.B.; von Hippel, P.T.; Broh, B.A. Are Schools the Great Equalizer? Cognitive Inequality during the Summer Months and the School Year. Am. Sociol. Rev. 2004, 69, 613–635. [Google Scholar] [CrossRef]
- Caspi, A.; Taylor, A.; Moffitt, T.E.; Plomin, R. Neighborhood Deprivation Affects Children’s Mental Health: Environmental Risks Identified in a Genetic Design. Psychol. Sci. 2000, 11, 338–342. [Google Scholar] [CrossRef] [PubMed]
- Malinowska-Cieślik, M.; Mazur, J.; Nałęcz, H.; Małkowska-Szkutnik, A. Social and Behavioral Predictors of Adolescents’ Positive Attitude towards Life and Self. Int. J. Environ. Res. Public. Health 2019, 16, 4404. [Google Scholar] [CrossRef] [Green Version]
- Sastry, N.; Pebley, A. Family and Neighborhood Sources of Socioeconomic Inequality in Children’s Achievement. Demography 2010, 47, 777–800. [Google Scholar] [CrossRef]
- Hicks, A.L.; Handcock, M.S.; Sastry, N.; Pebley, A.R. Sequential Neighborhood Effects: The Effect of Long-Term Exposure to Concentrated Disadvantage on Children’s Reading and Math Test Scores. Demography 2017, 55, 1–31. [Google Scholar] [CrossRef] [Green Version]
- Birch, L.; Savage, J.S.; Ventura, A. Influences on the Development of Children’s Eating Behaviours: From Infancy to Adolescence. Can. J. Diet. Pract. Res. Publ. Dietit. Can. 2007, 68, s1–s56. [Google Scholar]
- Blackwell, D.L.; Hayward, M.D.; Crimmins, E.M. Does Childhood Health Affect Chronic Morbidity in Later Life? Soc. Sci. Med. 2001, 52, 1269–1284. [Google Scholar] [CrossRef]
- Allen, J.P.; Porter, M.R.; McFarland, F.C.; Marsh, P.; McElhaney, K.B. The Two Faces of Adolescents’ Success with Peers: Adolescent Popularity, Social Adaptation, and Deviant Behavior. Child Dev. 2005, 76, 747–760. [Google Scholar] [CrossRef] [Green Version]
- Oliva, A.; Antolín, L.; López, A.M. Development and Validation of a Scale for the Measurement of Adolescents’ Developmental Assets in the Neighborhood. Soc. Indic. Res. 2012, 106, 563–576. [Google Scholar] [CrossRef]
- Nieuwenhuis, J. Neighborhood Social Capital and Adolescents’ Individual Health Development. Soc. Sci. Med. 2020, 265, 113417. [Google Scholar] [CrossRef]
- Yamaguchi, A. Effects of Social Capital on General Health Status. Glob. J. Health Sci. 2014, 6, 45. [Google Scholar] [CrossRef] [Green Version]
- Nutbeam, D.; Muscat, D.M. Health Promotion Glossary 2021. Health Promot. Int. 2021. [Google Scholar] [CrossRef]
- Waverijn, G.; Heijmans, M.; Spreeuwenberg, P.; Groenewegen, P.P. Associations between Neighborhood Social Capital, Health Literacy, and Self-Rated Health Among People With Chronic Illness. J. Health Commun. 2016, 21, 36–44. [Google Scholar] [CrossRef]
- Berkman, N.D.; Davis, T.C.; McCormack, L. Health Literacy: What Is It? J. Health Commun. 2010, 15, 9–19. [Google Scholar] [CrossRef]
- Ratzan, S.C. Health literacy: Communication for the public good. Health Promot. Int. 2001, 16, 207–214. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHO. Draft WHO European Roadmap for Implementation of Health Literacy Initiatives through the Life Course; World Health Organization Regional Office for Europe: Copenhagen, Denmark, 2019; p. 5. [Google Scholar]
- Nutbeam, D. Defining, measuring and improving health literacy. Health Evaluation and Promotion 2015, 42, 450–456. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.; Begoray, D.; MacDonald, M. A Social Ecological Conceptual Framework for Understanding Adolescent Health Literacy in the Health Education Classroom. Am. J. Community Psychol. 2009, 44, 350. [Google Scholar] [CrossRef]
- Paakkari, L.; Kokko, S.; Villberg, J.; Paakkari, O.; Tynjälä, J. Health Literacy and Participation in Sports Club Activities among Adolescents. Scand. J. Public Health 2017, 45, 854–860. [Google Scholar] [CrossRef] [PubMed]
- Paakkari, L.; Simovska, V.; Pedersen, U.; Schulz, A. Materials for Teachers: Learning about Health and Health Promotion in Schools: Key Concepts and Activities; Schools for Health in Europe Network Foundation: Haderslev, Denmark, 2019; ISBN 978-87-971891-0-8. [Google Scholar]
- Sørensen, K.; Okan, O. Health Literacy. Health Literacy of Children and Adolescents in School Settings; Global Health Literacy Academy: Risskov, Denmark, 2020. [Google Scholar]
- Okan, O.; Bauer, U.; Levin-Zamir, D.; Pinheiro, P.; Sørensen, K. International Handbook of Health Literacy: Research, Practice and Policy across the Lifespan; Policy Press: Bristol, UK, 2019; ISBN 978-1-4473-4451-3. [Google Scholar]
- Paakkari, L.; Torppa, M.; Mazur, J.; Boberova, Z.; Sudeck, G.; Kalman, M.; Paakkari, O. A Comparative Study on Adolescents’ Health Literacy in Europe: Findings from the HBSC Study. Int. J. Environ. Res. Public. Health 2020, 17, 3543. [Google Scholar] [CrossRef]
- Martin, G.; Inchley, J.; Humphris, G.; Currie, C. Assessing the Psychometric and Ecometric Properties of Neighborhood Scales Using Adolescent Survey Data from Urban and Rural Scotland. Popul. Health Metr. 2017, 15, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Inchley, J.; Currie, D.; Budisavljevic, S.; Torsheim, T.; Jåstad, A.; Cosma, A. Spotlight on Adolescent Health and Well Being: Findings from the 2017/2018 Health Behaviour in School-Aged Children (HBSC) Survey in Europe and Canada. International Report: Key Findings; WHO Regional Office for Europe: Copenhagen, Denmark, 2020. [Google Scholar]
- Bröder, J.; Okan, O.; Bauer, U.; Bruland, D.; Schlupp, S.; Bollweg, T.M.; Saboga-Nunes, L.; Bond, E.; Sørensen, K.; Bitzer, E.-M.; et al. Health Literacy in Childhood and Youth: A Systematic Review of Definitions and Models. BMC Public Health 2017, 17, 361. [Google Scholar] [CrossRef]
- Zanbar, L.; Nouman, H. Predictors of Self-Efficacy among Residents of Low-Income Neighborhoods: Implications for Social Work Practice. J. Soc. Work 2020. [Google Scholar] [CrossRef]
- Guo, S.; Armstrong, R.; Waters, E.; Sathish, T.; Alif, S.M.; Browne, G.R.; Yu, X. Quality of Health Literacy Instruments Used in Children and Adolescents: A Systematic Review. BMJ Open 2018, 8, e020080. [Google Scholar] [CrossRef]
- Weis, M.; Heikamp, T.; Trommsdorff, G. Gender differences in school achievement: The role of self-regulation. Front. Psychol. 2013, 4, 442. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- OECD. Girls’ and Boys’ Performance in PISA; OECD Publishing: Paris, France, 2020. [Google Scholar] [CrossRef] [Green Version]
- Lee, H.Y.; Lee, J.; Kim, N.K. Gender Differences in Health Literacy Among Korean Adults: Do Women Have a Higher Level of Health Literacy Than Men? Am. J. Mens. Health. 2015, 9, 370–379. [Google Scholar] [CrossRef]
- Paakkari, O.; Torppa, M.; Villberg, J.; Kannas, L.; Paakkari, L. Subjective health literacy among school-aged children. Health Educ. 2018, 118, 182–195. [Google Scholar] [CrossRef] [Green Version]
- Paakkari, O.; Torppa, M.; Boberova, Z.; Välimaa, R.; Maier, G.; Mazur, J.; Paakkari, L. The cross-national measurement invariance of the health literacy for school-aged children (HLSAC) instrument. Eur. J. Public Health 2019, 29, 4322013436. [Google Scholar] [CrossRef]
- Caldwell, E.P.; Melton, K. Health Literacy of Adolescents. J. Pediatr. Nurs. Nurs. Care Child. Fam. 2020, 55, 116–119. [Google Scholar] [CrossRef]
- Driessnack, M.; Chung, S.; Perkhounkova, E.; Hein, M. Using the “Newest Vital Sign” to Assess Health Literacy in Children. J. Pediatr. Health Care 2014, 28, 165–171. [Google Scholar] [CrossRef]
- Loer, A.-K.M.; Domanska, O.M.; Stock, C.; Jordan, S. Subjective Generic Health Literacy and Its Associated Factors among Adolescents: Results of a Population-Based Online Survey in Germany. Int. J. Environ. Res. Public. Health 2020, 17, 8682. [Google Scholar] [CrossRef]
- Nelson, L.R.; Stupiansky, N.W.; Ott, M.A. The Influence of Age, Health Literacy, and Affluence on Adolescents’ Capacity to Consent to Research. J. Empir. Res. Hum. Res. Ethics 2016, 11, 115–121. [Google Scholar] [CrossRef] [Green Version]
- Schmidt, C.O.; Fahland, R.A.; Franze, M.; Splieth, C.; Thyrian, J.R.; Plachta-Danielzik, S.; Hoffmann, W.; Kohlmann, T. Health-Related Behaviour, Knowledge, Attitudes, Communication and Social Status in School Children in Eastern Germany. Health Educ. Res. 2010, 25, 542–551. [Google Scholar] [CrossRef]
- Coley, R.L.; Sims, J.; Thomson, D.; Votruba-Drzal, E. The Intergenerational Transmission of Socioeconomic Inequality through School and Neighborhood Processes. J. Child. Poverty 2019, 25, 79–100. [Google Scholar] [CrossRef]
- Mancuso, C.A.; Rincon, M. Impact of Health Literacy on Longitudinal Asthma Outcomes. J. Gen. Intern. Med. 2006, 21, 813–817. [Google Scholar] [CrossRef] [Green Version]
- Sukys, S.; Trinkuniene, L.; Tilindiene, I. Subjective Health Literacy among School-Aged Children: First Evidence from Lithuania. Int. J. Environ. Res. Public. Health 2019, 16, 3397. [Google Scholar] [CrossRef] [Green Version]
- Mmari, K.; Lantos, H.; Blum, R.W.; Brahmbhatt, H.; Sangowawa, A.; Yu, C.; Delany-Moretlwe, S. A Global Study on the Influence of Neighborhood Contextual Factors on Adolescent Health. J. Adolesc. Health 2014, 55, S13–S20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perrow, A.H.E.R.F. Promoting Health Literacy in Secondary Schools: A Review. Br. J. Sch. Nurs. 2015, 10, 82–87. [Google Scholar] [CrossRef]
- Arafat, S.; Majumder, M.; Kabir, R.; Papadopoulos, K.; Uddin, M. Health Literacy in School. In Optimizing Health Literacy or Improved Clinical Practices; Papalois, V.E., Theodosopoulou, M., Eds.; IGI Global: Hershey, PA, USA, 2018; pp. 175–197. [Google Scholar]
- Runarsdottir, E.M.; Vilhjalmsson, R. Ethnic Differences in Youth Well-Being: The Role of Sociodemographic Background and Social Support. Scand. J. Public Health 2015, 43, 580–587. [Google Scholar] [CrossRef] [PubMed]
- Bánfai-Csonka, H.; Bánfai, B.; Jeges, S.; Gyebnár, B.; Betlehem, J. Health Literacy among Participants from Neighbourhoods with Different Socio-Economic Statuses in the Southern Region of Hungary: A Pilot Study. BMC Public Health 2020, 20, 1060. [Google Scholar] [CrossRef]
- Smart, M.; Felton, J.; Meghea, C.; Buchalski, Z.; Maschino, L.; Sadler, R. Is a School’s Neighborhood Physical Disorder Related to Its Academic Outcomes? Child Youth Care Forum 2021, 50, 247–259. [Google Scholar] [CrossRef]
- Vamos, S.; Okan, O.; Sentell, T.; Rootman, I. Making a Case for Education for Health Literacy: An International Perspective. Int. J. Environ. Res. Public Health 2020, 17, 1436. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
{kind=link}
| Czech Republic | Poland | Slovakia | |
|---|---|---|---|
| Total | 6281 | 3341 | 1899 |
| Gender | |||
| Boys | 3106 | 1593 | 899 |
| Girls | 3175 | 1748 | 1000 |
| Age | |||
| 13 years | 3052 | 1620 | 1078 |
| 15 years | 3229 | 1721 | 821 |
| Czech Republic | Poland | Slovakia | p | |
|---|---|---|---|---|
| Social | ||||
| Safe place | ||||
| Sometimes or rarely/never | 7.3 | 10.1 | 8.2 | Chi-sq = 421.3 |
| Most of time | 35.6 | 50.3 | 26.1 | df = 4 |
| Always | 57.1 | 39.6 | 65.8 | p < 0.001 |
| Good place to live | ||||
| Not good | 4.7 | 5.1 | 4.2 | Chi-sq = 229.5 |
| Ok | 22.1 | 34.7 | 19.8 | df = 4 |
| Good or very good | 73.2 | 60.3 | 76.0 | p < 0.001 |
| Social capital index | ||||
| Low | 25.7 | 25.6 | 31.2 | Chi-sq = 49.7 |
| Average | 53.7 | 56.2 | 54.1 | df = 4 |
| High | 20.6 | 18.2 | 14.6 | p < 0.001 |
| Structural | ||||
| Area well off | ||||
| Not well off | 17.1 | 5.1 | 5.9 | Chi-sq = 2372.8 |
| Average | 62.8 | 73.2 | 21.6 | df = 4 |
| Very well off | 20.1 | 21.8 | 72.5 | p < 0.001 |
| Local area problems | ||||
| Poor (high deprivation) | 16.7 | 35.9 | 13.4 | Chi-sq = 665.8 |
| Average | 49.0 | 43.3 | 44.0 | df = 4 |
| Good (low deprivation) | 34.2 | 20.8 | 42.5 | p < 0.001 |
| Czech Republic | Poland | Slovakia | |
|---|---|---|---|
| Safe place | |||
| Sometimes or rarely/never | 27.7 ± 6.9 | 29.6 ± 4.8 | 28.1 ± 6.4 |
| Most of time | 29.6 ± 5.4 | 30.3 ± 4.3 | 30.0 ± 4.8 |
| Always | 30.8 ± 5.9 | 30.9 ± 4.7 | 31.9 ± 5.0 |
| K-W chi-sq | 156.9 | 30.5 | 98.3 |
| p | <0.001 | <0.001 | <0.001 |
| Good place to live | |||
| Not good | 28.3 ± 7.1 | 30.3 ± 4.8 | 28.3 ± 6.8 |
| Ok | 29.1 ± 5.7 | 29.8 ± 4.3 | 30.0 ± 5.6 |
| Good or very good | 30.6 ± 5.8 | 30.8 ± 4.6 | 31.6 ± 4.9 |
| K-W chi-sq | 101.4 | 44.8 | 36.8 |
| p | <0.001 | <0.001 | <0.001 |
| Social capital index | |||
| Low | 29.1 ± 6.0 | 29.6 ± 4.6 | 30.0 ± 5.5 |
| Average | 30.1 ± 5.4 | 30.4 ± 4.3 | 31.3 ± 4.6 |
| High | 31.6 ± 6.6 | 31.7 ± 4.7 | 32.7 ± 6.0 |
| K-W chi-sq | 168.6 | 81.5 | 64.0 |
| p | <0.001 | <0.001 | <0.001 |
| Czech Republic | Poland | Slovakia | |
|---|---|---|---|
| Area well off | |||
| Not well off | 29.0 ± 6.4 | 29.1 ± 5.3 | 28.7 ± 7.0 |
| Average | 30.2 ± 5.5 | 30.3 ± 4.3 | 29.9 ± 5.3 |
| Very well off | 31.1 ± 6.4 | 31.2 ± 4.9 | 31.7 ± 4.9 |
| K-W chi-sq | 84.5 | 37.8 | 47.5 |
| p | <0.001 | <0.001 | <0.001 |
| Local area problems | |||
| Poor (high deprivation) | 29.3 ± 6.8 | 30.4 ± 4.6 | 29.9 ± 6.2 |
| Average | 29.9 ± 5.5 | 30.4 ± 4.4 | 30.9 ± 5.0 |
| Good (low deprivation) | 30.9 ± 5.7 | 30.6 ± 4.7 | 31.7 ± 5.0 |
| K-W chi-sq | 64.9 | 0.7 | 20.0 |
| p | <0.001 | 0.688 | <0.001 |
| Combined Index | Czech Republic | Poland | Slovakia | |||
|---|---|---|---|---|---|---|
| Range of School Mean Value | ICC (%) | Range of School Mean Value | ICC (%) | Range of School Mean Value | ICC (%) | |
| HLSAC index (10–40) | 22.00–34.74 | 2.10 | 26.36–34.50 | 3.56 | 24.04–34.67 | 1.81 |
| FAS (0–13) | 4.00–10.03 | 6.94 | 4.57–11.71 | 16.35 | 3.00–10.18 | 9.34 |
| Social features of neighbourhood (z-score) | −1.20–0.66 | 5.73 | −0.89–0.92 | 2.19 | −0.86–0.61 | 3.41 |
| Structural features of neighbourhood (z-score) | −1.82–0.71 | 6.86 | −1.19–0.98 | 2.79 | −0.85–1.05 | 2.47 |
| Independent Variable | B | SE | Wald Chi-Sq | Df | p |
|---|---|---|---|---|---|
| Constant | 27.805 | 0.7241 | 1474.531 | 1 | 0.000 |
| −0.682 | 0.0995 | 46.998 | 1 | 0.000 |
| 0.141 | 0.0480 | 8.646 | 1 | 0.003 |
| 0.180 | 0.0211 | 73.190 | 1 | 0.000 |
| |||||
| Czech Republic | −0.994 | 0.1491 | 44.486 | 1 | 0.000 |
| Poland | −0.545 | 0.1650 | 10.904 | 1 | 0.001 |
| 0.988 | 0.0536 | 339.840 | 1 | 0.000 |
| 0.541 | 0.1208 | 20.018 | 1 | 0.000 |
| 0.308 | 0.0445 | 48.024 | 1 | 0.000 |
| |||||
| Czech Republic | −0.145 | 0.1398 | 1.076 | 1 | 0.300 |
| Poland | −0.598 | 0.1509 | 15.718 | 1 | 0.000 |
| (Scale) | 27.339 | 0.3640 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kleszczewska, D.; Porwit, K.; Boberova, Z.; Sigmund, E.; Vasickova, J.; Paakkari, L. Adolescent Health Literacy and Neighbourhood Features: HBSC Findings from Czech Republic, Poland, and Slovakia. Int. J. Environ. Res. Public Health 2021, 18, 7388. https://doi.org/10.3390/ijerph18147388
Kleszczewska D, Porwit K, Boberova Z, Sigmund E, Vasickova J, Paakkari L. Adolescent Health Literacy and Neighbourhood Features: HBSC Findings from Czech Republic, Poland, and Slovakia. International Journal of Environmental Research and Public Health. 2021; 18(14):7388. https://doi.org/10.3390/ijerph18147388
Chicago/Turabian StyleKleszczewska, Dorota, Katarzyna Porwit, Zuzana Boberova, Eric Sigmund, Jana Vasickova, and Leena Paakkari. 2021. "Adolescent Health Literacy and Neighbourhood Features: HBSC Findings from Czech Republic, Poland, and Slovakia" International Journal of Environmental Research and Public Health 18, no. 14: 7388. https://doi.org/10.3390/ijerph18147388
APA StyleKleszczewska, D., Porwit, K., Boberova, Z., Sigmund, E., Vasickova, J., & Paakkari, L. (2021). Adolescent Health Literacy and Neighbourhood Features: HBSC Findings from Czech Republic, Poland, and Slovakia. International Journal of Environmental Research and Public Health, 18(14), 7388. https://doi.org/10.3390/ijerph18147388