
A Systematic Review of the Current Measures of Theory of Mind in Adults with Schizophrenia


 ,
,
Abstract
1. Introduction
2. Materials and Methods
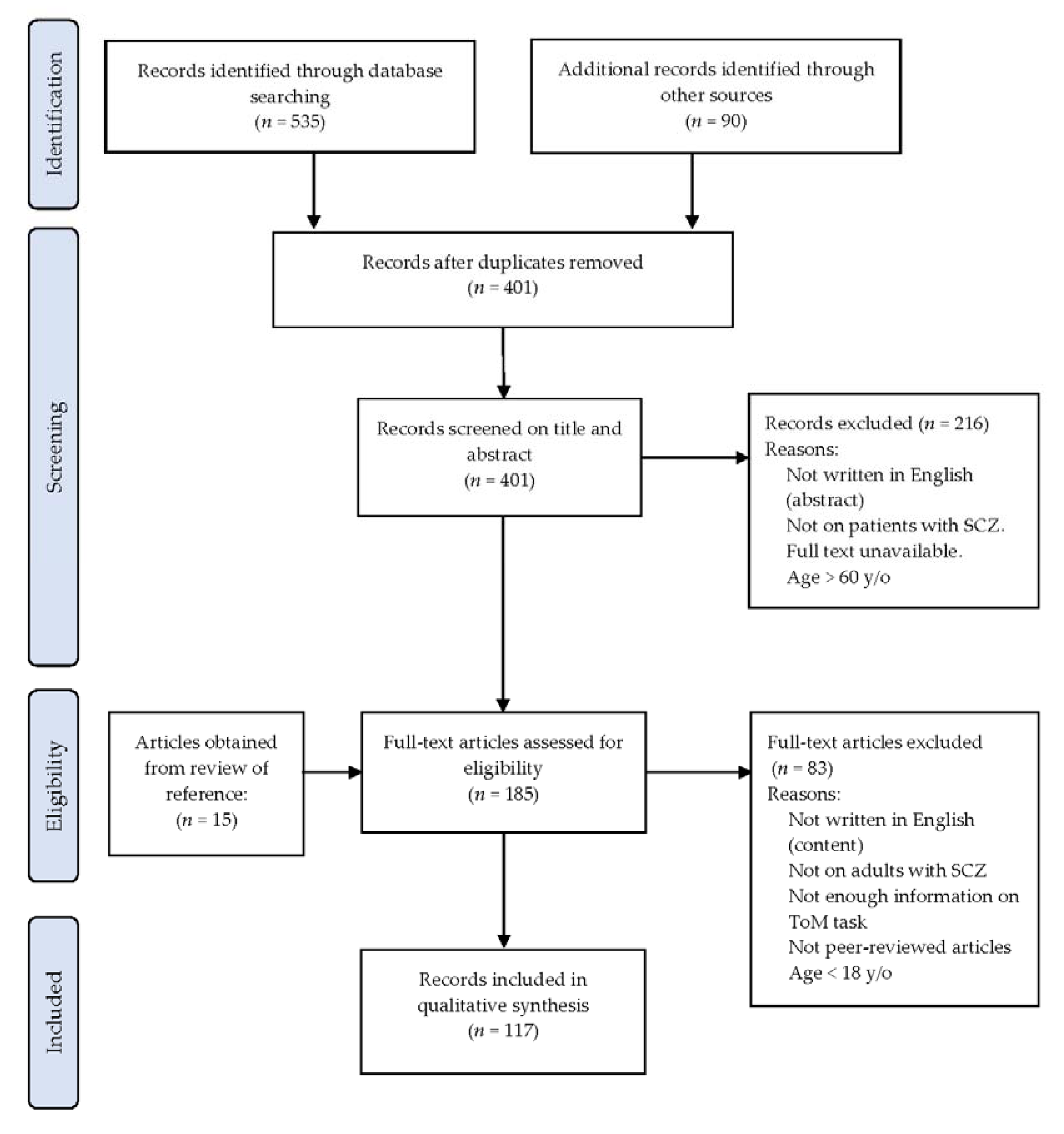
2.1. Database Search
2.2. Inclusion and Exclusion Criteria
2.3. Search Review
2.4. Data Extraction and Analysis
3. Results
3.1. Identified ToM Tasks and Quality Assessment
3.2. Concept and Construct
3.3. Administration
3.4. Psychometric Properties
4. Discussion
4.1. Concept and Construct
4.2. Administration
4.3. Psychometric Properties
4.4. Limitations and Suggestions for Further Investigations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Biedermann, F. Theory of mind and its relevance in schizophrenia. Curr. Opin. Psychiatry 2012, 25, 71–75. [Google Scholar] [CrossRef] [PubMed]
- Sodian, B.; Kristen, S. Theory of mind. In Handbook of Epistemic Cognition; Routledge: New York, NY, USA, 2016; pp. 80–97. [Google Scholar]
- Chung, Y.S.; Barch, D.; Strube, M. A meta-analysis of mentalizing impairments in adults with schizophrenia and autism spectrum disorder. Schizophr. Bull. 2014, 40, 602–616. [Google Scholar] [CrossRef]
- Bora, E.; Walterfang, M.; Velakoulis, D. Theory of mind in behavioural-variant frontotemporal dementia and alzheimer’s disease: A meta-analysis. J. Neurol. Neurosurg. Psychiatry 2015, 86, 714–719. [Google Scholar] [CrossRef] [PubMed]
- Bora, E.; Bartholomeusz, C.; Pantelis, C. Meta-analysis of theory of mind (ToM) impairment in bipolar disorder. Psychol. Med. 2016, 46, 253–264. [Google Scholar] [CrossRef] [PubMed]
- Bora, E.; Berk, M. Theory of mind in major depressive disorder: A meta-analysis. J. Affect. Disord. 2016, 191, 49–55. [Google Scholar] [CrossRef]
- Nemeth, N.; Matrai, P.; Hegyi, P.; Czeh, B.; Czopf, L.; Hussain, A.; Pammer, J.; Szabo, I.; Solymar, M.; Kiss, L.; et al. Theory of mind disturbances in borderline personality disorder: A meta-analysis. Psychiatry Res. 2018, 270, 143–153. [Google Scholar] [CrossRef]
- Brüne, M.; Özgürdal, S.; Ansorge, N.; von Reventlow, H.G.; Peters, S.; Nicolas, V.; Tegenthoff, M.; Juckel, G.; Lissek, S. An fMRI study of “theory of mind” in at-risk states of psychosis: Comparison with manifest schizophrenia and healthy controls. NeuroImage 2011, 55, 329–337. [Google Scholar] [CrossRef]
- Achim, A.M.; Ouellet, R.; Roy, M.A.; Jackson, P.L. Mentalizing in first-episode psychosis. Psychiatry Res. 2012, 196, 207–213. [Google Scholar] [CrossRef] [PubMed]
- Thompson, A.; Papas, A.; Bartholomeusz, C.; Allott, K.; Amminger, G.P.; Nelson, B.; Wood, S.; Yung, A. Social cognition in clinical “at risk” for psychosis and first episode psychosis populations. Schizophr. Res. 2012, 141, 204–209. [Google Scholar] [CrossRef]
- Bora, E.; Gökçen, S.; Kayahan, B.; Veznedaroglu, B. Deficits of social-cognitive and social-perceptual aspects of theory of mind in remitted patients with schizophrenia. J. Nerv. Ment. Dis. 2008, 196, 95–99. [Google Scholar] [CrossRef]
- Wang, Y.Y.; Wang, Y.; Zou, Y.M.; Ni, K.; Tian, X.; Sun, H.W.; Lui, S.S.Y.; Cheung, E.F.C.; Suckling, J.; Chan, R.C.K. Theory of mind impairment and its clinical correlates in patients with schizophrenia, major depressive disorder and bipolar disorder. Schizophr. Res. 2018, 197, 349–356. [Google Scholar] [CrossRef] [PubMed]
- Akil, M.; Kolachana, B.S.; Rothmond, D.A.; Hyde, T.M.; Weinberger, D.R.; Kleinman, J.E. Catechol-o-methyltransferase genotype and dopamine regulation in the human brain. J. Nerv. Ment. Dis. 2003, 23, 2008–2013. [Google Scholar] [CrossRef]
- Mohnke, S.; Erk, S.; Schnell, K.; Schutz, C.; Romanczuk-Seiferth, N.; Grimm, O.; Haddad, L.; Pohland, L.; Garbusow, M.; Schmitgen, M.M.; et al. Further evidence for the impact of a genome-wide-supported psychosis risk variant in znf804a on the theory of mind network. Neuropsychopharmacology 2014, 39, 1196–1205. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Brüne, M.; Abdel Hamid, M.; Lehmkämper, C.; Sonntag, C. Mental state attribution, neurocognitive functioning, and psychopathology: What predicts poor social competence in schizophrenia best? Schizophr. Res. 2007, 92, 151–159. [Google Scholar] [CrossRef] [PubMed]
- Mehl, S.; Rief, W.; Lullmann, E.; Ziegler, M.; Kesting, M.L.; Lincoln, T.M. Are theory of mind deficits in understanding intentions of others associated with persecutory delusions? J. Nerv. Ment. Dis. 2010, 198, 516–519. [Google Scholar] [CrossRef] [PubMed]
- Fett, A.-K.J.; Viechtbauer, W.; Penn, D.L.; van Os, J.; Krabbendam, L. The relationship between neurocognition and social cognition with functional outcomes in schizophrenia: A meta-analysis. Neurosci. Biobehav. Rev. 2011, 35, 573–588. [Google Scholar] [CrossRef]
- Pinkham, A.E.; Penn, D.L.; Green, M.F.; Harvey, P.D. Social cognition psychometric evaluation: Results of the initial psychometric study. Schizophr. Bull. 2016, 42, 494–504. [Google Scholar] [CrossRef]
- Vass, E.; Fekete, Z.; Simon, V.; Simon, L. Interventions for the treatment of theory of mind deficits in schizophrenia: Systematic literature review. Psychiatry Res. 2018, 267, 37–47. [Google Scholar] [CrossRef]
- Vass, E.; Simon, V.; Fekete, Z.; Lencse, L.; Ecseri, M.; Kis, B.; Simon, L. A novel virtual reality-based theory of mind intervention for outpatients with schizophrenia: A proof-of-concept pilot study. Clin. Psychol. Psychother. 2020, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Steinmair, D.; Horn, R.; Richter, F.; Wong, G.; Löffler Stastka, H. Mind reading improvements in mentalization-based therapy training. Bull. Menn. Clin. 2021, 85, 59–82. [Google Scholar] [CrossRef]
- Bechi, M.; Riccaboni, R.; Ali, S.; Fresi, F.; Buonocore, M.; Bosia, M.; Cocchi, F.; Smeraldi, E.; Cavallaro, R. Theory of mind and emotion processing training for patients with schizophrenia: Preliminary findings. Psychiatry Res. 2012, 198, 371–377. [Google Scholar] [CrossRef]
- Bechi, M.; Spangaro, M.; Bosia, M.; Zanoletti, A.; Fresi, F.; Buonocore, M.; Cocchi, F.; Guglielmino, C.; Smeraldi, E.; Cavallaro, R. Theory of mind intervention for outpatients with schizophrenia. Neuropsychol. Rehabil. 2013, 23, 383–400. [Google Scholar] [CrossRef]
- Vaskinn, A.; Andersson, S.; Østefjells, T.; Andreassen, O.A.; Sundet, K. Emotion perception, non-social cognition and symptoms as predictors of theory of mind in schizophrenia. Compr. Psychiatry 2018, 85, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Abu-Akel, A.; Shamay-Tsoory, S. Neuroanatomical and neurochemical bases of theory of mind. Neuropsychologia 2011, 49, 2971–2984. [Google Scholar] [CrossRef]
- Shamay-Tsoory, S.G.; Shur, S.; Barcal-Goodman, L.; Medlovich, S.; Harari, H.; Levkovitz, Y. Dissociation of cognitive from affective components of theory of mind in schizophrenia. Psychiatry Res. 2007, 149, 11–23. [Google Scholar] [CrossRef]
- Stone, V.E.; Baron-Cohen, S.; Calder, A.; Keane, J.; Young, A. Acquired theory of mind impairments in individuals with bilateral amygdala lesions. Neuropsychologia 2003, 41, 209–220. [Google Scholar] [CrossRef]
- Bora, E.; Yucel, M.; Pantelis, C. Theory of mind impairment in schizophrenia: Meta-analysis. Schizophr. Res. 2009, 109, 1–9. [Google Scholar] [CrossRef]
- Hutchins, T.L.; Prelock, P.A.; Bonazinga, L. Psychometric evaluation of the theory of mind inventory (ToMI): A study of typically developing children and children with autism spectrum disorder. J. Autism Dev. Disord. 2012, 42, 327–341. [Google Scholar] [CrossRef]
- Stone, V.E.; Baron-Cohen, S.; Knight, R.T. Frontal lobe contributions to theory of mind. J. Cogn. Neurosci. 1998, 10, 640–656. [Google Scholar] [CrossRef] [PubMed]
- Langdon, R. Defective self and/or other mentalising in schizophrenia: A cognitive neuropsychological approach. Cogn. Neuropsychiatry 1997, 2, 167–193. [Google Scholar] [CrossRef] [PubMed]
- Baron-Cohen, S.; Wheelwright, S. The ‘reading the mind in the eyes’ test revised version: A study with normal adults, and adults with asperger syndrome or high-functioning autism. J. Child. Psychol. Psychiatry 2001, 42, 241. [Google Scholar] [CrossRef] [PubMed]
- Corcoran, R.; Mercer, G.; Frith, C.D. Schizophrenia, symptomatology and social inference: Investigating ‘theory of mind’ in people with schizophrenia. Schizophr. Res. 1995, 17, 5–13. [Google Scholar] [CrossRef]
- Mitchley, N.J.; Barber, J.; Gray, J.M.; Brooks, D.N.; Livingston, M.G. Comprehension of irony in schizophrenia. Cogn. Neuropsychiatry 1998, 3, 127–138. [Google Scholar] [CrossRef]
- Happé, F.; Brownell, H.; Winner, E. Acquired ‘theory of mind’ impairments following stroke. Cognition 1999, 70, 211–240. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, P. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed]
- Prinsen, C.A.; Vohra, S.; Rose, M.R.; Boers, M.; Tugwell, P.; Clarke, M.; Williamson, P.R.; Terwee, C.B. How to select outcome measurement instruments for outcomes included in a “Core Outcome Set”—A practical guideline. Trials 2016, 17, 449. [Google Scholar] [CrossRef] [PubMed]
- Brown, T.; Subel, C. Known-group validity of the infant toddler sensory profile and the sensory processing measure-preschool. J. Occup. Ther. Sch. Early Interv. 2013, 6, 54–72. [Google Scholar] [CrossRef]
- Husted, J.A.; Cook, R.J.; Farewell, V.T.; Gladman, D.D. Methods for assessing responsiveness: A critical review and recommendations. J. Clin. Epidemiol. 2000, 53, 459–468. [Google Scholar] [CrossRef]
- Mokkink, L.B.; De Vet, H.C.; Prinsen, C.A.; Patrick, D.L.; Alonso, J.; Bouter, L.M.; Terwee, C.B. COSMIN risk of bias checklist for systematic reviews of patient-reported outcome measures. Qual. Life Res. 2018, 27, 1171–1179. [Google Scholar] [CrossRef]
- Hussey, I.; Hughes, S. Hidden invalidity among fifteen commonly used measures in social and personality psychology. Adv. Methods Pract. Psychol. Sci. 2020, 166–184. [Google Scholar] [CrossRef]
- Canty, A.L.; Neumann, D.L.; Fleming, J.; Shum, D.H.K. Evaluation of a newly developed measure of theory of mind: The virtual assessment of mentalising ability. Neuropsychol. Rehabil. 2017, 27, 834–870. [Google Scholar] [CrossRef]
- Olderbak, S.; Wilhelm, O.; Olaru, G.; Geiger, M.; Brenneman, M.W.; Roberts, R.D. A psychometric analysis of the reading the mind in the eyes test: Toward a brief form for research and applied settings. Front. Psychol. 2015, 6, 1503. [Google Scholar] [CrossRef]
- Schiffer, B.; Pawliczek, C.; Muller, B.W.; Wiltfang, J.; Brune, M.; Forsting, M.; Gizewski, E.R.; Leygraf, N.; Hodgins, S. Neural mechanisms underlying affective theory of mind in violent antisocial personality disorder and/or schizophrenia. Schizophr. Bull. 2017, 43, 1229–1239. [Google Scholar] [CrossRef]
- Pinkham, A.E.; Harvey, P.D.; Penn, D.L. Social cognition psychometric evaluation: Results of the final validation study. Schizophr. Bull. 2017, 44, 737–748. [Google Scholar] [CrossRef] [PubMed]
- Baron-Cohen, S.; Leslie, A.M.; Frith, U. Does the autistic child have a “theory of mind”? Cogn. 1985, 21, 37–46. [Google Scholar] [CrossRef]
- Happé, F.G. An advanced test of theory of mind: Understanding of story characters’ thoughts and feelings by able autistic, mentally handicapped, and normal children and adults. J. Autism Dev. Disord. 1994, 24, 129–154. [Google Scholar] [CrossRef] [PubMed]
- Frith, C.D.; Corcoran, R. Exploring ‘theory of mind’ in people with schizophrenia. Psychol. Med. 1996, 26, 521–530. [Google Scholar] [CrossRef]
- Baron-Cohen, S. The autistic child’s theory of mind: A case of specific developmental delay. J. Child Psychol. Psychiatry 1989, 30, 285–297. [Google Scholar] [CrossRef]
- Brüne, M. Emotion recognition, ‘theory of mind,’ and social behavior in schizophrenia. Psychiatry Res. 2005, 133, 135–147. [Google Scholar] [CrossRef]
- Sarfati, Y.; Hardy-Bayle, M.-C.; Nadel, J.; Chevalier, J.-F.; Widlocher, D. Attribution of mental states to others by schizophrenic patients. Cogn. Neuropsychiatry 1997, 2, 1–18. [Google Scholar] [CrossRef]
- Brunet, E.; Sarfati, Y.; Hardy-Baylé, M.C.; Decety, J. Abnormalities of brain function during a nonverbal theory of mind task in schizophrenia. Neuropsychologia 2003, 41, 1574–1582. [Google Scholar] [CrossRef]
- Corcoran, R.; Cahill, C.; Frith, C.D. The appreciation of visual jokes in people with schizophrenia: A study of mentalising ability. Schizophr. Res. 1997, 24, 319–327. [Google Scholar] [CrossRef]
- Langdon, R.; Davies, M.; Coltheart, M. Understanding minds and understanding communicated meanings in schizophrenia. Mind. Lang. 2002, 17, 68–104. [Google Scholar] [CrossRef]
- Martino, D.; Bucay, D.; Butman, J.; Allegri, R. Neuropsychological frontal impairments and negative symptoms in schizophrenia. Psychiatry Res. 2007, 152, 121–128. [Google Scholar] [CrossRef] [PubMed]
- Chen, K.W.; Lee, S.C.; Chiang, H.Y.; Syu, Y.C.; Yu, X.X.; Hsieh, C.L. Psychometric properties of three measures assessing advanced theory of mind: Evidence from people with schizophrenia. Psychiatry Res. 2017, 257, 490–496. [Google Scholar] [CrossRef] [PubMed]
- Okruszek, Ł.; Piejka, A.; Szczepocka, E.; Wysokiński, A.; Pluta, A. Affective and cognitive verbal theory of mind in schizophrenia: Results from a novel paradigm. J. Int. Neuropsychol. Soc. 2017, 24, 305–309. [Google Scholar] [CrossRef]
- Dziobek, I.; Fleck, S.; Kalbe, E.; Rogers, K.; Hassenstab, J.; Brand, M.; Kessler, J.; Woike, J.; Wolf, O.; Convit, A. Introducing MASC: A movie for the assessment of social cognition. J. Autism Dev. Disord. 2006, 36, 623–636. [Google Scholar] [CrossRef]
- Canty, A.L.; Neumann, D.L.; Shum, D.H.K. Using virtual reality to assess theory of mind subprocesses and error types in early and chronic schizophrenia. Schizophr. Res. 2017, 10, 15–19. [Google Scholar] [CrossRef]
- Castelli, F.; Happé, F.; Frith, U.; Frith, C. Movement and mind: A functional imaging study of perception and interpretation of complex intentional movement patterns. NeuroImage 2000, 12, 314–325. [Google Scholar] [CrossRef]
- Bell, M.; Fiszdon, J.; Greig, T.; Wexler, B. Social attribution test—multiple choice (SAT-MC) in schizophrenia: Comparison with community sample and relationship to neurocognitive, social cognitive and symptom measures. Schizophr. Res. 2010, 122, 164–171. [Google Scholar] [CrossRef]
- Koelkebeck, K.; Pedersen, A.; Suslow, T.; Kueppers, K.; Arolt, V.; Ohrmann, P. Theory of mind in first-episode schizophrenia patients: Correlations with cognition and personality traits. Schizophr. Res. 2010, 119, 115–123. [Google Scholar] [CrossRef]
- Abu-Akel, A.; Abushua’leh, K. ‘Theory of mind’ in violent and nonviolent patients with paranoid schizophrenia. Schizophr. Res. 2004, 69, 45–53. [Google Scholar] [CrossRef]
- Brothers, L. The social brain: A project for integrating primate behaviour and neurophysiology in a new domain. Concepts Neurosci. 1990, 1, 27–51. [Google Scholar]
- Couture, S.M.; Penn, D.L.; Roberts, D.L. The functional significance of social cognition in schizophrenia: A review. Schizophr. Bull. 2006, 32 (Suppl. 1), S44–S63. [Google Scholar] [CrossRef] [PubMed]
- Montag, C.; Dziobek, I.; Richter, I.; Neuhaus, K.; Lehmann, A.; Sylla, R.; Heekeren, H.; Heinz, A.; Gallinat, J. Different aspects of theory of mind in paranoid schizophrenia: Evidence from a video-based assessment. Psychiatry Res. 2011, 186, 203–209. [Google Scholar] [CrossRef] [PubMed]
- Park, S. A study on the theory of mind deficits and delusions in schizophrenic patients. Issues Ment. Health Nurs. 2018, 39, 269–274. [Google Scholar] [CrossRef] [PubMed]
- Guo, J.Y.; Ragland, J.D.; Carter, C.S. Memory and cognition in schizophrenia. Mol. Psychiatry 2019, 24, 633–642. [Google Scholar] [CrossRef]
- Holland, J.L.; Christian, L.M. The influence of topic interest and interactive probing on responses to open-ended questions in web surveys. Soc. Sci. Comput. Rev. 2009, 27, 196–212. [Google Scholar] [CrossRef]
- Hur, J.W.; Byun, M.S.; Shin, N.Y.; Shin, Y.S.; Kim, S.N.; Jang, J.H.; Kwon, J.S. General intellectual functioning as a buffer against theory-of-mind deficits in individuals at ultra-high risk for psychosis. Schizophr. Res. 2013, 149, 83–87. [Google Scholar] [CrossRef]
- Li, D.D.; Li, X.S.; Yu, F.Q.; Chen, X.G.; Zhang, L.; Li, D.; Wei, Q.; Zhang, Q.; Zhu, C.Y.; Wang, K. Comparing the ability of cognitive and affective theory of mind in adolescent onset schizophrenia. Neuropsychiatr. Dis. Treat. 2017, 13, 937–945. [Google Scholar] [CrossRef]
- Bibby, H. Theory of mind after traumatic brain injury. Neuropsychologia 2005, 43, 99–114. [Google Scholar] [CrossRef] [PubMed]
- Dal Monte, O.; Schintu, S.; Pardini, M.; Berti, A.; Wassermann, E.M.; Grafman, J.; Krueger, F. The left inferior frontal gyrus is crucial for reading the mind in the eyes: Brain lesion evidence. Cortex 2014, 58, 9–17. [Google Scholar] [CrossRef] [PubMed]
- Hajdúk, M.; Heretik, A., Jr. Theory of mind in people with schizophrenia. Ceska Slov. Psychiatry 2013, 109, 171–177. [Google Scholar]
- Harrison, F. Getting started with meta-analysis. Methods Ecol. Evol. 2011, 2, 1–10. [Google Scholar] [CrossRef]
- Valentine, J.C.; Pigott, T.D.; Rothstein, H.R. How many studies do you need? A primer on statistical power for meta-analysis. J. Educ. Behav. Stat. 2010, 35, 215–247. [Google Scholar] [CrossRef]
- Portney, L.; Watkins, M. Foundations of Clinical Research: Applications to Practice, 3rd ed.; FA Davis Company: Philadelphia, PA, USA, 2015. [Google Scholar]
- Fertuck, E.A.; Mergenthaler, E.; Target, M.; Levy, K.N.; Clarkin, J.F. Development and criterion validity of a computerized text analysis measure of reflective functioning. Psychother. Res. 2012, 22, 298–305. [Google Scholar] [CrossRef]
- Richter, F.; Steinmair, D.; Löffler-Stastka, H. Construct validity of the mentalization scale (MentS) within a mixed psychiatric sample. Front. Psychol. 2021, 12. [Google Scholar] [CrossRef] [PubMed]
- Fonagy, P.; Luyten, P.; Moulton-Perkins, A.; Lee, Y.-W.; Warren, F.; Howard, S.; Ghinai, R.; Fearon, P.; Lowyck, B. Development and validation of a self-report measure of mentalizing: The reflective functioning questionnaire. PLoS ONE. 2016, 11, e0158678. [Google Scholar] [CrossRef]
- Dimaggio, G.; Popolo, R.; Salvatore, G.; Lysaker, P. Mentalizing in schizophrenia is more than just solving theory of mind tasks. Front. Psychol. 2013, 4, 83. [Google Scholar] [CrossRef]
- McCabe, R.; Leudar, I.; Antaki, C. Do people with schizophrenia display theory of mind deficits in clinical interactions? Psychol. Med. 2004, 34, 401–412. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Psychometric Property | Measure | Criteria for Good Measurement Properties (Reference) |
|---|---|---|
| Reliability | ||
| Internal consistency | Cronbach’s alpha (α) Omega (ω) | * α ≥ 0.70 ω ≥ 0.70 [41] |
| Test–retest reliability | Intraclass correlation coefficient (ICC) or weighted Kappa | * ICC or weighted Kappa ≥ 0.70 |
| Construct validity | ||
| Unidimensionality | Classical test theory Item response theory (IRT)/Rasch analysis | * CFA: CFI or TLI or comparable measure > 0.95 OR RMSEA <0.06 OR SRMR < 0.08 * No violation of unidimensionality3: CFI or TLI or comparable measure > 0.95 OR RMSEA < 0.06 OR SRMR < 0.08 AND no violation of local independence: residual correlations among the items after controlling for the dominant factor < 0.20 OR Q3′s < 0.37 AND no violation of monotonicity: adequate looking graphs OR item scalability > 0.30 AND adequate model fit: IRT: χ2 > 0.01; Rasch: infit and outfit mean squares ≥ 0.5 and ≤1.5 OR Z standardized values ≥ 2 and <2 |
| Known-group validity | Independent t-test or Analysis of variance (p) | Significant difference: p < 0.05 [38] |
| Convergent validity | Pearson’s correlation coefficient (r) or Spearman’s correlation coefficient (ρ) | r or ρ ≥ 0.70 |
| Criterion validity | ||
| Concurrent, predictive | Pearson’s correlation coefficient (r) or Spearman’s correlation coefficient (ρ) | r or ρ ≥ 0.70 |
| Ecological validities | Pearson’s correlation coefficient (r) or Spearman’s correlation coefficient (ρ) | r or ρ ≥ 0.70 |
| Responsiveness | ||
| Internal responsiveness | Effect size (ES) and Standardized response mean (SRM) | Low: ES and SRM = 0.2 Medium: ES and SRM = 0.5 High: ES and SRM = 0.8 [39] |
| External responsiveness | Area under the ROC curve (AUC) | * AUC ≥ 0.7 |
| Name of Each Type of ToM Task (Reference) | ToM Concept | Construct | n of Included Studies | Task Content | Presentation Modality | Answer Mode | Inclusion of Control Questions/ Items | Scoring | |
|---|---|---|---|---|---|---|---|---|---|
| Hinting task V1 [33] | Infer real intentions behind indirect words | Cog and Aff | 12 | Ten short stories about a social interaction between two characters. Each story ends with one character dropping a hint. | Verbal stories | Open-ended questions | No | 0, 1, 2. | |
| V2 [16] | Movie sequence as presentation modality. | Multisensory movie (verbal, visual, auditory) | 0, 1, 2. | ||||||
| First order False Belief stories V1 [46,47] | FB1 | Understand one has a false belief about reality | Cog and Aff | 17 | Sally and Anne story; Cigarettes story. | Verbal stories and visual adds | Open-ended questions | Q: M and C | ToM: 0, 1. Explanation: 0, 1, 2, 3. |
| V2 [48] | FB1 with deception | Understand psychological states guide behaviors and to deceive | First order FB and deception stories with series of cartoon drawings. | 0, 1, 2. Scored only when control question is correctly answered | |||||
| Second order False Belief stories V1 [47,49] | FB2 | Understand one has a false belief about the belief of another | Cog | 15 | Ice-Cream Van story; Burglar story. | Verbal stories and visual adds | Open-ended questions | Q: M and C | 0, 1, 2. |
| V2 [48] | FB2 with deception | Understand one ignores misinformation because another is trying to deceive | Cog and Aff | Second order FB and deception stories with series of cartoon drawings. | 0, 1, 2. Scored only when control question is correctly answered. | ||||
| False Belief picture sequencing V1 [31] | Correctly complete a set of pictures based on false belief inferences | Cog | 14 | Arrange four four-card picture sequences of false beliefs in a correct order. Four types of stories: social-script, mechanical, false-belief and capture. | Visual picture sequences | Both versions: Sequence story pictures. V2 includes an additional open-ended questions | I: Inferential reasoning ability | 0–6. | |
| V2 [50] | Six picture stories of false beliefs and 23 questions with first and second order ToM and non-mental questions. | Picture sequencing: 0–6; ToM questionnaire: 0, 1. | |||||||
| Character Intention task [51,52] | Understand the intention of a person in subtle social cues | Cog and Aff | 5 | Thirty or 42 sets of comic strips. Each strip: Three pictures in sequence and answer cards (Attribution of intention and Attribution of false belief). | Visual pictures | Multiple choice questions | I: Basic reasoning ability | 0, 1. | |
| Visual Jokes [53] | Detect visual jokes involving attribution of ignorance, false belief or deception | Cog | 5 | Two sets of 10 cartoon jokes. Set 1: Mental state attribution to false belief and deception. Set 2: Physical/behavior scene. | Visual jokes | Open-ended questions | I: Other general cognitive deficits | 0, 1. | |
| Irony task [34,54] | Understand the opposition between literal and true meanings of words | Cog and Aff | 5 | Nine or more stories with ironical utterance. | Verbal stories and written copy | Multiple choice questions | Q: C | 0, 1. | |
| Faux Pas [30,55] | Infer different perspectives: speaker’s thinking and listener’s feeling | Cog and Aff | 11 | FP stories with questions of recognition and understanding of FP. | Verbal stories with a print copy | Open-ended questions | I: Basic reasoning ability, attention, Q: M or C. | 0, 1. | |
| Yoni’s Verbal and Eye Gaze Cues [26] | Judge mental states based on verbal and eye gaze cues. | Cog and Aff | 6 | Each of 87 trials: a cartoon outline of a face and four colored pictures around each corner. Questions: first-order or second-order ToM, cognitive or affective ToM. | Visual and Verbal (written questions) | Multiple choice questions | Q: Attention and C | 0, 1. | |
| Story test V1 [35] | Multiple concepts: various, 4–5 | Cog and Aff | 6 | All three versions use stories. Eight ToM: Double bluff, mistakes, persuasion, white lies. | Verbal and visual adds | Open-ended questions | I: Cause-effect inference | 0, 1. | |
| V2 [56] | Five ToM: Figure of speech, lies, white lies, joke. | Q: M and C | 0, 1. | ||||||
| V3 [57] | Eighteen ToM stories. False beliefs, false attributions, lies, sarcasm, faux pas. | Q: M and C | 0, 1, 2. | ||||||
| Movie for Social Cognition V1 [58] | Multiple concepts: 5 | Cog and Aff ToM; Emotion perception | 3 | Movie for the Assessment of Social Cognition (MASC): 15 min movie about characters getting together for a dinner party: paused 46 times for 48 questions. ToM: first- and second-order false belief, faux pas, metaphor, or sarcasm. | Scenario: multi-modalities. Question: verbal and written | Multiple-choice questions | Q: M and C, I: Reasoning ability | 0, 1. Outputs: Error categories, mental state modalities and non-social inferencing. M and C: 1, 0.5, 0. | |
| V2 [59] | Multiple concepts: false belief, deception, faux pas, humor, sarcasm, and persuasion | Virtual Assessment of Mentalising Ability (VAMA): 12 video clips depicting a social drama within interactive virtual environment. | Interactive multi-modalities | I: Reasoning ability | Scored in two ways. Three-point scale: 0 (impaired), 0 (hyper), 1 (reduced) and 2 (accurate). Dichotomous scale: 1 (accurate), 0 (incorrect: any wrong response). | ||||
| Reading the Mind in the Eyes Test [32] | Infer mental states from the pictures of persons’ eyes and apply affective terms | Emotion recognition; Vocabulary comprehension; Aff ToM | 9 | Thirty-six eye photos showing emotions. Choose one term from four choices. Include definitions of emotional terms for reference. | Visual photos and verbal question | Multiple-choice questions | I: Face-recognition problems | 0, 1 | |
| The “Moving Shapes” paradigm V1 [60] | Infer intentions of silent cartoon figures enacting social drama | ToM, Social perception; Visual-spatial Problem solving | 6 | Twelve animations with two characters, a big red triangle and a small blue triangle, moving on framed white background. | Non-verbal animations | Open-ended questions | I: Alexithymia problem and empathetic ability | Four dimensions: Intentionality: 0–5; Appropriateness: 0–3. Certainty: 0–3; Length: 0–4. | |
| V2 [60,61,62] | A large triangle, small triangle and small circle enact social drama. Both versions contain following questions. | Multiple choice questions | No | 0, 1. | |||||
| ToM Task | n of Included Studies | Reliability (n of Reporting Study) | Validity (n of Reporting Study) | |||||
|---|---|---|---|---|---|---|---|---|
| Internal Consistency | Test–retest Reliability | Unidimensionality | Known-Group Validity (SCZ vs. HC) | Convergent Validity | Criterion Validity | Ecological Validity | ||
| HT | 11 | ω = 0.57 (1) | ICC = 0.78 (1) | NA | p < 0.0001 to p = 0.03 (11) | r = 0.352 to 0.477 (5) | r = 0.243 to 0.276 (2) | NA |
| FB1 | 15 | NA | ICC = 0.31 (1) | NA | p = 0.055 to 0.293 (7); p < 0.001 to p < 0.01 (7) | NA | NA | NA |
| FB2 | 14 | NA | ICC = 0.31 (1) | NA | p = 0.17 to 0.27 (3); p < 0.0001 to p = 0.02 (11) | NA | NA | NA |
| FB-seq | 14 | α = 0.54 | NA | Supported: IRT: χ2 (2) = 3.65, p = 0.186, CFI = 0.994, TLI = 0.988, RMSEA = 0.054 (1) | p = 0.056 to 0.282 (3); p < 0.0005 to p = 0.023 (9) | NA | r = 0.23 to 0.31 (1) | NA |
| CIT | 4 | NA | NA | NA | p = 0.88 (1); p < 0.0001 to p < 0.05 (3) | NA | NA | NA |
| VJ | 5 | α = 0.83 (1) | NA | NA | p = 0.08 (1); p < 0.0001 to p < 0.001 (4) | NA | NA | NA |
| IR | 5 | NA | NA | NA | p < 0.0001 to p < 0.01 (5) | NA | NA | NA |
| FP | 11 | α = 0.816 (1) | ICC = 0.76 (1) | NA | p = 0.0003 to 0.041 (9) | r = 0.34 to 0.68 (3) | NA | NA |
| Yoni | 6 | NA | NA | NA | p > 0.05 on first order ToM (2); p > 0.05 on cognitive ToM (2); p < 0.001 to p = 0.049 (6) | NA | r = -0.261 (1) | NA |
| ST | 5 | NA | ICC = 0.5 (1) | NA | p < 0.001 to 0.038 (4) | NA | r = 0.01 to 0.24 (1) | r = 0.07 to 0.19 (1) |
| MSC | 3 | NA | NA | NA | p < 0.001 (3) | r = 0.51 to 0.63 (3) | NA | NA |
| RMET | 9 | α = 0.735 (1) | ICC = 0.24 (1); r = 0.753 (1) | NA | p < 0.0001 to p < 0.05 (8) | r = 0.46 to 0.49 (1) | r = 0.01 to 0.43 (2) | r = 0.02 to 0.26 (1) |
| MS | 6 | α = 0.80 to 0.84 (2) | NA | Not supported: χ2 (152) = 194.997, TLI = 0.858, CFI = 0.873, RMSEA = 0.069 (1) | p < 0.0001 to p = 0.001 (5) | r = 0.29 to 0.526 (4) | r = 0.29 to 0.47 (5); r = 0.23 (1) | NA |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yeh, Y.-C.; Lin, C.-Y.; Li, P.-C.; Hung, C.-F.; Cheng, C.-H.; Kuo, M.-H.; Chen, K.-L. A Systematic Review of the Current Measures of Theory of Mind in Adults with Schizophrenia. Int. J. Environ. Res. Public Health 2021, 18, 7172. https://doi.org/10.3390/ijerph18137172
Yeh Y-C, Lin C-Y, Li P-C, Hung C-F, Cheng C-H, Kuo M-H, Chen K-L. A Systematic Review of the Current Measures of Theory of Mind in Adults with Schizophrenia. International Journal of Environmental Research and Public Health. 2021; 18(13):7172. https://doi.org/10.3390/ijerph18137172
Chicago/Turabian StyleYeh, Ya-Chin, Chung-Ying Lin, Ping-Chia Li, Chi-Fa Hung, Chun-Hua Cheng, Ming-Hui Kuo, and Kuan-Lin Chen. 2021. "A Systematic Review of the Current Measures of Theory of Mind in Adults with Schizophrenia" International Journal of Environmental Research and Public Health 18, no. 13: 7172. https://doi.org/10.3390/ijerph18137172
APA StyleYeh, Y.-C., Lin, C.-Y., Li, P.-C., Hung, C.-F., Cheng, C.-H., Kuo, M.-H., & Chen, K.-L. (2021). A Systematic Review of the Current Measures of Theory of Mind in Adults with Schizophrenia. International Journal of Environmental Research and Public Health, 18(13), 7172. https://doi.org/10.3390/ijerph18137172