
The Impact of Land-Based Physical Activity Interventions on Self-Reported Health and Well-Being of Indigenous Adults: A Systematic Review


Abstract
1. Introduction
2. Materials and Methods
2.1. Inclusion/Exclusion Criteria
2.2. Study Screening and Selection
2.3. Data Analysis
3. Results
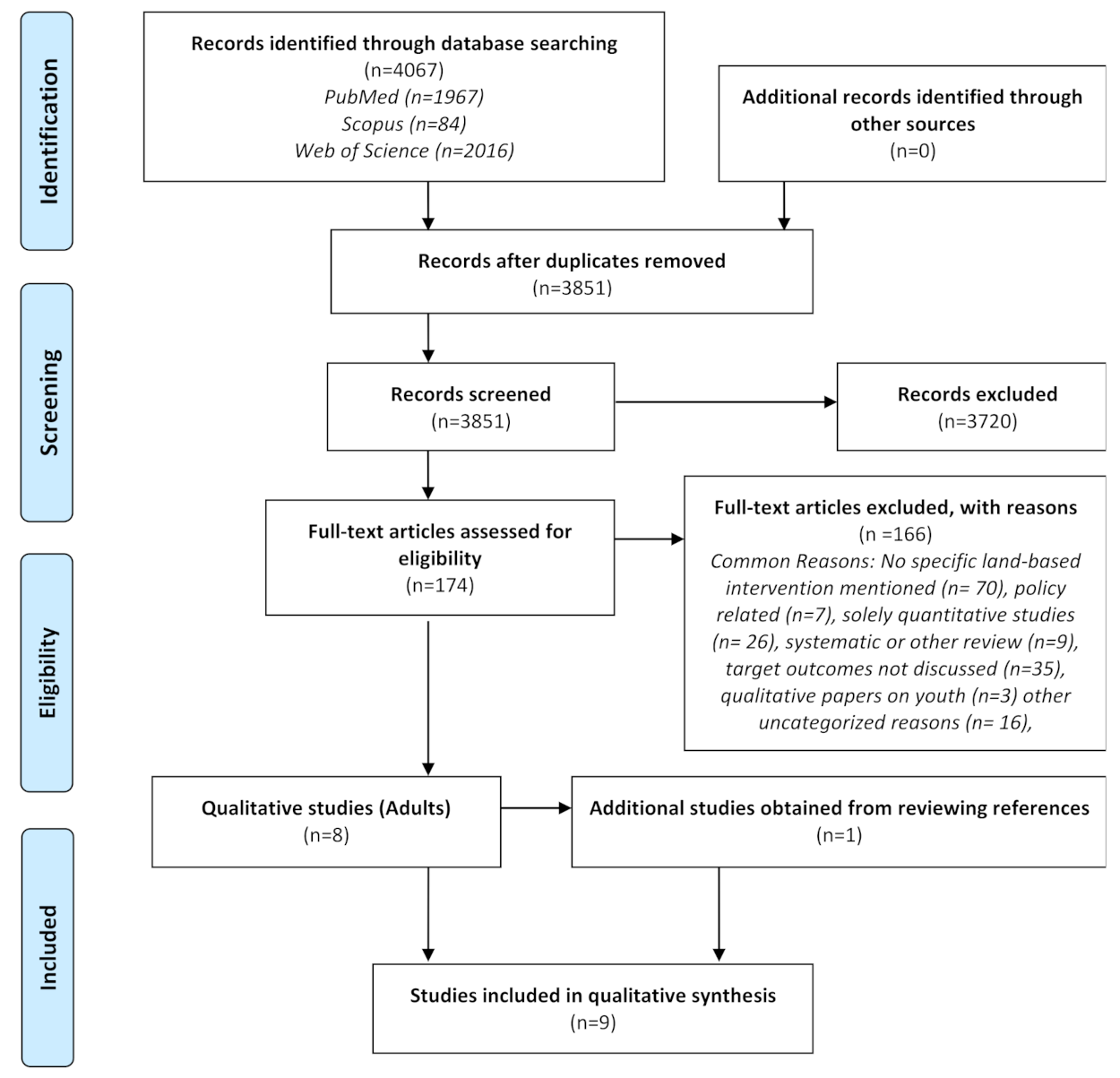
3.1. Study Selection
3.2. Study Characteristics
3.3. Thematic Analysis
3.3.1. Land-Based Physical Activities
3.3.2. Physical Health
3.3.3. Spiritual Health
3.3.4. Emotional and Mental Health
3.3.5. Community Engagement
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Butcher, E.; Breheny, M. Dependence on place: A source of autonomy in later life for older Maori. J. Aging Stud. 2016, 37, 48–58. [Google Scholar] [CrossRef]
- Green, B.L. Culture is treatment: Considering pedagogy in the care of Aboriginal people. J. Psychosoc. Nurs. Ment. Health Serv. 2010, 48, 27–34. [Google Scholar] [CrossRef]
- Durkheim, E. Sociology. Its Subject, Method and Purpose; Canon Publication: Moscow, Russia, 1995. [Google Scholar]
- Furgal, C.; Seguin, J. Climate change, health, and vulnerability in Canadian northern Aboriginal communities. Environ. Health Perspect. 2006, 114, 1964–1970. [Google Scholar] [CrossRef]
- Hossain, B.; Lamb, L. Cultural Attachment and Wellbeing Among Canada’s Indigenous People: A Rural Urban Divide. J. Happiness Stud. 2020, 21. [Google Scholar] [CrossRef]
- Cunsolo Willox, A.; Harper, S.L.; Ford, J.D.; Landman, K.; Houle, K.; Edge, V.L.; The Rigolet Inuit Community Government. “From this place and of this place:” climate change, sense of place, and health in Nunatsiavut, Canada. Adv. Nurs. Sci. 2012, 75, 538–547. [Google Scholar] [CrossRef]
- Cunsolo Willox, A.; Harper, S.L.; Edge, V.L.; Landman, K.; Houle, K.; Ford, J.D. The land enriches the soul: On climatic and environmental change, affect, and emotional health and well-being in Rigolet, Nunatsiavut, Canada. Emot. Space Soc. 2011, 6, 14–24. [Google Scholar] [CrossRef]
- Gone, J.P. Redressing First Nations historical trauma: Theorizing mechanisms for indigenous culture as mental health treatment. Transcult. Psychiatry 2013, 50, 683–706. [Google Scholar] [CrossRef]
- Johnson-Jennings, M.; Billiot, S.; Walters, K. Returning to Our Roots: Tribal Health and Wellness through Land-Based Healing. Genealogy 2020, 4, 91. [Google Scholar] [CrossRef]
- Schultz, K.; Walters, K.L.; Beltran, R.; Stroud, S.; Johnson-Jennings, M. “I’m stronger than I thought”: Native women reconnecting to body, health, and place. Health Place 2016, 40, 21–28. [Google Scholar] [CrossRef]
- Lombard, K.A.; Beresford, S.A.; Ornelas, I.J.; Topaha, C.; Becenti, T.; Thomas, D.; Vela, J.G. Healthy gardens/healthy lives: Navajo perceptions of growing food locally to prevent diabetes and cancer. Health Promot. Pr. 2014, 15, 223–231. [Google Scholar] [CrossRef]
- Sushames, A.; van Uffelen, J.G.; Gebel, K. Do physical activity interventions in Indigenous people in Australia and New Zealand improve activity levels and health outcomes? A systematic review. Int. J. Behav. Nutr. Phys. Act. 2016, 13, 129. [Google Scholar] [CrossRef] [PubMed]
- Kaholokula, J.K.; Look, M.; Mabellos, T.; Zhang, G.; de Silva, M.; Yoshimura, S.; Solatorio, C.; Wills, T.; Seto, T.B.; Sinclair, K.A. Cultural Dance Program Improves Hypertension Management for Native Hawaiians and Pacific Islanders: A Pilot Randomized Trial. J. Racial Ethn. Health Disparities 2017, 4, 35–46. [Google Scholar] [CrossRef] [PubMed]
- Bethune, R.; Absher, N.; Obiagwu, M.; Qarmout, T.; Steeves, M.; Yaghoubi, M.; Tikoo, R.; Szafron, M.; Dell, C.; Farag, M. Social determinants of self-reported health for Canada’s indigenous peoples: A public health approach. Public Health 2019, 176, 172–180. [Google Scholar] [CrossRef] [PubMed]
- Hopkins, S.E.; Kwachka, P.; Lardon, C.; Mohatt, G.V. Keeping busy: A Yup’ik/Cup’ik perspective on health and aging. Int. J. Circumpolar Health 2007, 66, 42–50. [Google Scholar] [CrossRef]
- Kriska, A.M.; Hanley, A.J.G.; Harris, S.B.; Zinman, B. Physical Activity, Physical Fitness, and Insulin and Glucose Concentrations in an Isolated Native Canadian Population Experiencing Rapid Lifestyle Change. Diabetes Care 2001, 24, 1787–1792. [Google Scholar] [CrossRef][Green Version]
- Oliver, N.; Perkins, D.; Hare, L.; Larsen, K. ‘Stories from the past, the reality of the present, taking control of the future’—Lifestyle changes among Pukapuka people in the Illawarra. Health Promot. J. Austr. 2007, 18, 105–108. [Google Scholar] [CrossRef]
- Valera, B.; Dewailly, E.; Poirier, P. Cardiac autonomic activity and blood pressure among Nunavik Inuit adults exposed to environmental mercury: A cross-sectional study. Environ. Health 2008, 7, 29. [Google Scholar] [CrossRef]
- Nu, J.; Bersamin, A. Collaborating With Alaska Native Communities to Design a Cultural Food Intervention to Address Nutrition Transition. Prog. Community Health Partn. 2017, 11, 71–80. [Google Scholar] [CrossRef]
- Dórea, J.G.; de Souza, J.R.; Rodrigues, P.; Ferrari, I.; Barbosa, A.C. Hair mercury (signature of fish consumption) and cardiovascular risk in Munduruku and Kayabi Indians of Amazonia. Environ. Res. 2005, 97, 209–219. [Google Scholar] [CrossRef]
- Kant, S.; Vertinsky, I.; Zheng, B.; Smith, P.M. Social, cultural, and land use determinants of the health and well-being of Aboriginal peoples of Canada: A path analysis. J. Public Health Policy 2013, 34, 462–476. [Google Scholar] [CrossRef][Green Version]
- Iwasaki, Y.; Bartlett, J.G. Culturally Meaningful Leisure as a Way of Coping with Stress among Aboriginal Individuais with Diabetes. J. Leis. Res. 2006, 38, 321–338. [Google Scholar] [CrossRef]
- Ebbesson, S.O.E.; Ebbesson, L.O.E.; Swenson, M.; Kennish, J.M.; Robbins, D.C. A successful diabetes prevention study in Eskimos: The Alaska Siberia project. Int. J. Circumpolar Health 2005, 64, 409–424. [Google Scholar] [CrossRef]
- Look, M.A.; Kaholokula, J.K.; Carvhalo, A.; Seto, T.; de Silva, M. Developing a culturally based cardiac rehabilitation program: The HELA study. Prog. Community Health Partn. 2012, 6, 103–110. [Google Scholar] [CrossRef]
- Look, M.A.; Maskarenic, G.G.; De Silva, M.; Seto, T.; Mau, M.L.; Kaholokula, J.K. Kumu Hula Perspectives on Health. Hawaii J. Med. Public Health 2014, 73, 21–25. [Google Scholar]
- Chadwick, J.Q.; Tullier, M.A.; Wolbert, L.; Coleman, C.; Branam, D.E.; Wharton, D.F.; Cannady, T.K.; Copeland, K.C.; Short, K.R. Collaborative implementation of a community-based exercise intervention with a partnering rural American Indian community. Clin. Trials 2019, 16, 391–398. [Google Scholar] [CrossRef]
- Philibert, A.; Schwartz, H.; Merg, D. An Exploratory Study of Diabetes in a First Nation Community with Respect to Serum Concentrations of p,p’-DDE and PCBs and Fish Consumption. Int. J. Environ. Res. Public Health 2009, 6, 3179–3189. [Google Scholar] [CrossRef]
- Ketheesan, S.; Rinaudo, M.; Berger, M.; Wenitong, M.; Juster, R.P.; McEwen, B.S.; Sarnyai, Z. Stress, allostatic load and mental health in Indigenous Australians. Stress 2020, 23, 509–518. [Google Scholar] [CrossRef]
- Flint, C.G.; Robinson, E.S.; Kellogg, J.; Ferguson, G.; Boufajreldin, L.; Dolan, M.; Raskin, I.; Lila, M.A. Promoting wellness in Alaskan villages: Integrating traditional knowledge and science of wild berries. Ecohealth 2011, 8, 199–209. [Google Scholar] [CrossRef]
- MacDonald, J.P.; Cunsolo Willox, A.; Ford, J.D.; Shiwak, I.; Wood, M.; IMHACC Team; The Rigolet Inuit Community Government. Protective factors for mental health and well-being in a changing climate: Perspectives from Inuit youth in Nunatsiavut, Labrador. Soc. Sci. Med. 2015, 141, 133–141. [Google Scholar] [CrossRef]
- Espinoza Giacinto, R.; Castaneda, S.F.; Perez, R.L.; Nodora, J.N.; Gonzalez, P.; Lopez, E.J.; Talavera, G.A. Diabetes Cultural Beliefs and Traditional Medicine Use Among Health Center Patients in Oaxaca, Mexico. J. Immigr. Minor. Health 2016, 18, 1413–1422. [Google Scholar] [CrossRef]
- Wolsko, C.; Lardon, C.; Hopkins, S.; Ruppert, E. Conceptions of wellness among the Yup’ik of the Yukon-Kuskokwim Delta: The vitality of social and natural connection. Ethn. Health 2006, 11, 345–363. [Google Scholar] [CrossRef]
- Gall, A.; Butler, T.L.; Lawler, S.; Garvey, G. Traditional, complementary and integrative medicine use among Indigenous peoples with diabetes in Australia, Canada, New Zealand and the United States. Aust. N.Z. J. Public Health 2021. [Google Scholar] [CrossRef]
- Hanemaayer, R.; Anderson, K.; Haines, J.; Lickers, K.R.; Lickers Xavier, A.; Gordon, K.; Tait Neufeld, H. Exploring the Perceptions of and Experiences with Traditional Foods among First Nations Female Youth: A Participatory Photovoice Study. Int. J. Environ. Res. Public Health 2020, 17, 2214. [Google Scholar] [CrossRef]
- Tsuji, L.J.S.; Ho, E. Traditional Environmental Knowledge and Western Science: In Search of Common Ground. Can. J. Nativ. Stud. 2002, 22, 237. [Google Scholar]
- Bartlett, C.; Marshall, M.; Marshall, A. Two-Eyed Seeing and other lessons learned within a co-learning journey of bringing together indigenous and mainstream knowledges and ways of knowing. J. Environ. Stud. Sci. 2012, 2, 331–340. [Google Scholar] [CrossRef]
- Peltier, C. An Application of Two-Eyed Seeing: Indigenous Research Methods With Participatory Action Research. Int. J. Qual. Methods 2018, 17, 1609406918812346. [Google Scholar] [CrossRef]
- Tobias, J.K.; Richmond, C.A.M.; Luginaah, I. Community-Based Participatory Research (CBPR) with Indigenous Communities: Producing Respectful and Reciprocal Research. J. Empir. Res. Hum. Res. Ethics Int. J. 2013, 8, 129–140. [Google Scholar] [CrossRef]
- Holkup, P.A.; Tripp-Reimer, T.; Salois, E.M.; Weinert, C. Community-based participatory research: An approach to intervention research with a Native American community. ANS Adv. Nurs. Sci. 2004, 27, 162–175. [Google Scholar] [CrossRef]
- Castleden, H.; Garvin, T. Modifying Photovoice for community-based participatory Indigenous research. Soc. Sci. Med. 2008, 66, 1393–1405. [Google Scholar] [CrossRef]
- Marsh, T.N.; Cote-Meek, S.; Toulouse, P.; Najavits, L.M.; Young, N.L. The Application of Two-Eyed Seeing Decolonizing Methodology in Qualitative and Quantitative Research for the Treatment of Intergenerational Trauma and Substance Use Disorders. Int. J. Qual. Methods 2015, 14, 1609406915618046. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; The Prisma Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- United Nations. Fact sheet No. 1, The United Nations Permenant Forum on Indigenous issues (fifth session): Indigenous Peoples and Identity, May 2006. Available online: https://www.un.org/esa/socdev/unpfii/documents/5session_factsheet1.pdf (accessed on 15 August 2020).
- United Nations. Convention on the Rights of the Child. Commissioner. Available online: https://www.ohchr.org/en/professionalinterest/pages/crc.aspx (accessed on 27 August 2020).
- The Joanna Briggs Institute. The Joanna Briggs Institute Critical Appraisal Tools for Use in JBI Systematic Reviews: Checklist for Qualitative Research. Available online: https://jbi.global/sites/default/files/2019-05/JBI_Critical_Appraisal-Checklist_for_Qualitative_Research2017_0.pdf (accessed on 15 August 2020).
- Thomas, J.; Harden, A. Methods for the thematic synthesis of qualitative research in systematic reviews. BMC Med. Res. Methodol. 2008, 8. [Google Scholar] [CrossRef] [PubMed]
- Forbes, A.; Ritchie, S.; Walker, J.; Young, N. Applications of Two-Eyed Seeing in Primary Research Focused on Indigenous Health: A Scoping Review. Int. J. Qual. Method 2020, 19, 1–18. [Google Scholar] [CrossRef]
- Robertson, S.; Ljubicic, G. Nunamii’luni quvianaqtuq (It is a happy moment to be on the land): Feelings, freedom and the spatial political ontology of well-being in Gjoa Haven and Tikiranajuk, Nunavut. Environ. Plan. D Soc. Space 2019, 37, 542–560. [Google Scholar] [CrossRef]
- The University of British Columbia. Indigenous Peoples: Language Guidelines 2021 (version 3.0). Available online: http://assets.brand.ubc.ca/downloads/ubc_indigenous_peoples_language_guide.pdf (accessed on 16 June 2021).
- Lines, L.A.; Yellowknives Dene First Nation Wellness Division; Jardine, C.G. Connection to the land as a youth-identified social determinant of Indigenous Peoples’ health. BMC Public Health 2019, 19, 176. [Google Scholar] [CrossRef]
- Nystad, K.; Spein, A.R.; Ingstad, B. Community resilience factors among indigenous Sami adolescents: A qualitative study in Northern Norway. Transcult. Psychiatry 2014, 51, 651–672. [Google Scholar] [CrossRef]
- Teufel-Shone, N.I.; Fitzgerald, C.; Teufel-Shone, L.; Gamber, M. Systematic review of physical activity interventions implemented with American Indian and Alaska Native populations in the United States and Canada. Am. J. Health Promot. 2009, 23, S8–S32. [Google Scholar] [CrossRef]
- Bazzarre, T.L. Adapting physical activity interventions to prevent obesity in culturally diverse populations. Am. J. Health Promot. 2009, 23, S1–S3. [Google Scholar] [CrossRef]
- Proust, F.; Johnson-Down, L.; Berthiaume, L.; Greffard, K.; Julien, P.; Robinson, E.; Lucas, M.; Dewailly, É. Fatty acid composition of birds and game hunted by the Eastern James Bay Cree people of Québec. Int. J. Circumpolar Health 2016, 75, 30583. [Google Scholar] [CrossRef][Green Version]
- Restoule, J.P.; Gruner, S.; Metatawabin, E. Learning from place: A return to traditional mushkegowuk ways of knowing. Can. J. Educ. 2013, 36, 68–86. [Google Scholar]
- Pelletier, C.A.; Smith-Forrester, J.; Klassen-Ross, T. A systematic review of physical activity interventions to improve physicalfitness and health outcomes among Indigenous adults living in Canada. Prev. Med. Rep. 2017, 8, 242–249. [Google Scholar] [CrossRef] [PubMed]
- Isaac, G.; Finn, S.; Joe, J.R.; Hoover, E.; Gone, J.P.; Lefthand-Begay, C.; Hill, S. Native American Perspectives on Health and Traditional Ecological Knowledge. Environ. Health Perspect. 2018, 126, 125002. [Google Scholar] [CrossRef] [PubMed]
- Khalafzai, M.A.K.; McGee, T.K.; Parlee, B. Flooding in the James Bay region of Northern Ontario, Canada: Learning from traditional knowledge of Kashechewan First Nation. Int. J. Disaster Risk Reduct. 2019, 36, 101100. [Google Scholar] [CrossRef]
- Royer, M.-J.; Herrmann, T.; Sonnentag, O.; Fortier, D.; Delusca, K.; Cuciurean, R. Linking Cree Hunters? and scientific observations of changing inland ice and meteorological conditions in the subarctic Eastern James Bay region, Canada. Clim. Chang. 2013, 119. [Google Scholar] [CrossRef]
- Royer, M.J.S. Climate, Environment and Cree Observations: James Bay Territory, Canada, 1st ed.; Springer International Publishing AG: Cham, Switzerland; Basel, Switzerland, 2016; pp. 15–16. [Google Scholar]
- Kutz, S.; Tomaselli, M. “Two-eyed seeing” supports wildlife health. Science 2019, 364, 1135. [Google Scholar] [CrossRef]
- Tsuji, L.J.S.; Tsuji, S.R.J.; Zuk, A.M.; Davey, R.; Liberda, E.N. Harvest Programs in First Nations of Subarctic Canada: The Benefits Go Beyond Addressing Food Security and Environmental Sustainability Issues. Int. J. Environ. Res. Public Health 2020, 17, 8113. [Google Scholar] [CrossRef]
- Ryan, G.; Sean, M.D.; Jordyn, G.; Christine, M.D. Cheyenne River Sioux Traditions and Resistance to the Dakota Access Pipeline. Relig. Soc. 2020, 11, 75. [Google Scholar] [CrossRef]
- Foulds, H.J.A.; Bredin, S.S.D.; Warburton, D.E.R. The effectiveness of community based physical activity interventions with Aboriginal peoples. Prev. Med. 2011, 53, 411–416. [Google Scholar] [CrossRef]
- Israel, B.A.; Schulz, A.J.; Parker, E.; Becker, A.; Allen, A.J.; Guzman, R. Critical issues in developing and following CBPR principles. In Community-Based Participatory Research for Health, 2nd ed.; Minkler, M., Wallerstein, N., Eds.; Jossey-Bass: San Francisco, CA, USA, 2008; pp. 47–66. [Google Scholar]
- Bingham, B.; Moniruzzaman, A.; Patterson, M.; Sareen, J.; Distasio, J.; O’Neil, J.; Somers, J.M. Gender differences among Indigenous Canadians experiencing homelessness and mental illness. BMC Psychol. 2019, 7, 57. [Google Scholar] [CrossRef]
- Jen’nan Ghazal, R.; Bridget, K.G. Gender and Health Inequality. Annu. Rev. Sociol. 2010, 36, 371–386. [Google Scholar] [CrossRef]
- Breda, K.L. Participatory Action Research. In Nursing Research Using Participatory Action Research: Qualitative Designs and Methods in Nursing; De Chesnay, M., Ed.; Springer Publishing Company: New York, NY, USA, 2014; pp. 1–12. [Google Scholar] [CrossRef]


{kind=link}
| Study | Population; Region | Total Sample Size (N); Sex; Age | Objective | Traditional Physical Activity | Data Recruitment | Methodology |
|---|---|---|---|---|---|---|
| Wolsko, Lardon, Hopkins and Ruppert [32] | Yup’ik; Yukon- Kuskokwin Delta, USA |
|
|
|
|
|
| Hopkins, Kwachka, Lardon and Mohatt [15] | Yup’ik; Yukon- Kuskokwin Delta, USA |
|
| Subsistence activities Hunting, fishing, and berry picking | Advertisements (village traditional councils and local health clinics)
|
|
| Look, Kaholokula, Carvhalo, Seto and de Silva [24] | Native Hawaiians; Hawaii, USA |
|
|
|
|
|
| Look, Maskarenic, De Silva, Seto, Mau and Kaholokula [25] | Native Hawaiians; Hawaii, USA |
|
|
|
|
|
| Lombard, Beresford, Ornelas, Topaha, Becenti, Thomas and Vela [11] | Navajo; San Juan County, New Mexico, USA |
|
|
|
|
|
| Schultz, Walters, Beltran, Stroud and Johnson-Jennings [10] | Choctaw Tribe; Oklahoma, USA |
|
|
|
|
|
| Johnson-Jennings, Billiot and Walters [9] | The United Houma Nation; Louisiana, USA |
|
|
|
|
|
| Iwasaki and Bartlett [22] | Urban Indigenous (First Nations & Métis); Region not specified, Canada |
|
|
|
|
|
| Robertson and Ljubicic [48] | Uqsuqtuurmiut; Uqsuqtuuq (Gjoa Haven, Nunavut), Canada |
|
|
|
|
|
| Descriptive Themes | Analytical Themes |
|---|---|
| Land-based Physical Activities | |
| Physical health | |
| Spiritual health | |
| Emotional and Mental health |
|
| Community Engagement |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ahmed, F.; Zuk, A.M.; Tsuji, L.J.S. The Impact of Land-Based Physical Activity Interventions on Self-Reported Health and Well-Being of Indigenous Adults: A Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 7099. https://doi.org/10.3390/ijerph18137099
Ahmed F, Zuk AM, Tsuji LJS. The Impact of Land-Based Physical Activity Interventions on Self-Reported Health and Well-Being of Indigenous Adults: A Systematic Review. International Journal of Environmental Research and Public Health. 2021; 18(13):7099. https://doi.org/10.3390/ijerph18137099
Chicago/Turabian StyleAhmed, Fatima, Aleksandra M. Zuk, and Leonard J. S. Tsuji. 2021. "The Impact of Land-Based Physical Activity Interventions on Self-Reported Health and Well-Being of Indigenous Adults: A Systematic Review" International Journal of Environmental Research and Public Health 18, no. 13: 7099. https://doi.org/10.3390/ijerph18137099
APA StyleAhmed, F., Zuk, A. M., & Tsuji, L. J. S. (2021). The Impact of Land-Based Physical Activity Interventions on Self-Reported Health and Well-Being of Indigenous Adults: A Systematic Review. International Journal of Environmental Research and Public Health, 18(13), 7099. https://doi.org/10.3390/ijerph18137099