
Maternal Anxiety, Infant Stress, and the Role of Live-Performed Music Therapy during NICU Stay in The Netherlands

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Setting and Population
2.2. Developmental Care Practices at Our NICU
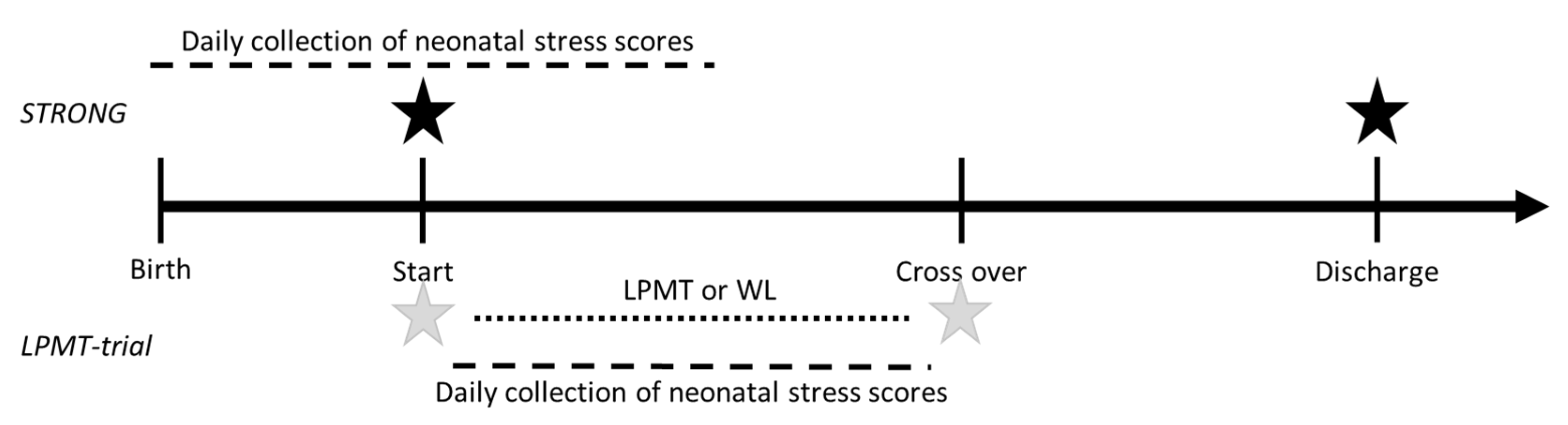
2.3. Measures and Procedure
2.3.1. Outcome Measures for Maternal Anxiety
2.3.2. Outcome Measure for Infant Stress
2.3.3. Interventional Music Therapy
2.4. Statistical Analyses
3. Results
3.1. Participants Characteristics
3.1.1. Characteristics of Participants in the STRONG Study
3.1.2. Characteristics of Participants in the LPMT Trial
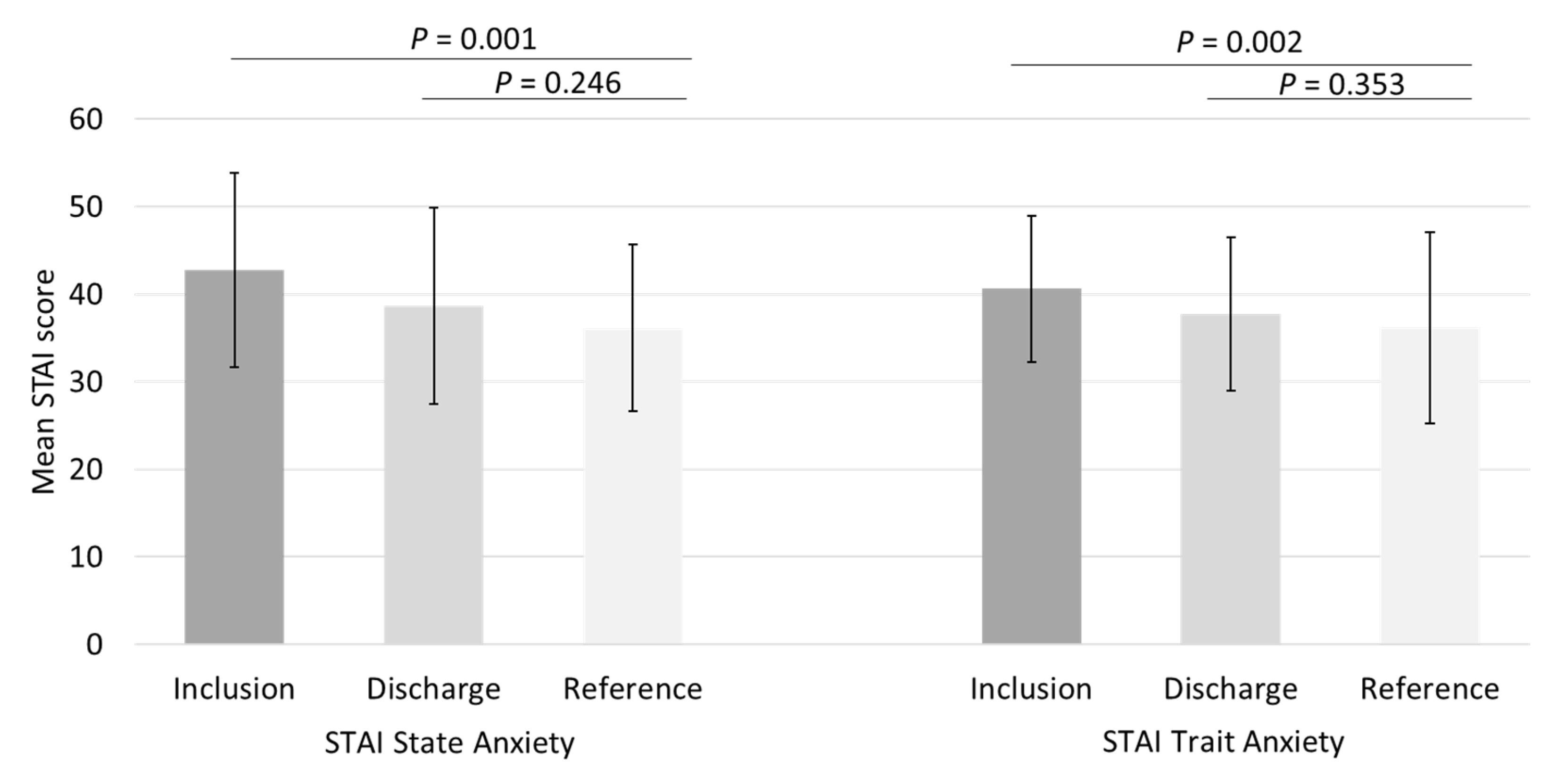
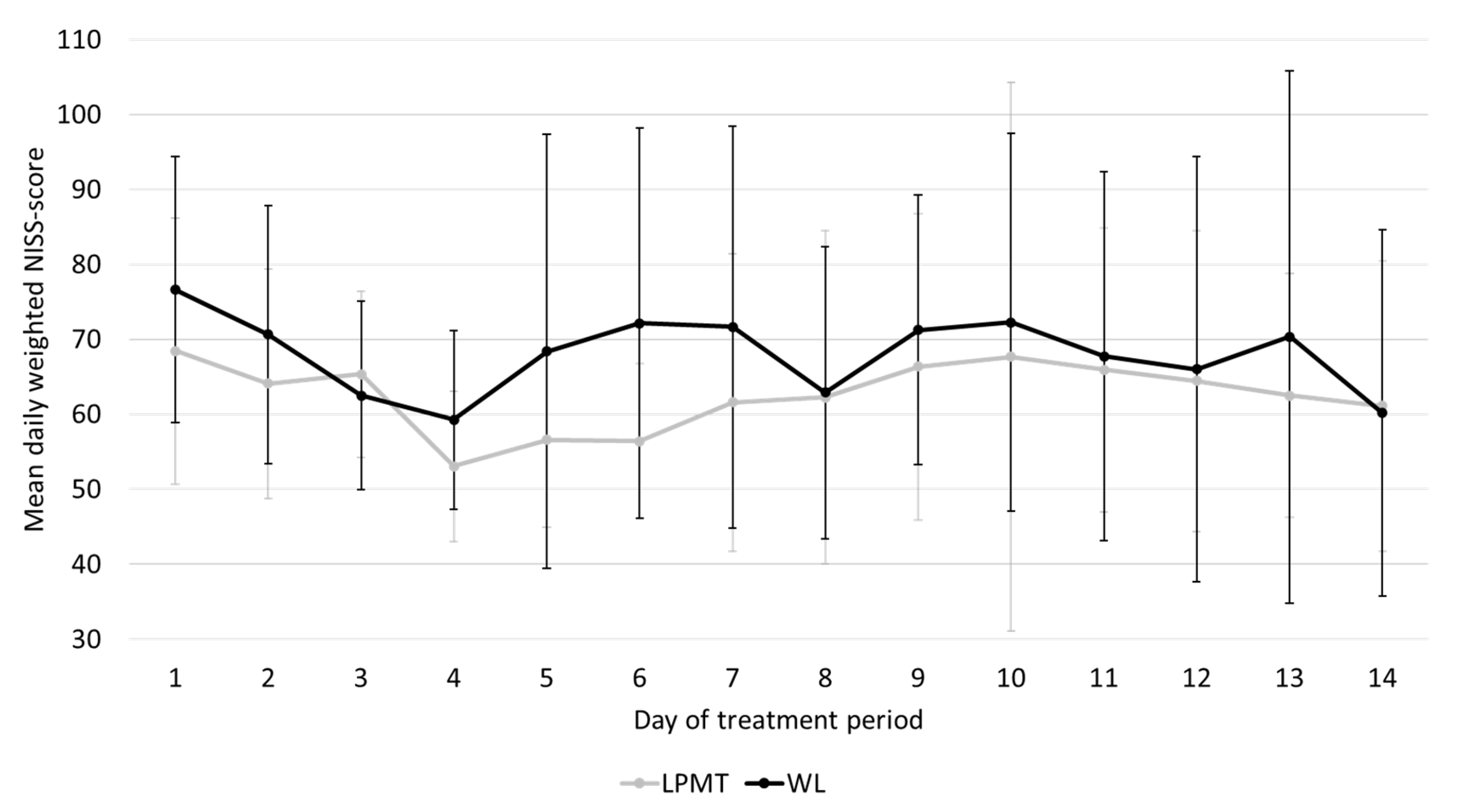
3.2. Maternal Anxiety during NICU Stay and Association between Infant Stress and Maternal Anxiety Symptoms
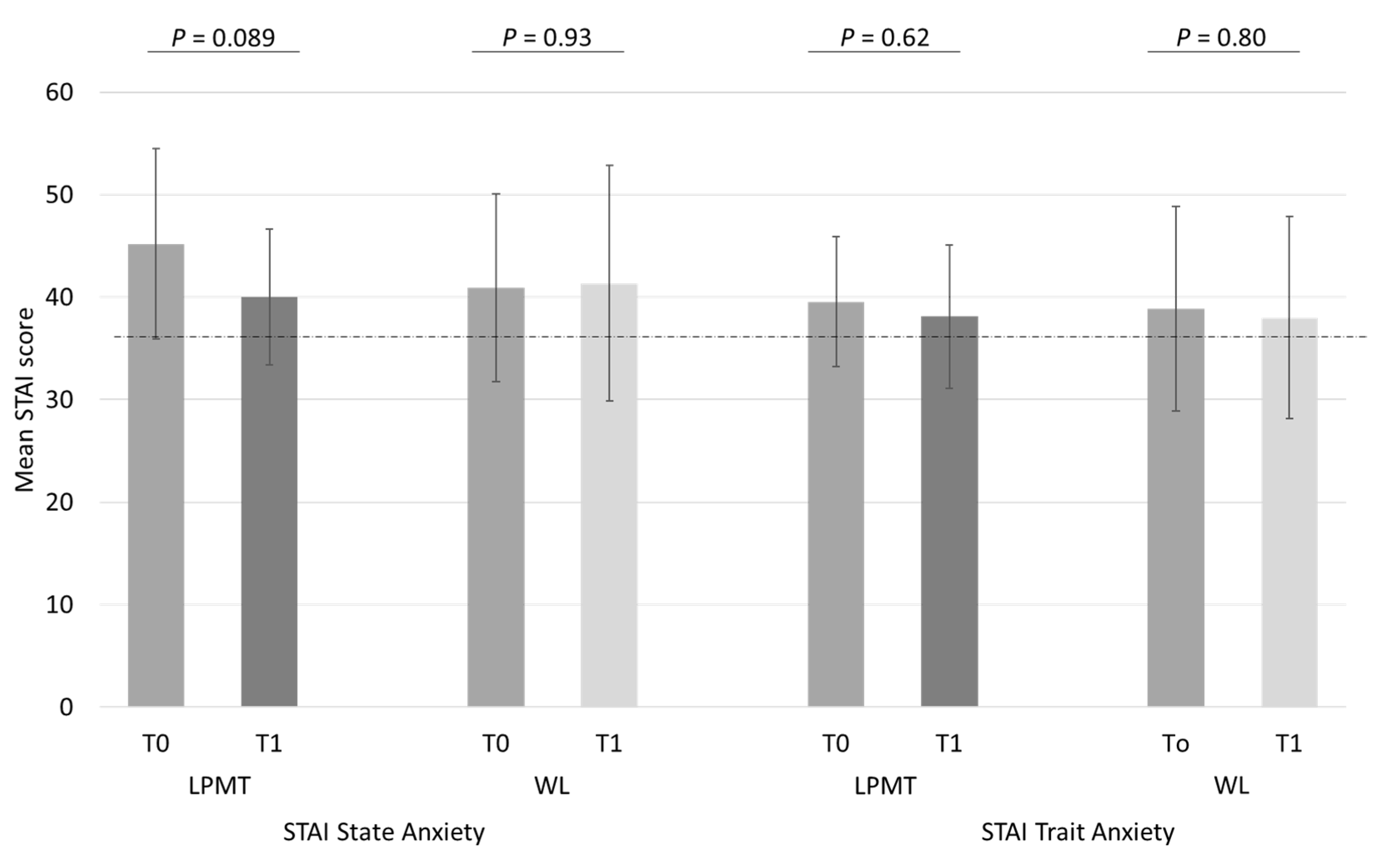
3.3. Effects of Our Music Therapy Program on Maternal Anxiety
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Obeidat, H.M.; Bond, E.A.; Callister, L.C. The Parental Experience of Having an Infant in the Newborn Intensive Care Unit. J. Perinat. Educ. 2009, 18, 23–29. [Google Scholar] [CrossRef]
- Cong, X.; Wu, J.; Vittner, D.; Xu, W.; Hussain, N.; Galvin, S.; Fitzsimons, M.; McGrath, J.M.; Henderson, W.A. The impact of cumulative pain/stress on neurobehavioral development of preterm infants in the NICU. Early Hum. Dev. 2017, 108, 9–16. [Google Scholar] [CrossRef] [Green Version]
- Cheong, J.L.Y.; Burnett, A.C.; Treyvaud, K.; Spittle, A.J. Early environment and long-term outcomes of preterm infants. J. Neural Transm. 2020, 127, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Valeri, B.O.; Holsti, L.; Linhares, M.B.M. Neonatal Pain and Developmental Outcomes in Children Born Preterm: A Systematic Review. Clin. J. Pain 2015, 31, 355–362. [Google Scholar] [CrossRef]
- Caporali, C.; Pisoni, C.; Gasparini, L.; Ballante, E.; Zecca, M.; Orcesi, S.; Provenzi, L. A global perspective on parental stress in the neonatal intensive care unit: A meta-analytic study. J. Perinat. 2020, 40, 1739–1752. [Google Scholar] [CrossRef]
- Staver, M.A.; Moore, T.A.; Hanna, K.M. Maternal Distress in the Neonatal Intensive Care Unit: A Concept Analysis. Adv. Neonatal Care 2019, 19, 394–401. [Google Scholar] [CrossRef] [PubMed]
- Pace, C.C.; Spittle, A.J.; Molesworth, C.M.L.; Lee, K.J.; Northam, E.A.; Cheong, J.L.Y.; Davis, P.G.; Doyle, L.W.; Treyvaud, K.; Anderson, P.J. Evolution of Depression and Anxiety Symptoms in Parents of Very Preterm Infants During the Newborn Period. JAMA Pediatr. 2016, 170, 863–870. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oyetunji, A.; Chandra, P. Postpartum stress and infant outcome: A review of current literature. Psychiatry Res. 2020, 284, 112769. [Google Scholar] [CrossRef]
- Schecter, R.; Pham, T.; Hua, A.; Spinazzola, R.; Sonnenklar, J.; Li, D.; Papaioannou, H.; Milanaik, R. Prevalence and Longevity of PTSD Symptoms Among Parents of NICU Infants Analyzed Across gestational Age Categories. Clin. Pediatr. 2020, 59, 163–169. [Google Scholar] [CrossRef]
- Gerstein, E.D.; Njoroge, W.F.M.; Paul, R.A.; Smyser, C.D.; Rogers, C.E. Maternal Depression and Stress in the Neonatal Intensive Care Unit: Associations With Mother-Child Interactions at Age 5 Years. J. Am. Acad. Child. Adolesc. Psychiatry 2019, 58, 350–358. [Google Scholar] [CrossRef]
- Zelkowitz, P.; Na, S.; Wang, T.; Bardin, C.; Papageorgiou, A. Early maternal anxiety predicts cognitive and behavioural outcomes of VLBW children at 24 months corrected age. Acta Paediatr. 2011, 100, 700–704. [Google Scholar] [CrossRef]
- Holditch-Davis, D.; White-Traut, R.C.; Levy, J.A.; O’Shea, T.M.; Geraldo, V.; David, R.J. Maternally administered interventions for preterm infants in the NICU: Effects on maternal psychological distress and mother–infant relationship. Infant Behav. Dev. 2014, 37, 695–710. [Google Scholar] [CrossRef] [Green Version]
- Sabnis, A.; Fojo, S.; Nayak, S.S.; Lopez, E.; Tarn, D.M.; Zeltzer, L. Reducing Parental Trauma and Stress in Neonatal Intensive Care: Systematic Review and Meta-Analysis of Hospital Interventions. J. Perinatol. 2019, 39, 375–386. [Google Scholar] [CrossRef]
- Shaw, R.J.; St John, N.; Lilo, E.; Jo, B.; Benitz, W.; Stevenson, D.K.; Horwitz, S.M. Prevention of Traumatic Stress in Mothers of Preterms: 6-Month Outcomes. Pediatrics 2014, 134, e481–e488. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hynan, M.T.; Hall, S.L. Psychosocial program standards for NICU parents. J. Perinatol. 2015, 35, S1–S4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- AMTA: American Music Therapy Association. Available online: https://www.musictherapy.org/about/quotes/ (accessed on 31 May 2021).
- Loewy, J.; Stewart, K.; Dassler, A.; Telsey, A.; Homel, P. The Effects of Music Therapy on Vital Signs, Feeding, and Sleep in Premature Infants. Pediatrics 2013, 131, 902–918. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haslbeck, F.B. Music therapy for premature infants and their parents: An integrative review. Nord. J. Music Ther. 2012, 21, 203–226. [Google Scholar] [CrossRef]
- Williamson, S.; McGrath, J.M. What Are the Effects of the Maternal Voice on Preterm Infants in the NICU? Adv. Neonatal Care 2019, 19, 294–310. [Google Scholar] [CrossRef] [PubMed]
- Bieleninik, Ł.; Ghetti, C.; Gold, C. Music Therapy for Preterm Infants and Their Parents: A Meta-analysis. Pediatrics 2016, 138, e20160971. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bos, M.; van Dokkum, N.H.; Ravensbergen, A.G.; Kraft, K.E.; Bos, A.F.; Jaschke, A.C. Pilot study finds that performing live music therapy in intensive care units may be beneficial for infants’ neurodevelopment. Acta Paediatr. 2021, 1–2. [Google Scholar] [CrossRef]
- Ettenberger, M.; Bieleninik, Ł.; Epstein, S.; Elefant, C. Defining Attachment and Bonding: Overlaps, Differences and Implications for Music Therapy Clinical Practice and Research in the Neonatal Intensive Care Unit (NICU). Int. J. Environ. Res. Public Health 2021, 18, 1733. [Google Scholar] [CrossRef] [PubMed]
- Kehl, S.M.; La Marca-Ghaemmaghami, P.; Haller, M.; Pichler-Stachl, E.; Bucher, H.U.; Bassler, D.; Haslbeck, F.B. Creative Music Therapy with Premature Infants and Their Parents: A Mixed-Method Pilot Study on Parents’ Anxiety, Stress and Depressive Symptoms and Parent–Infant Attachment. Int. J. Environ. Res. Public Health 2021, 18, 265. [Google Scholar] [CrossRef] [PubMed]
- Spielberger, C.D.; Gorsuch, R.L.; Lushene, R.; Vagg, P.R.; Jacobs, G.A. State-Trait Anxiety Inventory for Adults Sampler Set Manual, Instrument and Scoring Guide; Consulting Psychologists Press/Mind Garden, Inc.: Palo Alto, CA, USA, 1983. [Google Scholar]
- Dennis, C.-L.; Coghlan, M.; Vigod, S. Can we identify mothers at-risk for postpartum anxiety in the immediate postpartum period using the State-Trait Anxiety Inventory? J. Affect. Disord. 2013, 150, 1217–1220. [Google Scholar] [CrossRef] [PubMed]
- Newnham, C.A.; Inder, T.E.; Milgrom, J. Measuring preterm cumulative stressors within the NICU: The neonatal infant stressor scale. Early Hum. Dev. 2009, 85, 549–555. [Google Scholar] [CrossRef] [PubMed]
- Pourkaviani, S.; Zhang, X.; Spear, E.A.; D’Agostino, M.; Satty, R.E.; Liu, S.H.; Stroustrup, A. Clinical validation of the neonatal infant stressor scale with 312 preterm infant salivary cortisol. Pediatr Res. 2020, 87, 1237–1243. [Google Scholar] [CrossRef]
- Loewy, J. NICU music therapy: Song of kind as critical lullaby in reseachrch and practice. Ann. N. Y. Acad. Sci. 2015, 1337, 178–185. [Google Scholar] [CrossRef]
- Van Dokkum, N.H.; Jaschke, A.C.; Ravensbergen, A.G.; Reijneveld, S.A.; Hakvoort, L.; de Kroon, M.L.A.; Bos, A.F. Feasibility of Live-Performed Music Therapy for Extremely and Very Preterm Infants in a Tertiary NICU. Front. Pediatr. 2020, 8, 581372. [Google Scholar] [CrossRef]
- Helle, N.; Barkmann, C.; Ehrhardt, S.; von der Wense, A.; Nestoriuc, Y.; Bindt, C. Postpartum anxiety and adjustment disorders in parents of infants with very low birth weight: Cross-sectional results from a controlled multicentre cohort study. J. Affect. Disord. 2016, 194, 128–134. [Google Scholar] [CrossRef]
- Bonacquisti, A.; Geller, P.A.; Patterson, C.A. Maternal depression, anxiety, stress, and maternal-infant attachment in the neonatal intensive care unit. J. Reprod. Infant Psychol. 2020, 38, 297–310. [Google Scholar] [CrossRef]
- Emmanuel, E.; St John, W. Maternal distress: A concept analysis. J. Adv. Nurs. 2010, 66, 2104–2115. [Google Scholar] [CrossRef] [Green Version]
- Medina, I.M.F.; Granero-Molina, J.; Fernández-Sola, C.; Hernández-Padilla, J.M.; Ávila, M.C.; Rodríguez, M.D.M.L. Bonding in neonatal intensive care units: Experiences of extremely preterm infants’ mothers. Women Birth 2018, 31, 325–330. [Google Scholar] [CrossRef] [PubMed]
- Greene, M.M.; Rossman, B.; Meier, P.; Patra, K. Elevated maternal anxiety in the NICU predicts worse fine motor outcome in VLBW infants. Early Hum. Dev. 2018, 116, 33–39. [Google Scholar] [CrossRef] [PubMed]
- Alkozei, A.; McMahon, E.; Lahav, A. Stress levels and depressive symptoms in NICU mothers in the early postpartum period. J. Matern. Fetal Neonatal Med. 2014, 27, 1738–1743. [Google Scholar] [CrossRef] [PubMed]
- Ribeiro, M.K.A.; Alcântara-Silva, T.R.M.; Oliveira, J.C.M.; Paula, T.C.; Dutra, J.B.R.; Pedrino, G.R.; Simões, K.; Sousa, R.B.; Rebelo, A.C.S. Music therapy intervention in cardiac autonomic modulation, anxiety, and depression in mothers of preterms: Randomized controlled trial. BMC Psychol. 2018, 6, 57. [Google Scholar] [CrossRef]
- Schlez, A.; Litmanovitz, I.; Bauer, S.; Dolfin, T.; Regev, R.; Arnon, S. Combining Kangaroo Care and Live Harp Music Therapy in the Neonatal Intensive Care Unit Setting. IMAJ 2011, 13, 354–358. [Google Scholar]
- Roa, E.; Ettenberger, M. Music Therapy Self-Care Group for Parents of Preterm Infants in the Neonatal Intensive Care Unit: A Clinical Pilot Intervention. Medicines 2018, 5, 134. [Google Scholar] [CrossRef] [Green Version]
- Menke, B.M.; Hass, J.; Diener, C.; Poschl, J. Family-centered music therapy—Empowering premature infants and their primary caregivers through music: Results of a pilot study. PLoS ONE 2021, 16, e0250071. [Google Scholar] [CrossRef]
- Garcia-Gonzalez, J.; Ventura-Miranda, M.I.; Requena-Mullor, M.; Parron-Carreño, T.; Alarcon-Rodriguez, R. State-trait anxiety levels during pregnancy and foetal parameters following intervention with music therapy. J. Affect. Disord. 2018, 232, 17–22. [Google Scholar] [CrossRef]
- Van Willenswaard, K.C.; Lynn, F.; McNeill, J.; McQueen, K.; Dennis, C.L.; Lobel, M.; Alderdice, F. Music interventions to reduce stress and anxiety in pregnancy: A systematic review and meta-analysis. BMC Psychiatry 2017, 17, 271. [Google Scholar] [CrossRef] [Green Version]
- Prouhet, P.M.; Gregory, M.R.; Russell, C.L.; Yaeger, L.H. Fathers’ Stress in the Neonatal Intensive Care Unit. Adv. Neonatal Care 2018, 18, 105–120. [Google Scholar] [CrossRef]
- Labrie, N.H.M.; van Veenendaal, N.R.; Ludolph, R.A.; Ket, J.C.F.; van der Schoor, S.R.D.; van Kempen, A.A.M.W. Effects of parent-provider communication during infant hospitalization in the NICU on parents: A systematic review with meta-synthesis and narrative synthesis. Patient Educ. Couns. 2021, 104, 1526–1552. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | STRONG (N = 45) | LPMT Trial (N = 23) | |
|---|---|---|---|
| LPMT (n = 13) ^ | Waitlist (n = 10) ^ | ||
| Child characteristics | |||
| Gestational age in weeks | 27 (26–28) | 26 (25–28) | 26 (25–28) |
| Birth weight (grams) | 1000 (790–1248) | 900 (703–1045) | 810 (734–965) |
| Male sex | 22 (49) | 6 (46) | 3 (30) |
| Multiple birth | 9 (20) | 2 (15) & | 1 (10) |
| Apgar 5 min | 7.0 (6.0–8.0) | 6.0 (4.5–7.5) | 7.5 (5.8–9.0) |
| NICU admission (days) | 34.5 (24–45) | 39 (24–48) | 53 (37–72) |
| ACS, ≥1 dose | 38 (84) | 12 (92) | 10 (100) |
| Sectio caesarea | 23 (51) | 9 (69) | 5 (50) |
| Mechanical ventilation | 30 (67) | 9 (69) | 9 (90) |
| Inotropic agents | 5 (11) | 3 (23) | 0 (0) |
| PDA, hemodynamically significant | 20 (44) | 3 (23) | 7 (70) * |
| NEC | 4 (9) | 4 (30) | 2 (20) |
| Surgical NEC | 2 (4) | 2 (15) | 1 (10) |
| Sepsis, culture proven | 16 (36) | 2 (15) | 3 (30) |
| IVH ≥ grade III | 6 (13) | 3 (23) | 0 (0) |
| PVL ≥ grade II | 1 (2) | 1 (8) | 0 (0) |
| Maternal history | |||
| First pregnancy | 27 (60) | 6 (46) | 6 (60) |
| Previously premature childbirth (<32 weeks of gestation) | 4 (9) | 3 (23) | 0 (0) |
| Social and/or psychological problems | 7 (16) | 0 (0) | 1 (10) # |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations All authors have read and agreed to the published version of the manuscript.. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kraft, K.E.; Jaschke, A.C.; Ravensbergen, A.-G.; Feenstra-Weelink, A.; van Goor, M.E.L.; de Kroon, M.L.A.; Reijneveld, S.A.; Bos, A.F.; van Dokkum, N.H. Maternal Anxiety, Infant Stress, and the Role of Live-Performed Music Therapy during NICU Stay in The Netherlands. Int. J. Environ. Res. Public Health 2021, 18, 7077. https://doi.org/10.3390/ijerph18137077
Kraft KE, Jaschke AC, Ravensbergen A-G, Feenstra-Weelink A, van Goor MEL, de Kroon MLA, Reijneveld SA, Bos AF, van Dokkum NH. Maternal Anxiety, Infant Stress, and the Role of Live-Performed Music Therapy during NICU Stay in The Netherlands. International Journal of Environmental Research and Public Health. 2021; 18(13):7077. https://doi.org/10.3390/ijerph18137077
Chicago/Turabian StyleKraft, Karianne E., Artur C. Jaschke, Anne-Greet Ravensbergen, Annet Feenstra-Weelink, Maud E. L. van Goor, Marlou L. A. de Kroon, Sijmen A. Reijneveld, Arend F. Bos, and Nienke H. van Dokkum. 2021. "Maternal Anxiety, Infant Stress, and the Role of Live-Performed Music Therapy during NICU Stay in The Netherlands" International Journal of Environmental Research and Public Health 18, no. 13: 7077. https://doi.org/10.3390/ijerph18137077
APA StyleKraft, K. E., Jaschke, A. C., Ravensbergen, A.-G., Feenstra-Weelink, A., van Goor, M. E. L., de Kroon, M. L. A., Reijneveld, S. A., Bos, A. F., & van Dokkum, N. H. (2021). Maternal Anxiety, Infant Stress, and the Role of Live-Performed Music Therapy during NICU Stay in The Netherlands. International Journal of Environmental Research and Public Health, 18(13), 7077. https://doi.org/10.3390/ijerph18137077