
Repurposing an EMG Biofeedback Device for Gait Rehabilitation: Development, Validity and Reliability

 ,
,
Abstract
1. Introduction
- 1-
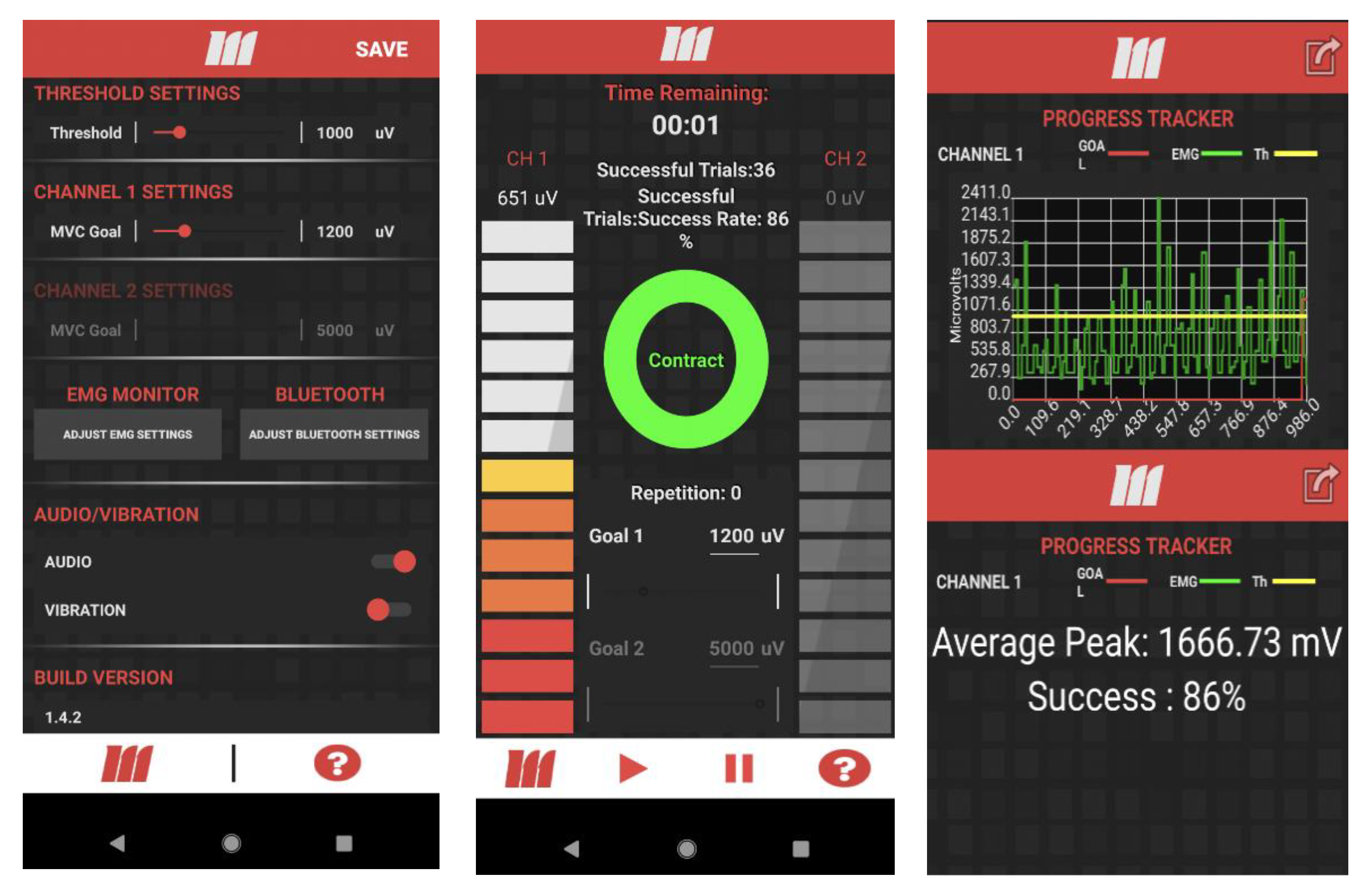
- Auditory and haptic feedback was added to the settings so that the participant would be able to select the mode of feedback when the activation goal is reached.
- 2-
- Success Rate was defined as the number of successful steps (where activation goal is met) divided by all steps (where the minimum threshold is met). The threshold can be defined in the settings of the app, but must be lower than the activation goal. The threshold was added to detect the muscle peaks that would correspond to a step that falls short of the activation goal. Success rate was added with motor learning in mind. This acts as both a measure of overall session performance and an outcome measure;
- 3-
- Calibration was added to detect and display the mean for peak muscle activity during the walking trial. This is beneficial in two ways: it can act as a normalization feature and can act as a baseline to set higher goals of activity for the muscle;
- 4-
- Cloud Upload was added with home and community training in mind. mTrigger signals from both channels are uploaded to Google Cloud and available for further investigation.
2. Materials and Methods
2.1. Repurposing mTrigger for Gait Rehabilitation
2.2. Validity and Reliability
2.3. Statistical Analyses
3. Results
3.1. Drift
3.2. Temporal Lag
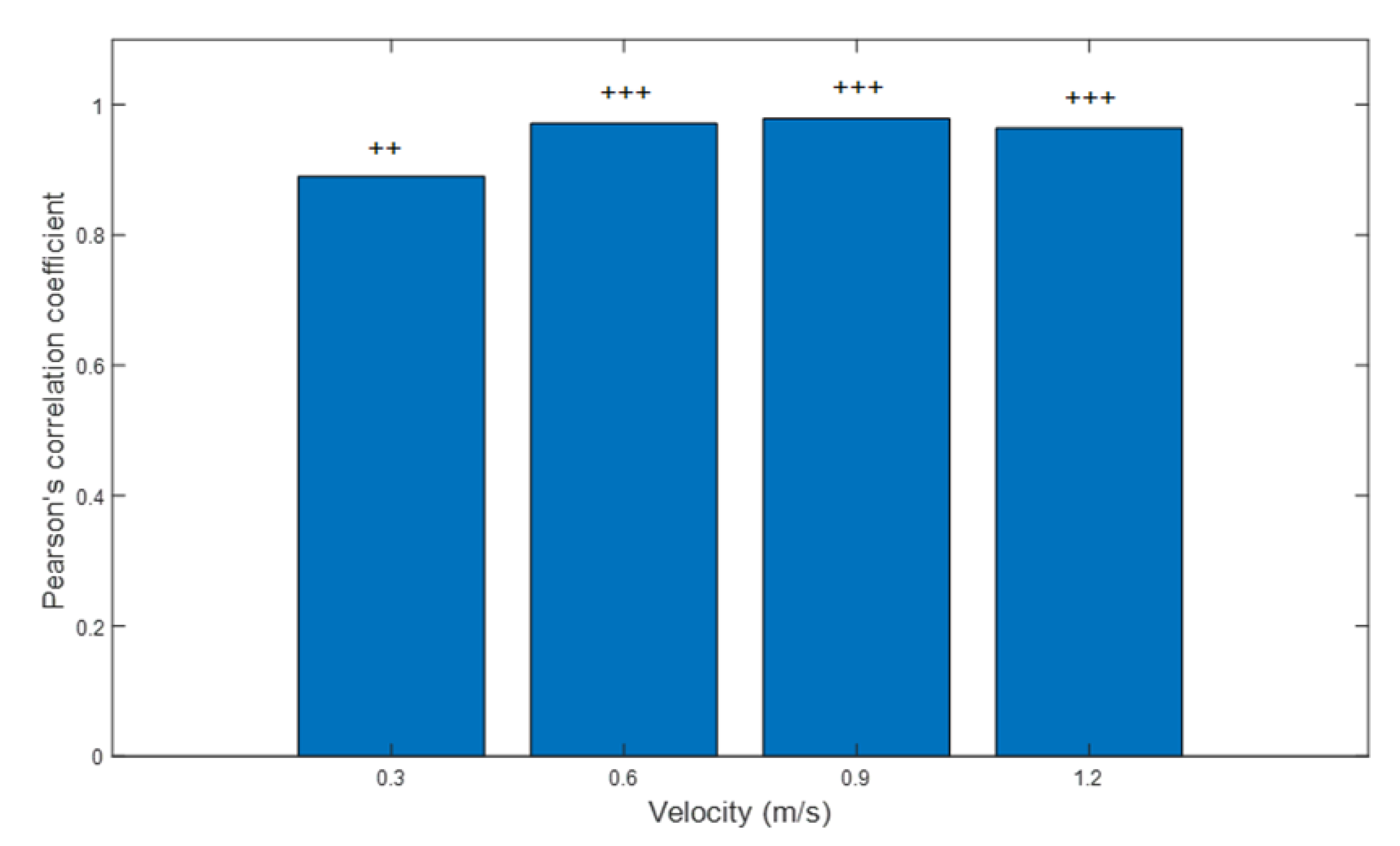
3.3. Validity: Treadmill Walking
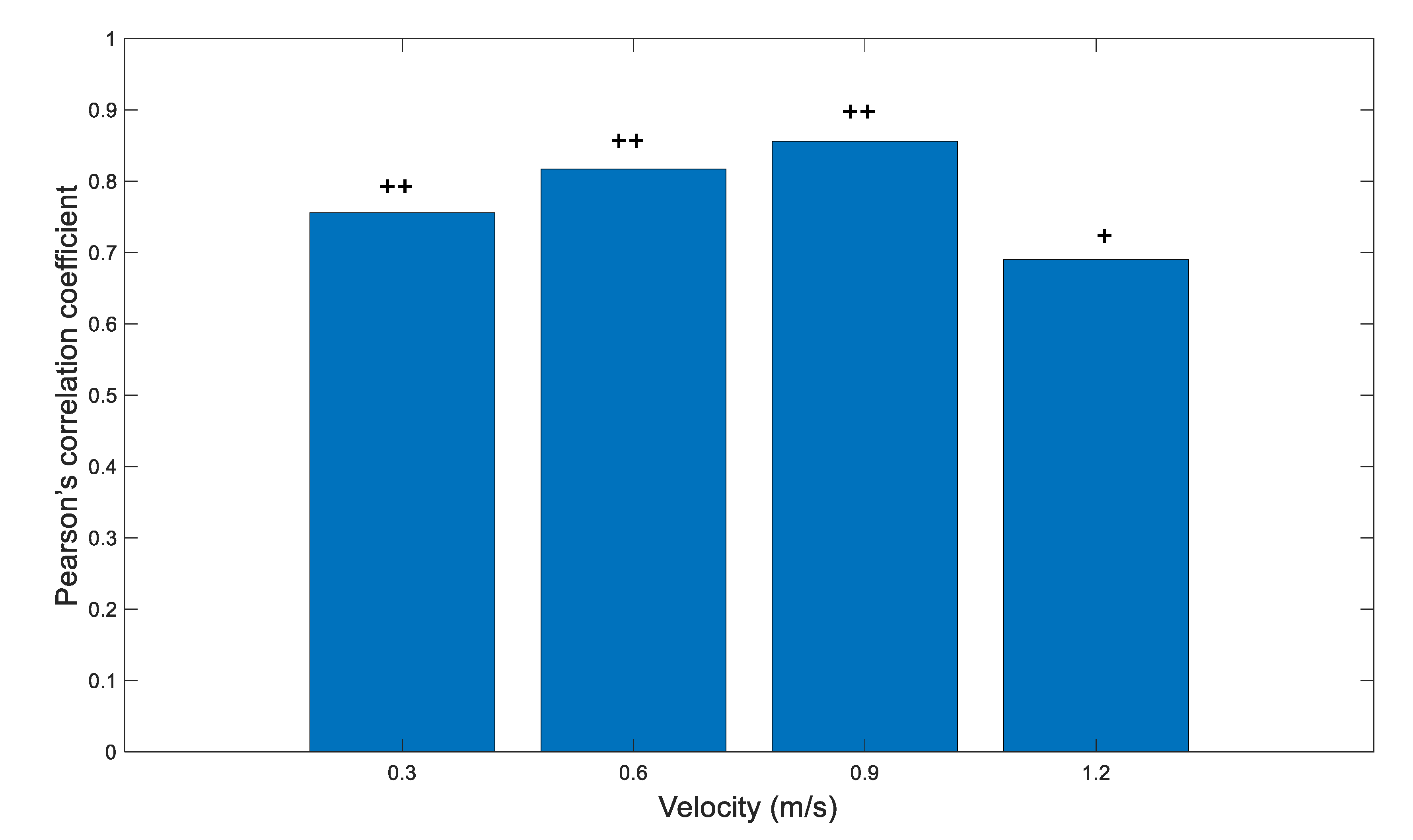
3.4. Validity: Overground Walking
3.5. Reliability: Treadmill Walking
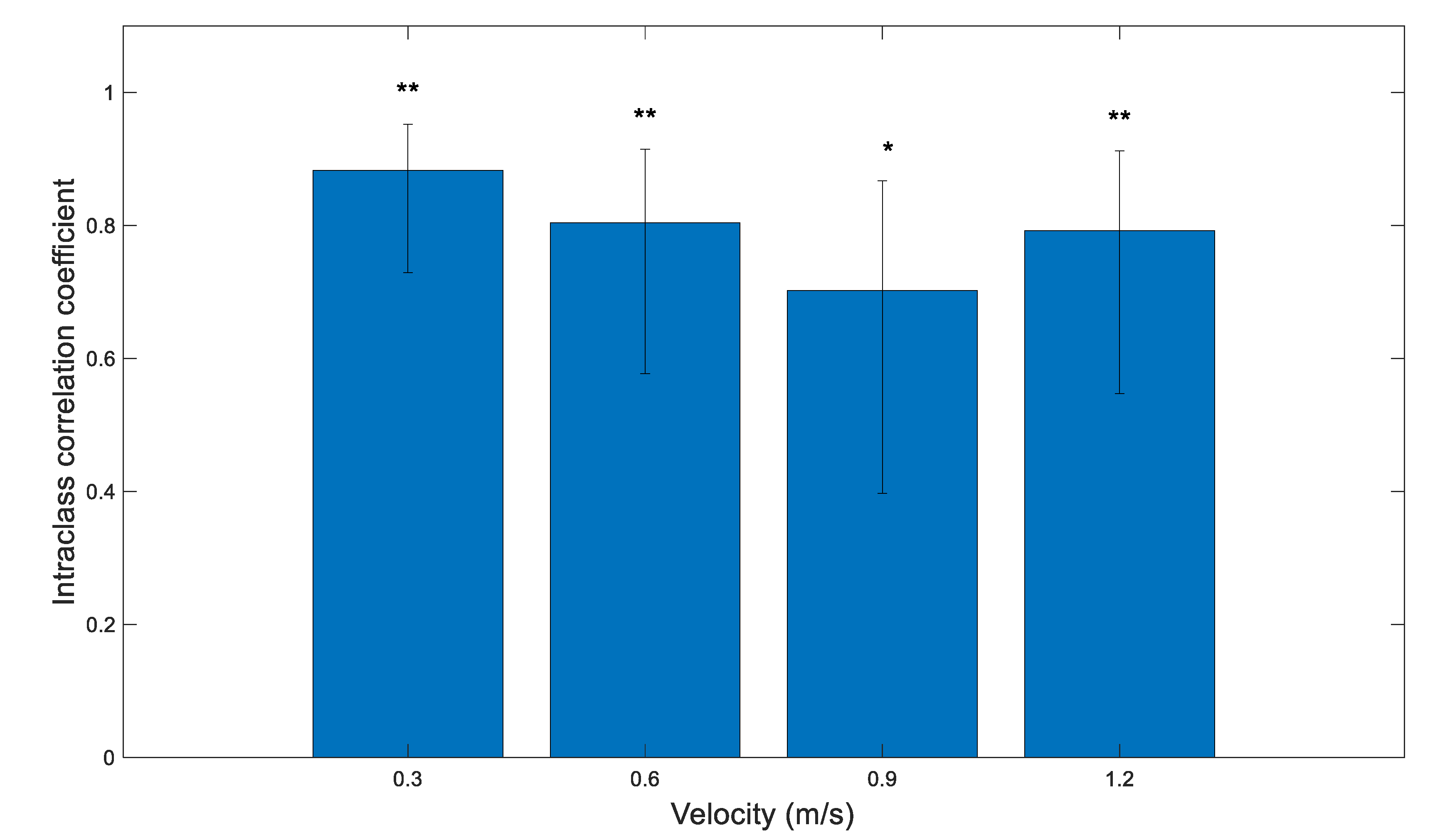
3.6. Reliability: Overground Walking
4. Discussion
5. Limitations
6. Conclusions and Future Directions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Giggins, O.M.; Persson, U.M.; Caulfield, B. Biofeedback in rehabilitation. J. Neuroeng. Rehabil. 2013, 10, 60. [Google Scholar] [CrossRef]
- Frank, D.L.; Khorshid, L.; Kiffer, J.F.; Moravec, C.S.; McKee, M.G. Biofeedback in medicine: Who, when, why and how? Ment. Health Fam. Med. 2010, 7, 85–91. [Google Scholar] [PubMed]
- Jonsdottir, J.; Cattaneo, D.; Recalcati, M.; Regola, A.; Rabuffetti, M.; Ferrarin, M.; Casiraghi, A. Task-Oriented Biofeedback to Improve Gait in Individuals with Chronic Stroke: Motor Learning Approach. Neurorehabilit. Neural Repair 2010, 24, 478–485. [Google Scholar] [CrossRef]
- Nash, J.; Neilson, P.D.; O’Dwyer, N.J. Reducing Spasticity to Control Muscle Contracture of Children with Cerebral Palsy. Dev. Med. Child Neurol. 2008, 31, 471–480. [Google Scholar] [CrossRef]
- Wright, Z.A.; Rymer, W.Z.; Slutzky, M.W. Reducing Abnormal Muscle Coactivation After Stroke Using a Myoelectric-Computer Interface: A Pilot Study. Neurorehabilit. Neural Repair 2013, 28, 443–451. [Google Scholar] [CrossRef]
- Draper, V.; Ballard, L. Electrical Stimulation Versus Electromyographic Biofeedback in the Recovery of Quadriceps Femoris Muscle Function Following Anterior Cruciate Ligament Surgery. Phys. Ther. 1991, 71, 455–461. [Google Scholar] [CrossRef]
- Kirnap, M.; Calis, M.; Turgut, A.O.; Halici, M.; Tuncel, M. The efficacy of EMG-biofeedback training on quadriceps muscle strength in patients after arthroscopic meniscectomy. N. Z. Med. J. 2005, 118, 1704. [Google Scholar]
- Yilmaz, O.O.; Şenocak, Ö.; Sahin, E.; Baydar, M.; Gulbahar, S.; Bircan, Ç.; Alper, S. Efficacy of EMG-biofeedback in knee osteoarthritis. Rheumatol. Int. 2009, 30, 887–892. [Google Scholar] [CrossRef]
- Ma, C.; Szeto, G.P.; Yan, T.; Wu, S.; Lin, C.; Li, L. Comparing Biofeedback with Active Exercise and Passive Treatment for the Management of Work-Related Neck and Shoulder Pain: A Randomized Controlled Trial. Arch. Phys. Med. Rehabil. 2011, 92, 849–858. [Google Scholar] [CrossRef]
- Bloom, R.; Przekop, A.; Sanger, T.D. Prolonged Electromyogram Biofeedback Improves Upper Extremity Function in Children with Cerebral Palsy. J. Child Neurol. 2010, 25, 1480–1484. [Google Scholar] [CrossRef]
- Franz, J.R.; Maletis, M.; Kram, R. Real-time feedback enhances forward propulsion during walking in old adults. Clin. Biomech. 2014, 29, 68–74. [Google Scholar] [CrossRef] [PubMed]
- Pietrosimone, B.; McLeod, M.M.; Florea, D.; Gribble, P.A.; Tevald, M.A. Immediate increases in quadriceps corticomotor excitability during an electromyography biofeedback intervention. J. Electromyogr. Kinesiol. 2015, 25, 316–322. [Google Scholar] [CrossRef] [PubMed]
- Vogt, A.P.; Boppana, A.; Bamberg, S.J.M. Using a pilot study to establish experimental methods for inexpensive instrumented insoles used in dynamic skiing analysis. In Proceedings of the 36th Annual International Conference of the IEEE Engineering in Medicine and Biology Society EMBC, Chicago, IL, USA, 26–30 August 2014; p. 84. [Google Scholar]
- Tate, J.J.; Milner, C. Real-Time Kinematic, Temporospatial, and Kinetic Biofeedback During Gait Retraining in Patients: A Systematic Review. Phys. Ther. 2010, 90, 1123–1134. [Google Scholar] [CrossRef] [PubMed]
- Stanton, R.; Ada, L.; Dean, C.M.; Preston, E. Biofeedback improves activities of the lower limb after stroke: A systematic review. J. Physiother. 2011, 57, 145–155. [Google Scholar] [CrossRef]
- Jonsdottir, J.; Cattaneo, D.; Regola, A.; Crippa, A.; Recalcati, M.; Rabuffetti, M.; Ferrarin, M.; Casiraghi, A. Concepts of Motor Learning Applied to a Rehabilitation Protocol Using Biofeedback to Improve Gait in a Chronic Stroke Patient: An A-B System Study with Multiple Gait Analyses. Neurorehabilit. Neural Repair 2007, 21, 190–194. [Google Scholar] [CrossRef]
- Tsaih, P.-L.; Chiu, M.-J.; Luh, J.-J.; Yang, Y.-R.; Lin, J.-J.; Hu, M.-H. Practice Variability Combined with Task-Oriented Electromyographic Biofeedback Enhances Strength and Balance in People with Chronic Stroke. Behav. Neurol. 2018, 2018, 1–9. [Google Scholar] [CrossRef]
- Najafi, Z.; Rezaeitalab, F.; Yaghubi, M.; Manzari, Z.S. The Effect of Biofeedback on the Motor– Muscular Situation in Rehabilitation of Stroke Patients. J. Caring Sci. 2018, 7, 89–93. [Google Scholar] [CrossRef][Green Version]
- Tamburella, F.; Moreno, J.C.; Valenzuela, D.S.H.; Pisotta, I.; Iosa, M.; Cincotti, F.; Mattia, D.; Pons, J.L.; Molinari, M. Influences of the biofeedback content on robotic post-stroke gait rehabilitation: Electromyographic vs. joint torque biofeedback. J. Neuroeng. Rehabil. 2019, 16, 95. [Google Scholar] [CrossRef]
- Aiello, E.; Gates, D.; Patritti, B.; Cairns, K.; Meister, M.; Clancy, E.; Bonato, P. Visual EMG Biofeedback to Improve Ankle Function in Hemiparetic Gait. In 27th Annual International Conference of the IEEE Engineering in Medicine and Biology Society—Inventation and Call for Papers, Proceedings of the IEEE Engineering in Medicine and Biology 27th Annual Conference, Shanghai, China, 1–4 September 2005; IEEE: Houghton, MI, USA, 2005; Volume 6, pp. 106–107. [Google Scholar] [CrossRef]
- Burnside, I.G.; Tobias, H.S.; Bursill, D. Electromyographic feedback in the remobilization of stroke patients: A controlled trial. Arch. Phys. Med. Rehabil. 1982, 63, 217–222. [Google Scholar]
- Colborne, G.; Olney, S.J.; Griffin, M.P. Feedback of ankle joint angle and soleus electromyography in the rehabilitation of hemiplegic gait. Arch. Phys. Med. Rehabil. 1993, 74, 1100–1106. [Google Scholar] [CrossRef]
- Wolf, S.L.; Binder-Macleod, S.A. Electromyographic Biofeedback Applications to the Hemiplegic Patient. Phys. Ther. 1983, 63, 1393–1403. [Google Scholar] [CrossRef] [PubMed]
- Spencer, J.; Wolf, S.L.; Kesar, T.M. Biofeedback for Post-stroke Gait Retraining: A Review of Current Evidence and Future Research Directions in the Context of Emerging Technologies. Front. Neurol. 2021, 12. [Google Scholar] [CrossRef] [PubMed]
- Aruin, A.S.; Hanke, T.A.; Sharma, A. Base of support feedback in gait rehabilitation. Int. J. Rehabil. Res. 2003, 26, 309–312. [Google Scholar] [CrossRef]
- Bradley, L.; Hart, B.B.; Mandana, S.; Flowers, K.; Riches, M.; Sanderson, P. Electromyographic biofeedback for gait training after stroke. Clin. Rehabil. 1998, 12, 11–22. [Google Scholar] [CrossRef]
- Chen, I.-C.; Cheng, P.-T.; Chen, C.-L.; Chen, S.-C.; Chung, C.-Y.; Yeh, T.-H. Effects of balance training on hemiplegic stroke patients. Chang. Gung Med. J. 2002, 25, 583–590. [Google Scholar] [PubMed]
- Cheng, P.-T.; Wu, S.-H.; Liaw, M.-Y.; Wong, A.M.; Tang, F.-T. Symmetrical body-weight distribution training in stroke patients and its effect on fall prevention. Arch. Phys. Med. Rehabil. 2001, 82, 1650–1654. [Google Scholar] [CrossRef] [PubMed]
- Engardt, M.; Ribbe, T.; Olsson, E. Vertical ground reaction force feedback to enhance stroke patients’ symmetrical body-weight distribution while rising/sitting down. Scand. J. Rehabil. Med. 1993, 25, 41–48. [Google Scholar]
- Eser, F.; Yavuzer, G.; Karakuş, D.; Karaoglan, B. The effect of balance training on motor recovery and ambulation after stroke: A randomized controlled trial. Eur. J. Phys. Rehabil. Med. 2008, 44, 19–25. [Google Scholar]
- Gok, H.; Geler-Kulcu, D.; Alptekin, N.; Dincer, G. Efficacy of treatment with a kinaesthetic ability training device on balance and mobility after stroke: A randomized controlled study. Clin. Rehabil. 2008, 22, 922–930. [Google Scholar] [CrossRef]
- Intiso, D.; Santilli, V.; Grasso, M.G.; Rossi, R.; Caruso, I. Rehabil. of walking with electromyographic biofeedback in foot-drop after stroke. Stroke 1994, 25, 1189–1192. [Google Scholar] [CrossRef]
- Kerdoncuff, V.; Duruflé, A.; Petrilli, S.; Nicolas, B.; Robineau, S.; Lassalle, A.; Le Tallec, H.; Ramanantsitonta, J.; Gallien, P. Intérêt de la rééducation par biofeedback visuel sur plateforme de stabilométrie dans la prise en charge des troubles posturaux des hémiplégiques vasculaires. Ann. Readapt. Méd. Phys. 2004, 47, 169–176. [Google Scholar] [CrossRef] [PubMed]
- Mandel, A.R.; Nymark, J.R.; Balmer, S.J.; Grinnell, D.M.; O’Riain, M.D. Electromyographic versus rhythmic positional biofeedback in computerized gait retraining with stroke patients. Arch. Phys. Med. Rehabil. 1990, 71, 649–654. [Google Scholar]
- Montoya, R.; Dupui, P.; Pagès, B.; Bessou, P. Step-length biofeedback device for walk Rehabilitation. Med Biol. Eng. Comput. 1994, 32, 416–420. [Google Scholar] [CrossRef] [PubMed]
- Morris, M.; Matyas, T.; Bach, T.M.; Goldie, P. Electrogoniometric feedback: Its effect on genu recurvatum in stroke. Arch. Phys. Med. Rehabil. 1992, 73, 1147–1154. [Google Scholar]
- Sackley, C.M.; Lincoln, N.B. Single blind randomized controlled trial of visual feedback after stroke: Effects on stance symmetry and function. Disabil. Rehabil. 1997, 19, 536–546. [Google Scholar] [CrossRef]
- Schauer, M.; Mauritz, K.-H. Musical motor feedback (MMF) in walking hemiparetic stroke patients: Randomized trials of gait improvement. Clin. Rehabil. 2003, 17, 713–722. [Google Scholar] [CrossRef] [PubMed]
- Campanini, I.; Disselhorst-Klug, C.; Rymer, W.Z.; Merletti, R. Surface EMG in Clinical Assessment and NeuroRehabilitation: Barriers Limiting Its Use. Front. Neurol. 2020, 11, 934. [Google Scholar] [CrossRef]
- Fini, N.; Holland, A.E.; Keating, J.; Simek, J.; Bernhardt, J. How Physically Active Are People Following Stroke? Systematic Review and Quantitative Synthesis. Phys. Ther. 2017, 97, 707–717. [Google Scholar] [CrossRef]
- Ovbiagele, B.; Goldstein, L.B.; Higashida, R.T.; Howard, V.J.; Johnston, S.C.; Khavjou, O.; Lackland, D.T.; Lichtman, J.H.; Mohl, S.; Sacco, R.L.; et al. Forecasting the Future of Stroke in the United States: A Policy Statement from the American Heart Association and American Stroke Association. Stroke 2013, 44, 2361–2375. [Google Scholar] [CrossRef]
- Yue, Z.; Zhang, X.; Wang, J. Hand Rehabilitation Robotics on Poststroke Motor Recovery. Behav. Neurol. 2017, 2017, 1–20. [Google Scholar] [CrossRef]
- Housley, S.N.; Garlow, A.R.; Ducote, K.; Howard, A.; Thomas, T.; Wu, D.; Richards, K.; Butler, A.J. Increasing Access to Cost Effective Home-Based Rehabil. for Rural Veteran Stroke Survivors. Austin J. Cerebrovasc. Dis. Stroke 2016, 3, 1–11. [Google Scholar] [PubMed]
- National Institute of Neurological Disorders and Stroke. Stroke Research Priorities Meeting 2012/2012. Available online: https://www.ninds.nih.gov/About-NINDS/Strategic-Plans-Evaluations/Strategic-Plans/Stroke-Research-Priorities-Meeting-2012 (accessed on 15 March 2019).
- Schmitz, A.; Silder, A.; Heiderscheit, B.; Mahoney, J.; Thelen, D.G. Differences in lower-extremity muscular activation during walking between healthy older and young adults. J. Electromyogr. Kinesiol. 2009, 19, 1085–1091. [Google Scholar] [CrossRef] [PubMed]
- Neptune, R.; Kautz, S.; Zajac, F. Contributions of the individual ankle plantar flexors to support, forward progression and swing initiation during walking. J. Biomech. 2001, 34, 1387–1398. [Google Scholar] [CrossRef]
- Perry, J.; Garrett, M.; Gronley, J.K.; Mulroy, S.J. Classification of Walking Handicap in the Stroke Population. Stroke 1995, 26, 982–989. [Google Scholar] [CrossRef]
- Tudor-Locke, C.; Aguiar, E.J.; Han, H.; Ducharme, S.W., Jr.; Barreira, T.V.; Moore, C.C.; Busa, M.A.; Lim, J.; Sirard, J.R.; Chipkin, S.R.; et al. Walking cadence (steps/min) and intensity in 21–40 year olds: Cadence-adults. Int. J. Behav. Nutr. Phys. Act. 2019, 16, 1–11. [Google Scholar] [CrossRef]
- Logan, D.; Kiemel, T.; Dominici, N.; Cappellini, G.; Ivanenko, Y.; Lacquaniti, F.; Jeka, J.J. The many roles of vision during walking. Exp. Brain Res. 2010, 206, 337–350. [Google Scholar] [CrossRef]
- De Luca, C.J. The Use of Surface Electromyography in Biomechanics. J. Appl. Biomech. 1997, 13, 135–163. [Google Scholar] [CrossRef]
- Halaki, M.; Gi, K. Normalization of EMG Signals: To Normalize or Not to Normalize and What to Normalize to? In Computational Intelligence in Electromyography Analysis—A Perspective on Current Applications and Future Challenges; BoD—Books on Demand: Norderstedt, Germany, 2012. [Google Scholar]
- Cram, J.R.; Rommen, D. Effects of skin preparation on data collected using an EMG muscle-scanning procedure. Appl. Psychophysiol. Biofeedback 1989, 14, 75–82. [Google Scholar] [CrossRef]
- Winkel, J. Significance of skin temperature changes in surface electromyography. Graefe’s Arch. Clin. Exp. Ophthalmol. 1991, 63, 345–348. [Google Scholar] [CrossRef]
- Talib, I.; Sundaraj, K.; Lam, C.K.; Hussain, J.; Ali, A. A review on crosstalk in myographic signals. Graefe’s Arch. Clin. Exp. Ophthalmol. 2019, 119, 9–28. [Google Scholar] [CrossRef]
- Chowdhury, R.H.; Reaz, M.B.I.; Ali, M.A.B.M.; Bakar, A.A.A.; Chellappan, K.; Chang, T.G. Surface Electromyography Signal Processing and Classification Techniques. Sensors 2013, 13, 12431–12466. [Google Scholar] [CrossRef] [PubMed]
- Cömert, A.; Hyttinen, J. Investigating the possible effect of electrode support structure on motion artifact in wearable bioelectric signal monitoring. Biomed. Eng. Online 2015, 14, 1–18. [Google Scholar] [CrossRef] [PubMed]
- van Brakel, J.P.G. Robust Peak Detection Algorithm Using Z-Scores; Stack Overflow: New York, NY, USA, 2014. [Google Scholar]
- Magill, R.A. Knowledge is More than We Can Talk about: Implicit Learning in Motor Skill Acquisition. Res. Q. Exerc. Sport 1998, 69, 104–110. [Google Scholar] [CrossRef]
- Sharma, D.; Chevidikunnan, M.F.; Khan, F.R.; Gaowgzeh, R.A. Effectiveness of knowledge of result and knowledge of performance in the learning of a skilled motor activity by healthy young adults. J. Phys. Ther. Sci. 2016, 28, 1482–1486. [Google Scholar] [CrossRef] [PubMed]
- Keogh, J.W.; Hume, P. Evidence for biomechanics and motor learning research improving golf performance. Sports Biomech. 2012, 11, 288–309. [Google Scholar] [CrossRef]
- Cirstea, C.; Ptito, A.; Levin, M. Feedback and Cognition in Arm Motor Skill Reacquisition After Stroke. Stroke 2006, 37, 1237–1242. [Google Scholar] [CrossRef]
- Van Vliet, P.M.; Wulf, G. Extrinsic feedback for motor learning after stroke: What is the evidence? Disabil. Rehabil. 2006, 28, 831–840. [Google Scholar] [CrossRef]
- ARIFIN, W.N. Sample Size Calculator. Available online: http://wnarifin.github.io (accessed on 20 May 2021).
- Koo, T.K.; Li, M.Y. A Guideline of Selecting and Reporting Intraclass Correlation Coefficients for Reliability Research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef]
- Mukaka, M.M. Statistics Corner: A Guide to Appropriate Use of Correlation Coefficient in Medical Research. Malawi Med. J. 2012, 24, 69–71. Available online: www.mmj.medcol.mw (accessed on 28 May 2021). [PubMed]
- Vogt, M.; Rips, A.; Emmelmann, C. Comparison of iPad Pro®’s LiDAR and TrueDepth Capabilities with an Industrial 3D Scanning Solution. Technologies 2021, 9, 25. [Google Scholar] [CrossRef]
- Gámez, A.B.; Morante, J.J.H.; Gil, J.L.M.; Esparza, F.; Martínez, C.M. The effect of surface electromyography biofeedback on the activity of extensor and dorsiflexor muscles in elderly adults: A randomized trial. Sci. Rep. 2019, 9, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Cumberland Consensus Working Group; Cheeran, B.; Cohen, L.; Dobkin, B.; Ford, G.; Greenwood, R.; Howard, D.; Husain, M.; MacLeod, M.; Nudo, R.; et al. The Future of Restorative Neurosciences in Stroke: Driving the Translational Research Pipeline from Basic Science to Rehabil. of People After Stroke. Neurorehabilit. Neural Repair 2008, 23, 97–107. [Google Scholar] [CrossRef]
- Stinear, C.; Ackerley, S.; Byblow, W. Rehabil. is Initiated Early After Stroke, but Most Motor Rehabil. Trials Are Not. Stroke 2013, 44, 2039–2045. [Google Scholar] [CrossRef]
- Guadagnoli, M.A.; Lee, T.D. Challenge Point: A Framework for Conceptualizing the Effects of Various Practice Conditions in Motor Learning. J. Mot. Behav. 2004, 36, 212–224. [Google Scholar] [CrossRef] [PubMed]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
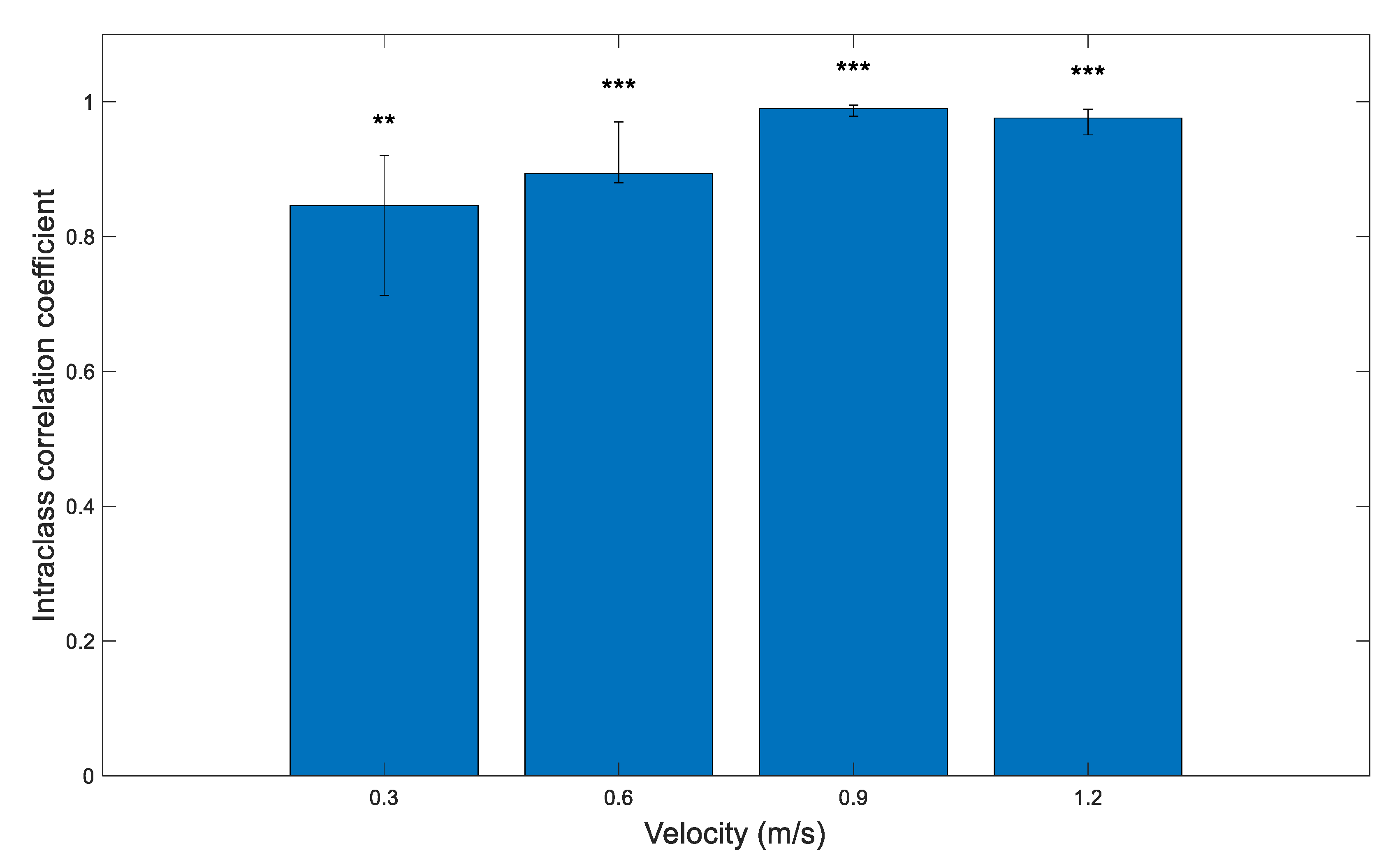
| Velocity(m/s) | ICC | Confidence Interval |
|---|---|---|
| 0.3 | 0.846 | n = 32, 95% CI (0.713–0.920) |
| 0.6 | 0.939 | n = 32, 95% CI (0.880–0.970) |
| 0.9 | 0.990 | n = 32, 95% CI (0.979–0.995) |
| 1.2 | 0.976 | n = 31, 95% CI (0.951–0.989) |
| Velocity (m/s) | ICC | Confidence Interval |
|---|---|---|
| 0.3 | 0.883 | n = 21, 95% CI (0.729–0.952) |
| 0.6 | 0.804 | n = 21, 95% CI (0.577–0.915) |
| 0.9 | 0.702 | n = 21, 95% CI (0.397–0.867) |
| 1.2 | 0.792 | n = 20, 95% CI (0.547–0.912) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Koiler, R.; Bakhshipour, E.; Glutting, J.; Lalime, A.; Kofa, D.; Getchell, N. Repurposing an EMG Biofeedback Device for Gait Rehabilitation: Development, Validity and Reliability. Int. J. Environ. Res. Public Health 2021, 18, 6460. https://doi.org/10.3390/ijerph18126460
Koiler R, Bakhshipour E, Glutting J, Lalime A, Kofa D, Getchell N. Repurposing an EMG Biofeedback Device for Gait Rehabilitation: Development, Validity and Reliability. International Journal of Environmental Research and Public Health. 2021; 18(12):6460. https://doi.org/10.3390/ijerph18126460
Chicago/Turabian StyleKoiler, Reza, Elham Bakhshipour, Joseph Glutting, Amy Lalime, Dexter Kofa, and Nancy Getchell. 2021. "Repurposing an EMG Biofeedback Device for Gait Rehabilitation: Development, Validity and Reliability" International Journal of Environmental Research and Public Health 18, no. 12: 6460. https://doi.org/10.3390/ijerph18126460
APA StyleKoiler, R., Bakhshipour, E., Glutting, J., Lalime, A., Kofa, D., & Getchell, N. (2021). Repurposing an EMG Biofeedback Device for Gait Rehabilitation: Development, Validity and Reliability. International Journal of Environmental Research and Public Health, 18(12), 6460. https://doi.org/10.3390/ijerph18126460