
Resilience as a Protective Factor in Basic Military Training, a Longitudinal Study of the Swiss Armed Forces

 ,
, 
Abstract
1. Introduction
2. Methods
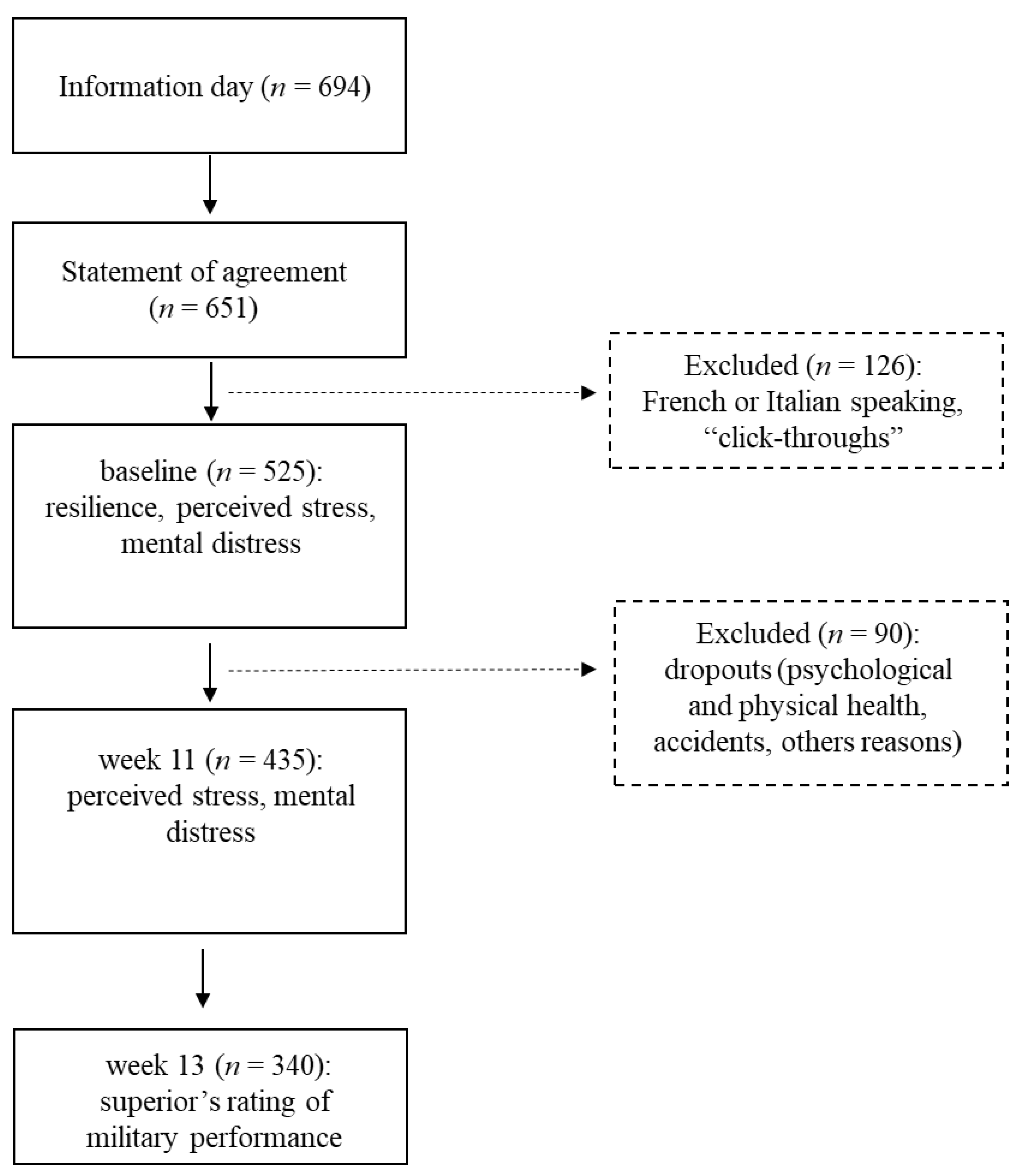
2.1. Procedure and Study Design
2.2. Participants
2.3. Measures
2.3.1. Demographic Information
2.3.2. Resilience
2.3.3. Perceived Stress
2.3.4. Mental Distress
2.3.5. Military Performance
2.3.6. Dropouts
2.4. Statistical Analysis
3. Results
3.1. Sample Characteristics
3.2. Resilience, Perceived Stress and Mental Distress at Baseline and at Week 11, and Military Performance at Week 13
3.3. Resilience at Baseline as Predictor of Perceived Stress and Mental Distress at Week 11 and Military Performance at Week 13
3.4. Perceived Stress at Week 11
3.5. Mental Distress at Week 11
3.6. Military Performance at Week 13
3.7. Resilience, Perceived stress and Mental Distress at Baseline among Recruits Continuing Their Military Duty and Dropouts
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- The American Institute of Stress. Workplace Stress Weatherford (TX). Available online: https://www.stress.org/workplace-stress/ (accessed on 1 January 2021).
- Cox, T.; Griffiths, A.; Rial-Gonzalez, E. Work-Related Stress; Office for Official Publications of the European Communities: Luxembourg, 2000. [Google Scholar]
- Glise, K.; Wiegner, L.; Jonsdottir, I.H. Long-term follow-up of residual symptoms in patients treated for stress-related exhaustion. BMC Psychol. 2020, 8, 26. [Google Scholar] [CrossRef] [PubMed]
- Robb, G.; Sultana, S.; Ameratunga, S.; Jackson, R. A systematic review of epidemiological studies investigating risk factors for work-related road traffic crashes and injuries. Inj. Prev. 2008, 14, 51–58. [Google Scholar] [CrossRef]
- Russo, M.; Lucifora, C.; Pucciarelli, F.; Piccoli, B. Work hazards and workers’ mental health: An investigation based on the fifth European Working Conditions Survey. Med. Lav. 2019, 110, 115–129. [Google Scholar] [CrossRef] [PubMed]
- Adriaenssens, J.; De Gucht, V.; Maes, S. Causes and consequences of occupational stress in emergency nurses, a longitudinal study. J. Nurs. Manag. 2015, 23, 346–358. [Google Scholar] [CrossRef]
- Gu, B.; Tan, Q.; Zhao, S. The association between occupational stress and psychosomatic wellbeing among Chinese nurses: A cross-sectional survey. Medicine 2019, 98, e15836. [Google Scholar] [CrossRef]
- Cruz, S.P.; Cruz, J.C.; Cabrera, J.H.; Abellán, M.V. Factors related to the probability of suffering mental health problems in emergency care professionals. Rev. Lat. Am. Enferm. 2019, 27, e3144. [Google Scholar] [CrossRef] [PubMed]
- Lang, U. Resilienz-Resilience; Kohlhammer: Stuttgart, Germany, 2019. [Google Scholar]
- Masten, A.S.; Cicchetti, D. Risk and resilience in development and psychopathology: The legacy of Norman Garmezy. Dev. Psychopathol. 2012, 24, 333–334. [Google Scholar] [CrossRef]
- Masten, A.S.; Tellegen, A. Resilience in developmental psychopathology: Contributions of the Project Competence Longitudinal Study. Dev. Psychopathol. 2012, 24, 345–361. [Google Scholar] [CrossRef]
- Wheaton, B. Sampling the Stress Universe. In Stress and Mental Health: Contemporary Issues and Prospects for the Future; Avison, W.R., Gotlib, I.H., Eds.; Springer: Boston, MA, USA, 1994; pp. 77–114. [Google Scholar]
- Dhabhar, F.S. A hassle a day may keep the doctor away: Stress and the augmentation of immune function. Integr. Comp. Biol. 2002, 42, 556–564. [Google Scholar] [CrossRef]
- Lazarus, R.S.; Folkman, S. Stress, Appraisal, and Coping; Springer: New York, NY, USA, 1984. [Google Scholar]
- Holmes, T.H.; Rahe, R.H. The Social Readjustment Rating Scale. J. Psychosom. Res. 1967, 11, 213–218. [Google Scholar] [CrossRef]
- Adamsson, A.; Bernhardsson, S. Symptoms that may be stress-related and lead to exhaustion disorder: A retrospective medical chart review in Swedish primary care. BMC Fam. Pract. 2018, 19, 172. [Google Scholar] [CrossRef] [PubMed]
- Cartwright, S.; Cooper, C.L. Public policy and occupational health psychology in Europe. J. Occup. Health Psychol. 1996, 1, 349–361. [Google Scholar] [CrossRef] [PubMed]
- Nakkas, C.; Annen, H.; Brand, S. Psychological distress and coping in military cadre candidates. Neuropsychiatr. Dis. Treat. 2016, 12, 2237–2243. [Google Scholar] [CrossRef] [PubMed]
- Nakkas, C.; Annen, H.; Brand, S. Somatization and Coping in Ethnic Minority Recruits. Mil. Med. 2019, 184, e680–e685. [Google Scholar] [CrossRef]
- Crum-Cianflone, N.F.; Powell, T.M.; LeardMann, C.A.; Russell, D.W.; Boyko, E.J. Mental Health and Comorbidities in U.S. Military Members. Mil. Med. 2016, 181, 537–545. [Google Scholar] [CrossRef]
- Hoge, C.W.; Castro, C.A.; Messer, S.C.; McGurk, D.; Cotting, D.I.; Koffman, R.L. Combat duty in Iraq and Afghanistan, mental health problems, and barriers to care. N. Engl. J. Med. 2004, 351, 13–22. [Google Scholar] [CrossRef]
- Thomas, J.L.; Wilk, J.E.; Riviere, L.A.; McGurk, D.; Castro, C.A.; Hoge, C.W. Prevalence of mental health problems and functional impairment among active component and National Guard soldiers 3 and 12 months following combat in Iraq. Arch. Gen. Psychiatry 2010, 67, 614–623. [Google Scholar] [CrossRef]
- Gallaway, M.S.; Fink, D.S.; Millikan, A.M.; Mitchell, M.M.; Bell, M.R. The association between combat exposure and negative behavioral and psychiatric conditions. J. Nerv. Ment. Dis. 2013, 201, 572–578. [Google Scholar] [CrossRef] [PubMed]
- LeardMann, C.A.; Smith, T.C.; Smith, B.; Wells, T.S.; Ryan, M.A. Baseline self reported functional health and vulnerability to post-traumatic stress disorder after combat deployment: Prospective US military cohort study. BMJ 2009, 338, b1273. [Google Scholar] [CrossRef]
- Riviere, L.A.; Kendall-Robbins, A.; McGurk, D.; Castro, C.A.; Hoge, C.W. Coming home may hurt: Risk factors for mental ill health in US reservists after deployment in Iraq. Br. J. Psychiatry J. Ment. Sci. 2011, 198, 136–142. [Google Scholar] [CrossRef]
- Bryan, C.J.; Hernandez, A.M.; Allison, S.; Clemans, T. Combat exposure and suicide risk in two samples of military personnel. J. Clin. Psychol. 2013, 69, 64–77. [Google Scholar] [CrossRef]
- Kessler, R.C.; Heeringa, S.G.; Stein, M.B.; Colpe, L.J.; Fullerton, C.S.; Hwang, I.; Naifeh, J.A.; Nock, M.K.; Petukhova, M.; Sampson, N.A.; et al. Thirty-day prevalence of DSM-IV mental disorders among nondeployed soldiers in the US Army: Results from the Army Study to Assess Risk and Resilience in Servicemembers (Army STARRS). JAMA Psychiatry 2014, 71, 504–513. [Google Scholar] [CrossRef] [PubMed]
- Boesch, M.; Sefidan, S.; Ehlert, U.; Annen, H.; Wyss, T.; Steptoe, A.; La Marca, R. Mood and autonomic responses to repeated exposure to the Trier Social Stress Test for Groups (TSST-G). Psychoneuroendocrinology 2014, 43, 41–51. [Google Scholar] [CrossRef] [PubMed]
- Waaktaar, T.; Torgersen, S. How resilient are resilience scales? The Big Five scales outperform resilience scales in predicting adjustment in adolescents. Scand. J. Psychol. 2010, 51, 157–163. [Google Scholar] [CrossRef] [PubMed]
- Annen, H. Resilience-An overview. Mil. Power Rev. Swiss Armed Forces 2017, 1, 24–35. [Google Scholar]
- Masten, A.S. Regulatory processes, risk, and resilience in adolescent development. Ann. N. Y. Acad. Sci. 2004, 1021, 310–319. [Google Scholar] [CrossRef]
- Masten, A.S.; Best, K.M.; Garmezy, N. Resilience and development: Contributions from the study of children who overcome adversity. Dev. Psychopathol. 1990, 2, 425–444. [Google Scholar] [CrossRef]
- Masten, A.S.; Burt, K.B.; Roisman, G.I.; Obradovic, J.; Long, J.D.; Tellegen, A. Resources and resilience in the transition to adulthood: Continuity and change. Dev. Psychopathol. 2004, 16, 1071–1094. [Google Scholar] [CrossRef]
- Masten, A.S.; Hubbard, J.J.; Gest, S.D.; Tellegen, A.; Garmezy, N.; Ramirez, M. Competence in the context of adversity: Pathways to resilience and maladaptation from childhood to late adolescence. Dev. Psychopathol. 1999, 11, 143–169. [Google Scholar] [CrossRef]
- Masten, A.S.; O’Connor, M.J. Vulnerability, stress, and resilience in the early development of a high risk child. J. Am. Acad. Child Adolesc. Psychiatry 1989, 28, 274–278. [Google Scholar] [CrossRef]
- Ridings, L.E.; Anton, M.T.; Winkelmann, J.; Davidson, T.M.; Wray, L.; Streck, C.J.; Ruggiero, K.J. Trauma Resilience and Recovery Program: Addressing Mental Health in Pediatric Trauma Centers. J. Pediatr. Psychol. 2019, 44, 1046–1056. [Google Scholar] [CrossRef] [PubMed]
- Galatzer-Levy, I.R.; Huang, S.H.; Bonanno, G.A. Trajectories of resilience and dysfunction following potential trauma: A review and statistical evaluation. Clin. Psychol. Rev. 2018, 63, 41–55. [Google Scholar] [CrossRef] [PubMed]
- Resnick, B.A.; Inguito, P.L. The Resilience Scale: Psychometric properties and clinical applicability in older adults. Arch. Psychiatr. Nurs. 2011, 25, 11–20. [Google Scholar] [CrossRef] [PubMed]
- Kermott, C.A.; Johnson, R.E.; Sood, R.; Jenkins, S.M.; Sood, A. Is higher resilience predictive of lower stress and better mental health among corporate executives? PLoS ONE 2019, 14, e0218092. [Google Scholar] [CrossRef] [PubMed]
- Herrmann, D.; Scherg, H.; Verres, R.; von Hagens, C.; Strowitzki, T.; Wischmann, T. Resilience in infertile couples acts as a protective factor against infertility-specific distress and impaired quality of life. J. Assist. Reprod. Genet. 2011, 28, 1111–1117. [Google Scholar] [CrossRef] [PubMed]
- Leak, R.K.; Calabrese, E.J.; Kozumbo, W.J.; Gidday, J.M.; Johnson, T.E.; Mitchell, J.R.; Ozaki, C.K.; Wetzker, R.; Bast, A.; Belz, R.G.; et al. Enhancing and Extending Biological Performance and Resilience. Dose Response 2018, 16, 1559325818784501. [Google Scholar] [CrossRef] [PubMed]
- Mjelde, F.V.; Smith, K.; Lunde, P.; Espevik, R. Military teams—A demand for resilience. Work 2016, 54, 283–294. [Google Scholar] [CrossRef]
- Nindl, B.C.; Billing, D.C.; Drain, J.R.; Beckner, M.E.; Greeves, J.; Groeller, H.; Teien, H.K.; Marcora, S.; Moffitt, A.; Reilly, T.; et al. Perspectives on resilience for military readiness and preparedness: Report of an international military physiology roundtable. J. Sci. Med. Sport 2018, 21, 1116–1124. [Google Scholar] [CrossRef]
- Campbell-Sills, L.; Cohan, S.L.; Stein, M.B. Relationship of resilience to personality, coping, and psychiatric symptoms in young adults. Behav. Res. Ther. 2006, 44, 585–599. [Google Scholar] [CrossRef]
- Zurita-Ortega, F.; Chacón-Cuberos, R.; Cofre-Bolados, C.; Knox, E.; Muros, J.J. Relationship of resilience, anxiety and injuries in footballers: Structural equations analysis. PLoS ONE 2018, 13, e0207860. [Google Scholar] [CrossRef]
- Charney, D.S. Psychobiological mechanisms of resilience and vulnerability: Implications for successful adaptation to extreme stress. Am. J. Psychiatry 2004, 161, 195–216. [Google Scholar] [CrossRef] [PubMed]
- Crum, A.J.; Akinola, M.; Martin, A.; Fath, S. The role of stress mindset in shaping cognitive, emotional, and physiological responses to challenging and threatening stress. Anxiety Stress Coping 2017, 30, 379–395. [Google Scholar] [CrossRef]
- Wagnild, G.M.; Young, H.M. Development and psychometric evaluation of the Resilience Scale. J. Nurs. Meas. 1993, 1, 165–178. [Google Scholar]
- Yang, C.; Zhou, Y.; Cao, Q.; Xia, M.; An, J. The Relationship Between Self-Control and Self-Efficacy Among Patients With Substance Use Disorders: Resilience and Self-Esteem as Mediators. Front. Psychiatry 2019, 10, 388. [Google Scholar] [CrossRef] [PubMed]
- Torabizadeh, C.; Asadabadi Poor, Z.; Shaygan, M. The Effects of Resilience Training on the Self-Efficacy of Patients with Type 2 Diabetes: A Randomized Controlled Clinical Trial. Int. J. Community Based Nurs. Midwifery 2019, 7, 211–221. [Google Scholar] [CrossRef]
- Eisen, S.V.; Schultz, M.R.; Glickman, M.E.; Vogt, D.; Martin, J.A.; Osei-Bonsu, P.E.; Drainoni, M.L.; Elwy, A.R. Postdeployment resilience as a predictor of mental health in operation enduring freedom/operation iraqi freedom returnees. Am. J. Prev. Med. 2014, 47, 754–761. [Google Scholar] [CrossRef]
- Kobasa, S.C.; Maddi, S.R.; Kahn, S. Hardiness and health: A prospective study. J. Pers. Soc. Psychol. 1982, 42, 168–177. [Google Scholar] [CrossRef]
- Bartone, P.T.; Johnsen, B.H.; Eid, J.; Hystad, S.W.; Laberg, J.C. Hardiness, avoidance coping, and alcohol consumption in war veterans: A moderated-mediation study. Stress Health 2017, 33, 498–507. [Google Scholar] [CrossRef] [PubMed]
- Gayton, S.D.; Kehoe, E.J. Character Strengths and Hardiness of Australian Army Special Forces Applicants. Mil. Med. 2015, 180, 857–862. [Google Scholar] [CrossRef][Green Version]
- Bartone, P.T.; Bowles, S.V. Coping with recruiter stress: Hardiness, performance and well-being in US Army recruiters. Mil. Psychol. 2020, 32, 390–397. [Google Scholar] [CrossRef]
- Bartone, P.T.; Hystad, S.W.; Eid, J.; Brevik, J.I. Psychological hardiness and coping style as risk/resilience factors for alcohol abuse. Mil. Med. 2012, 177, 517–524. [Google Scholar] [CrossRef]
- Bonanno, G.A. Loss, Trauma, and Human Resilience: Have We Underestimated the Human Capacity to Thrive After Extremely Aversive Events? Am. Psychol. 2004, 59, 20–28. [Google Scholar] [CrossRef]
- Bonanno, G.A.; Papa, A.; O’Neill, K. Loss and human resilience. Appl. Prev. Psychol. 2001, 10, 193–206. [Google Scholar] [CrossRef]
- Youssef, C.M.; Luthans, F. Positive organizational behavior in the workplace: The impact of hope, optimism, and resilience. J. Manag. 2007, 33, 774–800. [Google Scholar] [CrossRef]
- World Medical Association. World Medical Association Declaration of Helsinki: Ethical principles for medical research involving human subjects. Jama 2013, 310, 2191–2194. [Google Scholar] [CrossRef] [PubMed]
- Boesch, M.; Sefidan, S.; Annen, H.; Ehlert, U.; Roos, L.; Van Uum, S.; Russell, E.; Koren, G.; La Marca, R. Hair cortisol concentration is unaffected by basic military training, but related to sociodemographic and environmental factors. Stress 2015, 18, 35–41. [Google Scholar] [CrossRef] [PubMed]
- Walther, A.; Breidenstein, J.; Bösch, M.; Sefidan, S.; Ehlert, U.; Annen, H.; Wyss, T.; La Marca, R. Associations between digit ratio (2D4D), mood, and autonomic stress response in healthy men. Psychophysiology 2019, 56, e13328. [Google Scholar] [CrossRef]
- Wyss, T.; Boesch, M.; Roos, L.; Tschopp, C.; Frei, K.M.; Annen, H.; La Marca, R. Aerobic Fitness Level Affects Cardiovascular and Salivary Alpha Amylase Responses to Acute Psychosocial Stress. Sports Med. Open 2016, 2, 33. [Google Scholar] [CrossRef]
- Tuch, C.; Teubel, T.; La Marca, R.; Roos, L.; Annen, H.; Wyss, T. Physical fitness level affects perception of chronic stress in military trainees. Stress Health 2017, 33, 490–497. [Google Scholar] [CrossRef]
- Roos, L.; Boesch, M.; Sefidan, S.; Frey, F.; Mäder, U.; Annen, H.; Wyss, T. Adapted marching distances and physical training decrease recruits’ injuries and attrition. Mil. Med. 2015, 180, 329–336. [Google Scholar] [CrossRef]
- Schumacher, J.; Leppert, K.; Gunzelrnann, T.; Strauss, B.; Braehler, E. Die Resilienzskala-Ein Fragebogen zur Erfassung der psychischen Widerstandsf‰higkeit als Personmerkmal. Z. Klin. Psychol. Psychiatr. Psychother. 2005, 53, 16–39. [Google Scholar]
- Kocalevent, R.D.; Zenger, M.; Heinen, I.; Dwinger, S.; Decker, O.; Brähler, E. Resilience in the General Population: Standardization of the Resilience Scale (RS-11). PLoS ONE 2015, 10, e0140322. [Google Scholar] [CrossRef] [PubMed]
- Fliege, H.; Rose, M.; Arck, P.; Levenstein, S.; Klapp, B. Validierung des “Perceived StressQuestionnaire” (PSQ) an einer deutschenStichprobe. Diagnostica 2001, 47, 142–152. [Google Scholar] [CrossRef]
- Levenstein, S.; Prantera, C.; Varvo, V.; Scribano, M.L.; Berto, E.; Luzi, C.; Andreoli, A. Development of the Perceived Stress Questionnaire: A new tool for psychosomatic research. J. Psychosom. Res. 1993, 37, 19–32. [Google Scholar] [CrossRef]
- Franke, G.; Franke, G.H. Brief Symptom Inventory-Deutsche Version. Manual; Beltz: Göttingen, Germany, 2000. [Google Scholar]
- Derogatis, L.R. Symptom Checklist-90R (SCL-90-R); Pearson: Bloomington, MN, USA, 1994. [Google Scholar]
- Annen, H. Support-Oriented appraisal. Action research in the Swiss Armed Forces; Verlag Huber: Frauenfeld, Switzerland, 2000. [Google Scholar]
- Reivich, K.J.; Seligman, M.E.P.; McBride, S. Master resilience training in the U.S. Army. Am. Psychol. 2011, 66, 25–34. [Google Scholar] [CrossRef]
- Green, K.T.; Calhoun, P.S.; Dennis, M.F.; Beckham, J.C. Exploration of the resilience construct in posttraumatic stress disorder severity and functional correlates in military combat veterans who have served since September 11, 2001. J. Clin. Psychiatry 2010, 71, 823–830. [Google Scholar] [CrossRef]
- Pietrzak, R.H.; Southwick, S.M. Psychological resilience in OEF-OIF Veterans: Application of a novel classification approach and examination of demographic and psychosocial correlates. J. Affect. Disord. 2011, 133, 560–568. [Google Scholar] [CrossRef]
- Goldmann, E.; Calabrese, J.R.; Prescott, M.R.; Tamburrino, M.; Liberzon, I.; Slembarski, R.; Shirley, E.; Fine, T.; Goto, T.; Wilson, K.; et al. Potentially modifiable pre-, peri-, and postdeployment characteristics associated with deployment-related posttraumatic stress disorder among ohio army national guard soldiers. Ann. Epidemiol. 2012, 22, 71–78. [Google Scholar] [CrossRef]
- Crowell-Williamson, G.A.; Fruhbauerova, M.; DeCou, C.R.; Comtois, K.A. Perceived burdensomeness, bullying, and suicidal ideation in suicidal military personnel. J. Clin. Psychol. 2019, 75, 2147–2159. [Google Scholar] [CrossRef]
- Dragonetti, J.D.; Gifford, T.W.; Yang, M.S. The Process of Developing a Unit-Based Army Resilience Program. Curr. Psychiatry Rep. 2020, 22, 48. [Google Scholar] [CrossRef]
- Thabrew, H.; Fleming, T.; Hetrick, S.; Merry, S. Co-design of eHealth Interventions With Children and Young People. Front. Psychiatry 2018, 9, 481. [Google Scholar] [CrossRef] [PubMed]
- Thabrew, H.; Stasiak, K.; Hetrick, S.E.; Wong, S.; Huss, J.H.; Merry, S.N. E-Health interventions for anxiety and depression in children and adolescents with long-term physical conditions. Cochrane Database Syst. Rev. 2018, 8, Cd012489. [Google Scholar] [CrossRef] [PubMed]
- El Morr, C.; Ritvo, P.; Ahmad, F.; Moineddin, R. Effectiveness of an 8-Week Web-Based Mindfulness Virtual Community Intervention for University Students on Symptoms of Stress, Anxiety, and Depression: Randomized Controlled Trial. JMIR Ment. Health 2020, 7, e18595. [Google Scholar] [CrossRef] [PubMed]
- Soh, H.L.; Ho, R.C.; Ho, C.S.; Tam, W.W. Efficacy of digital cognitive behavioural therapy for insomnia: A meta-analysis of randomised controlled trials. Sleep Med. 2020, 75, 315–325. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variables | Timepoints | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Baseline | Week 11 | Week 13 | M | SD | ||||||
| Resilience | Perceived Stress | Mental Distress | Perceived Stress | Mental Distress | Military Performance | |||||
| Sample size (n) | 459 | 520 | 517 | 361 | 352 | 340 | ||||
| Baseline | ||||||||||
| Resilience | - | −0.38 ** | −0.27 ** | −0.28 ** | −0.24 ** | 0.15 * | 58.9 | 11.1 | ||
| Perceived stress | - | 0.55 ** | 0.41 ** | 0.12 * | −0.11 | 32.2 | 16.5 | |||
| Mental distress baseline | - | 0.33 ** | 0.24 ** | −0.05 | 0.47 | 0.45 | ||||
| Week 11 | ||||||||||
| Perceived stress | - | 0.30 ** | −0.11 | 41.5 | 14.4 | |||||
| Mental distress | - | 0.00 | 0.58 | 0.66 | ||||||
| Week 13 | ||||||||||
| Military performance | - | 2.82 | 0.46 | |||||||
| Perceived Stress (Week 11) | |||||
|---|---|---|---|---|---|
| Variables | B | SE B | β | R2 | ΔR2 |
| Step 1 | |||||
| Perceived stress (baseline) | 0.28 | 0.05 | 0.32 *** | 0.20 | 0.19 |
| Mental distress (baseline) | 6.70 | 2.04 | 0.20 ** | ||
| Step 2 | |||||
| Perceived stress (baseline) | 0.24 | 0.06 | 0.27 *** | 0.21 | 0.20 |
| Mental distress (baseline) | 6.26 | 2.03 | 0.18 ** | ||
| Resilience (baseline) | −0.16 | 0.08 | −0.12 * | ||
| Mental Distress (Week 11) | |||||
|---|---|---|---|---|---|
| Variables | B | SE B | β | R2 | ΔR2 |
| Step 1 | |||||
| Mental distress (baseline) | 0.41 | 0.10 | 0.26 *** | 0.07 | 0.07 |
| Perceived stress (baseline) | 0.00 | 0.00 | 0.01 | ||
| Step 2 | |||||
| Mental distress (baseline) | 0.38 | 0.10 | 0.24 *** | 0.10 | 0.09 |
| Perceived stress (baseline) | 0.00 | 0.00 | −0.06 | ||
| Resilience (baseline) | −0.01 | 0.00 | −0.19 ** | ||
| Military Performance (Week 13) | |||||
|---|---|---|---|---|---|
| Variables | B | SE B | β | R2 | ΔR2 |
| Step 1 | |||||
| Perceived stress (baseline) | 0.00 | 0.00 | −0.10 | 0.01 | 0.00 |
| Mental distress (baseline) | 0.02 | 0.08 | 0.02 | ||
| Step 2 | |||||
| Perceived stress (baseline) | 0.00 | 0.00 | −0.06 | 0.03 | 0.01 |
| Mental distress (baseline) | 0.02 | 0.08 | 0.02 | ||
| Resilience (baseline) | 0.01 | 0.00 | 0.13 * | ||
| Group | ||||
|---|---|---|---|---|
| Dropout: | Dropout Other Reasons: | Non-Dropouts | Group | |
| Mental Health | Physical Health, Accidents, Others | |||
| Degrees of freedom | 2 | |||
| N | 20 | 50 | 384 | |
| M (SD) | M (SD) | M (SD) | F partial eta2 | |
| Resilience (baseline) | 57.00 (11.24) | 55.54 (12.48) | 59.48 (10.87) | 3.13 * 0.01 [S] |
| Perceived stress (baseline) | 46.75 (22.74) | 35.97 (17.10) | 31.40 (15.80) | 9.64 *** 0.04 [S] |
| Mental distress (baseline) | 0.85 (0.71) | 0.58 (0.52) | 0.44 (0.41) | 9.48 *** 0.04 [S] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sefidan, S.; Pramstaller, M.; La Marca, R.; Wyss, T.; Sadeghi-Bahmani, D.; Annen, H.; Brand, S. Resilience as a Protective Factor in Basic Military Training, a Longitudinal Study of the Swiss Armed Forces. Int. J. Environ. Res. Public Health 2021, 18, 6077. https://doi.org/10.3390/ijerph18116077
Sefidan S, Pramstaller M, La Marca R, Wyss T, Sadeghi-Bahmani D, Annen H, Brand S. Resilience as a Protective Factor in Basic Military Training, a Longitudinal Study of the Swiss Armed Forces. International Journal of Environmental Research and Public Health. 2021; 18(11):6077. https://doi.org/10.3390/ijerph18116077
Chicago/Turabian StyleSefidan, Sandra, Maria Pramstaller, Roberto La Marca, Thomas Wyss, Dena Sadeghi-Bahmani, Hubert Annen, and Serge Brand. 2021. "Resilience as a Protective Factor in Basic Military Training, a Longitudinal Study of the Swiss Armed Forces" International Journal of Environmental Research and Public Health 18, no. 11: 6077. https://doi.org/10.3390/ijerph18116077
APA StyleSefidan, S., Pramstaller, M., La Marca, R., Wyss, T., Sadeghi-Bahmani, D., Annen, H., & Brand, S. (2021). Resilience as a Protective Factor in Basic Military Training, a Longitudinal Study of the Swiss Armed Forces. International Journal of Environmental Research and Public Health, 18(11), 6077. https://doi.org/10.3390/ijerph18116077