
Bioimpedance Vector Patterns according to Age and Handgrip Strength in Adolescent Male and Female Athletes

 ,
,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Subjects
2.2. Anthropometric and Body Composition Measurements
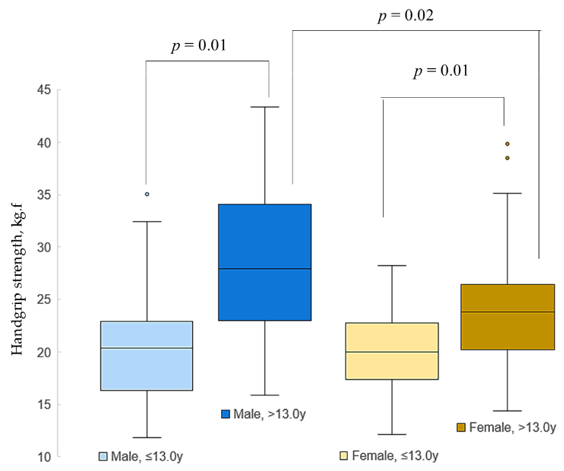
2.3. Handgrip Strength
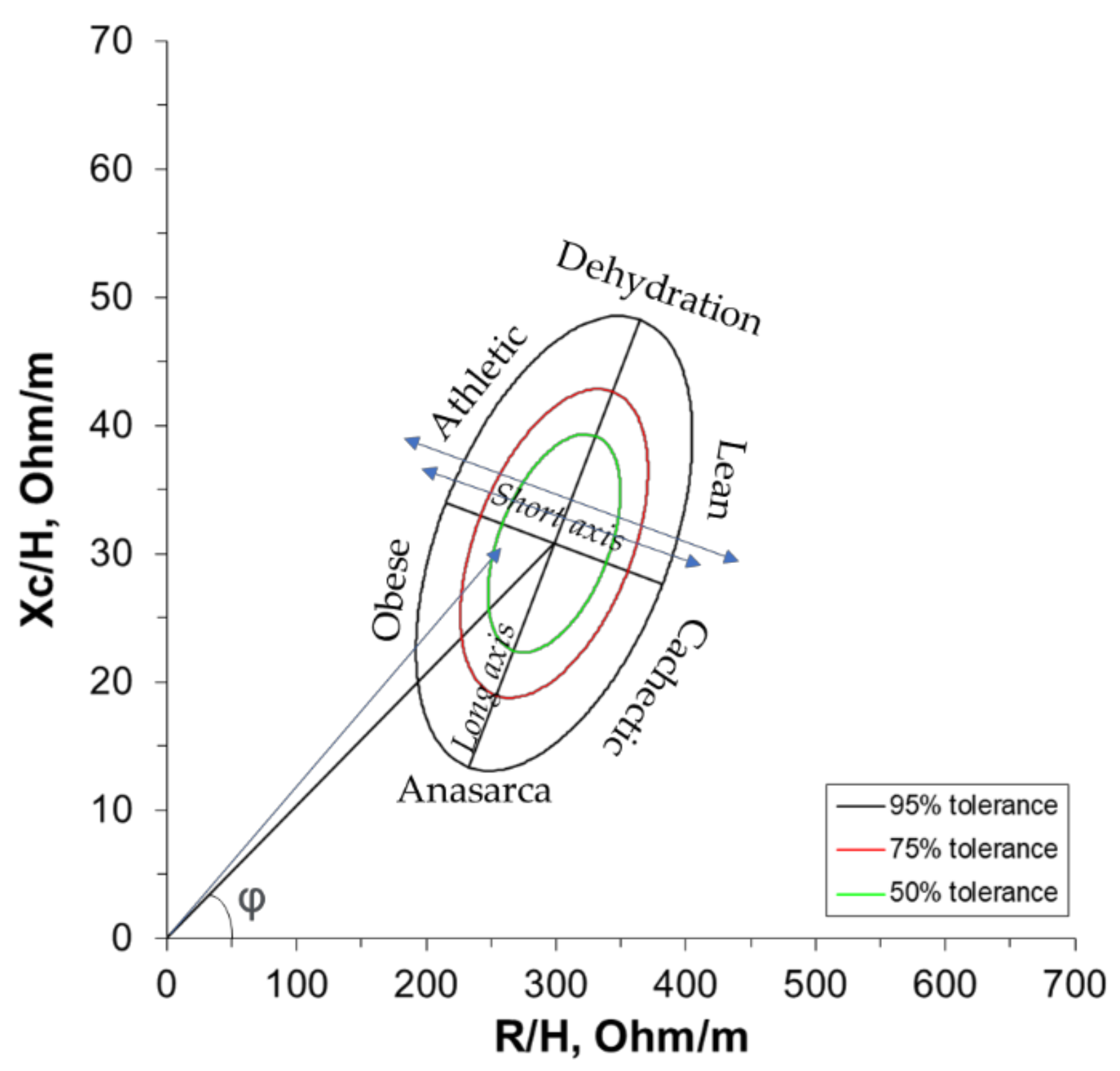
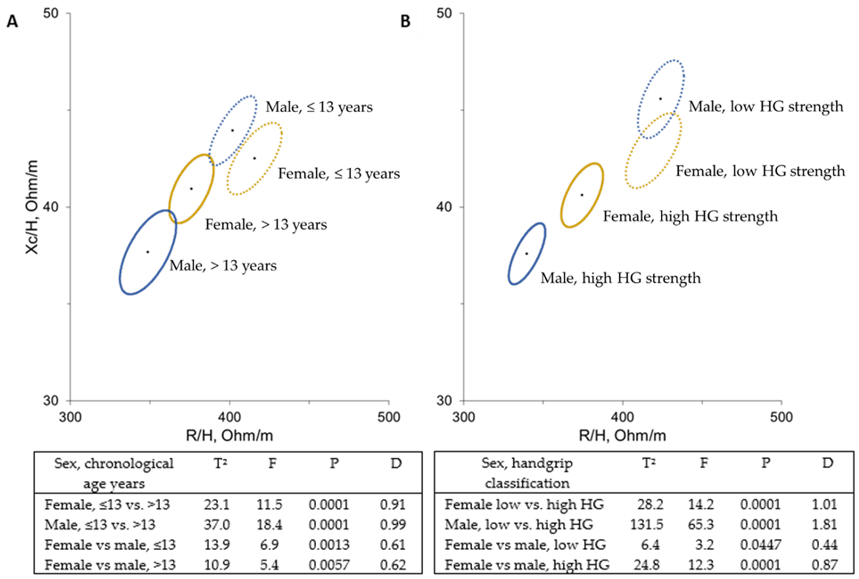
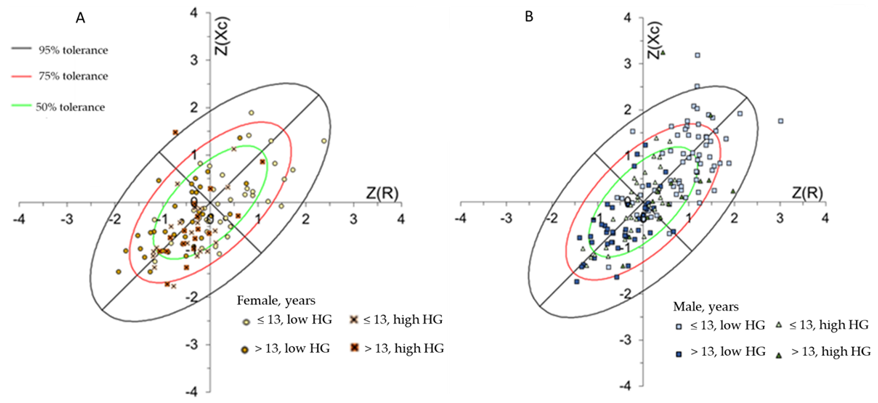
2.4. Bioelectrical Impedance Vector Analysis
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Rogol, A.D.; Clark, P.A.; Roemmich, J.N. Growth and pubertal development in children and adolescents: Effects of diet and physical activity. Am. J. Clin. Nutr. 2000, 72, 521S–528S. [Google Scholar] [CrossRef] [PubMed]
- Bielemann, R.M.; Domingues, M.R.; Horta, B.L.; Menezes, A.M.B.; Gonçalves, H.; Assunção, M.C.F.; Hallal, P.C. Physical activity throughout adolescence and bone mineral density in early adulthood: The 1993 Pelotas (Brazil) Birth Cohort Study. Osteoporos. Int. 2014, 25, 2007–2015. [Google Scholar] [CrossRef][Green Version]
- Jiménez-Pavón, D.; Fernández-Vázquez, A.; Alexy, U.; Pedrero, R.; Cuenca-García, M.; Polito, A.; Vanhelst, J.; Manios, Y.; Kafatos, A.; Molnar, D.; et al. Association of objectively measured physical activity with body components in European adolescents. BMC Public Health 2013, 13, 667–675. [Google Scholar] [CrossRef]
- Maughan, R.J.; Watson, J.S.; Weir, J. Strength and cross-sectional area of human skeletal muscle. J. Physiol. 1983, 338, 37–49. [Google Scholar] [CrossRef] [PubMed]
- Moliner-Urdiales, D.; Ortega, F.B.; Vicente-Rodriguez, G.; Rey-Lopez, J.P.; Gracia-Marco, L.; Widhalm, K.; Sjöström, M.; Moreno, L.A.; Castillo, M.J.; Ruiz, J.R. Association of physical activity with muscular strength and fat-free mass in adolescents: The HELENA study. Eur. J. Appl. Physiol. 2010, 109, 1119–1127. [Google Scholar] [CrossRef]
- Ubago-Guisado, E.; Vlachopoulos, D.; Ferreira de Moraes, A.C.; Torres-Costoso, A.; Wilkinson, K.; Metcalf, B.; Sánchez-Sánchez, J.; Gallardo, L.; Gracia-Marco, L. Lean mass explains the association between muscular fitness and bone outcomes in 13-year-old boys. Acta Paediatr. 2017, 106, 1658–1665. [Google Scholar] [CrossRef]
- Campa, F.; Semprini, G.; Júdice, P.; Messina, G.; Toselli, S. Anthropometry, Physical and Movement Features, and Repeated-sprint Ability in Soccer Players. Int. J. Sports Med. 2019, 40, 100–109. [Google Scholar] [CrossRef] [PubMed]
- Ortega, F.B.; Ruiz, J.R.; Castillo, M.J.; Sjöström, M. Physical fitness in childhood and adolescence: A powerful marker of health. Int. J. Obes. 2008, 32, 1–11. [Google Scholar] [CrossRef]
- Richards, L.; Palmiter-Thomas, P. Grip strength measurement: A critical review of tools, methods, and clinical utility. Crit. Rev. Phys. Rehabil. Med. 1996, 8, 87–109. [Google Scholar] [CrossRef]
- Silva, A.M. Structural and functional body components in athletic health and performance phenotypes. Eur. J. Clin. Nutr. 2019, 73, 215–224. [Google Scholar] [CrossRef]
- Gómez-Campos, R.; Andruske, C.L.; de Arruda, M.; Sulla-Torres, J.; Pacheco-Carrillo, J.; Urra-Albornoz, C.; Cossio-Bolaños, M. Normative data for handgrip strength in children and adolescents in the Maule Region, Chile: Evaluation based on chronological and biological age. PLoS ONE 2018, 13, e0201033. [Google Scholar] [CrossRef]
- Dugdale, J.H.; Arthur, C.A.; Sanders, D.; Hunter, A.M. Reliability and validity of field-based fitness tests in youth soccer players. Eur. J. Sport Sci. 2019, 19, 745–756. [Google Scholar] [CrossRef] [PubMed]
- Pizzigalli, L.; Cremasco, M.M.; La Torre, A.; Rainoldi, A.; Benis, R. Hand grip strength and anthropometric characteristics in Italian female national basketball teams. J. Sports Med. Phys. Fit. 2017, 57, 521–528. [Google Scholar] [CrossRef]
- Matias, C.N.; Santos, D.A.; Júdice, P.B.; Magalhães, J.P.; Minderico, C.S.; Fields, D.A.; Lukaski, H.C.; Sardinha, L.B.; Silva, A.M. Estimation of total body water and extracellular water with bioimpedance in athletes: A need for athlete-specific prediction models. Clin. Nutr. 2016, 35, 468–474. [Google Scholar] [CrossRef]
- Moon, J.R. Body composition in athletes and sports nutrition: An examination of the bioimpedance analysis technique. Eur. J. Clin. Nutr. 2013, 67, S54–S59. [Google Scholar] [CrossRef]
- Koury, J.C.; Ribeiro, M.A.; Massarani, F.A.; Vieira, F.; Marini, E. Fat-free mass in adolescent athletes: Accuracy of bioimpedance equations and identification of new predictive equations. Nutrition 2019, 60, 59–65. [Google Scholar] [CrossRef] [PubMed]
- Castizo-Olier, J.; Irurtia, A.; Jemni, M.; Carrasco-Marginet, M.; Fernández-García, R.; Rodríguez, F.A. Bioelectrical impedance vector analysis (BIVA) in sport and exercise: Systematic review and future perspectives. PLoS ONE 2018, 13, e0197957. [Google Scholar] [CrossRef]
- Marini, E.; Campa, F.; Buffa, R.; Stagi, S.; Matias, C.N.; Toselli, S.; Sardinha, L.B.; Silva, A.M. Phase angle and bioelectrical impedance vector analysis in the evaluation of body composition in athletes. Clin. Nutr. 2020, 39, 447–454. [Google Scholar] [CrossRef]
- Piccoli, A.; Rossi, B.; Pillon, L.; Bucciante, G. A new method for monitoring body fluid variation by bioimpedance analysis: The RXc graph. Kidney Int. 1994, 46, 534–539. [Google Scholar] [CrossRef]
- Baumgartner, R.N.; Chumlea, W.C.; Roche, A.F. Bioelectric impedance phase angle and body composition. Am. J. Clin. Nutr. 1988, 48, 16–23. [Google Scholar] [CrossRef] [PubMed]
- Kyle, U.G.; Bosaeus, I.; De Lorenzo, A.D.; Deurenberg, P.; Elia, M.; Gómez, J.M.; Heitmann, B.L.; Kent-Smith, L.; Melchior, J.C.; Pirlich, M.; et al. Bioelectrical impedance analysis—Part II: Utilization in clinical practice. Clin. Nutr. 2004, 23, 1430–1453. [Google Scholar] [CrossRef]
- Campa, F.; Matias, C.N.; Marini, E.; Heymsfield, S.B.; Toselli, S.; Sardinha, L.B.; Silva, A.M. Identifying Athlete Body Fluid Changes During a Competitive Season with Bioelectrical Impedance Vector Analysis. Int. J. Sports Physiol. Perform. 2020, 15, 361–367. [Google Scholar] [CrossRef] [PubMed]
- Campa, F.; Matias, C.; Gatterer, H.; Toselli, S.; Koury, J.C.; Andreoli, A.; Melchiorri, G.; Sardinha, L.B.; Silva, A.M. Classic bioelectrical impedance vector reference values for assessing body composition in male and female athletes. Int. J. Environ. Res. Public Health 2019, 16, 5066. [Google Scholar] [CrossRef] [PubMed]
- Desbrow, B.; Cox, G.; Desbrow, B.; Burke, L.M.; Cox, G.R.; Sawyer, S.M. Sports Dietitians Australia Position Statement: Sports Nutrition for the Adolescent Athlete Sports Dietitians Australia Position Statement: Sports Nutrition for the Adolescent Athlete. Int. J. Sport Nutr. Exerc. Metab. 2014, 24, 570–584. [Google Scholar] [CrossRef] [PubMed]
- Malina, R.M.; Rogol, A.D.; Cumming, S.P.; Coelho e Silva, M.J.; Figueiredo, A.J. Biological maturation of youth athletes: Assessment and implications. Br. J. Sports Med. 2015, 49, 852–859. [Google Scholar] [CrossRef] [PubMed]
- Mathias-Genovez, M.G.; Oliveira, C.C.; Camelo, J.S.; Del Ciampo, L.A.; Monteiro, J.P. Bioelectrical Impedance of Vectorial Analysis and Phase Angle in Adolescents. J. Am. Coll. Nutr. 2016, 35, 262–270. [Google Scholar] [CrossRef]
- Horlick, M.; Arpadi, S.M.; Bethel, J.; Wang, J.; Moye, J.; Cuff, P.; Pierson, R.N.; Kotler, D. Bioelectrical impedance analysis models for prediction of total body water and fat-free mass in healthy and HIV-infected children and adolescents. Am. J. Clin. Nutr. 2002, 76, 991–999. [Google Scholar] [CrossRef]
- Piccoli, A.; Pillon, L.; Dumler, F. Impedance vector distribution by sex, race, body mass index, and age in the United States: Standard reference intervals as bivariate Z scores. Nutrition 2002, 18, 153–167. [Google Scholar] [CrossRef]
- Piccoli, A.; Pastori, G. BIVA Software 2002; Department of Medical and Surgical Sciences, University of Padova: Padova, Italy, 2002. [Google Scholar]
- Ferreira, A.; Ara, D.; Batalha, N.; Collado-Mateo, D. Phase Angle from Bioelectric Impedance and Maturity-Related Factors in Adolescent Athletes: A Systematic Review. Sustainability 2020, 12, 4806–4820. [Google Scholar]
- Koury, J.C.; Trugo, N.M.F.; Torres, A.G. Phase angle and bioelectrical impedance vectors in adolescent and adult male athletes. Int. J. Sports Physiol. Perform. 2014, 9, 798–804. [Google Scholar] [CrossRef]
- Koury, J.C.; de Oliveira-Junior, A.V.; Portugal, M.R.C.; de Oliveira, K.d.J.F.; Donangelo, C.M. Bioimpedance parameters in adolescent athletes in relation to bone maturity and biochemical zinc indices. J. Trace Elem. Med. Biol. 2018, 46, 26–31. [Google Scholar] [CrossRef] [PubMed]
- Dodds, R.M.; Syddall, H.E.; Cooper, R.; Kuh, D.; Cooper, C. Avan Aihie Sayer Global variation in grip strength: A systematic review and meta-analysis of normative data. Age Ageing 2016, 45, 209–216. [Google Scholar] [CrossRef] [PubMed]
- De Palo, T.; Messina, G.; Edefonti, A.; Perfumo, F.; Pisanello, L.; Peruzzi, L.; Di Iorio, B.; Mignozzi, M.; Vienna, A.; Conti, G.; et al. Normal values of the bioelectrical impedance vector in childhood and puberty. Nutrition 2000, 16, 417–424. [Google Scholar] [CrossRef]
- Toselli, S.; Marini, E.; Latessa, P.M.; Benedetti, L.; Campa, F. Maturity related differences in body composition assessed by classic and specific bioimpedance vector analysis among male elite youth soccer players. Int. J. Environ. Res. Public Health 2020, 17, 729. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Rodríguez, F.; Cristi-Montero, C.; González-Ruíz, K.; Correa-Bautista, J.E.; Ramírez-Vélez, R. Bioelectrical impedance vector analysis and muscular fitness in healthy men. Nutrients 2016, 8, 407. [Google Scholar] [CrossRef]
- Mattiello, R.; Amaral, M.A.; Mundstock, E.; Ziegelmann, P.K. Reference values for the phase angle of the electrical bioimpedance: Systematic review and meta-analysis involving more than 250,000 subjects. Clin. Nutr. 2019, 39, 1411–1417. [Google Scholar] [CrossRef] [PubMed]
- Campa, F.; Silva, A.M.; Iannuzzi, V.; Mascherini, G.; Benedetti, L.; Toselli, S. The role of somatic maturation on bioimpedance patterns and body composition in male elite youth soccer players. Int. J. Environ. Res. Public Health 2019, 16, 4711. [Google Scholar] [CrossRef]
- Buffa, R.; Floris, G.; Marini, E. Bioelectrical impedance vector in pre- and postmenarcheal females. Nutrition 2002, 18, 474–478. [Google Scholar] [CrossRef]
- Toselli, S.; Campa, F.; Latessa, P.M.; Greco, G.; Loi, A.; Grigoletto, A.; Zaccagni, L. Differences in maturity and anthropometric and morphological characteristics among young male basketball and soccer players and non-players. Int. J. Environ. Res. Public Health 2021, 18, 3902. [Google Scholar] [CrossRef]
- Deurenberg, P.; Kusters, C.S.; Smit, H.E. Assessment of body composition by bioelectrical impedance in children and young adults is strongly age-dependent. Eur. J. Clin. Nutr. 1990, 44, 261–268. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Equations | Reference | |
|---|---|---|
| Phase angle | =arc tangent (Xc/R) × (180°/π) | Baumgartner et al. [20] |
| Fat-free mass | =[3.474 + 0.459*H2/R + 0.064 × Wt]/[0.769 − 0.009*age − 0.016 × sex] | Horlick et al. [27] |
| Total body water | =0.725 + 0.475 × H2/R + 0.140 × Wt | Horlick et al. [27] |
| Characteristics | All | Age (Years) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Female | Male | p | Female | p | Male | p | |||
| ≤13.0 | >13.0 | ≤13.0 | >13.0 | ||||||
| n | 112 | 161 | 59 | 53 | 101 | 60 | |||
| Age (years) | 13.0 ± 0.9 | 12.8 ± 0.9 | 0.183 | 12.25 ± 0.46 | 13.82 ± 0.55 | <0.01 | 12.28 ± 0.42 | 13.81 ± 0.50 | <0.01 |
| Weight (kg) | 51.1 ± 10.1 | 48.9 ± 11.5 | 0.098 | 46.7 ± 9.9 | 56.0 ± 8.0 | <0.01 | 45.9 ± 10.8 | 53.8 ± 10.9 | <0.01 |
| Height (cm) | 157.7 ± 7.4 | 156.1 ± 9.9 | 0.153 | 155.3 ± 6.8 | 160.3 ± 7.2 | <0.01 | 152.0 ± 7.9 ** | 163.1 ± 9.0 | <0.01 |
| BMI (kg/m2) | 20.5 ± 3.4 | 19.8 ± 3.2 | 0.124 | 19.2 ± 3.1 | 21.8 ± 3.2 | <0.01 | 19.7 ± 3.4 | 20.1 ± 2.8 ** | 0.446 |
| R (Ω) | 624.1 ± 70.2 | 591.7 ± 72.5 | <0.01 | 643.8 ± 70.3 | 602.2 ± 63.8 | <0.01 | 607.6 ± 72.6 ** | 565 ± 64.5 ** | <0.01 |
| R/H (Ω/m) | 396.9 ± 50.4 | 382.2 ± 62.9 | 0.041 | 415.6 ± 51.8 | 376 ± 39.9 | <0.01 | 402.0 ± 59.4 | 348.8 ± 54 ** | <0.01 |
| Xc (Ω) | 65.7 ± 7.7 | 64.4 ± 9.2 | 0.230 | 65.8 ± 7.6 | 65.5 ± 7.8 | 0.836 | 66.4 ± 9.1 | 61.0 ± 8.5 ** | <0.01 |
| Xc/H (Ω/m) | 41.8 ± 5.4 | 41.6 ± 7.6 | 0.851 | 42.5 ± 5.6 | 40.9 ± 5.0 | 0.125 | 43.9 ± 7.2 | 37.7 ± 6.6 ** | <0.01 |
| Z (Ω) | 627.6 ± 70.2 | 595.8 ± 73.0 | <0.01 | 647.2 ± 70.4 | 605.8 ± 63.9 | 0.002 | 612.2 ± 73.2 ** | 568.3 ± 64.5 ** | <0.01 |
| PhA (degree) | 6.0 ± 0.7 | 6.2 ± 0.7 | 0.033 | 5.87 ± 0.6 | 6.24 ± 0.67 | 0.002 | 6.24 ± 0.67 *** | 6.20 ± 0.83 | 0.746 |
| FFM (kg) | 38.9 ± 5.4 | 40.9 ± 8.2 | 0.021 | 36.3 ± 4.8 | 41.7 ± 4.5 | <0.01 | 37.8 ± 6.6 | 46.2 ± 7.9 *** | <0.01 |
| FM (kg) | 12.2 ± 6.3 | 7.9 ± 6 | <0.01 | 10.4 ± 5.9 | 14.3 ± 6.2 | <0.01 | 8.1 ± 6.2 * | 7.7 ± 5.8 *** | 0.665 |
| FM (%) | 22.7 ± 8.3 | 15.2 ± 8.7 | 0.001 | 20.8 ± 8.1 | 24.8 ± 8.0 | 0.010 | 16.2 ± 9.0 *** | 13.4 ± 7.9 *** | 0.046 |
| TBW (L) | 27.1 ± 4.1 | 27.7 ± 5.9 | 0.371 | 25.3 ± 3.9 | 29.1 ± 3.3 | <0.01 | 25.6 ± 5.0 | 31.1 ± 5.8 * | <0.01 |
| HG (kgf) | 21.0 ± 4.8 | 22.2 ± 6.5 | 0.110 | 19.4 ± 3.9 | 22.8 ± 5.1 | <0.01 | 19.6 ± 4.9 | 26.5 ± 6.7 ** | <0.01 |
| Variables | All * | Female | Male | ||||||
|---|---|---|---|---|---|---|---|---|---|
| β | 95%CI | p-Value | β | 95%CI | p-Value | β | 95%CI | p-Value | |
| Chronological age | 0.572 | 0.024–1.119 | 0.041 | 0.109 | –0.331–1.457 | 0.215 | 0.792 | 0.070–1.513 | 0.032 |
| Fat-free mass | 0.622 | 0.554–0.690 | <0.01 | 0.561 | 0.429–0.694 | 0.001 | 0.636 | 0.559–0.714 | <0.01 |
| Phase angle | 0.058 | –0.117–1.087 | 0.114 | 0.093 | –0.535–1.794 | 0.245 | 0.610 | –0.093–1.313 | 0.089 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cattem, M.V.d.O.; Sinforoso, B.T.; Campa, F.; Koury, J.C. Bioimpedance Vector Patterns according to Age and Handgrip Strength in Adolescent Male and Female Athletes. Int. J. Environ. Res. Public Health 2021, 18, 6069. https://doi.org/10.3390/ijerph18116069
Cattem MVdO, Sinforoso BT, Campa F, Koury JC. Bioimpedance Vector Patterns according to Age and Handgrip Strength in Adolescent Male and Female Athletes. International Journal of Environmental Research and Public Health. 2021; 18(11):6069. https://doi.org/10.3390/ijerph18116069
Chicago/Turabian StyleCattem, Marcus Vinicius de Oliveira, Bruna Taranto Sinforoso, Francesco Campa, and Josely Correa Koury. 2021. "Bioimpedance Vector Patterns according to Age and Handgrip Strength in Adolescent Male and Female Athletes" International Journal of Environmental Research and Public Health 18, no. 11: 6069. https://doi.org/10.3390/ijerph18116069
APA StyleCattem, M. V. d. O., Sinforoso, B. T., Campa, F., & Koury, J. C. (2021). Bioimpedance Vector Patterns according to Age and Handgrip Strength in Adolescent Male and Female Athletes. International Journal of Environmental Research and Public Health, 18(11), 6069. https://doi.org/10.3390/ijerph18116069