
Hospital-Based Healthcare Workers Victims of Workplace Violence in Italy: A Scoping Review


Abstract
1. Introduction
1.1. Critical Issues on Definitions and Complexity Elements in Studying the Concept of Violence and Workplace Violence
1.2. Legal Aspects of WPV in Italy
2. Materials and Methods
2.1. The Scoping Review Question
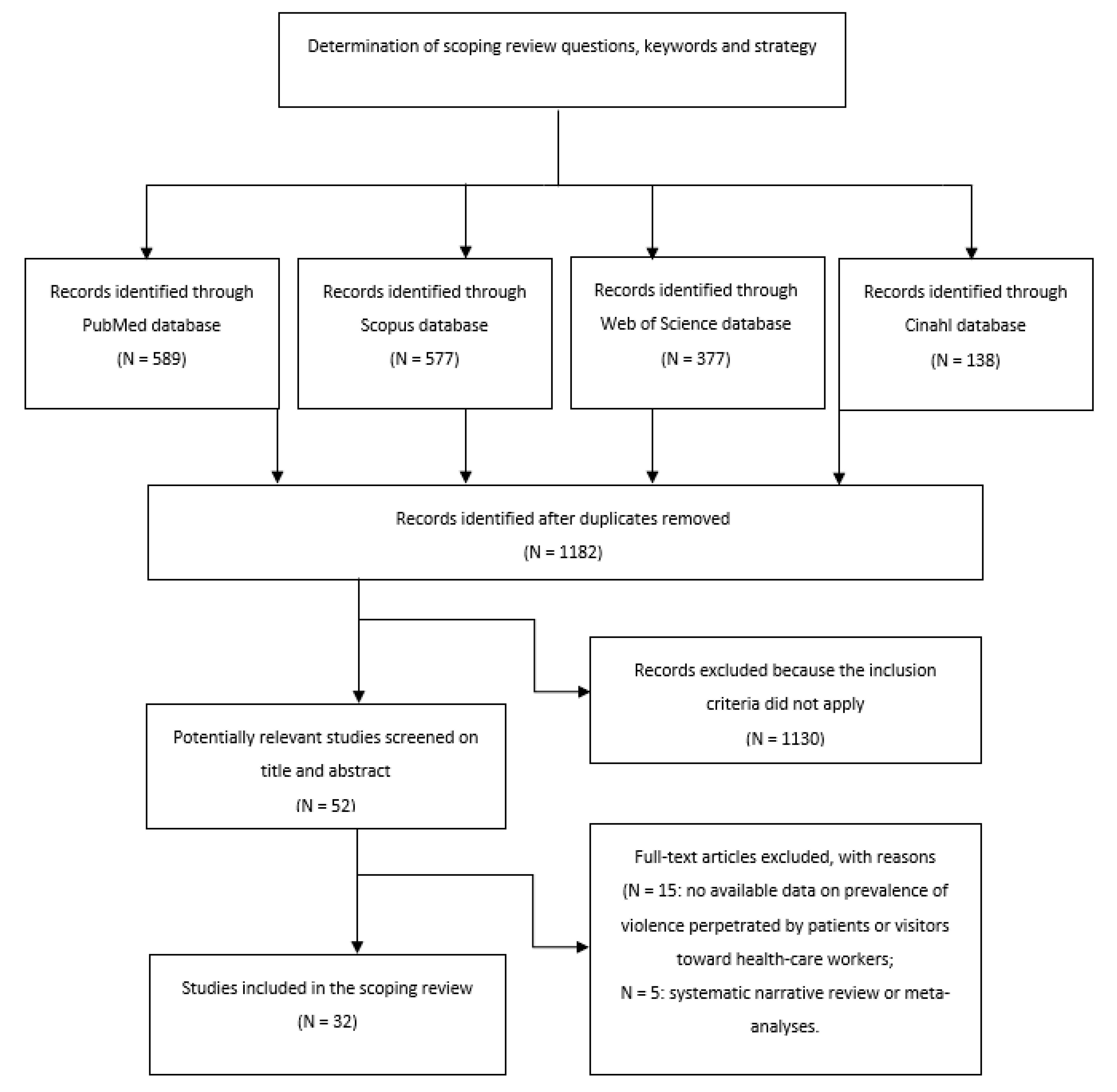
2.2. Search Strategy
- Original research papers and scientific reports;
- Publications written in English or Italian (languages spoken by the authors);
- Articles reporting primary quantitative and/or qualitative data on the prevalence of healthcare workers as victims of aggression or sexual harassment perpetrated by patients or visitors.
2.3. Screening Procedure
2.4. Data Extraction and Results Reporting
3. Results
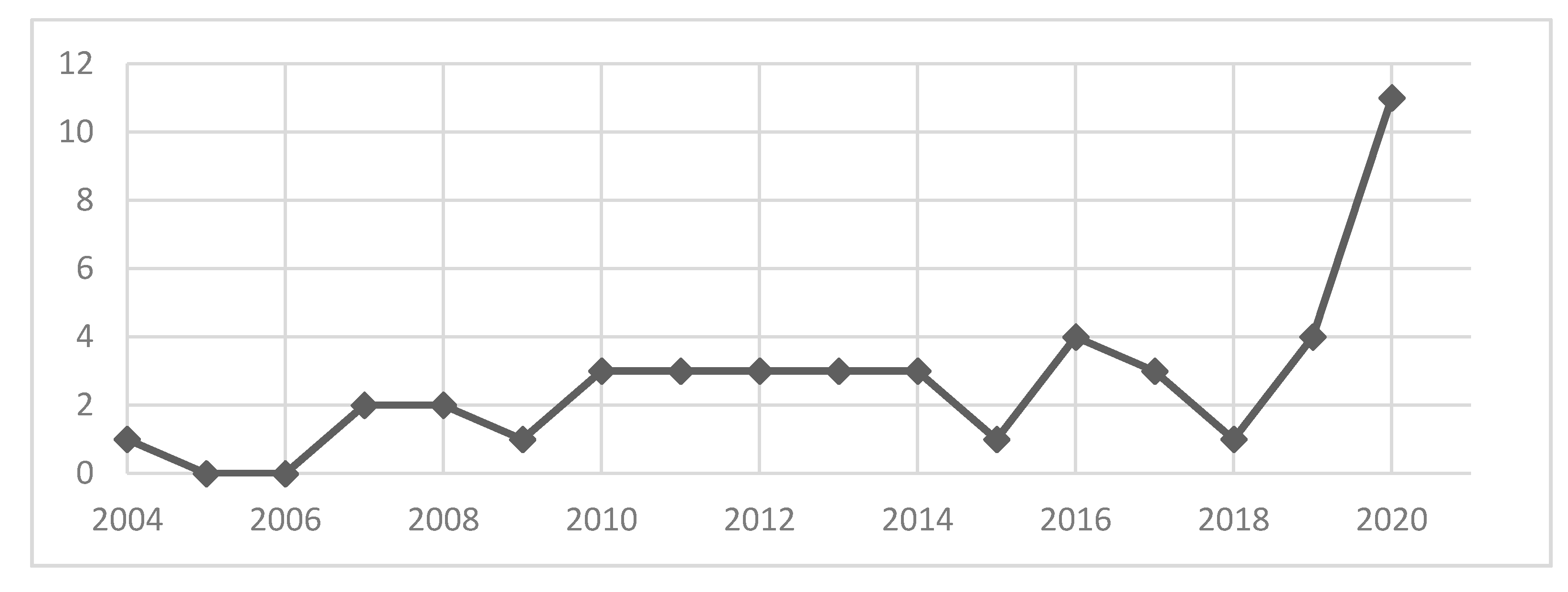
3.1. Methodology and Study Design
3.2. Description of Violent Behavior
3.3. Prevalence and Form of WPV
3.4. Context and Characteristics of Healthcare Workers Involved in WPV
3.5. Characteristics of Violent Patients and Their Relatives and/or Visitors
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Estrada, F.; Nilsson, A.; Jerre, K.; Wikman, S. Violence at work—The emergence of a social problem. J. Scand. Stud. Criminol. Crime Prev. 2010, 11, 46–65. [Google Scholar] [CrossRef]
- Bentley, T.A.; Catley, B.; Forsyth, D.; Tappin, D. Understanding workplace violence: The value of a systems perspective. Appl. Ergon. 2014, 45, 839–848. [Google Scholar] [CrossRef] [PubMed]
- Escribano, R.B.; Beneit, J.; Garcia, J.L. Violence in the workplace: Some critical issues looking at the health sector. Heliyon 2019, 5, e01283. [Google Scholar] [CrossRef] [PubMed]
- Brophy, J.T.; Keith, M.M.; Hurley, M. Assaulted and unheard: Violence against healthcare staff. New Solut. A J. Environ. Occup. Health Policy 2018, 27, 581–606. [Google Scholar] [CrossRef]
- World Health Organization-Violence Against Health Workers. Available online: https://www.who.int/violence_injury_prevention/violence/workplace/en/ (accessed on 14 March 2021).
- Occupational Safety and Health Administration—Preventing Workplace Violence in Healthcare and Social Assistance. Available online: https://www.osha.gov/stakeholder/preventing-workplace-violence (accessed on 14 March 2021).
- World Medical Association—73rd World Health Assembly, Agenda Item 3: Covid-19 Pandemic Response. 2020. Available online: https://www.wma.net/wp-content/uploads/2020/05/WHA73-WMA-statement-on-Covid-19-pandemic-response-.pdf (accessed on 14 March 2021).
- Liu, J.; Gan, Y.; Jiang, H.; Li, L.; Dwyer, R.; Lu, K.; Yan, S.; Sampson, O.; Xu, H.; Wang, C.; et al. Prevalence of workplace violence against healthcare workers: A systematic review and meta-analysis. Occup. Environ. Med. 2019, 76, 927–937. [Google Scholar] [CrossRef] [PubMed]
- Vento, S.; Cainelli, F.; Vallone, A. Violence against healthcare workers: A worldwide phenomenon with serious consequences. Front. Public Health 2020, 8, 570459. [Google Scholar] [CrossRef]
- Havaei, F. Does the Type of Exposure to Workplace Violence Matter to Nurses’ Mental Health? Healthcare 2021, 9, 41. [Google Scholar] [CrossRef]
- McKay, D.; Heisler, M.; Mishori, R.; Catton, H.; Kloiber, O. Attacks against health-care personnel must stop, especially as the world fights COVID-19. Lancet 2020, 395, 1743–1745. [Google Scholar] [CrossRef]
- Nowrouzi-Kia, B.; Chai, E.; Usuba, K.; Nowrouzi-Kia, B.; Casole, J. Prevalence of type II and type III workplace violence against physicians: A systematic review and meta-analysis. Int. J. Occup. Environ. Med. 2019, 10, 99–110. [Google Scholar] [CrossRef]
- Taylor, J.L.; Rew, L. A systematic review of the literature: Workplace violence in the emergency department. J. Clin. Nurs. 2011, 20, 1072–1085. [Google Scholar] [CrossRef] [PubMed]
- Mastronardi, V.M.; Pomilla, A.; Ricci, S.; D’Argenio, A. Stalking of Psychiatrists: Psychopathological Characteristics and Gender Differences in an Italian Sample. Int. J. Offender Ther. Comp. Criminol. 2013, 57, 526–543. [Google Scholar] [CrossRef]
- Binmadi, N.O.; Alblowi, J.A. Prevalence and policy of occupational violence against oral healthcare workers: Systematic review and meta-analysis. BMC Oral Health 2019, 19, 1–8. [Google Scholar] [CrossRef]
- Njaka, S.; Edeogu, O.C.; Oko, C.C.; Goni, M.D.; Nkadi, N. Work place violence (WPV) against healthcare workers in Africa: A systematic review. Heliyon 2020, 6, e04800. [Google Scholar] [CrossRef] [PubMed]
- Babiarczyk, B.; Turbiarz, A.; Tomagová, M.; Zeleníková, R.; Önler, E.; Sancho Cantus, D. Violence against nurses working in the health sector in five European countries—Pilot study. Int. J. Nurs. Pract. 2019, 25, e12744. [Google Scholar] [CrossRef] [PubMed]
- Li, N.; Wang, Z.; Dear, K. Violence against health professionals and facilities in China: Evidence from criminal litigation records. J. Forensic Leg. Med. 2019, 67, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Serrano Vicente, M.I.; Fernández Rodrigo, M.T.; Satústegui Dordá, P.J.; Urcola Pardo, F. Agresiones a profesionales del sector sanitario en España, revisión sistemática. Rev. Española Salud Pública 2020, 93, e201910097. [Google Scholar]
- Sahebi, A.; Jahangiri, K.; Sohrabizadeh, S.; Golitaleb, M. Prevalence of workplace violence types against personnel of emergency medical services in Iran: A systematic review and meta-analysis. Iran. J. Psychiatry 2019, 14, 325–334. [Google Scholar] [CrossRef]
- Mento, C.; Silvestri, M.C.; Bruno, A.; Muscatello, M.R.A.; Cedro, C.; Pandolfo, G.; Zoccali, R.A. Workplace violence against healthcare professionals: A systematic review. Aggress. Violent Behav. 2020, 51, 101381. [Google Scholar] [CrossRef]
- Byon, H.D.; Lee, M.; Choi, M.; Sagherian, K.; Crandall, M.; Lipscomb, J. Prevalence of type II workplace violence among home healthcare workers: A meta-analysis. Am. J. Ind. Med. 2020, 63, 442–455. [Google Scholar] [CrossRef] [PubMed]
- Waddington, P.A.J.; Badger, D.; Bull, R. Appraising the inclusive definition of workplace ‘violence’. Br. J. Criminol. 2005, 45, 141–164. [Google Scholar] [CrossRef]
- World Health Organization. World Report on Violence and Health; World Health Organization: Geneva, Switzerland, 2002. [Google Scholar]
- Cooper, C.; Swanson, N. Workplace Violence in the Health Sector. STATE of the Art; Organización Internacional de Trabajo, Organización Mundial de la Salud, Consejo Internacional de Enfermeras Internacional de Servicios Públicos: Geneva, Switzerlanda, 2002. [Google Scholar]
- Beech, B.; Leather, P. Workplace violence in the health care sector: A review of staff training and integration of training evaluation models. Aggress. Violent Behav. 2006, 11, 27–43. [Google Scholar] [CrossRef]
- Gacki-Smith, J.; Juarez, A.M.; Boyett, L.; Homeyer, C.; Robinson, L.; MacLean, S.L. Violence against nurses working in US emergency departments. JONA J. Nurs. Adm. 2009, 39, 340–349. [Google Scholar] [CrossRef] [PubMed]
- Wassell, J.T. Workplace violence intervention effectiveness: A systematic literature review. Saf. Sci. 2009, 47, 1049–1055. [Google Scholar] [CrossRef]
- EU-OSHA. Workplace Violence and Harassment: A European Picture. European Agency for Safety and Health at Work 2010. Available online: https://osha.europa.eu/en/publications/workplace-violence-and-harassment-european-picture (accessed on 19 March 2021).
- Farrell, G.A.; Shafiei, T. Workplace aggression, including bullying in nursing and midwifery: A descriptive survey (the SWAB study). Int. J. Nurs. Stud. 2012, 49, 1423–1431. [Google Scholar] [CrossRef]
- Piquero, N.L.; Piquero, A.R.; Craig, J.M.; Clipper, S.J. Assessing research on workplace violence, 2000–2012. Aggress. Violent Behav. 2013, 18, 383–394. [Google Scholar] [CrossRef]
- Camerino, D.; Estryn-Behar, M.; Conway, P.M.; van Der Heijden, B.I.J.M.; Hasselhorn, H.-M. Work-related factors and violence among nursing staff in the European NEXT study: A longitudinal cohort study. Int. J. Nurs. Stud. 2008, 45, 35–50. [Google Scholar] [CrossRef]
- Hahn, S.; Zeller, A.; Needham, I.; Kok, G.; Dassen, T.; Halfens, R.J. Patient and visitor violence in general hospitals: A systematic review of the literature. Aggress. Violent Behav. 2008, 13, 431–441. [Google Scholar] [CrossRef]
- Hershcovis, M.S.; Turner, N.; Barling, J.; Arnold, K.A.; Dupré, K.E.; Inness, M.; LeBlanc, M.M.; Sivanathan, N. Predicting workplace aggression: A meta-analysis. J. Appl. Psychol. 2007, 92, 228–238. [Google Scholar] [CrossRef] [PubMed]
- University of Iowa Injury Prevention Research Center. Workplace Violence—A Report to the Nation; University of Iowa: Iowa City, IA, USA, 2001. [Google Scholar]
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef]
- Levac, D.; Colquhoun, H.; O’Brien, K.K. Scoping studies: Advancing the methodology. Implement. Sci. 2010, 5, 1–9. [Google Scholar] [CrossRef]
- Daudt, H.M.; van Mossel, C.; Scott, S.J. Enhancing the scoping study methodology: A large, inter-professional team’s experience with Arksey and O’Malley’s framework. BMC Med. Res. Methodol. 2013, 13, 1–9. [Google Scholar] [CrossRef]
- Magnavita, N. Violence prevention in a small-scale psychiatric unit. Program planning and evaluation. Int. J. Occup. Environ. Health 2011, 17, 336–344. [Google Scholar] [CrossRef]
- Ramacciati, N.; Gili, A.; Mezzetti, A.; Ceccagnoli, A.; Addey, B.; Rasero, L. Violence towards Emergency Nurses: The 2016 Italian National Survey—A cross-sectional study. J. Nurs. Manag. 2019, 27, 792–805. [Google Scholar] [CrossRef] [PubMed]
- Magnavita, N. Workplace Violence and Occupational Stress in Healthcare Workers: A Chicken-and-Egg SituationResults of a 6-Year Follow-up Study. J. Nurs. Scholarsh. 2014, 46, 366–376. [Google Scholar] [CrossRef] [PubMed]
- Arnetz, J.E. The Violent Incident Form (VIF): A practical instrument for the registration of violent incidents in the health care workplace. Work Stress 1998, 12, 17–28. [Google Scholar] [CrossRef]
- Grattagliano, I.; Amoruso, A.; Scandamarro, G.; Pierri, G.; Pastore, A.; Margari, F. Stalking of social healthcare workers: Preliminary results of a study conducted by the region of Apulia, Italy. Riv. Di Psichiatr. 2014, 49, 273–278. [Google Scholar] [CrossRef]
- Acquadro Maran, D.A.; Varetto, A.; Zedda, M. Italian nurses’ experience of stalking: A questionnaire survey. Violence Vict. 2014, 29, 109–121. [Google Scholar] [CrossRef] [PubMed]
- Ferri, P.; Silvestri, M.; Artoni, C.; Di Lorenzo, R. Workplace violence in different settings and among various health professionals in an Italian general hospital: A cross-sectional study. Psychol. Res. Behav. Manag. 2016, 9, 263–275. [Google Scholar] [CrossRef] [PubMed]
- Cannavò, M.; Fusaro, N.; Colaiuda, F.; Rescigno, G.; Fioravanti, M. Violence on health care workers. Clin. Ther. 2017, 168, e99–e112. [Google Scholar] [CrossRef]
- Cannavò, M.; La Torre, F.; Sestili, C.; La Torre, G.; Fioravanti, M. Work related violence as a predictor of stress and correlated disorders in emergency department healthcare professionals. Clin. Ther. 2019, 170, e110–e123. [Google Scholar] [CrossRef]
- Franchini, L.; Colombo, C.; Aiolfi, I.; Alajmo, V.B.M.; Beckman, E.M.; Edel, M.; Marcocci, L.; Ragone, N.; Travaini, G. A Descriptive Study of Suffered and Witnessed Aggressions in Two Rehabilitative Italian Units. Clin. Neuropsychiatry 2020, 17, 158–163. [Google Scholar] [CrossRef]
- Zampieron, A.; Galeazzo, M.; Turra, S.; Buja, A. Perceived aggression towards nurses: Study in two Italian health institutions. J. Clin. Nurs. 2010, 19, 2329–2341. [Google Scholar] [CrossRef]
- Catanesi, R.; Carabellese, F.; Candelli, C.; Valerio, A.; Martinelli, D. Violent patients: What Italian psychiatrists feel and how this could change their patient care. Int. J. Offender Ther. Comp. Criminol. 2010, 54, 441–447. [Google Scholar] [CrossRef]
- Zoleo, M.; Della Rocca, F.; Tedeschi, F.; Zucchetto, M.; Maddalena, G.; Vettore, G. Violence against health workers: Findings from three emergency departments in the teaching hospital of Padua, Italy. Intern. Emerg. Med. 2020, 15, 1067–1074. [Google Scholar] [CrossRef]
- Firenze, A.; Santangelo, O.E.; Gianfredi, V.; Alagna, E.; Cedrone, F.; Provenzano, S.; La Torre, G. Violence on doctors. An observational study in Northern Italy. La Med. Del Lav. 2020, 111, 46–53. [Google Scholar] [CrossRef]
- Aguglia, A.; Belvederi Murri, M.; Conigliaro, C.; Cipriani, N.; Vaggi, M.; Di Salvo, G.; Maina, G.; Cavone, V.; Aguglia, E.; Serafini, G.; et al. Workplace violence and burnout among mental health workers. Psychiatr. Serv. 2020, 71, 284–288. [Google Scholar] [CrossRef]
- Ramacciati, N.; Ceccagnoli, A.; Addey, B.; Lumini, E.; Rasero, L. Violence towards emergency nurses: A narrative review of theories and frameworks. Int. Emerg. Nurs. 2018, 39, 2–12. [Google Scholar] [CrossRef]
- Magnavita, N.; Heponiemi, T.; Chirico, F. Workplace violence is associated with impaired work functioning in nurses: An Italian cross-sectional study. J. Nurs. Scholarsh. 2020, 52, 281–291. [Google Scholar] [CrossRef] [PubMed]
- Magnavita, N.; Heponiemi, T. Workplace Violence Against Nursing Students and Nurses: An Italian Experience. J. Nurs. Scholarsh. 2011, 43, 203–210. [Google Scholar] [CrossRef] [PubMed]
- Ferri, P.; Stifani, S.; Accoto, A.; Bonetti, L.; Rubbi, I.; Di Lorenzo, R. Violence against nurses in the triage area: A mixed-methods study. J. Emerg. Nurs. 2020, 46, 384–397. [Google Scholar] [CrossRef]
- Bizzarri, J.V.; Piacentino, D.; Kotzalidis, G.D.; Moser, S.; Cappelletti, S.; Weissenberger, G.; Pompili, M.; Conca, A.; Bizzarri, V.J. Aggression and violence toward healthcare workers in a psychiatric service in Italy: A retrospective questionnaire-based survey. J. Nerv. Ment. Dis. 2020, 208, 299–305. [Google Scholar] [CrossRef]
- Converso, D.; Sottimano, I.; Balducci, C. Violence exposure and burnout in healthcare sector: Mediating role of work ability. La Med. Del Lav. 2021, 112, 58–67. [Google Scholar] [CrossRef]
- Acquadro Maran, D.; Varetto, A.; Zedda, M.; Magnavita, N. Workplace violence toward hospital staff and volunteers: A survey of an Italian sample. J. Aggress. Maltreatment Trauma 2018, 27, 76–95. [Google Scholar] [CrossRef]
- Berlanda, S.; Pedrazza, M.; Fraizzoli, M.; de Cordova, F. Addressing risks of violence against healthcare staff in emergency departments: The effects of job satisfaction and attachment style. Biomed Res. Int. 2019, 2019. [Google Scholar] [CrossRef]
- Terzoni, S.; Ferrara, P.; Cornelli, R.; Ricci, C.; Oggioni, C.; Destrebecq, A. Violence and unsafety in a major Italian hospital: Experience and perceptions of health care workers. La Med. Del Lav. 2015, 106, 403–411. [Google Scholar]
- Romito, P.; Ballard, T.; Maton, N. Sexual harassment among female personnel in an Italian hospital—Frequency and correlates. Violence Against Women 2004, 10, 386–417. [Google Scholar] [CrossRef]
- Magnavita, N.; Heponiemi, T.; Bevilacqua, L.; Capri, A.; Roccia, K.; Quaranta, D.; Ciriello, S.; Gabriele, M.; Giudice, A.; Lilli, M.; et al. Analysis of violence against health care workers through medical surveillance at the workplace in a 8-yr period. G. Ital. Di Med. Del Lav. Ed Ergon. 2011, 33 (Suppl. 3), 274–277. [Google Scholar]
- Magnavita, N.; Fileni, A.; Pescarini, L.; Magnavita, G. Violence against radiologists. I: Prevalence and preventive measures. Radiol. Med. 2012, 117, 1019–1033. [Google Scholar] [CrossRef]
- Magnavita, N.; Heponiemi, T. Violence towards health care workers in a Public Health Care Facility in Italy: A repeated cross-sectional study. BMC Health Serv. Res. 2012, 12, 1–9. [Google Scholar] [CrossRef]
- Gravante, F.; Lombardi, A.; Cecere, L.; Russo, G.; De Rosa, F.; Gagliardi, A.M.; Gilli, A.; Ramacciati, N. Emergency nurses and workplace violence: A cross-sectional study in Campania, South Italy. Prof. Inferm. 2020, 73, 89–97. [Google Scholar] [CrossRef]
- Viottini, E.; Politano, G.; Fornero, G.; Pavanelli, P.L.; Borelli, P.; Bonaudo, M.; Gianino, M.M. Determinants of aggression against all health care workers in a large-sized university hospital. BMC Health Serv. Res. 2020, 20, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health. Recommendation n. 8 to prevent acts of violence against health workers. 2007. [Google Scholar]
- Guglielmetti, C.; Gilardi, S.; Licata, M.; De Luca, G. The healthcare operators’ experience with aggressive patients and their visitors: A cross-sectional study in four clinical departments. La Med. Del Lav. 2016, 107, 223–234. [Google Scholar]
- Lin, Y.H.; Liu, H.E. The impact of workplace violence on nurses in South Taiwan. Int. J. Nurs. Stud. 2005, 42, 773–778. [Google Scholar] [CrossRef]
- Carmi-Iluz, T.; Peleg, R.; Freud, T.; Shvartzman, P. Verbal and physical violence towards hospital-and community-based physicians in the Negev: An observational study. BMC Health Serv. Res. 2005, 5, 1–6. [Google Scholar] [CrossRef]
- Paola, F.; Malik, T.; Qureshi, A. Violence against physicians. J. Gen. Intern. Med. 1994, 9, 503–506. [Google Scholar] [CrossRef]
- Adib, S.M.; Al-Shatti, A.K.; Kamal, S.; El-Gerges, N.; Al-Raqem, M. Violence against nurses in healthcare facilities in Kuwait. Int. J. Nurs. Stud. 2002, 39, 469–478. [Google Scholar] [CrossRef]
- Winstanley, S.; Whittington, R. Aggression towards health care staff in a UK general hospital: Variation among professions and departments. J. Clin. Nurs. 2004, 13, 3–10. [Google Scholar] [CrossRef]
- Whittington, R.; Shuttleworth, S.; Hill, L. Violence to staff in a general hospital setting. J. Adv. Nurs. 1996, 24, 326–333. [Google Scholar] [CrossRef]
- Landau, S.F.; Bendalak, J.; Amitay, G.; Marcus, O. Factors related to negative feelings experienced by emergency department patients and accompanying persons: An Israeli study. Isr. J. Health Policy Res. 2018, 7, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Howerton Child, R.H.; Mentes, J.C. Violence against women: The phenomenon of workplace violence against nurses. Issues Ment. Health Nurs. 2010, 31, 89–95. [Google Scholar] [CrossRef]
- Phillips, J.P. Workplace violence against health care workers in the United States. N. Engl. J. Med. 2016, 374, 1661–1669. [Google Scholar] [CrossRef] [PubMed]
- Wax, J.R.; Pinette, M.G.; Cartin, A. Workplace violence in health care—it’s not “Part of the Job”. Obstet. Gynecol. Surv. 2016, 71, 427–434. [Google Scholar] [CrossRef]
- Findorff, M.J.; McGovern, P.M.; Wall, M.M.; Gerberich, S.G. Reporting violence to a health care employer: A cross-sectional study. AAOHN J. 2005, 53, 399–406. [Google Scholar] [CrossRef] [PubMed]
- Papalia, F.; Magnavita, N. Unknown occupational risk: Physical violence at the workplace. Giornale italiano di medicina del lavoro ed ergonomia 2003, 25, 176–177. [Google Scholar]
- Tragno, M.; Duveau, A.; Tarquinio, C. Les violences et agressions physiques au travail: Analyse de la littérature. Eur. Rev. Appl. Psychol. 2007, 57, 237–255. [Google Scholar] [CrossRef]
- Alameddine, M.; Kazzi, A.; El-Jardali, F.; Dimassi, H.; Maalouf, S. Occupational violence at Lebanese emergency departments: Prevalence, characteristics and associated factors. J. Occup. Health 2011, 1109210208. [Google Scholar] [CrossRef]
- Newman, C.J.; De Vries, D.H.; Kanakuze, J.D.A.; Ngendahimana, G. Workplace violence and gender discrimination in Rwanda’s health workforce: Increasing safety and gender equality. Hum. Resour. Health 2011, 9, 1–13. [Google Scholar] [CrossRef]
- Zelnick, J.R.; Gibbs, A.; Loveday, M.; Padayatchi, N.; O’donnell, M.R. Health-care workers’ perspectives on workplace safety, infection control, and drug-resistant tuberculosis in a high-burden HIV setting. J. Public Health Policy 2013, 34, 388–402. [Google Scholar] [CrossRef] [PubMed]
- Toth, F. How health care regionalisation in Italy is widening the North-South gap. Health Econ. Policy Law 2014, 9, 231–249. [Google Scholar] [CrossRef]
- Mangano, A. An analysis of the regional differences in health care utilization in Italy. Health Place 2010, 16, 301–308. [Google Scholar] [CrossRef] [PubMed]
- Arnetz, J.E.; Hamblin, L.; Ager, J.; Luborsky, M.; Upfal, M.J.; Russell, J.; Essenmacher, L. Underreporting of workplace violence: Comparison of self-report and actual documentation of hospital incidents. Workplace Health Saf. 2015, 63, 200–210. [Google Scholar] [CrossRef] [PubMed]
- LeBlanc, M.M.; Barling, J. Workplace aggression. Curr. Dir. Psychol. Sci. 2004, 13, 9–12. [Google Scholar] [CrossRef]
- May, D.D.; Grubbs, L.M. The extent, nature, and precipitating factors of nurse assault among three groups of registered nurses in a regional medical center. J. Emerg. Nurs. 2002, 28, 11–17. [Google Scholar] [CrossRef] [PubMed]
- Rasool, S.F.; Wang, M.; Tang, M.; Saeed, A.; Iqbal, J. How Toxic Workplace Environment Effects the Employee Engagement: The Mediating Role of Organizational Support and Employee Wellbeing. Int. J. Environ. Res. Public Health 2021, 18, 2294. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| First Author | Year of Publication | Research Location | Sample, Response Rate in % | Tools |
|---|---|---|---|---|
| Romito et al. | 2004 | Public hospital (Trieste) | 265 healthcare workers (Physicians and nurses). Response rate = 61.6% | Sexual Experiences Questionnaire modified |
| Grottoli et al. | 2007 | - | 355 healthcare workers | - |
| Camerino et al. | 2008 | General Hospital (outpatient departments, surgery, geriatrics, medicine, pediatrics and psychiatric departments) | 5541 nurses. Response rate = 61.6% | Ad-hoc questionnaire |
| Zampieron et al. | 2010 | 94 different clinical units (outpatient departments, surgery, geriatrics, medicine, pediatrics and psychiatric departments of two Italian health institution | 595 nurses. Response rate = 85% | Ad-hoc questionnaire |
| Catanesi et al. | 2010 | - | 1202 psychiatrists’ members of the Italian Society of Psychiatry. Response rate = 20.2% | Ad-hoc questionnaire |
| Cerri et al. | 2010 | - | 467 healthcare workers | - |
| Magnavita & Heponiemi | 2011 | General Hospital | 346 nursing students and 275 nurses from a general hospital. Response rate = 94.2% | Violent Incident Form |
| Magnavita et al. | 2012 | Public hospital | 992 radiologists | Violent Incident Form |
| Magnavita & Heponiemi | 2012 | A general hospital and Public Health Care Facilities | 1166 healthcare workers. Response rate = 80.1% | Violent Incident Form |
| Mastronardi et al. | 2013 | 42 public mental health centers | 478 psychiatrists: 246 publics and 232 privates. | Ad hoc interview |
| Gagliardi et al. | 2013 | - | 396 professionals | - |
| Grattagliano et al. | 2014 | Public mental health centers and private psychiatrists (Bari) | 101 healthcare workers (doctors, psychologists, nurses, socio-health workers). | Adhoc questionnaire |
| Magnavita | 2014 | Health unit (Rome) | 698 healthcare workers. Response rate = 96.5%. | Violent Incident Form |
| Acquadro Maran et al. | 2014 | Different wards of 4 Italian state hospitals located in the North of the country | 765 nurses from different wards (obstetrics, emergency internal medicine, otolaryngology and pediatrics). Response rate= 38.4% | The modified Italian version of the Questionnaire constructed by The Network for Surviving Stalking (NSS) |
| Terzoni et al. | 2015 | Different wards of a major Italian hospital | 903 healthcare workers (336 nurses, 195 medical doctors, 109 administrative employees, 52 auxiliaries and 47 physiotherapists, 164 included laboratory technicians, workmen, midwives, professional educators, auxiliary personnel, biologists, head nurses, or did not specify). Response rate = 48.7% | ISTAT (Istituto nazionale di statistica) questionnaire |
| Luciani et al. | 2016 | A major Italian Hospital (Lombardy Region) | 198 nurses | - |
| Ferri et al. | 2016 | 15 wards of a general hospital | 419 professionals (77 physicians, 17 head nurses, 259 nurses, 66 nursing assistants). Response rate = 56.2% | Violent Incident Form |
| Cannavò et al. | 2017 | Emergency Departments of a general hospital | 51 healthcare workers (administrative staff = 4, physicians = 5) and nurses = 42). Response rate = 87.9% | Questionario sulla Violenza in Sanità |
| Acquadro Maran et al. | 2018 | A hospital in northern Italy | 108 healthcare workers and 96 volunteers working in cardiology and oncology wards | Violent Incident Form |
| Ramacciati et al. | 2019 | All the Italian Emergency Departments | 816 Emergency nurses in all Italian regions. Response rate = 7% | Questionario per l’Indagine Nazionale 2016 sulla Violenza verso gli Infermieri di Pronto Soccorso |
| Berlanda et al. | 2019 | Eight Emergency departments in northeastern Italy | 149 (87 Physician and 62 nurses). Response rate = 37.7%) | Adhoc questionnaire |
| Cannavò et al. | 2019 | An Emergency Department of a general hospital and an acute psychiatric inpatients unit | 323 healthcare workers (nurses, auxiliary and administrative staff). Response rate = 80.7% | Health Violence questionnaire |
| Franchini et al. | 2020 | Private Hospital (Milan). Rehabilitative psychiatric and neurological wards | 55 healthcare workers (41 nurses, 6 healthcare assistant, 4 residents, 4 social educators). | A semi-structured interview |
| Ferri et al. | 2020 | An emergency department of a general hospital | 27 Italian nurses involved in the triage area. Response rate = 100% | Violent Incident Form |
| Bizzarri et al. | 2020 | Psychiatric Services (Bolzano) | 164 mental health workers. Response rate = 77.7%. | Risk Analysis Questionnaire |
| Magnavita et al. | 2020 | General Hospital | 275 nurses. Response rate = 91.1% | Violent Incident Form |
| Viottini et al. | 2020 | University Hospital (Turin) | 10,970 healthcare workers (nurses, medical doctors, support staff, administratives) | Aggression Reporting Form |
| Zoleo et al. | 2020 | Three emergency departments of a teaching hospital (Padua) | 171 healthcare workers (Nurse, Physician and Patient care assistant) from general, pediatric and obstetric-gynecological emergency departments. | Ad-hoc questionnaire |
| Firenze et al. | 2020 | Doctors from Northern Italy | 4545 healthcare workers. | Ad-hoc questionnaire |
| Aguglia et al. | 2020 | Emergency psychiatric wards in 3 Hospitals and 3 Mental Health Centres | 183 mental health workers: nurses = 56, psychiatrists = 39, residents = 58, other professionals = 30. Response rate = 67% | Ad-hoc structured questionnaire |
| Gravante et al. | 2020 | Emergency Departments in Campania Region | 83 emergency nurses | - |
| Converso et al. | 2021 | Two large hospitals in northern Italy | 300 nurses. Response rate = 60% | Violent Incident Form |
| Authors | Profession | Workplace Violence in % | Patients Violence in % | Visitors Violence in % | ||||
|---|---|---|---|---|---|---|---|---|
| Verbal | Physical | Harassment | Verbal | Physical | Verbal | Physical | ||
| Zampieron et al. 2010 | Nurses | 81.6 | 4.8 | - | - | - | - | - |
| Romito et al. 2004 | Nurses and physicians | 29 | - | - | - | - | ||
| Magnavita et al. 2011 | Physicians Nurses Psychiatrists others | 11.9 | 9.2 | 23 | - | - | - | - |
| Magnavita andHeponiemi, 2011 | Nurses Nursing students | 34.9 | 9.5 | - | 65.4 | 14.7 | ||
| Magnavita et al. 2012 | radiologists | 16.3 | 5.9 | 27.6 | ||||
| Converso et al. 2021 | Nurses | 85.8 | 6.6 | - | 36.8 | 59.8 | ||
| Aguglia et al. 2020 | Mental health workers: Psychiatrists, residents, nurses and others | 41.5 | 2.7 | - | - | - | ||
| Magnavita et al. 2020 | Nurses | 19.6 | 9.8 | - | - | - | ||
| Bizzarri et al. 2020 | mental health workers | 90.9 | 44.5 | - | - | - | ||
| Ramacciati et al. 2018 | Nurses | 76.0 | - | - | - | |||
| Acquadro Maran et al. 2018 | HCWs in oncology and cardiology | 50.5 | 25.0 | - | - | - | ||
| Ferri et al. 2020 | Nurses | 92.3 | 0 | - | 30.8 | 61.5 | ||
| Terzoni et al. 2015 | Nurses Physicians Laboratory technicians Physiotherapists Auxiliaries Administratives | 40.2 | 11.5 | - | 75.0 | 58.0 | 23.1 | 27.6 |
| Magnavita, 2014 | Physicians Nurses Technicians | 52.6 | 24.6 | - | - | - | ||
| Berlanda et al. 2019 | Physicians and Nurses | 93.3 | 53.0 | - | 95.30 | 52.35 | 85.91 | 20.81 |
| Firenze et al. 2020 | Physicians | 51.5 | 39.4 | - | 23.0 | 78.0 | 58.0 | 59.0 |
| Authors | Profession | WPV in % | Patients Violence in % | Visitors Violence in % | ||||
|---|---|---|---|---|---|---|---|---|
| Verbal | Physical | Harassment | Verbal | Physical | Verbal | Physical | ||
| Magnavita & Heponiemi, 2012 | Physicians Nurses Psychiatrists others | 65.5 | 25.7 | 5.5 | 50.8 | 23.1 | ||
| Magnavita et al. 2012 | radiologists | 48.8 | 30.0 | 20.7 | 32.5 | 37.1 | 15.9 | 34.3 |
| Catanesi et al. 2010 | Psychiatrists | 90.9 | 64.6 | 72.0 | - | - | ||
| Aguglia et al. 2020 | Mental health workers: Psychiatrists, residents, nurses and others | 89.6 | 50.3 | - | - | - | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Civilotti, C.; Berlanda, S.; Iozzino, L. Hospital-Based Healthcare Workers Victims of Workplace Violence in Italy: A Scoping Review. Int. J. Environ. Res. Public Health 2021, 18, 5860. https://doi.org/10.3390/ijerph18115860
Civilotti C, Berlanda S, Iozzino L. Hospital-Based Healthcare Workers Victims of Workplace Violence in Italy: A Scoping Review. International Journal of Environmental Research and Public Health. 2021; 18(11):5860. https://doi.org/10.3390/ijerph18115860
Chicago/Turabian StyleCivilotti, Cristina, Sabrina Berlanda, and Laura Iozzino. 2021. "Hospital-Based Healthcare Workers Victims of Workplace Violence in Italy: A Scoping Review" International Journal of Environmental Research and Public Health 18, no. 11: 5860. https://doi.org/10.3390/ijerph18115860
APA StyleCivilotti, C., Berlanda, S., & Iozzino, L. (2021). Hospital-Based Healthcare Workers Victims of Workplace Violence in Italy: A Scoping Review. International Journal of Environmental Research and Public Health, 18(11), 5860. https://doi.org/10.3390/ijerph18115860