
Impacts of Social Participation on Self-Rated Health of Aging Women in China: With a Mediating Role of Caring for Grandchildren

Abstract
1. Introduction
2. Literature Review
3. Material and Method
3.1. Data
3.2. Variables Selection
3.2.1. Outcome Variable
3.2.2. Explanatory Variables
3.2.3. Mediator
3.2.4. Control Variables
3.2.5. Instrumental Variable
3.3. Core Models Development
3.3.1. Oprobit Model
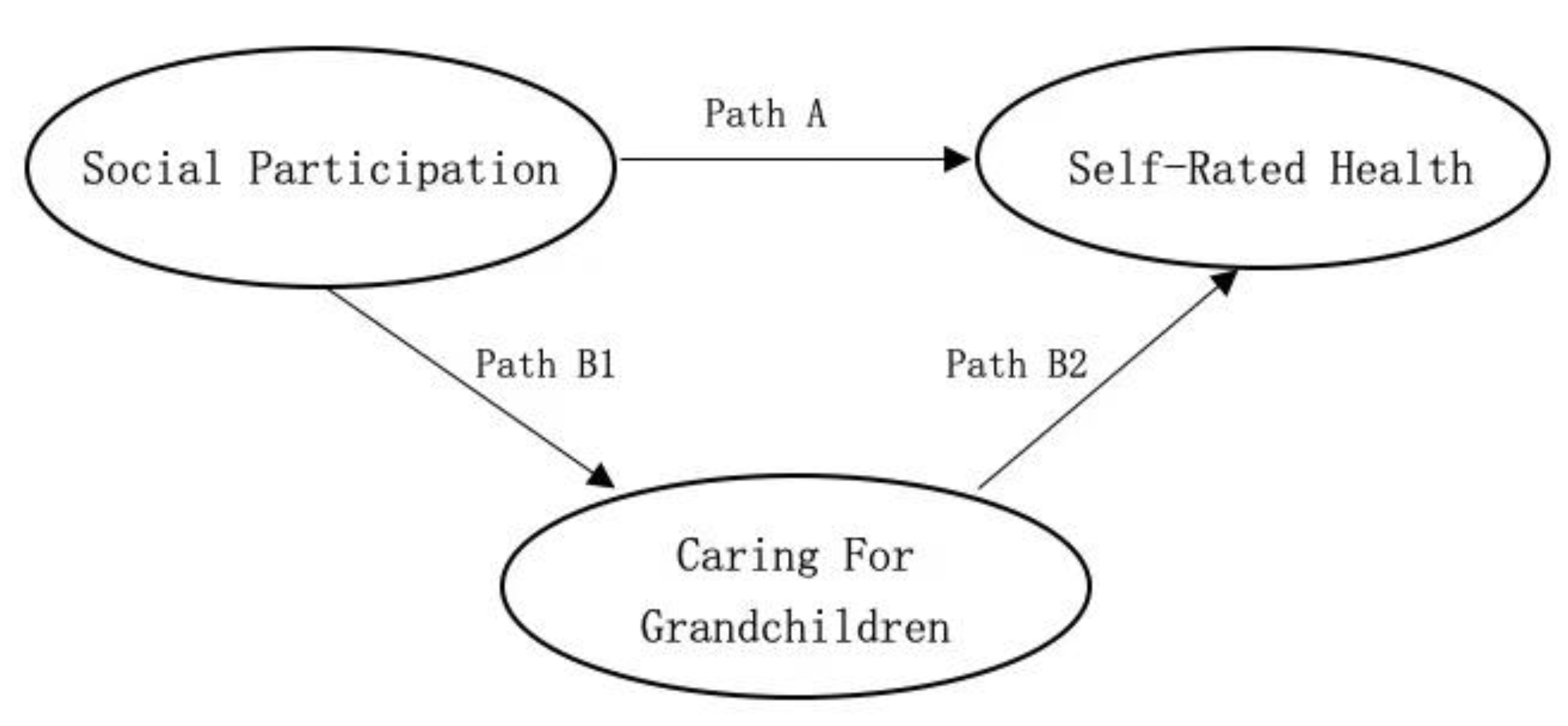
3.3.2. Mediating Effect
3.3.3. Propensity Score Matching (PSM)
3.3.4. Instrumental Variable Regression
4. Results
4.1. Sample Description
4.2. Impacts of Social Participation on Self-Rated Health of Aging Women
4.2.1. Oprobit Regression Results
4.2.2. Impacts of Different Types of Social Participation on Self-Rated Health
4.2.3. Heterogeneity Analysis
4.2.4. The Mediating Effect of Caring for Grandchildren
4.3. Robustness Test
4.3.1. Narrow down the Targeted Sample
4.3.2. Adjust Control Variables
4.3.3. Replacing the Measuring Question of the Outcome Variable
4.3.4. Propensity Score Matching (PSM)
4.4. Endogenous Variable Processing
5. Discussion
6. Conclusions
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cox, R.B.P.R. The aging of populations and its economic and social implications. J. R. Statis. Socs. 1958, 121, 253–254. [Google Scholar] [CrossRef]
- Statistical Bulletin on National Economic and Social Development. Available online: http://www.stats.gov.cn/tjsj/zxfb/202002/t20200228_1728913.html (accessed on 18 April 2021). (In Chinese)
- World Health Organization Active Ageing. A Policy Framework Geneva. 1 April 2002. pp. 1–60. Available online: http://whqlibdoc.who.int/hq/2002/who_nmh_nph_02.8.pdf (accessed on 18 April 2021).
- Gergen, M.M.; Gergen, K.J. Positive aging: New images for a new age. Ageing Int. 2001, 27, 3–23. [Google Scholar] [CrossRef]
- Rowe, J.W.; Kahn, R.L. Human aging: Usual and successful. Science 1987, 237, 143–149. [Google Scholar] [CrossRef]
- Johnson, K.; Mutchler, J. The Emergence of a Positive Gerontology: From Disengagement to Social Involvement. Gerontologist 2013, 54, 93–100. [Google Scholar] [CrossRef]
- Van Dyk, S.; Lessenich, S.; Denninger, T.; Richter, A. The Many Meanings of “Active Ageing”: Confronting Public Discourse with Older People’s Stories. Rech. Sociol. Anthropol. 2013, 44, 41–44. [Google Scholar] [CrossRef]
- Havighurst, R.J. Successful ageing. Gerontologist 1961, 1, 8–13. [Google Scholar] [CrossRef]
- Cottrell, L. The Adjustment of the Individual to his Age and Sex Roles. Am. Sociol. Rev. 1942, 7, 617–620. [Google Scholar] [CrossRef]
- Hooyman, N.R.; Kiyak, H.A. Social Gerontology: A Multidisciplinary Perspective, 9th ed.; Pearson: New York, NY, USA, 2011. [Google Scholar]
- Shi, W. How Does the Involvement of Older Mass Organizations Affect Elder Abuse? Soc. Sci. Ningxia 2019, 6, 108–116. (In Chinese) [Google Scholar]
- Okun, M.A.; Yeung, E.W.; Brown, S. Volunteering by older adults and risk of mortality: A meta-analysis. Psychol. Aging 2013, 28, 564–577. [Google Scholar] [CrossRef] [PubMed]
- Son, J.; Wilson, J. Volunteer Work and Hedonic, Eudemonic, and Social Well-Being. Sociol. Forum. 2012, 27, 658–681. [Google Scholar] [CrossRef]
- Li, Y.; Xu, L.; Chi, I.; Guo, P. Participation in productive activities and health outcomes among older adults in urban China. Gerontologist 2014, 54, 784–796. [Google Scholar] [CrossRef] [PubMed]
- Li, Q. Seniors’ Volunteerism in Urban Communities: A Survey in Jinan City. Soc. Sci. 2010, 6, 72–79, 189. (In Chinese) [Google Scholar]
- Wu, J.J.; Ling, B.J.; Zhang, X. The Effect of the Old People’s Participation in Volunteer Activities on Their Subjective Well-Being: A Survey in Chaoyang District of Beijing. South China Popu. 2012, 27, 24–31. (In Chinese) [Google Scholar]
- Wang, J.W. The Research of Effect on Subjective Well-Being of the Elderly from Volunteering Activity Participation. Sci. Res. Aging 2015, 3, 58–63. (In Chinese) [Google Scholar]
- Jylhä, M. What is self-rated health and why does it predict mortality? Toward a unified conceptual model. Soc. Sci. Med. 2009, 69, 307–316. [Google Scholar] [CrossRef]
- Idler, E.L.; Benyamini, Y. Self-rated health and mortality: A review of twenty-seven community studies. J. Health Soc. Behav. 1997, 38, 21–37. [Google Scholar] [CrossRef]
- Idler, E.L.; Hudson, S.V.; Leventhal, H. The Meanings of Self-Ratings of Health: A Qualitative and Quantitative Approach. Res. Aging 1999, 21, 458–476. [Google Scholar] [CrossRef]
- Kaplan, G.; Baron-Epel, O. What lies behind the subjective evaluation of health status? Soc. Sci. Med. 2003, 56, 1669–1676. [Google Scholar] [CrossRef]
- Feng, Q.; Zhu, H.; Zhen, Z.; Gu, D. Self-Rated Health, Interviewer-Rated Health, and Their Predictive Powers on Mortality in Old Age. J. Gerontol. B Psychol. Sci. Soc. Sci. 2016, 71, 538–550. [Google Scholar] [CrossRef]
- DeSalvo, K.B.; Bloser, N.; Reynolds, K.; He, J.; Muntner, P. Mortality prediction with a single general self-rated health question. A Meta-Anal. J. Gen. Intern. Med. 2006, 21, 267–275. [Google Scholar] [CrossRef]
- Households Size and Composition Around the World 2017. Available online: https://www.un.org/en/development/desa/population/publications/pdf/ageing/household_size_and_composition_around_the_world_2017_data_booklet.pdf (accessed on 18 April 2021).
- He, Y.; Wang, Y.P. Do intergeneration care and elder care by children lead to early retirement of parents? Popu. Res. 2015, 39, 78–90. (In Chinese) [Google Scholar]
- Chen, F.; Liu, G.; Mair, C.A. Intergeneration Ties in Context: Grandparents Caring for Grandchildren in China. Soc. Forces 2011, 2, 571–594. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.; Lou, V.W.Q. Patterns of productive activity engagement as a longitudinal predictor of depressive symptoms among older adults in urban China. Aging Ment. Health 2017, 21, 1147–1154. [Google Scholar] [CrossRef]
- Short, S.E.; Zhai, F.Y.; Xu, S.Y.; Yang, M.L. China’s one-child policy and the care of children: An analysis of qualitative and quantitative data. Soc. Forces 2001, 79, 913–943. [Google Scholar] [CrossRef]
- Yasuda, T.; Iwai, N.; Yi, C.-C.; Xie, G. Intergenerational Coresidence in China, Japan, South Korea and Taiwan: Comparative Analyses Based on the East Asian Social Survey 2006. J. Comp. Fam. Stud. 2011, 42, 703–722. [Google Scholar] [CrossRef]
- Hughes, M.E.; Waite, L.J.; LaPierre, T.A.; Luo, Y. All in the family: The impact of caring for grandchildren on grandparents’ health. J. Gerontol. B Psychol. Sci. Soc. Sci. 2007, 62, S108–S119. [Google Scholar] [CrossRef] [PubMed]
- Hawkes, K.; O’Connell, J.F.; Jones, N.G.B.; Alvarez, H.; Charnov, E.L. Grandmothering, menopause, and the evolution of human life histories. Proc. Natl. Acad. Sci. USA 1998, 95, 1336–1339. [Google Scholar] [CrossRef] [PubMed]
- Zhang, W.; Feng, Q.; Liu, L.; Zhen, Z. Social Engagement and Health: Findings from the 2013 Survey of the Shanghai Elderly Life and Opinion. Int. J. Aging Hum. Develop. 2015, 80, 332–356. [Google Scholar] [CrossRef]
- Prokos, A.H.; Keene, J.R. The Life Course and Cumulative Disadvantage: Poverty among Grandmother-Headed Families. Res. Aging 2012, 34, 592–621. [Google Scholar] [CrossRef]
- Lee, J.; Bauer, J.W. Motivations for Providing and Utilizing Child Care by Grandmothers in South Korea. J. Marriage Fam. 2013, 75, 381–402. [Google Scholar] [CrossRef]
- Zhao, Y.H.; Strauss, J.; Chen, X.X.; Wang, Y.F.; Gong, J.Q.; Meng, Q.Q.; Wang, G.W.; Wang, H.L. China Health and Retirement Longitudinal Study Wave 4 User’s Guide; National School of Development, Peking University: Beijing, China, 2020. [Google Scholar]
- Sharma, N.; Chakrabarti, S.; Grover, S. Gender differences in caregiving among family-caregivers of people with mental illnesses. World J. Psychiatry 2016, 6, 7–17. [Google Scholar] [CrossRef]
- Williams, L.A.; Giddings, L.S.; Bellamy, G.; Gott, M. ‘Because it’s the wife who has to look after the man’: A descriptive qualitative study of older women and the intersection of gender and the provision of family caregiving at the end of life. Palliat. Med. 2017, 31, 223–230. [Google Scholar] [CrossRef]
- Qing, S.S. Gender Role Attitudes, Family Responsibilities and Female-male Labor Force Participation Patterns. Soc. Sci. 2017, 11, 91–100. (In Chinese) [Google Scholar] [CrossRef]
- Adamson, J.; Lawlor, D.A.; Ebrahim, S. Chronic diseases, locomotor activity limitation and social participation in older women: Cross sectional survey of British Women’s Heart and Health Study. Age Ageing 2004, 33, 293–298. [Google Scholar] [CrossRef]
- Kim, J.H.; Kim, M.; Kim, J. Social Activities and Health of Korean Elderly Women by Age Groups. Educ. Gerontol. 2013, 39, 640–654. [Google Scholar] [CrossRef]
- Erlinghagen, M.; Hank, K. The participation of older Europeans in volunteer work. Ageing Soc. 2016, 26, 567–584. [Google Scholar] [CrossRef]
- Xie, L.L.; Wang, B. Social Participation Profile of the Chinese Elderly in the Context of Active Ageing: Patterns and Determinants. Popu. Res. 2019, 43, 17–30. (In Chinese) [Google Scholar]
- YU, Z.H. Elderly Volunteering Service Participation Inclination Predictors’Analysis of China’s Urban and Rural Areas: Based on Data of the 4th Sampling Survey of the Living Conditions of the Elderly in Urban and Rural Areas of China. Northwest Popu. J. 2019, 40, 57–65. (In Chinese) [Google Scholar] [CrossRef]
- Angrist, J.D.; Krueger, A.B. Instrumental Variables and the Search for Identification: From Supply and Demand to Natural Experiments. J. Econ. Perspect. 2001, 15, 69–85. [Google Scholar] [CrossRef]
- Levasseur, M.; Richard, L.; Gauvin, L.; Raymond, E. Inventory and analysis of definitions of social participation found in the aging literature: Proposed taxonomy of social activities. Soc. Sci. Med. 2010, 71, 2141–2149. [Google Scholar] [CrossRef]
- Noreau, L.; Desrosiers, J.; Robichaud, L.; Fougeyrollas, P.; Rochette, A.; Viscogliosi, C. Measuring social participation: Reliability of the LIFE-H in older adults with disabilities. Disabil. Rehabil. 2004, 26, 346–352. [Google Scholar] [CrossRef]
- Poulin, V.; Desrosiers, J. Reliability of the LIFE-H satisfaction scale and relationship between participation and satisfaction of older adults with disabilities. Disabil. Rehabil. 2009, 31, 1311–1317. [Google Scholar] [CrossRef]
- Borawski, E.A.; Kinney, J.M.; Kahana, E. The meaning of older adults’ health appraisals: Congruence with health status and determinant of mortality. J. Gerontol. B Psychol. Sci. Soc. Sci. 1996, 51, S157–S170. [Google Scholar] [CrossRef]
- Jang, Y.; Chiriboga, D.A.; Borenstein, A.R.; Small, B.J.; Mortimer, J.A. Health-related quality of life in community-dwelling older Whites and African Americans. J. Aging Health 2009, 21, 336–349. [Google Scholar] [CrossRef]
- Stock, J.H.; Yogo, M. Testing for Weak Instruments in Linear IV Regression. In Identification and Inference for Econometric Models; Andrews, D.W.K., Ed.; Cambridge University Press: New York, NY, USA, 2005; pp. 80–108. [Google Scholar]
- Gu, L.; Wu, S.; Zhao, S.; Zhou, H.; Zhang, S.; Gao, M.; Qu, Z.; Zhang, W.; Tian, D. Association of Social Support and Medication Adherence in Chinese Patients with Type 2 Diabetes Mellitus. Int. J. Environ. Res. Public Health 2017, 14, 1522. [Google Scholar] [CrossRef]
- Hughes, T.F.; Flatt, J.D.; Fu, B.; Chang, C.-C.H.; Ganguli, M. Engagement in social activities and progression from mild to severe cognitive impairment: The MYHAT study. Int. Psychogeriatr. 2013, 25, 587–595. [Google Scholar] [CrossRef] [PubMed]
- Thomas, P.A. Trajectories of Social Engagement and Limitations in Late Life. J. Health Soc. Behav. 2011, 52, 430–443. [Google Scholar] [CrossRef] [PubMed]
- Peng, D.; Fei, W. Productive Ageing in China: Development of Concepts and Policy Practice. Ageing Int. 2013, 38, 4–14. [Google Scholar] [CrossRef]
- Xiao, H.; Li, P. The impact of taking care of grandchildren on the mental health of rural middle aged and elders in China. Chin. J. Health Policy 2019, 2, 41–50. (In Chinese) [Google Scholar]
- Bai, Y.; Bian, F.; Zhang, L.; Cao, Y. The Impact of Social Support on the Health of the Rural Elderly in China. Int. J. Environ. Res. Public Health 2020, 17, 2004. [Google Scholar] [CrossRef] [PubMed]
- Musick, M.A.; Herzog, A.R.; House, J.S. Volunteering and mortality among older adults: Findings from a national sample. J. Gerontol. B Psychol. Sci. Soc. Sci. 1999, 54, S173–S180. [Google Scholar] [CrossRef]
- Krause, N.; Ingersoll-Dayton, B.; Liang, J.; Sugisawa, H. Religion, social support, and health among the Japanese elderly. J. Health Soc. Behav. 1999, 40, 405–421. [Google Scholar] [CrossRef]
- Xia, X.P. Issuses about elder volunteers under the context of active aging. Chin. J. Gerontol. 2015, 35, 2862–2864. (In Chinese) [Google Scholar]
- Liu, W.; Yang, F.P. The Evaluation of Active Aging Development in China—Based on Regional and Provincial Data. Popu. J. 2019, 41, 100–112. (In Chinese) [Google Scholar] [CrossRef]
- Davison, K.K.; Lawson, C.T. Do attributes in the physical environment influence children’s physical activity? A review of the literature. Int. J. Behav. Nutr. Phys. Act. 2016, 3, 19. [Google Scholar] [CrossRef]
- Levasseur, M.; Généreux, M.; Bruneau, J.F.; Vanasse, A.; Chabot, É.; Beaulac, C.; Bédard, M.M. Importance of proximity to resources, social support, transportation and neighborhood security for mobility and social participation in older adults: Results from a scoping study. BMC Public Health 2015, 15, 503. [Google Scholar] [CrossRef] [PubMed]
- Peng, D.P. “The Sequence of Spatial Difference”: Mechanism of the Elders’ Social Participation in Small Cities—Based on the Investigation in Lin’an District, Zhejiang Province. Soc. Constr. 2019, 6, 41–50. (In Chinese) [Google Scholar]
- Takagi, D.; Kondo, K.; Kawachi, I. Social participation and mental health: Moderating effects of gender, social role and rurality. BMC Public Health. 2013, 13, 701. [Google Scholar] [CrossRef]
- Dong, J.Q.; Jia, J.M. An Empirical Study on the Evolutional Effects of Citizenization of City-Villagers. J. South China Agr. Univ. (Soc. Sci. Ed.) 2013, 12, 51–58. (In Chinese) [Google Scholar]
- Utz, R.L.; Carr, D.; Nesse, R.; Wortman, C.B. The effect of widowhood on older adults’ social participation: An evaluation of activity, disengagement, and continuity theories. Gerontologist 2002, 42, 522–533. [Google Scholar] [CrossRef]
- Gallagher, S.K.; Gerstel, N. Kinkeeping and friend keeping among older women: The effect of marriage. Gerontologist 1993, 33, 675–681. [Google Scholar] [CrossRef] [PubMed]
- Ward, R.; Logan, J.; Spitze, G. The Influence of Parent and Child Needs on Coresidence in Middle and Later Life. J. Marriage Fam. 1992, 54, 209–221. [Google Scholar] [CrossRef]


{kind=link}
| Variable | Original Question | Codes |
|---|---|---|
| Age | What is your date of birth on your ID card or household register? | Calculated by 2018 minus the respondent’s birth year. |
| Residence | Was your address, BB000_W3, in the village or city/town? | 1 = Central City/Town; 2 = Urban–Rural Integration Zone; 3 = Rural; 4 = Special Zone |
| Smoking | Have you ever chewed tobacco, smoked a pipe, smoked self-rolled cigarettes, or smoked cigarettes/cigars? | 1 = Yes; 0 = No |
| Drinking | Did you drink any alcoholic beverages, such as beer, wine, or liquor in the past year? How often? | 1 = Yes; 0 = No |
| Education | What is the highest level of education you have now (not including adult education)? | 1 = No formal education (illiterate); 2 = Did not finish primary school; 3 = Middle school; 4 = High school and vocational school; 5 = college (associate degree) or above |
| Marriage | What is your marital status? | 1 = Married with Spouse Present; 2 = Married But Not Living with Spouse Temporarily for Reasons Such as Work; 3 = Separated; 4 = Divorced; 5 = Widowed; 6 = Never Married |
| Minority | Are you Han or Ethnic Minorities? | 1 = Han Nationality; 0 = Ethnic Minorities |
| Income | Did you receive any wage or bonus income in the past year? | 1 = Yes; 0 = No |
| Insurance | Are you the policy holder/primary beneficiary of any of the types of health insurance listed below? | 1 = Yes; 0 = No |
| Region | What is your address in [ZIWTime]? | Based on provided addresses, dividing the region into east, central, and west regions; 0 = East; 1 = Central; 2 = West. |
| Variable | Total | Social Participation | Non-Social Participation | |
|---|---|---|---|---|
| Mean (SD) | Mean (SD) | Mean (SD) | Range | |
| Outcome Variable | ||||
| Self-rated Health | 2.860 (1.000) | 2.940 (0.980) | 2.780 (1.010) | 1–5 |
| Explanatory Variable | ||||
| Social Participation | 0.483 (0.500) | 1.000 (0.000) | 0.000 (0.000) | 0–1 |
| Mediator | ||||
| Caring for Grandchildren | 0.360 (0.480) | 0.390 (0.490) | 0.330 (0.470) | 0–1 |
| Instrumental Variable | ||||
| Relationship with Children | 3.578 (0.759) | 3.600 (0.740) | 3.550 (0.770) | 1–5 |
| Control Variable | ||||
| Age | 69.320 (7.220) | 68.610 (6.840) | 69.960 (7.480) | 60–108 |
| Age2 | 4857.840 (1053.610) | 4754.520 (988.890) | 4950.090 (1098.570) | 3600–11,664 |
| Residence | 2.520 (0.820) | 2.430 (0.860) | 2.620 (0.750) | 1–4 |
| Smoking | 0.020 (0.130) | 0.020 (0.140) | 0.010 (0.110) | 0–1 |
| Drinking | 0.130 (0.340) | 0.150 (0.360) | 0.110 (0.310) | 0–1 |
| Education | 1.910 (0.990) | 2.080 (1.040) | 1.740 (0.910) | 1–5 |
| Marriage | 2.180 (1.790) | 2.190 (1.800) | 2.170 (1.790) | 1–6 |
| Minority | 0.920 (0.260) | 0.930 (0.260) | 0.920 (0.270) | 0–1 |
| Insurance | 0.970 (0.180) | 0.970 (0.170) | 0.960 (0.200) | 0–1 |
| Income | 0.070 (0.260) | 0.070 (0.260) | 0.070 (0.260) | 0–1 |
| Region | 0.990 (0.820) | 0.940 (0.820) | 1.040 (0.820) | 0–2 |
| Variable | (1) | (2) | (3) Marginal Effects (dy/dx) | ||
|---|---|---|---|---|---|
| Oprobit | Oprobit | Fair | Good | Very Good | |
| Social Participation | 0.187 *** (0.030) | 0.117 *** (0.032) | 0.011 *** (0.003) | 0.013 *** (0.004) | 0.018 *** (0.005) |
| Age | −0.138 *** (0.041) | −0.013 *** (0.004) | −0.016 *** (0.005) | −0.021 *** (0.006) | |
| Age2 | 0.001 *** (0) | 0.000 *** (0) | 0.000 *** (0) | 0.000 *** (0) | |
| Residence | −0.122 *** (0.021) | −0.011 *** (0.002) | −0.014 *** (0.002) | −0.018 *** (0.003) | |
| Smoking | −0.0431 (0.132) | −0.004 (0.012) | −0.005 (0.015) | −0.007 (0.02) | |
| Drinking | 0.173 *** (0.048) | 0.016 *** (0.005) | 0.020 *** (0.005) | 0.026 *** (0.007) | |
| Education | 0.0189 (0.018) | 0.002 (0.002) | 0.002 (0.002) | 0.003 (0.003) | |
| Marriage | −0.0314 *** (0.010) | −0.003 *** (0.001) | −0.004 *** (0.001) | −0.005 *** (0.001) | |
| Minority | −0.00991 (0.062) | −0.001 (0.006) | −0.001 (0.007) | −0.001 (0.009) | |
| Insurance | −0.0498 (0.089) | −0.005 (0.008) | −0.006 (0.01) | −0.008 (0.013) | |
| Income | 0.304 *** (0.060) | 0.028 *** (0.006) | 0.034 *** (0.007) | 0.046 *** (0.009) | |
| Central Region | −0.178 *** (0.039) | −0.014 *** (0.003) | −0.020 *** (0.005) | −0.028 *** (0.006) | |
| West Region | −0.210 *** (0.040) | −0.018 *** (0.004) | −0.024 *** (0.005) | −0.033 *** (0.006) | |
| N | 5015 | 4575 | 4575 | 4575 | 4575 |
| pseudo R2 | 0.003 | 0.016 | |||
| Variable | Oprobit (dy/dx) | ||
|---|---|---|---|
| (1) | (2) | (3) | |
| Self-Rated Health (Very Good) | Self-Rated Health (Very Good) | Self-Rated Health (Very Good) | |
| Social Participation | 0.018 *** (0.005) | ||
| Type 1 Activity | 0.017 *** (0.005) | ||
| Type 2 Activity | 0.028 *** (0.007) | ||
| Control Variables | Yes | Yes | Yes |
| N | 4575 | 4575 | 4575 |
| pseudo R2 | 0.016 | 0.016 | 0.016 |
| Variable | Pooled | Subsample: Region | Subsample: Residence | Subsample: Partner | |||||
|---|---|---|---|---|---|---|---|---|---|
| (1) Full Sample | (2) East | (3) Central | (4) West | (5) Urban | (6) Urban–Rural Integration Zone | (7) Rural | (8) Yes | (9) No | |
| Very Good | Very Good | Very Good | Very Good | Very Good | Very Good | Very Good | Very Good | Very Good | |
| Social Participation | 0.018 *** (0.005) | 0.018 (0.011) | 0.021 *** (0.008) | 0.014 ** (0.006) | 0.036 *** (0.012) | 0.043 ** (0.019) | 0.011 ** (0.006) | 0.012 * (0.006) | 0.030 *** (0.008) |
| Region | Yes | No | No | No | Yes | Yes | Yes | Yes | Yes |
| Residence | Yes | Yes | Yes | Yes | No | No | No | Yes | Yes |
| Partner | Yes | Yes | Yes | Yes | Yes | Yes | Yes | No | No |
| Others | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| N | 4575 | 1547 | 1471 | 1557 | 954 | 292 | 3315 | 3362 | 1213 |
| pseudo R2 | 0.0156 | 0.0151 | 0.0177 | 0.0130 | 0.0176 | 0.0234 | 0.0127 | 0.0134 | 0.0207 |
| Variable | Oprobit | Probit | Oprobit |
|---|---|---|---|
| (1) | (2) | (3) | |
| Self-Rated Health (Very Good) | Caring for Grandchildren (Yes) | Self-Rated Health (Very Good) | |
| Social Participation | 0.018 *** (0.005) | 0.029 * (0.017) | 0.016 *** (0.006) |
| Caring for Grandchildren | 0.018 *** (0.006) | ||
| Control Variables | Yes | Yes | Yes |
| N | 4575 | 3006 | 2784 |
| pseudo R2 | 0.016 | 0.124 | 0.018 |
| Variable | Oprobit | |||
|---|---|---|---|---|
| (1) | (2) | (3) | (4) | |
| Self-Rated Health | Self-Rated Health | Self-Rated Health | Health Satisfaction | |
| Social Participation | 0.117 *** (0.032) | 0.212 ** (0.084) | 0.100 ** (0.046) | 0.082 ** (0.032) |
| Age | −0.138 *** (0.041) | −0.146 (0.099) | −0.096 ** (0.042) | |
| Age2 | 0.001 *** (0.000) | 0.001 (0.001) | 0.001 ** (0.000) | |
| Residence | −0.122 *** (0.021) | −0.083 (0.059) | −0.057 *** (0.021) | |
| Smoking | −0.043 (0.132) | 0.030 (0.359) | 0.019 (0.132) | |
| Drinking | 0.173 *** (0.048) | 0.097 (0.127) | 0.116 ** (0.047) | |
| Education | 0.019 (0.018) | 0.060 (0.050) | −0.081 *** (0.018) | |
| Marriage | −0.031 *** (0.010) | −0.057 ** (0.025) | −0.004 (0.010) | |
| Minority | −0.010 (0.062) | 0.219 (0.157) | −0.035 (0.062) | |
| Insurance | −0.050 (0.089) | −0.028 (0.228) | −0.013 (0.120) | −0.104 (0.089) |
| Income | 0.304 *** (0.060) | 0.273 (0.188) | 0.260 *** (0.086) | 0.277 *** (0.060) |
| Central Region | −0.178 *** (0.039) | 0.056 (0.106) | −0.158 *** (0.057) | −0.021 (0.039) |
| West Region | −0.210 *** (0.040) | −0.081 (0.105) | −0.195 *** (0.056) | −0.063 (0.039) |
| Age Gap | 0.105 * (0.061) | |||
| Bad Habit | 0.144 ** (0.064) | |||
| Literature | 0.101 * (0.054) | |||
| Partner | 0.153 *** (0.055) | |||
| Pension | −0.008 (0.066) | |||
| Disability | −0.606 *** (0.055) | |||
| N | 4575 | 686 | 2182 | 4525 |
| Pseudo R2 | 0.0156 | 0.0167 | 0.0321 | 0.0054 |
| Variable | Definition | Codes |
|---|---|---|
| Age Group | Categorized participants into 1. Youth; 2. Middle-Age; 3. Old Age; 4. Elderly; 5. Senior | 1 = 1–44 years old; 2 = 45–59 years old; 3 = 60–74 years old; 4 = 75–89 years old; 5 =≥ 90 years old |
| Bad Habit | Do you smoke or drink? | 1 = yes; 0 = no |
| Literature | Are you literate? | 1 = yes; 0 = no |
| Partner | Do you have a partner? | 1 = yes; 0 = no |
| Pension | Do you have a pension? | 1 = yes; 0 = no |
| Disability | Are you disabled? | 1 = yes; 0 = no |
| Methods | Sample | Have Social Participation = (1) | No Social Participation = (2) | ATT = (1)–(2) | SE | t-Value |
|---|---|---|---|---|---|---|
| KNN (K = 4) | Unmatched | 2.936 | 2.792 | 0.144 | 0.029 | 4.93 *** |
| Matched | 2.936 | 2.825 | 0.111 | 0.035 | 3.17 *** | |
| Radius Matching | Unmatched | 2.936 | 2.792 | 0.144 | 0.029 | 4.93 *** |
| Matched | 2.936 | 2.832 | 0.104 | 0.040 | 2.62 *** | |
| Local Linear Regression | Unmatched | 2.936 | 2.792 | 0.144 | 0.029 | 4.93 *** |
| Matched | 2.936 | 2.827 | 0.109 | 0.040 | 2.75 *** | |
| MDM | Unmatched | 2.936 | 2.792 | 0.144 | 0.029 | 4.93 *** |
| Matched | 2.936 | 2.858 | 0.078 | 0.034 | 2.27 *** | |
| Kernel Matching | Unmatched | 2.936 | 2.792 | 0.144 | 0.029 | 4.93 *** |
| Matched | 2.936 | 2.824 | 0.112 | 0.031 | 3.61 *** |
| Methods | Sample | Ps R2 | LR chi2 | p > chi2 | Mean Bias | Med Bias |
|---|---|---|---|---|---|---|
| KNN (K = 4) | Unmatched | 0.035 | 224.97 | 0.000 | 11.2 | 10.1 |
| Matched | 0.002 | 10.35 | 0.585 | 2.8 | 3.3 | |
| Radius Matching | Unmatched | 0.035 | 224.97 | 0.000 | 11.2 | 10.1 |
| Matched | 0.002 | 14.15 | 0.291 | 2.2 | 1.4 | |
| Local Linear Regression | Unmatched | 0.035 | 224.97 | 0.000 | 11.2 | 10.1 |
| Matched | 0.002 | 14.70 | 0.258 | 2.2 | 1.4 | |
| MDM | Unmatched | 0.035 | 224.97 | 0.000 | 11.2 | 10.1 |
| Matched | 0.003 | 16.34 | 0.176 | 2.0 | 0.7 | |
| Kernel Matching | Unmatched | 0.035 | 224.97 | 0.000 | 11.2 | 10.1 |
| Matched | 0.001 | 3.99 | 0.984 | 1.4 | 1.3 |
| Variable | (1) | (2) | (3) | ||
|---|---|---|---|---|---|
| Oprobit (dy/dx) | 2SLS | LIML | |||
| First Stage | Second Stage | First Stage | Second Stage | ||
| Social Participation | 1.775 *** (0.005) | 11.75 * (6.937) | 11.751 * (6.937) | ||
| Instrumental Variable | 0.016 * (0.010) | 0.016 * (0.010) | |||
| Control Variables | Yes | Yes | Yes | Yes | Yes |
| N | 4575 | 4510 | 4510 | 4510 | 4510 |
| F | 19.87 | 19.87 | |||
| pseudo R2 or R2 | 0.016 | 0.0482 | 0.0482 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tian, S.; Xu, L.; Wu, X. Impacts of Social Participation on Self-Rated Health of Aging Women in China: With a Mediating Role of Caring for Grandchildren. Int. J. Environ. Res. Public Health 2021, 18, 5790. https://doi.org/10.3390/ijerph18115790
Tian S, Xu L, Wu X. Impacts of Social Participation on Self-Rated Health of Aging Women in China: With a Mediating Role of Caring for Grandchildren. International Journal of Environmental Research and Public Health. 2021; 18(11):5790. https://doi.org/10.3390/ijerph18115790
Chicago/Turabian StyleTian, Shuliu, Lei Xu, and Xiangling Wu. 2021. "Impacts of Social Participation on Self-Rated Health of Aging Women in China: With a Mediating Role of Caring for Grandchildren" International Journal of Environmental Research and Public Health 18, no. 11: 5790. https://doi.org/10.3390/ijerph18115790
APA StyleTian, S., Xu, L., & Wu, X. (2021). Impacts of Social Participation on Self-Rated Health of Aging Women in China: With a Mediating Role of Caring for Grandchildren. International Journal of Environmental Research and Public Health, 18(11), 5790. https://doi.org/10.3390/ijerph18115790