
Are Core Stability Tests Related to Single Leg Squat Performance in Active Females?

 ,
,  ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Procedures
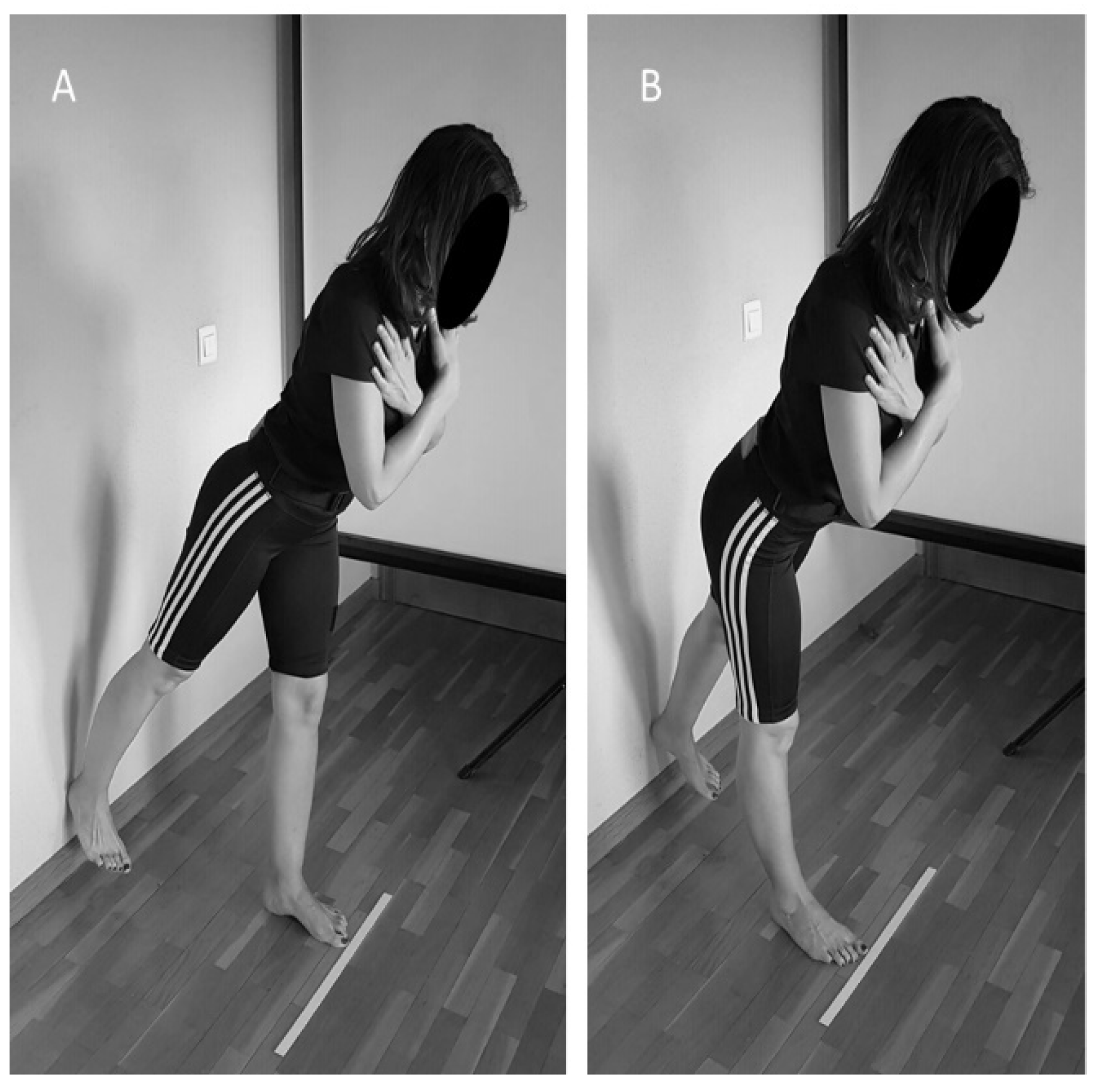
2.2.1. Weight-Bearing Dorsiflexion Test
2.2.2. Bird-Dog (BD) Test
2.2.3. Partial Range Single-Leg Deadlift Core Stability Test (SLD)
2.2.4. Single-Leg Squat Test (SLS)
2.3. Analysis
2.3.1. Data Analysis and Reduction
2.3.2. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Emamvirdi, M.; Letafatkar, A.; Tazji, M.K. The Effect of Valgus Control Instruction Exercises on Pain, Strength, and Functionality in Active Females with Patellofemoral Pain Syndrome. Sports Health Multidiscip. Approach 2019, 11, 223–237. [Google Scholar] [CrossRef]
- Hewett, T.E.; Myer, G.D.; Ford, K.R.; Paterno, M.V.; Quatman, C.E. Mechanisms, prediction, and prevention of ACL injuries: Cut risk with three sharpened and validated tools. J. Orthop. Res. 2016, 34, 1843–1855. [Google Scholar] [CrossRef] [PubMed]
- Hewett, T.E.; Ford, K.R.; Hoogenboom, B.J.; Myer, G.D. Understanding and preventing acl injuries: Current biome-chanical and epidemiologic considerations—Update 2010. N. Am. J. Sports Phys. Ther. 2010, 5, 234–251. [Google Scholar]
- Schmidt, E.; Harris-Hayes, M.; Salsich, G.B. Dynamic knee valgus kinematics and their relationship to pain in women with patellofemoral pain compared to women with chronic hip joint pain. J. Sport Health Sci. 2019, 8, 486–493. [Google Scholar] [CrossRef]
- Wilczyński, B.; Zorena, K.; Ślęzak, D. Dynamic Knee Valgus in Single-Leg Movement Tasks. Potentially Modifiable Factors and Exercise Training Options. A Literature Review. Int. J. Environ. Res. Public Health 2020, 17, 8208. [Google Scholar] [CrossRef]
- Alentorn-Geli, E.; Myer, G.D.; Silvers, H.J.; Samitier, G.; Romero, D.; Lázaro-Haro, C.; Cugat, R. Prevention of non-contact anterior cruciate ligament injuries in soccer players. Part 1: Mechanisms of injury and underlying risk factors. Knee Surg. Sports Traumatol. Arthrosc. 2009, 17, 705–729. [Google Scholar] [CrossRef] [PubMed]
- Hewett, T.E.; Myer, G.D.; Ford, K.R.; Heidt, R.S.; Colosimo, A.J.; McLean, S.G.; Bogert, A.J.V.D.; Paterno, M.V.; Succop, P. Biomechanical Measures of Neuromuscular Control and Valgus Loading of the Knee Predict Anterior Cruciate Ligament Injury Risk in Female Athletes: A Prospective Study. Am. J. Sports Med. 2005, 33, 492–501. [Google Scholar] [CrossRef] [PubMed]
- Nakagawa, T.H.; Moriya, E.T.U.; Maciel, C.D.; Serrão, F.V. Trunk, Pelvis, Hip, and Knee Kinematics, Hip Strength, and Gluteal Muscle Activation During a Single-Leg Squat in Males and Females With and Without Patellofemoral Pain Syndrome. J. Orthop. Sports Phys. Ther. 2012, 42, 491–501. [Google Scholar] [CrossRef]
- Harris-Hayes, M.; Steger-May, K.; Koh, C.; Royer, N.K.; Graci, V.; Salsich, G.B. Classification of Lower Extremity Movement Patterns Based on Visual Assessment: Reliability and Correlation With 2-Dimensional Video Analysis. J. Athl. Train. 2014, 49, 304–310. [Google Scholar] [CrossRef]
- Scholtes, S.A.; Salsich, G.B. A dynamic valgus index that combines hip and knee angles: Assessment of utility in females with patellofemoral pain. Int. J. Sports Phys. Ther. 2017, 12, 333–340. [Google Scholar]
- Leetun, D.T.; Ireland, M.L.; Willson, J.D.; Ballantyne, B.T.; Davis, I.M. Core Stability Measures as Risk Factors for Lower Extremity Injury in Athletes. Med. Sci. Sports Exerc. 2004, 36, 926–934. [Google Scholar] [CrossRef] [PubMed]
- De Blaiser, C.; Roosen, P.; Willems, T.; Danneels, L.; Bossche, L.V.; De Ridder, R. Is core stability a risk factor for lower extremity injuries in an athletic population? A systematic review. Phys. Ther. Sport 2018, 30, 48–56. [Google Scholar] [CrossRef] [PubMed]
- Jeong, J.; Choi, D.-H.; Shin, C.S. Core Strength Training Can Alter Neuromuscular and Biomechanical Risk Factors for Anterior Cruciate Ligament Injury. Am. J. Sports Med. 2021, 49, 183–192. [Google Scholar] [CrossRef] [PubMed]
- Dierks, T.A.; Manal, K.T.; Hamill, J.; Davis, I.S. Proximal and Distal Influences on Hip and Knee Kinematics in Runners With Patellofemoral Pain During a Prolonged Run. J. Orthop. Sports Phys. Ther. 2008, 38, 448–456. [Google Scholar] [CrossRef]
- Willson, J.D.; Dougherty, C.P.; Ireland, M.L.; Davis, I.M. Core Stability and Its Relationship to Lower Extremity Function and Injury. J. Am. Acad. Orthop. Surg. 2005, 13, 316–325. [Google Scholar] [CrossRef]
- Dempsey, A.R.; Elliott, B.C.; Munro, B.J.; Steele, J.; Lloyd, D.G. Whole body kinematics and knee moments that occur during an overhead catch and landing task in sport. Clin. Biomech. 2012, 27, 466–474. [Google Scholar] [CrossRef]
- Jamison, S.T.; Pan, X.; Chaudhari, A.M. Knee moments during run-to-cut maneuvers are associated with lateral trunk positioning. J. Biomech. 2012, 45, 1881–1885. [Google Scholar] [CrossRef]
- Shin, C.S.; Chaudhari, A.; Andriacchi, T.P. The effect of isolated valgus moments on ACL strain during single-leg landing: A simulation study. J. Biomech. 2009, 42, 280–285. [Google Scholar] [CrossRef]
- Shin, C.S.; Chaudhari, A.; Andriacchi, T.P. Valgus Plus Internal Rotation Moments Increase Anterior Cruciate Ligament Strain More Than Either Alone. Med. Sci. Sports Exerc. 2011, 43, 1484–1491. [Google Scholar] [CrossRef]
- Zazulak, B.T.; Hewett, T.E.; Reeves, N.P.; Goldberg, B.; Cholewicki, J. Deficits in Neuromuscular Control of the Trunk Predict Knee Injury Risk. Am. J. Sports Med. 2007, 35, 1123–1130. [Google Scholar] [CrossRef] [PubMed]
- Zazulak, B.T.; Hewett, T.E.; Reeves, N.P.; Goldberg, B.; Cholewicki, J. The Effects of Core Proprioception on Knee Injury. Am. J. Sports Med. 2007, 35, 368–373. [Google Scholar] [CrossRef] [PubMed]
- Dempsey, A.R.; Lloyd, D.G.; Elliott, B.C.; Steele, J.; Munro, B.J. Changing Sidestep Cutting Technique Reduces Knee Valgus Loading. Am. J. Sports Med. 2009, 37, 2194–2200. [Google Scholar] [CrossRef]
- Jamison, S.T.; Mcneilan, R.J.; Young, G.S.; Givens, D.L.; Best, T.M.; Chaudhari, A. Randomized Controlled Trial of the Effects of a Trunk Stabilization Program on Trunk Control and Knee Loading. Med. Sci. Sports Exerc. 2012, 44, 1924–1934. [Google Scholar] [CrossRef]
- Barbado, D.; López-Valenciano, A.; Juan-Recio, C.; Montero, C.; Van Dieën, J.H.; Vera-Garcia, F.J. Trunk Stability, Trunk Strength and Sport Performance Level in Judo. PLoS ONE 2016, 11, e0156267. [Google Scholar] [CrossRef]
- Barbado, D.; Irles-Vidal, B.; Prat-Luri, A.; García-Vaquero, M.P.; Vera-Garcia, F.J. Training intensity quantification of core stability exercises based on a smartphone accelerometer. PLoS ONE 2018, 13, e0208262. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, K.L.; Sosnoff, J.J. Smartphone accelerometry to assess postural control in individuals with multiple sclerosis. Gait Posture 2021, 84, 114–119. [Google Scholar] [CrossRef] [PubMed]
- Reynard, F.; Christe, D.; Terrier, P. Postural control in healthy adults: Determinants of trunk sway assessed with a chest-worn accelerometer in 12 quiet standing tasks. PLoS ONE 2019, 14, e0211051. [Google Scholar] [CrossRef]
- Capecci, M.; Pepa, L.; Verdini, F.; Ceravolo, M.G. A smartphone-based architecture to detect and quantify freezing of gait in Parkinson’s disease. Gait Posture 2016, 50, 28–33. [Google Scholar] [CrossRef]
- Rodríguez-Sanz, J.; Carrasco-Uribarren, A.; Cabanillas-Barea, S.; Hidalgo-García, C.; Fanlo-Mazas, P.; Lucha-López, M.O.; Tricás-Moreno, J.M. Validity and reliability of two Smartphone applications to measure the lower and upper cervical spine range of motion in subjects with chronic cervical pain. J. Back Musculoskelet. Rehabil. 2019, 32, 619–627. [Google Scholar] [CrossRef]
- Guillén-Rogel, P.; Franco-Escudero, C.; Marín, P.J. Test-retest reliability of a smartphone app for measuring core stability for two dynamic exercises. PeerJ 2019, 7, e7485. [Google Scholar] [CrossRef]
- Taunton, J.; Ryan, M.B.; Clement, D.B.; McKenzie, D.C.; Lloyd-Smith, D.R.; Zumbo, B.D. A retrospective case-control analysis of 2002 running injuries. Br. J. Sports Med. 2002, 36, 95–101. [Google Scholar] [CrossRef]
- Chumanov, E.S.; Wall-Scheffler, C.; Heiderscheit, B.C. Gender differences in walking and running on level and inclined surfaces. Clin. Biomech. 2008, 23, 1260–1268. [Google Scholar] [CrossRef] [PubMed]
- Earl, J.E.; Monteiro, S.K.; Snyder, K.R. Differences in Lower Extremity Kinematics Between a Bilateral Drop-Vertical Jump and A Single-Leg Step-down. J. Orthop. Sports Phys. Ther. 2007, 37, 245–252. [Google Scholar] [CrossRef]
- Hewett, T.E.; Ford, K.R.; Myer, G.D.; Wanstrath, K.; Scheper, M. Gender differences in hip adduction motion and torque during a single-leg agility maneuver. J. Orthop. Res. 2006, 24, 416–421. [Google Scholar] [CrossRef] [PubMed]
- Calatayud, J.; Martin, F.; Gargallo, P.; García-Redondo, J.; Colado, J.C.; Marín, P.J. The validity and reliability of a new instrumented device for measuring ankle dorsiflexion range of motion. Int. J. Sports Phys. Ther. 2015, 10, 197–202. [Google Scholar] [PubMed]
- Morales, C.R.; Lobo, C.C.; Sanz, D.R.; Corbalán, I.S.; Ruiz, B.B.R.; López, D.L. The concurrent validity and reliability of the Leg Motion system for measuring ankle dorsiflexion range of motion in older adults. PeerJ 2017, 5, e2820. [Google Scholar] [CrossRef] [PubMed]
- Weeks, B.K.; Carty, C.P.; Horan, S. Kinematic predictors of single-leg squat performance: A comparison of experienced physiotherapists and student physiotherapists. BMC Musculoskelet. Disord. 2012, 13, 207. [Google Scholar] [CrossRef] [PubMed]
- Wyndow, N.; De Jong, A.; Rial, K.; Tucker, K.; Collins, N.; Vicenzino, B.; Russell, T.; Crossley, K. The relationship of foot and ankle mobility to the frontal plane projection angle in asymptomatic adults. J. Foot Ankle Res. 2016, 9, 3. [Google Scholar] [CrossRef] [PubMed]
- Puig-Diví, A.; Escalona-Marfil, C.; Padullés-Riu, J.M.; Busquets, A.; Padullés-Chando, X.; Marcos-Ruiz, D. Validity and reliability of the Kinovea program in obtaining angles and distances using coordinates in 4 perspectives. PLoS ONE 2019, 14, e0216448. [Google Scholar] [CrossRef]
- Da Costa, G.V.; de Castro, M.P.; Sanchotene, C.G.; Ribeiro, D.C.; Fontana, H.D.B.; Ruschel, C. Relationship between passive ankle dorsiflexion range, dynamic ankle dorsiflexion range and lower limb and trunk kinematics during the single-leg squat. Gait Posture 2021, 86, 106–111. [Google Scholar] [CrossRef]
- Munro, A.; Herrington, L.; Carolan, M. Reliability of 2-Dimensional Video Assessment of Frontal-Plane Dynamic Knee Valgus During Common Athletic Screening Tasks. J. Sport Rehabil. 2012, 21, 7–11. [Google Scholar] [CrossRef] [PubMed]
- García-Vaquero, M.P.; Barbado, D.; Juan-Recio, C.; López-Valenciano, A.; Vera-Garcia, F.J. Isokinetic trunk flexion–extension protocol to assess trunk muscle strength and endurance: Reliability, learning effect, and sex differences. J. Sport Health Sci. 2020, 9, 692–701. [Google Scholar] [CrossRef] [PubMed]
- Kosse, N.M.; Caljouw, S.; Vervoort, D.; Vuillerme, N.; Lamoth, C.J.C. Validity and Reliability of Gait and Postural Control Analysis Using the Tri-axial Accelerometer of the iPod Touch. Ann. Biomed. Eng. 2014, 43, 1935–1946. [Google Scholar] [CrossRef]
- Powers, C.M. The Influence of Abnormal Hip Mechanics on Knee Injury: A Biomechanical Perspective. J. Orthop. Sports Phys. Ther. 2010, 40, 42–51. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Task | Familiarisation Session a | First Session a | F | p | d | SEM | ICC3,1 c | |
|---|---|---|---|---|---|---|---|---|
| Units b | Percentage c | |||||||
| BDR | 8.5 ± 2.8 | 8.5 ± 2.5 | 0.01 | 0.92 | −0.02 | 1.1 | 13.0 (9.8–19.6) | 0.84 (0.62–0.94) |
| BDL | 9.2 ± 3.2 | 9.9 ± 3.3 | 1.58 | 0.22 | 0.19 | 1.6 | 17.3 (13.1–25.2) | 0.77 (0.50–0.90) |
| SLDR | 13.0 ± 3.0 | 12.3 ± 2.6 | 1.46 | 0.24 | −0.22 | 1.2 | 9.7 (7.3–14.4) | 0.81 (0.57–0.92) |
| SLDL | 13.0 ± 2.8 | 12.3 ± 2.3 | 2.12 | 0.16 | −0.23 | 1.4 | 11.4 (8.7–16.7) | 0.71 (0.40–0.87) |
| Variables | BD | SLD | DFANK | FPPASLS | HFASLS |
|---|---|---|---|---|---|
| BD | 0.139 | −0.389 * | 0.043 | 0.039 | |
| SLD | −0.316 * | 0.234 | 0.314 * | ||
| DFANK | −0.337 * | 0.322 * | |||
| FPPASLS | 0.849 ** | ||||
| HFASLS |
| Variables | DKV a | Normal a | U Score | p |
|---|---|---|---|---|
| DFANK (cm) | 11.5 (10.5–12.1) | 13.5 (10.7–14.5) | 57.5 | 0.228 |
| BD (mm/s−2) | 8.1 (7.2–9.1) | 8.0 (5.5–10.2) | 84.0 | 0.905 |
| SLD (mm/s−2) | 12.0 (11.3–12.9) | 9.5 (6.6–12.6) | 1135.5 | 0.047 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guillén-Rogel, P.; Barbado, D.; Franco-Escudero, C.; San Emeterio, C.; Marín, P.J. Are Core Stability Tests Related to Single Leg Squat Performance in Active Females? Int. J. Environ. Res. Public Health 2021, 18, 5548. https://doi.org/10.3390/ijerph18115548
Guillén-Rogel P, Barbado D, Franco-Escudero C, San Emeterio C, Marín PJ. Are Core Stability Tests Related to Single Leg Squat Performance in Active Females? International Journal of Environmental Research and Public Health. 2021; 18(11):5548. https://doi.org/10.3390/ijerph18115548
Chicago/Turabian StyleGuillén-Rogel, Paloma, David Barbado, Cristina Franco-Escudero, Cristina San Emeterio, and Pedro J. Marín. 2021. "Are Core Stability Tests Related to Single Leg Squat Performance in Active Females?" International Journal of Environmental Research and Public Health 18, no. 11: 5548. https://doi.org/10.3390/ijerph18115548
APA StyleGuillén-Rogel, P., Barbado, D., Franco-Escudero, C., San Emeterio, C., & Marín, P. J. (2021). Are Core Stability Tests Related to Single Leg Squat Performance in Active Females? International Journal of Environmental Research and Public Health, 18(11), 5548. https://doi.org/10.3390/ijerph18115548