
Missing Diagnoses during the COVID-19 Pandemic: A Year in Review

 ,
,  , ,
, , {kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Population
2.2. The Catalan Healthcare System
2.3. New Diagnoses
2.4. COVID-19 Cases
2.5. Statistical Analysis
2.6. Diagnoses Counterfactuals
3. Results
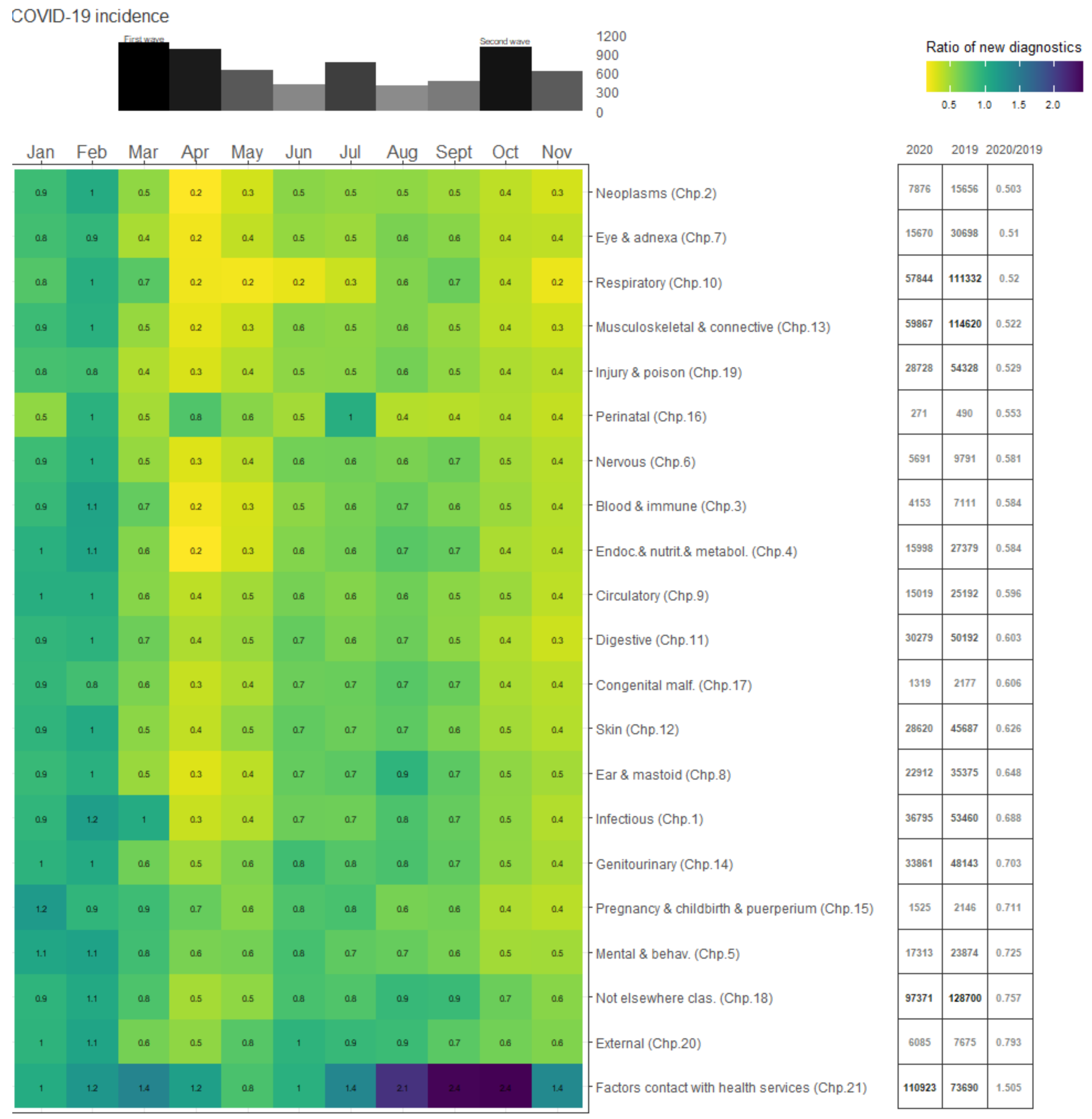
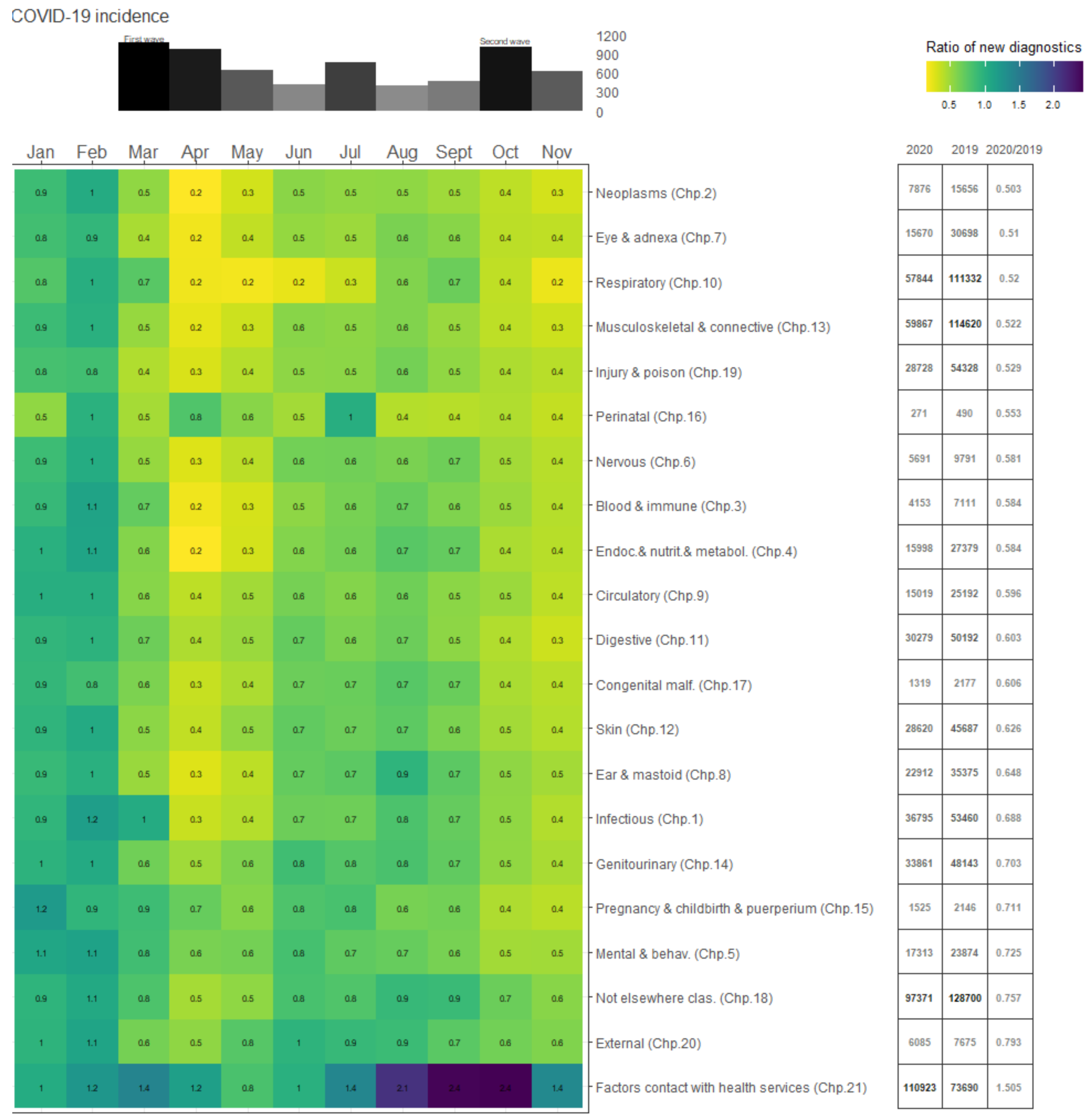
3.1. Main Results
3.2. Cancer Diagnoses
3.3. Socieconomic Gradient
4. Limitations
4.1. Missing Data
4.2. COVID-19 Under-Counting
4.3. Deaths and Missing Diagnoses
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Birkmeyer, J.D.; Barnato, A.; Birkmeyer, N.; Bessler, R.; Skinner, J. The Impact of the COVID-19 Pandemic on Hospital Admissions in the United States. Health Aff. 2020, 39, 2010–2017. [Google Scholar] [CrossRef] [PubMed]
- Bhatt, A.S.; Moscone, A.; McElrath, E.E.; Varshney, A.S.; Claggett, B.L.; Bhatt, D.L.; Januzzi, J.L.; Butler, J.; Adler, D.S.; Solomon, S.D.; et al. Fewer Hospitalizations for Acute Cardiovascular Conditions During the COVID-19 Pandemic. J. Am. Coll. Cardiol. 2020, 76, 280–288. [Google Scholar] [CrossRef] [PubMed]
- De Filippo, O.; D’Ascenzo, F.; Angelini, F.; Bocchino, P.P.; Conrotto, F.; Saglietto, A.; Secco, G.G.; Campo, G.; Gallone, G.; Gaido, L.; et al. Reduced Rate of Hospital Admissions for ACS during Covid-19 Outbreak in Northern Italy. N. Engl. J. Med. 2020, 383, 88–89. [Google Scholar] [CrossRef] [PubMed]
- Sarac, N.J.; Sarac, B.A.; Schoenbrunner, A.R.; Janis, J.E.; Harrison, R.K.; Phieffer, L.S.; Quatman, C.E.; Ly, T.V. A Review of State Guidelines for Elective Orthopaedic Procedures During the COVID-19 Outbreak. J. Bone Jt. Surg. Am. 2020, 102, 942–945. [Google Scholar] [CrossRef] [PubMed]
- Hartnett, K.P.; Kite-Powell, A.; DeVies, J.; Coletta, M.A.; Boehmer, T.K.; Adjemian, J.; Gundlapalli, A.V.; National Syndromic Surveillance Program Community of Practice. Impact of the COVID-19 Pandemic on Emergency Department Visits—United States, January 1, 2019–May 30, 2020. Morb. Mortal. Wkly. Rep. 2020, 69, 699–704. [Google Scholar] [CrossRef] [PubMed]
- Wong, L.E.; Hawkins, J.E.; Langness, S.; Murrell, K.L.; Iris, P.; Sammann, A. Where Are All the Patients? Addressing Covid-19 Fear to Encourage Sick Patients to Seek Emergency Care. 2020. Available online: https://catalyst.nejm.org/doi/full/10.1056/CAT.20.0193 (accessed on 10 December 2020).
- Maringe, C.; Spicer, J.; Morris, M.; Purushotham, A.; Nolte, E.; Sullivan, R.; Rachet, B.; Aggarwal, A. The impact of the COVID-19 pandemic on cancer deaths due to delays in diagnosis in England, UK: A national, population-based, modelling study. Lancet Oncol. 2020, 21, 1023–1034. [Google Scholar] [CrossRef]
- Sud, A.; Torr, B.; Jones, M.E.; Broggio, J.; Scott, S.; Loveday, C.; Garrett, A.; Gronthoud, F.; Nicol, D.L.; Jhanji, S.; et al. Effect of delays in the 2-week-wait cancer referral pathway during the COVID-19 pandemic on cancer survival in the UK: A modelling study. Lancet Oncol. 2020, 21, 1035–1044. [Google Scholar] [CrossRef]
- Tam, C.-C.F.; Cheung, K.-S.; Lam, S.; Wong, Y.T.A.; Yung, A.; Sze, M.; Lam, Y.-M.; Chan, C.; Tsang, T.-C.; Tsui, M.; et al. Impact of Coronavirus Disease 2019 (COVID-19) Outbreak on ST-Segment–Elevation Myocardial Infarction Care in Hong Kong, China. Circ. Cardiovasc. Qual. Outcomes 2020, 13, e006631. [Google Scholar] [CrossRef]
- Dong, E.; Du, H.; Gardner, L. An interactive web-based dashboard to track COVID-19 in real time. Lancet Infect. Dis. 2020, 20, 533–534. [Google Scholar] [CrossRef]
- Williams, R.; Jenkins, D.A.; Ashcroft, D.M.; Brown, B.; Campbell, S.; Carr, M.J.; Cheraghi-Sohi, S.; Kapur, N.; Thomas, O.; Webb, R.T.; et al. Diagnosis of physical and mental health conditions in primary care during the COVID-19 pandemic: A retrospective cohort study. Lancet Public Health 2020, 5, e543–e550. [Google Scholar] [CrossRef]
- National Center for Health Statistics. International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM). 2019. Available online: http://www.cdc.gov/nchs/icd/icd10cm.htm (accessed on 10 December 2020).
- Baltaxe, E.; Cano, I.; Herranz, C.; Barberan-Garcia, A.; Hernandez, C.; Alonso, A.; Arguis, M.J.; Bescos, C.; Burgos, F.; Cleries, M.; et al. Evaluation of integrated care services in Catalonia: Population-based and service-based real-life deployment protocols. BMC Health Serv. Res. 2019, 19, 370. [Google Scholar] [CrossRef]
- Cainzos-Achirica, M.; Capdevila, C.; Vela, E.; Cleries, M.; Bilal, U.; Garcia-Altes, A.; Enjuanes, C.; Garay, A.; Yun, S.; Farre, N.; et al. Individual income, mortality and healthcare resource use in patients with chronic heart failure living in a universal healthcare system: A population-based study in Catalonia, Spain. Int. J. Cardiol. 2019, 277, 250–257. [Google Scholar] [CrossRef]
- Gérvas, J.; Ferna, M.P.; Starfield, B.H. Primary Care, Financing and Gatekeeping in Western Europe. Fam. Pr. 1994, 11, 307–317. [Google Scholar] [CrossRef]
- Marimon-Suñol, S.; Rovira-Barberà, M.; Acedo-Anta, M.; Nozal-Baldajos, M.A.; Guanyabens-Calvet, J. Historia Clínica Compartida en Cataluña. Med. Clin. 2010, 134, 45–48. [Google Scholar] [CrossRef]
- Ministerio de Sanidad. Actualización no 265. Enfermedad por el Coronavirus (COVID-19). Available online: https://www.mscbs.gob.es/en/profesionales/saludPublica/ccayes/alertasActual/nCov/documentos/Actualizacion_265_COVID-19.pdf (accessed on 15 December 2020).
- Agència de Qualitat i Avaluació Sanitàries de Catalunya. Dades Actualitzades SARS-CoV-2. 2020. Available online: https://dadescovid.cat/?tipus=regio&codi=67&id_html=ambit_8&tipus_territori=aga (accessed on 15 December 2020).
- Instituto Nacional de Estadística de España. Population Figures and Demographic Censuses. 2020. Available online: https://www.ine.es/dynt3/inebase/en/index.htm?padre=1894&capsel=1895 (accessed on 15 December 2020).
- Institut Estadística de Catalunya. Number of Municipalities and Population. 2020. Available online: https://www.idescat.cat/pub/?id=aec&n=924&lang=en (accessed on 15 December 2020).
- Søreide, K.; Hallet, J.; Matthews, J.B.; Schnitzbauer, A.A.; Line, P.D.; Lai, P.B.S.; Otero, J.; Callegaro, D.; Warner, S.G.; Baxter, N.N.; et al. Immediate and long-term impact of the COVID-19 pandemic on delivery of surgical services. BJS 2020, 107, 1250–1261. [Google Scholar] [CrossRef]
- Rosenbaum, L. The Untold Toll—The Pandemic’s Effects on Patients without Covid-19. N. Engl. J. Med. 2020, 382, 2368–2371. [Google Scholar] [CrossRef]
- Hanna, T.P.; Evans, G.A.; Booth, C.M. Cancer, COVID-19 and the precautionary principle: Prioritizing treatment during a global pandemic. Nat. Rev. Clin. Oncol. 2020, 17, 268–270. [Google Scholar] [CrossRef]
- Allahwala, U.K.; Denniss, A.R.; Zaman, S.; Bhindi, R. Cardiovascular Disease in the Post-COVID-19 Era—The Impending Tsunami? Heart Lung Circ. 2020, 29, 809–811. [Google Scholar] [CrossRef]
- Lim, M.A.; Huang, I.; Yonas, E.; Vania, R.; Pranata, R. A wave of non-communicable diseases following the COVID-19 pandemic. Diabetes Metab. Syndr. Clin. Res. Rev. 2020, 14, 979–980. [Google Scholar] [CrossRef]
- Dinmohamed, A.G.; Cellamare, M.; Visser, O.; De Munck, L.; Elferink, M.A.G.; Westenend, P.J.; Wesseling, J.; Broeders, M.J.M.; Kuipers, E.J.; Merkx, M.A.W.; et al. The impact of the temporary suspension of national cancer screening programmes due to the COVID-19 epidemic on the diagnosis of breast and colorectal cancer in the Netherlands. J. Hematol. Oncol. 2020, 13, 1–4. [Google Scholar] [CrossRef]
- Nature Medicine Editorial. Keep mental health in mind. Nat. Med. 2020, 26, 631. [Google Scholar] [CrossRef] [PubMed]
- Moreno, C.; Wykes, T.; Galderisi, S.; Nordentoft, M.; Crossley, N.; Jones, N.; Cannon, M.; Correll, C.U.; Byrne, L.; Carr, S.; et al. How mental health care should change as a consequence of the COVID-19 pandemic. Lancet Psychiatry 2020, 7, 813–824. [Google Scholar] [CrossRef]
- Shinan-Altman, S.; Levkovich, I.; Tavori, G. Healthcare utilization among breast cancer patients during the COVID-19 outbreak. Palliat. Support. Care 2020, 18, 385–391. [Google Scholar] [CrossRef] [PubMed]
- Kamrath, C.; Mönkemöller, K.; Biester, T.; Rohrer, T.R.; Warncke, K.; Hammersen, J.; Holl, R.W. Ketoacidosis in Children and Adolescents with Newly Diagnosed Type 1 Diabetes During the COVID-19 Pandemic in Germany. JAMA 2020, 324, 801–804. [Google Scholar] [CrossRef] [PubMed]
- Rabbone, I.; Schiaffini, R.; Cherubini, V.; Maffeis, C.; Scaramuzza, A.; The Diabetes Study Group of the Italian Society for Pediatric Endocrinology and Diabetes. Has COVID-19 Delayed the Diagnosis and Worsened the Presentation of Type 1 Diabetes in Children? Diabetes Care 2020, 43, 2870–2872. [Google Scholar] [CrossRef]
- Zubkiewicz-Kucharska, A.; Seifert, M.; Stępkowski, M.; Noczyńska, A. Diagnosis of type 1 diabetes during the SARS-CoV-2 pandemic: Does lockdown affect the incidence and clinical status of patients? Adv. Clin. Exp. Med. 2021, 30, 127–134. [Google Scholar] [CrossRef]
- Cherubini, V.; Grimsmann, J.M.; Åkesson, K.; Birkebæk, N.H.; Cinek, O.; Dovč, K.; Gesuita, R.; Gregory, J.W.; Hanas, R.; Hofer, S.E.; et al. Temporal trends in diabetic ketoacidosis at diagnosis of paediatric type 1 diabetes between 2006 and 2016: Results from 13 countries in three continents. Diabetologia 2020, 63, 1530–1541. [Google Scholar] [CrossRef]
- Basatemur, E.; Jones, A.; Peters, M.; Ramnarayan, P. Paediatric critical care referrals of children with diabetic ketoacidosis during the COVID-19 pandemic. Arch. Dis. Child. 2021, 106, e21. [Google Scholar] [CrossRef]
- Monaghesh, E.; Hajizadeh, A. The role of telehealth during COVID-19 outbreak: A systematic review based on current evidence. BMC Public Health 2020, 20, 1193. [Google Scholar] [CrossRef]
- Solans, O.; Vidal-Alaball, J.; Cabo, P.R.; Mora, N.; Coma, E.; Simó, J.M.B.; Pérez, E.H.; Saigí-Rubió, F.; Olmos, C.; Piera-Jiménez, J.; et al. Characteristics of citizens and their use of teleconsultation in Primary Care in the Catalan public health system before and during COVID: Retrospective Descriptive Cross-Sectional Study. J. Med Internet Res. 2021, 22, e19149. [Google Scholar] [CrossRef]
- McCall, B. Could telemedicine solve the cancer backlog? Lancet Digit. Health 2020, 2, e456–e457. [Google Scholar] [CrossRef]
- Poppas, A.; Rumsfeld, J.S.; Wessler, J.D. Telehealth Is Having a Moment. J. Am. Coll. Cardiol. 2020, 75, 2989–2991. [Google Scholar] [CrossRef]
- Baena-Díez, J.M.; Barroso, M.; Cordeiro-Coelho, S.I.; Díaz, J.L.; Grau, M. Impact of COVID-19 outbreak by income: Hitting hardest the most deprived. J. Public Health 2020, 42, 698–703. [Google Scholar] [CrossRef]
- Williamson, E.J.; Walker, A.J.; Bhaskaran, K.; Bacon, S.; Bates, C.; Morton, C.E.; Curtis, H.J.; Mehrkar, A.; Evans, D.; Inglesby, P.; et al. Factors associated with COVID-19-related death using OpenSAFELY. Nature 2020, 584, 430–436. [Google Scholar] [CrossRef]
- van Dorn, A.; Cooney, R.E.; Sabin, M.L. COVID-19 exacerbating inequalities in the US. Lancet 2020, 395, 1243–1244. [Google Scholar] [CrossRef]
- Topriceanu, C.-C.; Wong, A.; Moon, J.; Hughes, A.D.; Bann, D.; Chaturvedi, N.; Patalay, P.; Conti, G.; Captur, G. Inequality in access to health and care services during lockdown—Findings from the COVID-19 survey in five UK national longitudinal studies. BMJ 2021, 11, e045813. [Google Scholar]
- Huff, C. Covid-19: Americans afraid to seek treatment because of the steep cost of their high deductible insurance plans. BMJ 2020, 371, m3860. [Google Scholar] [CrossRef]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pifarré i Arolas, H.; Vidal-Alaball, J.; Gil, J.; López, F.; Nicodemo, C.; Saez, M. Missing Diagnoses during the COVID-19 Pandemic: A Year in Review. Int. J. Environ. Res. Public Health 2021, 18, 5335. https://doi.org/10.3390/ijerph18105335
Pifarré i Arolas H, Vidal-Alaball J, Gil J, López F, Nicodemo C, Saez M. Missing Diagnoses during the COVID-19 Pandemic: A Year in Review. International Journal of Environmental Research and Public Health. 2021; 18(10):5335. https://doi.org/10.3390/ijerph18105335
Chicago/Turabian StylePifarré i Arolas, Héctor, Josep Vidal-Alaball, Joan Gil, Francesc López, Catia Nicodemo, and Marc Saez. 2021. "Missing Diagnoses during the COVID-19 Pandemic: A Year in Review" International Journal of Environmental Research and Public Health 18, no. 10: 5335. https://doi.org/10.3390/ijerph18105335
APA StylePifarré i Arolas, H., Vidal-Alaball, J., Gil, J., López, F., Nicodemo, C., & Saez, M. (2021). Missing Diagnoses during the COVID-19 Pandemic: A Year in Review. International Journal of Environmental Research and Public Health, 18(10), 5335. https://doi.org/10.3390/ijerph18105335