
CCOUC Ethnic Minority Health Project: A Case Study for Health EDRM Initiatives to Improve Disaster Preparedness in a Rural Chinese Population

 ,
,  , and
, and
Abstract
1. Introduction
1.1. Improving Disaster Preparedness and Resilience in Communities
1.2. The Ethnic Minority Health Project
2. The Ma’an Qiao Village Programme
2.1. Planning
2.2. Multidisciplinary Approach
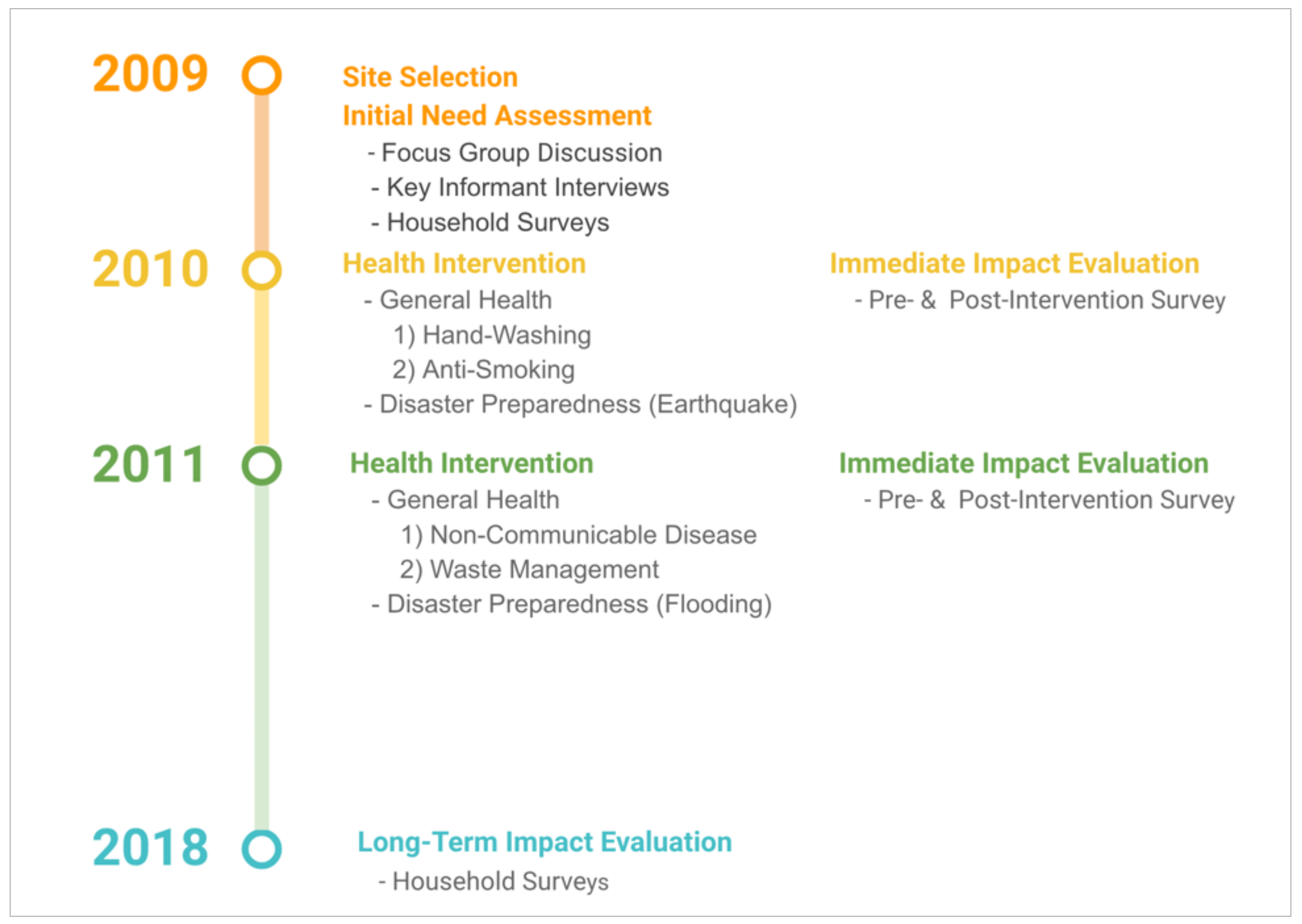
3. Interventions
3.1. Health Education Topics
3.1.1. Hand Hygiene
3.1.2. Smoking Behaviour
3.1.3. Non-Communicable Disease Management
3.1.4. Waste Management
3.1.5. Disaster Preparedness
3.2. Outcome Evaluation
3.2.1. Immediate Outcome Evaluation
3.2.2. Long-Term Outcome Evaluation
4. The EMHP: Achievements and Scaling-Up
4.1. Project Outcome
4.2. Scaling-Up
5. Limitations
6. Recommendations
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- UNDRR. Understanding Risk. 2019. Available online: https://www.undrr.org/building-risk-knowledge/understanding-risk (accessed on 28 February 2021).
- PreventionWeb: The Knowledge Platform for Disaster Risk Reduction. Vulnerability. Available online: https://www.preventionweb.net/disaster-risk/risk/vulnerability/ (accessed on 1 March 2021).
- World Health Organization (WHO). Health Emergency and Disaster Risk Management Framework. World Health Organization. 2019. Available online: https://apps.who.int/iris/handle/10665/326106 (accessed on 28 February 2021).
- Chan, E.Y.Y.; Ho, J.Y.-E.; Huang, Z.; Kim, J.H.; Lam, H.C.Y.; Chung, P.P.W.; Wong, C.K.P.; Liu, S.; Chow, S. Long-Term and Immediate Impacts of Health Emergency and Disaster Risk Management (Health-EDRM) Education Interventions in a Rural Chinese Earthquake-Prone Transitional Village. Int. J. Disaster Risk Sci. 2018, 9, 319–330. [Google Scholar] [CrossRef]
- Hung, K.; Mashino, S.; Chan, E.; MacDermot, M.; Balsari, S.; Ciottone, G.; Della Corte, F.; Dell’Aringa, M.; Egawa, S.; Evio, B.; et al. Health Workforce Development in Health Emergency and Disaster Risk Management: The Need for Evidence-Based Recommendations. Int. J. Environ. Res. Public Health 2021, 18, 3382. [Google Scholar] [CrossRef] [PubMed]
- CRED & UNDRR. Human Cost of Disasters: An Overview of the Last 20 Years 2000–2019. Available online: https://reliefweb.int/report/world/human-cost-disasters-overview-last-20-years-2000-2019 (accessed on 28 February 2021).
- National Bureau of Statistics of China. 2018. Available online: http://www.stats.gov.cn/english/Statisticaldata/AnnualData/ (accessed on 28 February 2021).
- The People’s Republic of China to the United Nations Office at Geneva and Other International Organisations in Switzerland. Regional Autonomy for Ethnic Minorities in China. n.d. Available online: http://www.china-un.ch/eng/rqrd/jblc/t187368.htm (accessed on 28 February 2021).
- Campos, B.C.; Ren, Y.; Petrick, M. The impact of education on income inequality between ethnic minorities and Han in China. China Econ. Rev. 2016, 41, 253–267. [Google Scholar] [CrossRef]
- Liu, X.; Lu, L. Income and Poverty Gaps between Han and Ethnic Minorities in Rural China, 2002 and 2013; Centre for Human Capital and Productivity (CHCP) Working Paper Series; Department of Economics Social Science Centre Western University London: London, ON, Canada, 2017; Available online: https://ir.lib.uwo.ca/cgi/viewcontent.cgi?article=1132&context=economicscibc (accessed on 28 February 2021).
- Chan, E.Y.; Hung, K.K.; Huang, Z.; Wong, C.K.; Lam, H.C.; Ho, H.; Fong, A.; Choi, C.; Lee, J.; Ho, J.Y.; et al. Building Bottom-up Health Emergency and Disaster Management (Health-EDRM) Programs in Disaster Prone and Resource Deficit Context: Lessons Learnt in the Ethnic Minority Health Program for Dai Minority at Ma’an Qiao Village, Sichuan Province China; IRDR Working Paper Series, Integrated Research on Disaster Risk (IRDR) an interdisciplinary body of the International Science Council (ISC); IRDR: Beijing, China, 2019. [Google Scholar] [CrossRef]
- CCOUC. Ethnic Minority Health Project. 2021. Available online: http://www.ccouc.ox.ac.uk/home-5 (accessed on 28 February 2021).
- Chan, E.Y.Y. Building Bottom-Up Health and Disaster Risk Reduction Programmes; Oxford University Press: Oxford, UK, 2018. [Google Scholar]
- Tam, G.; Chan, E.Y.Y.; Liu, S. Planning of a Health Emergency Disaster Risk Management Programme for a Chinese Ethnic Minority Community. Int. J. Environ. Res. Public Health 2019, 16, 1046. [Google Scholar] [CrossRef]
- United States Department of Health and Human Services (USDHHS). Healthy People in Healthy Communities: A Community Planning Guide Using Healthy People 2010; USDHHS: Washington, DC, USA, 2001.
- Li, W.; Zhu, J.; Zhang, Y.; Cao, Y.; Hu, Y.; Fu, L.; Huang, P.; Xie, Y.; Yin, L.; Xu, B. A Fusion Visualization Method for Disaster Information Based on Self-Explanatory Symbols and Photorealistic Scene Cooperation. ISPRS Int. J. Geo-Inf. 2019, 8, 104. [Google Scholar] [CrossRef]
- Li, W.; Zhu, J.; Fu, L.; Zhu, Q.; Xie, Y.; Hu, Y. An augmented representation method of debris flow scenes to improve public perception. Int. J. Geogr. Inf. Sci. 2020, 19, 1–24. [Google Scholar] [CrossRef]
- Chan, E.Y.Y.; Zhu, C.Y.; Lee, P.; Liu, K.S. Training Manual on Health and Disaster Preparedness in Rural China; CCOUC: London, UK, 2016. [Google Scholar]
- Sarabia, M.M.; Kägi, A.; Davison, A.C.; Banwell, N.; Montes, C.; Aebischer, C.; Hostettler, S. The challenges of impact evaluation: Attempting to measure the effectiveness of community-based disaster risk management. Int. J. Disaster Risk Reduct. 2020, 49, 101732. [Google Scholar] [CrossRef]
- National Research Council. Chapter: 5 Building Local Capacity and Accelerating Progress: Resilience from the Bottom Up. Disaster Resilience: A National Imperative. In Disaster Resilience: A National Imperative; The National Academies Press: Washington, DC, USA, 2012; Available online: https://www.nap.edu/read/13457/chapter/7 (accessed on 15 May 2021).
- Chan, E.Y.Y. Bottom-up disaster resilience. Nat. Geosci. 2013, 6, 327–328. [Google Scholar] [CrossRef]
- McNeish, R.; Rigg, K.K.; Tran, Q.; Hodges, S. Community-based behavioral health interventions: Developing strong community partnerships. Eval. Program. Plan. 2019, 73, 111–115. [Google Scholar] [CrossRef]
- Pascapurnama, D.N.; Murakami, A.; Chagan-Yasutan, H.; Hattori, T.; Sasaki, H.; Egawa, S. Integrated health education in disaster risk reduction: Lesson learned from disease outbreak following natural disasters in Indonesia. Int. J. Disaster Risk Reduct. 2018, 29, 94–102. [Google Scholar] [CrossRef]
- The Health Communication Unit at the Centre for Health Promotion, University of Toronto (THCU). Introduction to Health Promotion Program Planning. 2011. Available online: http://www.mentalhealthpromotion.net/resources/introduction-to-health-promotion-program-planning.pdf (accessed on 28 February 2021).
- Bani, I.A. Health needs assessment. J. Fam. Community Med. 2008, 15, 13–20. [Google Scholar]
- Cook, A. Partnership Working across UK Public Services Edinburgh: What Works Scotland. 2015. Available online: http://whatworksscotland.ac.uk/wp-content/uploads/2015/12/WWS-Evidence-Review-Partnership-03-Dec-2015-.pdf. (accessed on 28 February 2021).
- Eljiz, K.; Greenfield, D.; Hogden, A.; Taylor, R.; Siddiqui, N.; Agaliotis, M.; Milosavljevic, M. Improving knowledge translation for increased engagement and impact in healthcare. BMJ Open Qual. 2020, 9, e000983. [Google Scholar] [CrossRef] [PubMed]
- Loss, J.; Brew-Sam, N.; Metz, B.; Strobl, H.; Sauter, A.; Tittlbach, S. Capacity Building in Community Stakeholder Groups for Increasing Physical Activity: Results of a Qualitative Study in Two German Communities. Int. J. Environ. Res. Public Health 2020, 17, 2306. [Google Scholar] [CrossRef] [PubMed]
- Rosenbaum, S.J.D. Principles to Consider for the Implementation of a Community Health Needs Assessment Process; George Washington University: Washington, DC, USA, 2013. [Google Scholar]
- Dennis, S.; Hetherington, S.A.; Borodzicz, J.A.; Hermiz, O.; Zwar, N.A. Challenges to establishing successful partnerships in community health promotion programs: Local experiences from the national implementation of healthy eating activity and lifestyle (HEAL™) program. Health Promot. J. Aust. 2015, 26, 45–51. [Google Scholar] [CrossRef]
- Niekerk, D.V.; Nemakonde, L.D.; Kruger, L.; Forbes-Genade, K. Community-Based Disaster Risk Management. In Handbook of Disaster Research. Handbooks of Sociology and Social Research; Rodríguez, H., Donner, W., Trainor, J., Eds.; Springer: Cham, Switzerland, 2018; pp. 411–429. [Google Scholar] [CrossRef]
- Shaw, R. Community-Based Disaster Risk Reduction. In Oxford Research Encyclopedia of Natural Hazard Science; Oxford University Press: Oxford, UK, 2016. [Google Scholar] [CrossRef]
- Majd, P.M.; Torani, S.; Maroufi, S.S.; Dowlati, M.; Sheikhi, R.A. The importance of education on disasters and emergencies: A review article. J. Educ. Heal Promot. 2019, 8, 85. [Google Scholar] [CrossRef]
- UNICEF. Disaster Risk Reduction and Education. New York. 2011. Available online: https://www.unicef.org/environment/files/DRRandEDbrochure.pdf (accessed on 28 February 2021).
- Dufty, N. The use of social media in countrywide disaster risk reduction public awareness strategies. Aust. J. Emerg. Manag. 2015, 30, 12–15. [Google Scholar]
- Dufty, N. A New Approach to Disaster Education (Paper Presentation). In Proceedings of the International Emergency Management Society (TIEMS) Annual Conference, Manila, Philippines, 13–16 November 2018. [Google Scholar]
- Howard, G.; Bogh, C.; Goldstein, G.; Morgan, J. A Guide for Communities and Community Health Workers; World Health Organization: Geneva, Switzerland, 2002. [Google Scholar]
- Nifa, F.A.A.; Abbas, S.R.; Lin, C.K.; Othman, S.N. Developing a Disaster Education Program for Community Safety and Resilience. Available online: https://aip.scitation.org/doi/abs/10.1063/1.5005338 (accessed on 3 October 2017).
- Li, C.; Liang, W.; Quigley, C.; Zhao, Y.; Yu, L.-F. Earthquake Safety Training through Virtual Drills. IEEE Trans. Vis. Comput. Graph. 2017, 23, 1275–1284. [Google Scholar] [CrossRef]
- Kondo, S.; Hirose, Y.; Shiroshita, H. Risk Communication and Disaster Information. In Science of Societal Safety; Abe, S., Ozawa, M., Kawata, Y., Eds.; Springer: Singapore, 2019; Volume 2. [Google Scholar] [CrossRef]
- Mutasa, S.; Coetzee, C. Exploring the use of experiential learning in promoting the integration of disaster risk reduction into primary school curriculum: A case of Botswana. Jàmbá 2019, 11, 416. [Google Scholar] [CrossRef]
- Pickering, C.J.; O’Sullivan, T.L.; Morris, A.; Mark, C.; McQuirk, D.; Chan, E.Y.; Guy, E.; Chan, G.K.; Reddin, K.; Throp, R.; et al. The Promotion of ‘Grab Bags’ as a Disaster Risk Reduction Strategy. PLoS Curr. 2018, 10. [Google Scholar] [CrossRef]
- World Bank. World Development Report 2016: Digital Dividends. Sector Focus 3: E-Health. 2016, pp. 191–192. Available online: https://www.worldbank.org/en/publication/wdr2016 (accessed on 28 February 2021).
- Poushter, J.; Bishop, C.; Chwe, H. Social Media Use Continues to Rise in Developing Countries but Plateaus across Developed Ones. 2018. Available online: https://www.pewresearch.org/global/2018/06/19/social-media-use-continues-to-rise-in-developing-countries-but-plateaus-across-developed-ones/ (accessed on 28 February 2021).
- China Internet Watch. Statistics: China Internet Users. 2021. Available online: https://www.chinainternetwatch.com/statistics/china-internet-users/ (accessed on 28 February 2021).
- Ren, J.; Liu, C.; Gao, Q.-S.; Yang, L.; Huang, X.; Guo, Q. Use of appropriate healthcare technologies: A cross-sectional study in rural Zhejiang of China. BMC Health Serv. Res. 2015, 15, 295. [Google Scholar] [CrossRef]
- Nkanunye, C.C.; Obiechina, G.O. Health Communication Strategies as Gateway to effective Health Promotion and Well-being. J. Med. Res. Health Educ. 2017, 1, 13. [Google Scholar]
- World Health Organization (WHO). mHealth: Use of Appropriate Digital Technologies for Public Health. World Health Organization. 2018. Available online: https://apps.who.int/gb/ebwha/pdf_files/WHA71/A71_20-en.pdf (accessed on 28 February 2021).
- Centres for Disease Control and Prevention (CDC). CDC Guide to Writing for Social Media. 2015. Available online: https://www.cdc.gov/socialmedia/tools/guidelines/guideforwriting.html (accessed on 28 February 2021).
- Tavakoli, N.; Yarmohammadian, M.; Safdari, R. Role of mhealth in effective response to disaster. Int. J. Health Syst. Disaster Manag. 2015, 3, 129. [Google Scholar] [CrossRef]
- Zhao, J.; Freeman, B.; Li, M. Can Mobile Phone Apps Influence People’s Health Behavior Change? An Evidence Review. J. Med. Internet Res. 2016, 18, e287. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.; Lee, H.; Kim, Y.; Kim, J.; Cho, M.; Jang, J.; Jang, H. Mobile App-Based Health Promotion Programs: A Systematic Review of the Literature. Int. J. Environ. Res. Public Health 2018, 15, 2838. [Google Scholar] [CrossRef]
- Winarni, E.W.; Purwandari, E.P. Disaster Risk Reduction for Earthquake Using Mobile Learning Application to Improve the Students Understanding in Elementary School. Mediterr. J. Soc. Sci. 2018, 9, 205–214. [Google Scholar] [CrossRef]
- Tokyo Metropolitan Government. 2021. Available online: https://www.bousai.metro.tokyo.lg.jp/1005744/index.html (accessed on 28 February 2021).
- Stellefson, M.; Paige, S.R.; Chaney, B.H.; Chaney, J.D. Evolving Role of Social Media in Health Promotion: Updated Responsibilities for Health Education Specialists. Int. J. Environ. Res. Public Health 2020, 17, 1153. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Stakeholders | Sectors | Responsibilities |
|---|---|---|
| CCOUC (Physicians and public health professionals) | Public Health/ Medicine/ Academic and Research |
|
| The Wu Zhi Qiao Charitable Foundation | Architecture/ Housing |
|
| Local Government | Government |
|
| Village Leaders | Local Stakeholders |
|
| University Student Volunteers | Tertiary Education |
|
| 2010 a (n = 110) | 2011 b (n = 171) | 2018 c (n = 71) | |
|---|---|---|---|
| Male to female ratio | 1:1.6 | 1:1.3 | 1:1.4 |
| Age Category (years) | |||
| <45 | Mean = 44.5 Range = 20 to 73 >40 = 58% | 49.7% | 42.3% |
| 45–59 | 26.3% | 31.0% | |
| ≥60 | 24.0% | 26.8% | |
| Educational Attainment | |||
| Non-Literate | 31% | 41.0% | 24.0% |
| Primary School | 53% | 43.3% | 46.5% |
| Junior High School | NA | 12.3% | 21.1% |
| Senior High School | NA | 2.9% | 5.6% |
| Tertiary School | NA | 0.6% | 2.8% |
| Mean Household Size | NA | 3.9 | 4.2 |
| Income per person (RMB) | NA | 4029 | 18,026 |
| Agricultural Sector Occupation | 83% | 88.8% | 94.4% |
| Self-Reported Health Status | |||
| Good | NA | 39.5% | 61.8% |
| Average | NA | NA | 16.2% |
| Poor | NA | NA | 22.1% |
| Types (No. of Respondents) | Outcome Measures Health-Related Beliefs and Knowledge | 2010 & 2011 Interventions | 2018 | |
|---|---|---|---|---|
| Before | After | Evaluation | ||
| Hand hygiene (n = 100) | Believing in the need of handwashing before meal | 88% | 99% | 97% |
| Believing in the need of handwashing after toilet | 90% | 93% | 93% | |
| Knowing the health risks (e.g., diarrhoea) of poor hand hygiene | 85% | 99% (14%↑ p < 0.01) | 87% (12%↓ p < 0.01) | |
| Anti-smoking (n = 98) | Believing that smoking can cause lung cancer | 64% | 94% | 94% |
| Believing that passive smoking is more harmful for children | 80% | 97% | 91% | |
| Waste management (n = 125) | Knowing the health risks of misplaced excreta | 84% | 99% (15%↑ p < 0.01) | - |
| Knowing health risks of misplaced kitchen waste | 81% | 96% (15%↑ p < 0.01) | - | |
| Believing that it is safe to burn different types of wastes together | 67% | 47% (20%↓ p < 0.01) | 47% | |
| Non-communicable diseases management (n = 125) | Knowledge of hypertension | 57% | 85% (28%↑ p < 0.001) | - |
| Knowing the health risks (hypertension) of high salt intake | 71% | 95% (24%↑ p < 0.001) | 81% (14%↓ p < 0.01) | |
| Knowing health risks (diabetics) of higher meat intake | 41% | 79% (35%↑ p < 0.001) | - | |
| Disaster Preparedness (n = 110) | Believing the importance of disaster preparedness | 88% | 95% | 93% |
| Knowing how to prepare a ‘disaster kit’ | 45% | 65% (20%↑ p < 0.05) | - | |
| Intention to prepare a ‘disaster kit’ | 58% | 93% (35%↑ p < 0.001) | 68% (27%↓ p < 0.01) | |
| Being confident in dealing with future disasters | 89% | 95% | 85% (10%↓ p < 0.05) | |
| Knowing how to evacuate from floods | 94% | 98% | 98% | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hung, K.K.C.; MacDermot, M.K.; Chan, E.Y.Y.; Liu, S.; Huang, Z.; Wong, C.S.; Walline, J.H.; Graham, C.A. CCOUC Ethnic Minority Health Project: A Case Study for Health EDRM Initiatives to Improve Disaster Preparedness in a Rural Chinese Population. Int. J. Environ. Res. Public Health 2021, 18, 5322. https://doi.org/10.3390/ijerph18105322
Hung KKC, MacDermot MK, Chan EYY, Liu S, Huang Z, Wong CS, Walline JH, Graham CA. CCOUC Ethnic Minority Health Project: A Case Study for Health EDRM Initiatives to Improve Disaster Preparedness in a Rural Chinese Population. International Journal of Environmental Research and Public Health. 2021; 18(10):5322. https://doi.org/10.3390/ijerph18105322
Chicago/Turabian StyleHung, Kevin K. C., Makiko K. MacDermot, Emily Y. Y. Chan, Sida Liu, Zhe Huang, Chi S. Wong, Joseph H. Walline, and Colin A. Graham. 2021. "CCOUC Ethnic Minority Health Project: A Case Study for Health EDRM Initiatives to Improve Disaster Preparedness in a Rural Chinese Population" International Journal of Environmental Research and Public Health 18, no. 10: 5322. https://doi.org/10.3390/ijerph18105322
APA StyleHung, K. K. C., MacDermot, M. K., Chan, E. Y. Y., Liu, S., Huang, Z., Wong, C. S., Walline, J. H., & Graham, C. A. (2021). CCOUC Ethnic Minority Health Project: A Case Study for Health EDRM Initiatives to Improve Disaster Preparedness in a Rural Chinese Population. International Journal of Environmental Research and Public Health, 18(10), 5322. https://doi.org/10.3390/ijerph18105322