Obstetric Violence in Spain (Part II): Interventionism and Medicalization during Birth

 ,
, 
 , , and
, , and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Design, Population, and Sample
2.2. Data Collection
2.3. Statistical Analysis
3. Results
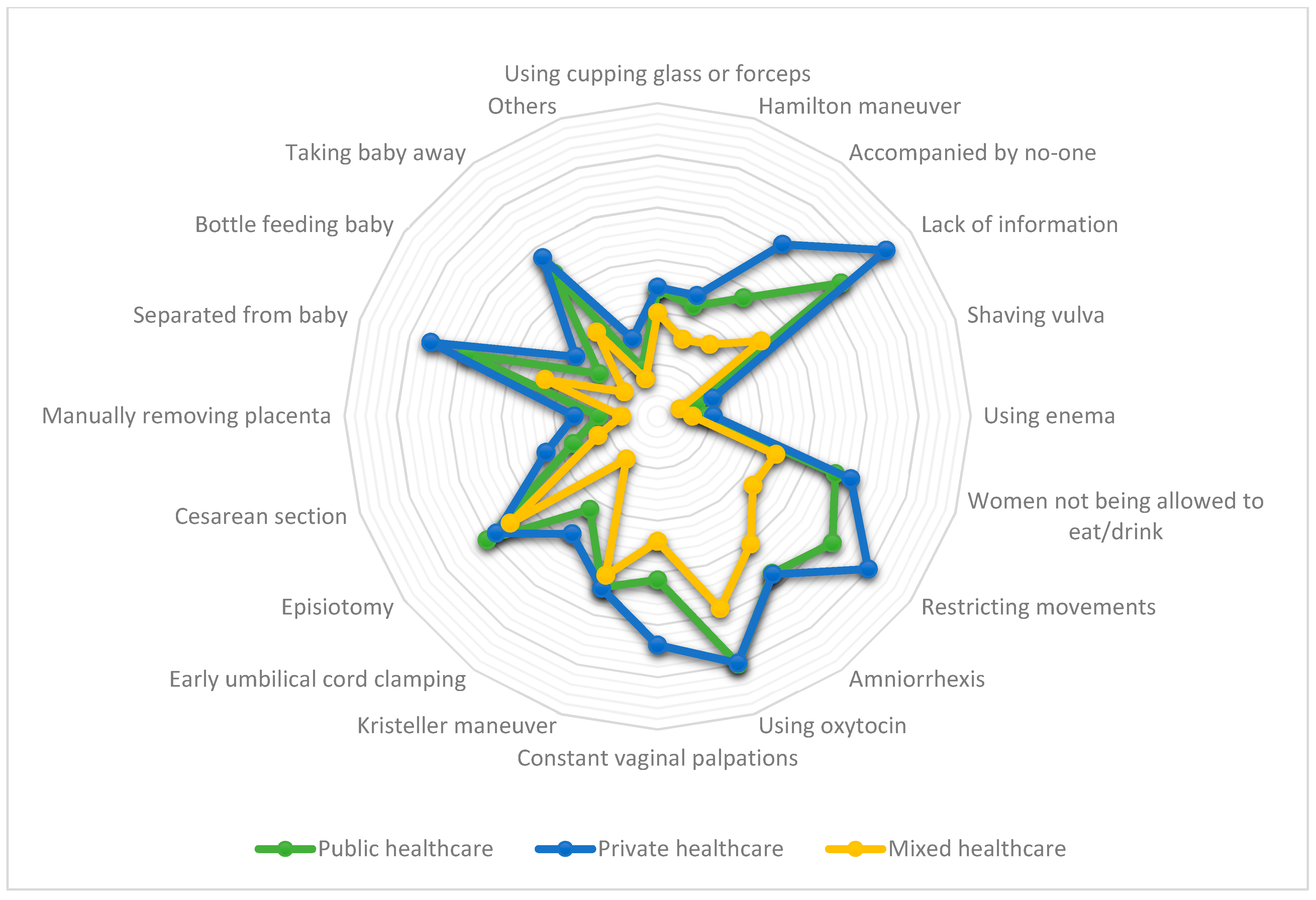
3.1. Satisfaction and Interventions while Giving Birth and Their Relation to Received Healthcare Type
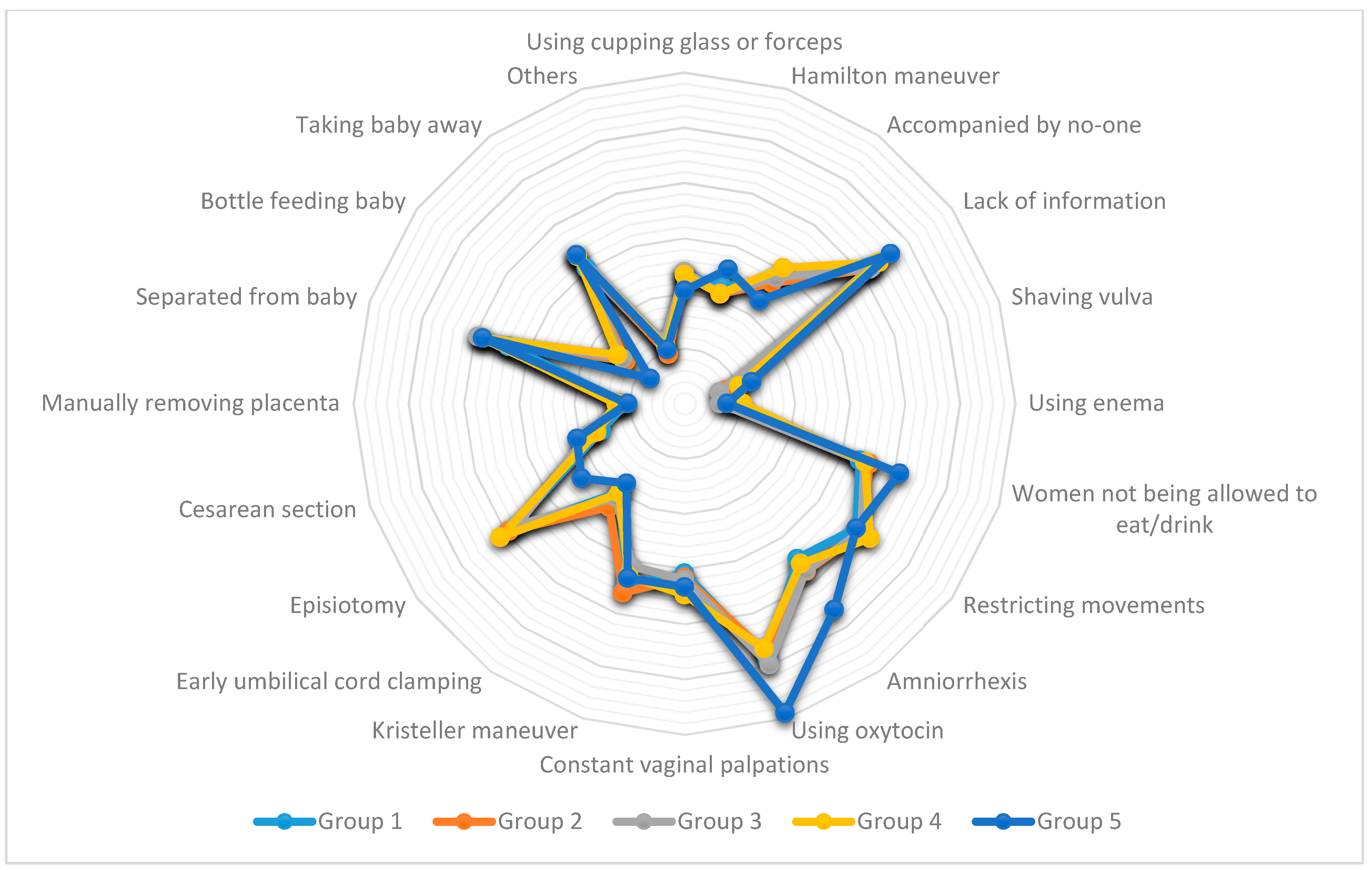
3.2. Interventions While Giving Birth and Their Relation to Cluster Groups
3.3. Obstetric Interventions Related to Women Perceiving OV
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Williams, C.R.; Jerez, C.; Klein, K.; Correa, M.; Belizán, J.M.; Cormick, G. Obstetric Violence: A Latin American Legal Response to Mistreatment during Childbirth. BJOG Int. J. Obstet. Gynaecol. 2018, 125, 1208–1211. [Google Scholar] [CrossRef]
- Pérez D’gregorio, R. Obstetric Violence: A New Legal Term Introduced in Venezuela. Int. J. Gynecol. Obstet. 2010, 111, 201–202. [Google Scholar] [CrossRef]
- Jardim, D.M.B.; Modena, C.M. Obstetric Violence in the Daily Routine of Care and Its Characteristics. Rev. Lat. Am. Enfermagem 2018, 26, e3069. [Google Scholar] [CrossRef]
- Bohren, M.A.; Vogel, J.P.; Hunter, E.C.; Lutsiv, O.; Makh, S.K.; Souza, J.P.; Aguiar, C.; Saraiva Coneglian, F.; Diniz, A.L.A.; Tunçalp, Ö.; et al. The Mistreatment of Women during Childbirth in Health Facilities Globally: A Mixed-Methods Systematic Review. PLoS Med. 2015, 12, e1001847. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Appropriate Technology for Birth. Lancet 1985, 24, 436–437. [Google Scholar]
- Šimonović, D. A Human Rights-Based Approach to Mistreatment and Violence against Women in Reproductive Health Services with a Focus on Childbirth and Obstetric Violence; New York, 2019. Available online: https://digitallibrary.un.org/record/3823698 (accessed on 29 December 2020).
- Vallana Sala, V.V. “It’s Nice to Make Them but Not Have Them”: Analysis of Obstetric Violence during Delivery Care in Colombia. Rev. Ciencias la Salud 2019, 17, 128–144. [Google Scholar] [CrossRef]
- Brandão, T.; Cañadas, S.; Galvis, A.; de los Ríos, M.M.; Meijer, M.; Falcon, K. Childbirth Experiences Related to Obstetric Violence in Public Health Units in Quito, Ecuador. Int. J. Gynecol. Obstet. 2018, 143, 84–88. [Google Scholar] [CrossRef] [PubMed]
- Begley, C.; Sedlicka, N.; Daly, D. Respectful and Disrespectful Care in the Czech Republic: An Online Survey. Reprod. Health 2018, 15, 198. [Google Scholar] [CrossRef] [PubMed]
- Lansky, S.; de Souza, K.V.; de Morais Peixoto, E.R.; Oliveira, B.J.; Diniz, C.S.G.; Vieira, N.F.; de Oliveira Cunha, R.; de Lima Friche, A.A. Obstetric Violence: Influences of the Senses of Birth Exhibition in Pregnant Women Childbirth Experience. Ciência e Saúde Coletiva 2019, 24, 2811–2824. [Google Scholar] [CrossRef]
- Cunha Rodrigues, F.A.; Gama Lira, S.V.; Magalhães, P.H.; Freitas, A.L.e.V.; da Silva Mitros, V.M.; Almeida, P.C. Violência Obstétrica No Processo de Parturição Em Maternidades Vinculadas à Rede Cegonha. Reprod. e Clim. 2017, 32, 78–84. [Google Scholar] [CrossRef]
- Šimonović, D. Report to the United Nations Special Rapporteur on Violence Against Women in Response to Her Call for Submissions Due 17 May 2019; RODA-Parents in Action: Zagreb, Croatia, 2019. Available online: https://www.ohchr.org/Documents/Issues/Women/SR/ReproductiveHealthCare/Roda%20%E2%80%93%20Parents%20in%20Action%20Croatia.pdf (accessed on 29 December 2020).
- Ravaldi, C.; Skoko, E.; Battisti, A.; Cericco, M.; Vannacci, A. Abuse and Disrespect in Childbirth Assistance in Italy: A Community-Based Survey. Eur. J. Obstet. Gynecol. Reprod. Biol. 2018, 224, 208–209. [Google Scholar] [CrossRef] [PubMed]
- Rubashkin, N.; Torres, C.; Escuriet, R.; Dolores Ruiz-Berdún, M. “Just a Little Help”: A Qualitative Inquiry into the Persistent Use of Uterine Fundal Pressure in the Second Stage of Labor in Spain. Birth 2019, 46, 517–522. [Google Scholar] [CrossRef] [PubMed]
- Ministerio de Sanidad Servicios Sociales e Igualdad. Informe Sobre La Atención Al Parto y Nacimiento En El Sistema Nacional de Salud; Madrid, Spain, 2012. Available online: https://www.mscbs.gob.es/organizacion/sns/planCalidadSNS/pdf/InformeFinalEAPN_revision8marzo2015.pdf (accessed on 29 December 2020).
- Salgado Barreira, Á.; Maceira Rozas, M.; López Ratón, M.; Atienza Merino, G. Variabilidad Del Parto En España. Análisis Del Conjunto Mínimo Básico de Datos Al Alta Hospitalaria. Progresos Obstet. y Ginecol. 2010, 53, 215–222. [Google Scholar] [CrossRef]
- Ministerio de Ciencia e Innovación. Labour Care in Healthy Women. Study of Variability and Systematic Review; Ministerio de Ciencia e Innovación: Madrid, Spain, 2009.
- Ministerio de Sanidad Consumo y Bienestar Social. Barómetro Sanitario 2018; Madrid, Spain, 2018. Available online: https://www.mscbs.gob.es/estadEstudios/estadisticas/BarometroSanitario/Barom_Sanit_2018/BS2018_mar.pdf (accessed on 29 December 2020).
- Ministerio de Sanidad. Guía de Práctica Clínica Sobre La Atención Al Parto Normal; Vitoria-Gasteiz, Spain, 2010. Available online: https://www.mscbs.gob.es/organizacion/sns/planCalidadSNS/pdf/equidad/guiaPracClinPartoCompleta.pdf (accessed on 29 December 2020).
- Mena-Tudela, D.; Iglesias-Casás, S.; González-Chordá, V.M.; Cervera-Gasch, A.; Andreu-Pejó, L.; Valero-Chilleron, M.J. Obstetric Violence in Spain (Part I): Women’s Perception and Interterritorial Differences. Int. J. Environ. Res. Public Health 2020, 17, 7726. [Google Scholar] [CrossRef] [PubMed]
- Villarmea, S.; Olza, I.; Recio, A. El Parto Es Nuestro: El Impacto de Una Asociación de Usuarias En La Reforma Del Sistema Obstétrico de España. Dilemata 2015, 7, 157–183. [Google Scholar]
- Pedersen, E.R.; Kurz, J. Using Facebook for Health-Related Research Study Recruitment and Program Delivery. Curr. Opin. Psychol. 2016, 9, 38–43. [Google Scholar] [CrossRef] [PubMed]
- Christensen, T.; Riis, A.H.; Hatch, E.E.; Wise, L.A.; Nielsen, M.G.; Rothman, K.J.; Sørensen, H.T.; Mikkelsen, E.M. Costs and Efficiency of Online and Offline Recruitment Methods: A Web-Based Cohort Study. J. Med. Internet Res. 2017, 19. [Google Scholar] [CrossRef]
- Ministerio de Sanidad Consumo y Bienestar Social. Portal Estadístico. Sistema de Información del Área de Especializada. Available online: https://pestadistico.inteligenciadegestion.mscbs.es/publicoSNS/C/siae/siae/hospitales/actividad-asistencial/actividad-obstetrica (accessed on 6 November 2020).
- Minsierio de Sanidad Consumo y Bienestar Social. Indicadores Clave del Sistema Nacional de Salud. Available online: http://inclasns.msssi.es/main.html (accessed on 30 July 2020).
- World Health Organization. WHO Recommendations: Intrapartum Care for a Positive Childbirth Experience. World Health Organization, 2018. Available online: https://www.who.int/reproductivehealth/publications/intrapartum-care-guidelines/en/ (accessed on 29 December 2020).
- World Health Organization. WHO Statement on Caesarean Section Rates. Geneva, Switzerland, 2015. Available online: https://apps.who.int/iris/bitstream/handle/10665/161442/WHO_RHR_15.02_eng.pdf?sequence=1 (accessed on 29 December 2020).
- Vila-Candel, R.; Martín, A.; Escuriet, R.; Castro-Sánchez, E.; Soriano-Vidal, F.J. Analysis of Caesarean Section Rates Using the Robson Classification System at a University Hospital in Spain. Int. J. Environ. Res. Public Health 2020, 17, 1575. [Google Scholar] [CrossRef]
- Hofmeyr, G.J.; Vogel, J.P.; Cuthbert, A.; Singata, M. Fundal Pressure during the Second Stage of Labour. Cochrane Database Syst. Rev. 2017, 3, CD006067. [Google Scholar] [CrossRef]
- Malvasi, A.; Zaami, S.; Tinelli, A.; Trojano, G.; Montanari Vergallo, G.; Marinelli, E. Kristeller Maneuvers or Fundal Pressure and Maternal/Neonatal Morbidity: Obstetric and Judicial Literature Review. J. Matern. Neonatal Med. 2019, 32, 2598–2607. [Google Scholar] [CrossRef]
- Guillén, F.F. What Is Obstetric Violence? Some Social, Ethical and Legal Aspects. ILEMATA 2015, 7, 113–128. [Google Scholar]
- Borges, M.T. A Violent Birth: Reframing Coerced Procedures During Childbirth as Obstetric Violence. Duke Law J. 2018, 67, 827–862. [Google Scholar] [PubMed]
- Renfrew, M.J.; McFadden, A.; Bastos, M.H.; Campbell, J.; Channon, A.A.; Cheung, N.F.; Silva, D.R.A.D.; Downe, S.; Kennedy, H.P.; Malata, A.; et al. Midwifery and Quality Care: Findings from a New Evidence-Informed Framework for Maternal and Newborn Care. Lancet 2014, 384, 1129–1145. [Google Scholar] [CrossRef]
- Miller, S.; Abalos, E.; Chamillard, M.; Ciapponi, A.; Colaci, D.; Comandé, D.; Diaz, V.; Geller, S.; Hanson, C.; Langer, A.; et al. Beyond Too Little, Too Late and Too Much, Too Soon: A Pathway towards Evidence-Based, Respectful Maternity Care Worldwide. Lancet 2016, 388, 2176–2192. [Google Scholar] [CrossRef]
- Sadler, M.; Santos, M.J.; Ruiz-Berdún, D.; Rojas, G.L.; Skoko, E.; Gillen, P.; Clausen, J.A. Moving beyond Disrespect and Abuse: Addressing the Structural Dimensions of Obstetric Violence. Reprod. Health Matters 2016, 24, 47–55. [Google Scholar] [CrossRef] [PubMed]
- Flores, Y.Y.R.; Ledezma, A.G.M.; Ibarra, L.E.H.; Acevedo, C.E.G. Social Construction of Obstetric Violence of Tenek and Nahuatl Women in Mexico. Rev. Esc. Enferm. 2019, 53, e03464. [Google Scholar] [CrossRef]
- Bowser, D.; Hill, K. Exploring Evidence for Disrespect and Abuse in Facility-Based Childbirth Report of a Landscape Analysis. Harvard School of Public Health: University Research Co., Boston, MA, USA, 2010, doi:10.1624/105812410X514413. Available online: https://cdn1.sph.harvard.edu/wp-content/uploads/sites/2413/2014/05/Exploring-Evidence-RMC_Bowser_rep_2010.pdf (accessed on 29 December 2020).
- Mena-Tudela, D.; González-Chordá, V.M.; Soriano-Vidal, F.J.; Bonanad-Carrasco, T.; Centeno-Rico, L.; Vila-Candel, R.; Castro-Sánchez, E.; Cervera Gasch, Á. Changes in Health Sciences Students’ Perception of Obstetric Violence after an Educational Intervention. Nurse Educ. Today 2020, 88, 104364. [Google Scholar] [CrossRef]
- Mena-Tudela, D.; Cervera-Gasch, Á.; Alemany-Anchel, M.J.; Andreu-Pejó, L.; González-Chordá, V.M. Design and Validation of the PercOV-S Questionnaire for Measuring Perceived Obstetric Violence in Nursing, Midwifery and Medical Students. Int. J. Environ. Res. Public Health 2020, 17, 8022. [Google Scholar] [CrossRef]
- Nutbeam, D. Health Literacy as a Public Health Goal: A Challenge for Contemporary Health Education and Communication Strategies into the 21st Century. Health Promot. Int. 2000, 15, 259–267. [Google Scholar] [CrossRef]
- Diamond-Smith, N.; Treleaven, E.; Murthy, N.; Sudhinaraset, M. Women’s Empowerment and Experiences of Mistreatment during Childbirth in Facilities in Lucknow, India: Results from a Cross-Sectional Study. BMC Pregnancy Childbirth 2017, 17 (Suppl. 2), 335. [Google Scholar] [CrossRef]
- Dennis, M.L.; Benova, L.; Owolabi, O.O.; Campbell, O.M.R. Meeting Need vs. Sharing the Market: A Systematic Review of Methods to Measure the Use of Private Sector Family Planning and Childbirth Services in Sub-Saharan Africa. BMC Health Serv. Res. 2018, 18, 699. [Google Scholar] [CrossRef] [PubMed]
- Campbell, O.M.R.; Benova, L.; Macleod, D.; Baggaley, R.F.; Rodrigues, L.C.; Hanson, K.; Powell-Jackson, T.; Penn-Kekana, L.; Polonsky, R.; Footman, K.; et al. Family Planning, Antenatal and Delivery Care: Cross-Sectional Survey Evidence on Levels of Coverage and Inequalities by Public and Private Sector in 57 Low- and Middle-Income Countries. Trop. Med. Int. Health 2016, 21, 486–503. [Google Scholar] [CrossRef] [PubMed]
- Hirose, A.; Yisa, I.O.; Aminu, A.; Afolabi, N.; Olasunmbo, M.; Oluka, G.; Muhammad, K.; Hussein, J. Technical Quality of Delivery Care in Private- and Public-Sector Health Facilities in Enugu and Lagos States, Nigeria. Health Policy Plan. 2018, 33, 666–674. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Healthcare Type | Feeling about Received Healthcare Type | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Empowered and Satisfied | Unsure, Vulnerable, Guilty, Incapable | Do Not Know/No Answer | Indifferent | ||||||||
| n | % | n | % | n | % | n | % | X2 | df1 | p2 | |
| Public | 3551 | 31.0 | 4728 | 41.3 | 839 | 7.3 | 2330 | 20.4 | 2419.76 | 6 | <0.001 |
| Private | 577 | 31.5 | 1016 | 55.5 | 74 | 4.0 | 163 | 8.9 | 1089.59 | 6 | <0.001 |
| Mixed | 2651 | 62.2 | 713 | 16.7 | 278 | 6.5 | 619 | 14.5 | 913.06 | 6 | <0.001 |
| Total | 6779 | 38.7 | 5467 | 36.8 | 1191 | 6.8 | 3112 | 17.7 | |||
| Unnecessary and/or Painful Procedures | Perceiving OV | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Public | Private | Mixed | |||||||
| Yes % (n) | No % (n) | Yes % (n) | No % (n) | Yes % (n) | No % (n) | X2 | df1 | p2 | |
| Yes | 76.1 (3705) | 23.9 (1161) | 89.8 (906) | 10.2 (103) | 48.8 (466) | 51.2 (489) | 461.16 | 2 | <0.001 |
| No | 11.2 (538) | 88.8 (4266) | 5.8 (38) | 94.2 (619) | 4.3 (121) | 95.7 (2670) | 114.09 | 2 | <0.001 |
| Do not know | 44.1 (220) | 55.9 (279) | 37.5 (21) | 62.5 (35) | 24.7 (36) | 75.3 (110) | 17.95 | 2 | <0.001 |
| Total | 43.9 (4463) | 56.1 (5706) | 56.0 (965) | 44.0 (757) | 16.0 (623) | 84.0 (3269) | |||
| Interventions | Cluster Group | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | ||||||||||
| n | % | n | % | n | % | n | % | n | % | X2 | df1 | p2 | ||
| Using cupping glass or forceps | Yes | 786 | 23.4 | 622 | 23.8 | 355 | 23.9 | 323 | 23.4 | 8 | 20.5 | 0.46 | 4 | 0.977 |
| No | 2569 | 76.6 | 1987 | 73.2 | 1128 | 76.1 | 1057 | 76.6 | 31 | 79.5 | ||||
| Hamilton maneuver | Yes | 749 | 22.3 | 544 | 20.9 | 311 | 21.0 | 288 | 20.9 | 10 | 25.6 | 2.96 | 4 | 0.564 |
| No | 2606 | 77.7 | 2065 | 79.1 | 1172 | 79.0 | 1092 | 79.1 | 29 | 74.4 | ||||
| Accompanied by no-one | Yes | 922 | 27.5 | 704 | 27.0 | 420 | 28.3 | 419 | 30.4 | 9 | 23.1 | 6.12 | 4 | 0.190 |
| No | 2433 | 72.5 | 1905 | 73.0 | 1063 | 71.7 | 961 | 69.6 | 30 | 76.9 | ||||
| Lack of information | Yes | 1414 | 42.1 | 1084 | 41.5 | 618 | 41.7 | 601 | 43.6 | 18 | 46.2 | 1.89 | 4 | 0.756 |
| No | 1941 | 57.9 | 1525 | 58.5 | 865 | 58.3 | 779 | 56.4 | 21 | 53.8 | ||||
| Shaving vulva | Yes | 227 | 6.8 | 212 | 8.1 | 100 | 6.7 | 143 | 10.4 | 5 | 12.8 | 21.74 | 4 | <0.001 |
| No | 3128 | 93.2 | 2394 | 91.9 | 13.83 | 93.3 | 1237 | 89.6 | 34 | 84.7 | ||||
| Using enema | Yes | 332 | 9.9 | 229 | 8.8 | 93 | 6.3 | 146 | 10.6 | 3 | 7.7 | 21.06 | 4 | <0.001 |
| No | 3023 | 90.1 | 2380 | 91.2 | 1390 | 93.7 | 1234 | 89.4 | 36 | 92.3 | ||||
| Women not being allowed to eat/drink | Yes | 1122 | 33.4 | 920 | 35.3 | 509 | 34.3 | 476 | 34.5 | 16 | 41.0 | 2.97 | 4 | 0.563 |
| No | 2233 | 66.6 | 1689 | 64.7 | 974 | 65.7 | 904 | 65.5 | 23 | 59.0 | ||||
| Restricting movements | Yes | 1290 | 38.5 | 1038 | 39.8 | 588 | 39.6 | 574 | 41.6 | 15 | 38.5 | 4.19 | 4 | 0.380 |
| No | 2065 | 61.4 | 1571 | 60.2 | 895 | 60.4 | 806 | 58.4 | 24 | 61.5 | ||||
| Amniorrhexis | Yes | 1166 | 34.8 | 982 | 37.6 | 555 | 37.4 | 495 | 35.9 | 18 | 46.2 | 8.05 | 4 | 0.090 |
| No | 2189 | 65.2 | 1627 | 62.4 | 928 | 62.6 | 885 | 64.1 | 21 | 53.8 | ||||
| Using oxytocin | Yes | 1636 | 48.8 | 1240 | 47.5 | 738 | 49.8 | 644 | 46.7 | 23 | 59.0 | 5.44 | 4 | 0.245 |
| No | 1719 | 51.2 | 1369 | 52.5 | 745 | 50.2 | 736 | 53.3 | 16 | 41.0 | ||||
| Constant vaginal palpations | Yes | 1032 | 30.8 | 825 | 31.6 | 475 | 32.0 | 479 | 34.7 | 13 | 33.3 | 7.16 | 4 | 0.128 |
| No | 2323 | 69.2 | 1784 | 68.4 | 1008 | 68.0 | 901 | 65.3 | 26 | 66.7 | ||||
| Kristeller maneuver | Yes | 1161 | 34.7 | 941 | 36.1 | 459 | 31.0 | 454 | 32.9 | 13 | 33.3 | 12.68 | 4 | 0.015 |
| No | 2192 | 65.3 | 1668 | 63.9 | 1024 | 69.0 | 923 | 67.1 | 26 | 66.7 | ||||
| Early umbilical cord clamping | Yes | 664 | 19.8 | 604 | 23.2 | 312 | 21.0 | 277 | 20.1 | 7 | 17.9 | 11.51 | 4 | 0.025 |
| No | 2691 | 80.2 | 2005 | 76.8 | 1171 | 79.0 | 1103 | 79.9 | 32 | 82.1 | ||||
| Episiotomy | Yes | 1321 | 39.4 | 1026 | 39.3 | 557 | 37.6 | 570 | 41.3 | 9 | 23.1 | 8.52 | 4 | 0.074 |
| No | 2034 | 60.6 | 1583 | 60.7 | 926 | 62.4 | 810 | 58.7 | 30 | 76.9 | ||||
| Cesarean section | Yes | 535 | 15.9 | 457 | 17.5 | 272 | 18.3 | 230 | 16.7 | 8 | 20.5 | 5.46 | 4 | 0.243 |
| No | 2820 | 84.1 | 2152 | 82.5 | 1211 | 81.7 | 1150 | 83.3 | 31 | 79.5 | ||||
| Manually removing placenta | Yes | 354 | 10.6 | 292 | 11.2 | 175 | 11.8 | 171 | 12.4 | 4 | 10.3 | 3.94 | 4 | 0.414 |
| No | 3001 | 89.4 | 2318 | 88.8 | 1308 | 88.2 | 1209 | 87.6 | 35 | 89.7 | ||||
| Separated from baby | Yes | 1128 | 33.6 | 1017 | 39.0 | 584 | 39.4 | 530 | 38.4 | 15 | 38.5 | 26.63 | 4 | <0.001 |
| No | 2227 | 66.4 | 1594 | 61.0 | 899 | 60.6 | 850 | 61.6 | 24 | 61.5 | ||||
| Bottle feeding baby | Yes | 447 | 13.3 | 343 | 13.1 | 206 | 13.9 | 207 | 15.0 | 3 | 7.7 | 4.24 | 4 | 0.374 |
| No | 2908 | 86.7 | 2266 | 86.9 | 1277 | 86.1 | 1176 | 85.0 | 36 | 92.3 | ||||
| Taking baby away | Yes | 1018 | 30.3 | 867 | 33.2 | 496 | 33.4 | 456 | 33.0 | 13 | 33.3 | 8.09 | 4 | 0.088 |
| No | 2337 | 69.7 | 1742 | 66.8 | 987 | 66.6 | 924 | 67.0 | 26 | 66.7 | ||||
| Others | Yes | 325 | 9.7 | 246 | 9.4 | 175 | 11.8 | 149 | 10.8 | 4 | 10.3 | 7.34 | 4 | 0.119 |
| No | 3030 | 90.3 | 2363 | 90.6 | 1305 | 88.2 | 1231 | 89.2 | 35 | 89.7 | ||||
| Factors | Wald | OR 2 (95% CI) | p |
|---|---|---|---|
| Cluster group | 2.796 | - | 0.593 |
| Received healthcare type 1 | 208.594 | - | <0.001 |
| Public | 102.884 | 0.451 (0.387–0.526) | <0.001 |
| Private | 193.914 | 0.173 (0.135–0.221) | <0.001 |
| Unnecessary and/or painful procedures 1 | 219.795 | 0.244 (0.202–0.294) | <0.001 |
| Cupping glass or forceps 1 | 14.63 | 0.702 (0.585–0.841) | <0.001 |
| Hamilton maneuver 1 | 20.992 | 0.656 (0.548–0.786) | <0.001 |
| Accompanied by no-one 1 | 25.713 | 0.639 (0.537–0.759) | <0.001 |
| Lack of information 1 | 131.523 | 0.420 (0.362–0.487) | <0.001 |
| Shaving vulva 1 | 3.792 | 0.728 (0.529–1.002) | 0.051 |
| Using enema | 0.267 | 1.072 (0.823–1.396) | 0.605 |
| Not being allowed to eat/drink | 0.007 | 1.007 (0.858–1.180) | 0.936 |
| Restricting movements 1 | 44.978 | 0.589 (0.505–0.688) | <0.001 |
| Amniorrhexis | 1.669 | 0.907 (0.782–1.052) | 0.196 |
| Using oxytocin | 0.154 | 0.971 (0.840–1.123) | 0.695 |
| Constant palpations 1 | 46.231 | 0.577 (0.492–0.676) | <0.001 |
| Kristeller maneuver 1 | 42.399 | 0.604 (0.519–0.703) | <0.001 |
| Early umbilical cord clamping 1 | 19.402 | 0.640 (0.525–0.781) | <0.001 |
| Episiotomy 1 | 16.555 | 0.723 (0.618–0.845) | <0.001 |
| Cesarean section 1 | 11.642 | 0.701 (0.572–0.860) | 0.001 |
| Manually removing placenta 1 | 5.905 | 0.740 (0.580–0.943) | 0.015 |
| Separated from baby 1 | 10.565 | 0.768 (0.655–0.901) | 0.001 |
| Bottle feeding baby 1 | 32.499 | 0.494 (0.387–0.629) | <0.001 |
| Taking baby away 1 | 5.007 | 0.833 (0.710–0.978) | 0.025 |
| Others 1 | 14.137 | 0.659 (0.530–0.819) | <0.001 |
| Interventions | Received Healthcare Type | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Public Healthcare | Private Healthcare | Mixed Healthcare | ||||||||
| n | % | n | % | n | % | X2 | df1 | p2 | ||
| Using cupping glass or forceps | Yes | 1541 | 24.2 | 282 | 24.7 | 271 | 19.8 | 13.14 | 2 | 0.001 |
| No | 4817 | 75.8 | 858 | 75.3 | 1097 | 80.2 | ||||
| Hamilton maneuver | Yes | 1413 | 22.2 | 277 | 24.3 | 212 | 15.5 | 36.52 | 2 | <0.001 |
| No | 4945 | 77.8 | 863 | 75.7 | 1156 | 84.5 | ||||
| Accompanied by no-one | Yes | 1778 | 28.0 | 464 | 40.7 | 232 | 17.0 | 174.28 | 2 | <0.001 |
| No | 4580 | 72.0 | 676 | 59.3 | 1136 | 83.0 | ||||
| Lack of information | Yes | 2760 | 43.4 | 640 | 56.1 | 335 | 24.5 | 270.69 | 2 | <0.001 |
| No | 3598 | 56.6 | 500 | 43.9 | 1033 | 75.5 | ||||
| Shaving vulva | Yes | 499 | 7.8 | 126 | 11.1 | 62 | 4.5 | 37.29 | 2 | <0.001 |
| No | 5859 | 92.2 | 1014 | 88.9 | 1306 | 95.5 | ||||
| Using enema | Yes | 589 | 9.3 | 122 | 10.7 | 92 | 6.7 | 13.11 | 2 | 0.001 |
| No | 5769 | 90.7 | 1018 | 89.3 | 1276 | 93.3 | ||||
| Women not being allowed to eat/drink | Yes | 2275 | 35.8 | 443 | 38.9 | 325 | 23.8 | 84.16 | 2 | <0.001 |
| No | 4083 | 64.2 | 697 | 61.1 | 1043 | 76.2 | ||||
| Restricting movements | Yes | 2633 | 41.4 | 563 | 49.9 | 309 | 22.6 | 220.02 | 2 | <0.001 |
| No | 3725 | 58.6 | 577 | 50.6 | 1059 | 77.4 | ||||
| Amniorrhexis | Yes | 2374 | 37.3 | 428 | 37.5 | 414 | 30.3 | 25.29 | 2 | <0.001 |
| No | 3984 | 62.7 | 712 | 62.5 | 954 | 69.7 | ||||
| Using oxytocin | Yes | 3182 | 50.0 | 568 | 49.8 | 531 | 38.8 | 58.11 | 2 | <0.001 |
| No | 3176 | 50.0 | 572 | 50.2 | 837 | 61.2 | ||||
| Constant vaginal palpations | Yes | 1995 | 31.4 | 500 | 43.9 | 329 | 24.0 | 114.75 | 2 | <0.001 |
| No | 4363 | 68.6 | 640 | 56.1 | 1039 | 76.0 | ||||
| Kristeller maneuver | Yes | 2195 | 34.5 | 394 | 34.7 | 439 | 32.1 | 3.14 | 2 | 0.208 |
| No | 4163 | 65.5 | 744 | 65.3 | 929 | 67.9 | ||||
| Early umbilical cord clamping | Yes | 1407 | 22.1 | 318 | 27.9 | 139 | 10.2 | 134.32 | 2 | <0.001 |
| No | 4951 | 77.9 | 822 | 72.1 | 1229 | 89.8 | ||||
| Episiotomy | Yes | 2571 | 40.4 | 435 | 38.2 | 477 | 34.9 | 15.33 | 2 | <0.001 |
| No | 3787 | 59.6 | 705 | 61.8 | 891 | 65.1 | ||||
| Cesarean section | Yes | 1082 | 17.0 | 256 | 22.5 | 164 | 12.0 | 48.52 | 2 | <0.001 |
| No | 5276 | 83.0 | 884 | 77.5 | 1204 | 88.0 | ||||
| Manually removing placenta | Yes | 720 | 11.3 | 182 | 16.0 | 94 | 6.9 | 51.75 | 2 | <0.001 |
| No | 5638 | 88.7 | 958 | 84.0 | 1274 | 93.1 | ||||
| Separated from baby | Yes | 2442 | 38.4 | 521 | 45.7 | 311 | 22.7 | 161.99 | 2 | <0.001 |
| No | 3916 | 61.6 | 619 | 54.3 | 1057 | 77.3 | ||||
| Bottle feeding baby | Yes | 877 | 13.8 | 221 | 19.4 | 108 | 7.9 | 70.56 | 2 | <0.001 |
| No | 5481 | 86.2 | 919 | 80.6 | 1260 | 92.1 | ||||
| Taking baby away | Yes | 2150 | 33.8 | 428 | 37.5 | 272 | 19.9 | 117.66 | 2 | <0.001 |
| No | 4208 | 66.2 | 712 | 62.5 | 1096 | 80.1 | ||||
| Others | Yes | 618 | 9.7 | 178 | 15.6 | 103 | 7.5 | 48.96 | 2 | <0.001 |
| No | 5740 | 90.3 | 962 | 84.4 | 1265 | 92.5 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mena-Tudela, D.; Iglesias-Casás, S.; González-Chordá, V.M.; Cervera-Gasch, Á.; Andreu-Pejó, L.; Valero-Chilleron, M.J. Obstetric Violence in Spain (Part II): Interventionism and Medicalization during Birth. Int. J. Environ. Res. Public Health 2021, 18, 199. https://doi.org/10.3390/ijerph18010199
Mena-Tudela D, Iglesias-Casás S, González-Chordá VM, Cervera-Gasch Á, Andreu-Pejó L, Valero-Chilleron MJ. Obstetric Violence in Spain (Part II): Interventionism and Medicalization during Birth. International Journal of Environmental Research and Public Health. 2021; 18(1):199. https://doi.org/10.3390/ijerph18010199
Chicago/Turabian StyleMena-Tudela, Desirée, Susana Iglesias-Casás, Víctor Manuel González-Chordá, Águeda Cervera-Gasch, Laura Andreu-Pejó, and María Jesús Valero-Chilleron. 2021. "Obstetric Violence in Spain (Part II): Interventionism and Medicalization during Birth" International Journal of Environmental Research and Public Health 18, no. 1: 199. https://doi.org/10.3390/ijerph18010199
APA StyleMena-Tudela, D., Iglesias-Casás, S., González-Chordá, V. M., Cervera-Gasch, Á., Andreu-Pejó, L., & Valero-Chilleron, M. J. (2021). Obstetric Violence in Spain (Part II): Interventionism and Medicalization during Birth. International Journal of Environmental Research and Public Health, 18(1), 199. https://doi.org/10.3390/ijerph18010199