Prevalence and Correlates of Asymptomatic Malaria and Anemia on First Antenatal Care Visit among Pregnant Women in Southeast, Tanzania


Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Population
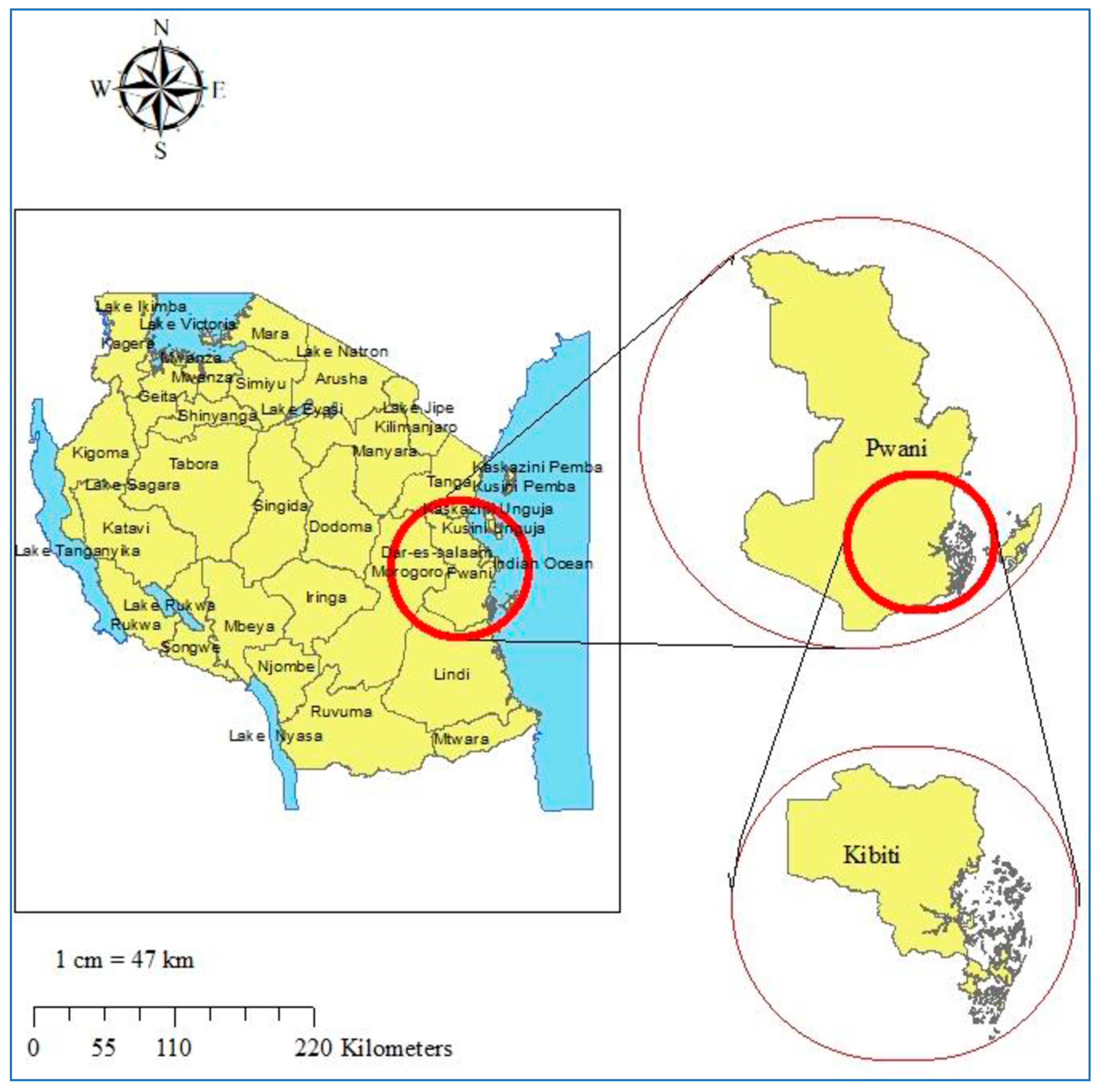
2.2. Study Site
2.3. Data Collection Procedures
2.4. Detection of Malaria Parasites by Rapid Diagnostic Test
2.5. Detection of Malaria Parasites by Real-Time PCR
2.6. Determination of Hemoglobin Concentration
2.7. Study Outcomes
2.8. Data Management and Analysis
2.9. Ethics Approval
3. Results
3.1. Prevalence of Asymptomatic Malaria at First Antenatal Care Visit
3.2. Factors Associated with Asymptomatic Malaria
3.3. Prevalence of Anemia at First Antenatal Care Visit
3.4. Factors Associated with Anemia
3.5. Factors Associated with Hemoglobin Concentration
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- McLean, E.; Cogswell, M.; Egli, I.; Wojdyla, D.; de Benoist, B. Worldwide prevalence of anaemia, WHO Vitamin and Mineral Nutrition Information System, 1993-2005. Public Health Nutr. 2009, 12, 444–454. [Google Scholar] [CrossRef]
- Amek, N.O.; Van Eijk, A.; Lindblade, K.A.; Hamel, M.; Bayoh, N.; Gimnig, J.; Laserson, K.F.; Slutsker, L.; Smith, T.; Vounatsou, P. Infant and child mortality in relation to malaria transmission in KEMRI/CDC HDSS, Western Kenya: Validation of verbal autopsy. Malar. J. 2018, 17, 37. [Google Scholar] [CrossRef] [PubMed]
- Ebeigbe, P.N.; Igberase, G.O. Reasons given by pregnant women for late initiation of antenatal care in the niger delta, Nigeria. Ghana Med. J. 2010, 44, 47–51. [Google Scholar] [PubMed]
- Gebremeskel, F.; Dibaba, Y.; Admassu, B. Timing of first antenatal care attendance and associated factors among pregnant women in Arba Minch Town and Arba Minch District, Gamo Gofa Zone, south Ethiopia. J. Environ. Public Health 2015, 2015, 971506. [Google Scholar] [CrossRef]
- van Eijk, A.M.; Hill, J.; Noor, A.M.; Snow, R.W.; ter Kuile, F.O. Prevalence of malaria infection in pregnant women compared with children for tracking malaria transmission in sub-Saharan Africa: A systematic review and meta-analysis. Lancet Glob. Health 2015, 3, e617–e628. [Google Scholar] [CrossRef]
- Cohee, L.M.; Kalilani-Phiri, L.; Boudova, S.; Joshi, S.; Mukadam, R.; Seydel, K.B.; Mawindo, P.; Thesing, P.; Kamiza, S.; Makwakwa, K.; et al. Submicroscopic malaria infection during pregnancy and the impact of intermittent preventive treatment. Malar. J. 2014, 13, 274. [Google Scholar] [CrossRef]
- Kalilani-Phiri, L.; Thesing, P.C.; Nyirenda, O.M.; Mawindo, P.; Madanitsa, M.; Membe, G.; Wylie, B.; Masonbrink, A.; Makwakwa, K.; Kamiza, S.; et al. Timing of malaria infection during pregnancy has characteristic maternal, infant and placental outcomes. PLoS ONE 2013, 8, e74643. [Google Scholar] [CrossRef]
- Salanti, A.; Dahlback, M.; Turner, L.; Nielsen, M.A.; Barfod, L.; Magistrado, P.; Jensen, A.T.; Lavstsen, T.; Ofori, M.F.; Marsh, K.; et al. Evidence for the involvement of VAR2CSA in pregnancy-associated malaria. J. Exp. Med. 2004, 200, 1197–1203. [Google Scholar] [CrossRef]
- Mlugu, E.M.; Minzi, O.; Asghar, M.; Farnert, A.; Kamuhabwa, A.A.R.; Aklillu, E. Effectiveness of Sulfadoxine-Pyrimethamine for Intermittent Preventive Treatment of Malaria and Adverse Birth Outcomes in Pregnant Women. Pathogens 2020, 9, 207. [Google Scholar] [CrossRef]
- Sumari, D.; Mwingira, F.; Selemani, M.; Mugasa, J.; Mugittu, K.; Gwakisa, P. Malaria prevalence in asymptomatic and symptomatic children in Kiwangwa, Bagamoyo district, Tanzania. Malar. J. 2017, 16, 222. [Google Scholar] [CrossRef]
- Steenkeste, N.; Rogers, W.O.; Okell, L.; Jeanne, I.; Incardona, S.; Duval, L.; Chy, S.; Hewitt, S.; Chou, M.; Socheat, D.; et al. Sub-microscopic malaria cases and mixed malaria infection in a remote area of high malaria endemicity in Rattanakiri province, Cambodia: Implication for malaria elimination. Malar. J. 2010, 9, 108. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Global Technical Strategy for Malaria 2016–2030. 2015. Available online: https://www.who.int/malaria/publications/atoz/9789241564991/en/ (accessed on 10 March 2020).
- World Health Organization. WHO Evidence Review Group: Intermittent Preventive Treatment of Malaria in Pregnancy (IPTp) with Sulfadoxine-Pyrimethamine (SP). Available online: https://www.who.int/malaria/mpac/sep2012/iptp_sp_erg_meeting_report_july2012.pdf (accessed on 1 December 2019).
- Kayentao, K.; Garner, P.; van Eijk, A.M.; Naidoo, I.; Roper, C.; Mulokozi, A.; MacArthur, J.R.; Luntamo, M.; Ashorn, P.; Doumbo, O.K.; et al. Intermittent preventive therapy for malaria during pregnancy using 2 vs 3 or more doses of sulfadoxine-pyrimethamine and risk of low birth weight in Africa: Systematic review and meta-analysis. JAMA 2013, 309, 594–604. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health, Community Development, Gender, Elderly and Children, Ministry of Health Zanzibar, National Bureau of Statistics, Office of Chief Government Statistician and ICF. Tanzania Malaria Indicator Survey 2017. Available online: https://dhsprogram.com/pubs/pdf/MIS31/MIS31.pdf (accessed on 4 December 2019).
- Exavery, A.; Mbaruku, G.; Mbuyita, S.; Makemba, A.; Kinyonge, I.P.; Kweka, H. Factors affecting uptake of optimal doses of sulphadoxine-pyrimethamine for intermittent preventive treatment of malaria in pregnancy in six districts of Tanzania. Malar. J. 2014, 13, 22. [Google Scholar] [CrossRef] [PubMed]
- Baraka, V.; Ishengoma, D.S.; Fransis, F.; Minja, D.T.R.; Madebe, R.A.; Ngatunga, D.; Van Geertruyden, J.-P. High-level Plasmodium falciparum sulfadoxine-pyrimethamine resistance with the concomitant occurrence of septuple haplotype in Tanzania. Malar. J. 2015, 14, 439. [Google Scholar] [CrossRef]
- Ministry of Health and Social Welfare. National Malaria Strategic Plan 2014–2020. Dar es Salaam: Ministry of Health and Social Welfare. 2014. Available online: https://www.out.ac.tz/wp-content/uploads/2019/10/Malaria-Strategic-Plan-2015-2020-1.pdf (accessed on 3 March 2020).
- Kramer, K.; Mandike, R.; Nathan, R.; Mohamed, A.; Lynch, M.; Brown, N.; Mnzava, A.; Rimisho, W.; Lengeler, C. Effectiveness and equity of the Tanzania National Voucher Scheme for mosquito nets over 10 years of implementation. Malar. J. 2017, 16, 255. [Google Scholar] [CrossRef]
- President’s Malaria Initiative Tanzania—Malaria Operational Plan FY 2019. Available online: https://www.pmi.gov/docs/default-source/default-document-library/malaria-operational-plans/fy19/fy-2019-tanzania-malaria-operational-plan.pdf?sfvrsn=3 (accessed on 4 February 2020).
- Mutagonda, R.F.; Minzi, O.M.S.; Massawe, S.N.; Asghar, M.; Farnert, A.; Kamuhabwa, A.A.R.; Aklillu, E. Pregnancy and CYP3A5 Genotype Affect Day 7 Plasma Lumefantrine Concentrations. Drug Metab. Dispos. 2019, 47, 1415–1424. [Google Scholar] [CrossRef]
- Mutagonda, R.F.; Kamuhabwa, A.A.; Minzi, O.M.; Massawe, S.N.; Maganda, B.A.; Aklillu, E. Malaria prevalence, severity and treatment outcome in relation to day 7 lumefantrine plasma concentration in pregnant women. Malar. J. 2016, 15, 278. [Google Scholar] [CrossRef]
- Mutagonda, R.F.; Kamuhabwa, A.A.R.; Minzi, O.M.S.; Massawe, S.N.; Asghar, M.; Homann, M.V.; Farnert, A.; Aklillu, E. Effect of pharmacogenetics on plasma lumefantrine pharmacokinetics and malaria treatment outcome in pregnant women. Malar. J. 2017, 16, 267. [Google Scholar] [CrossRef]
- Ministry of Health, Community Development, Gender, Elderly and Children (MoHCDGEC) [TanzaniaMainland], Ministry of Health (MoH) [Zanzibar]. Tanzania Malaria Operational Plan FY 2015. Available online: https://www.pmi.gov/docs/default-source/default-document-library/malaria-operational-plans/fy-15/fy-2015-tanzania-malaria-operational-plan.pdf (accessed on 1 December 2019).
- Khatib, R.A.; Chaki, P.P.; Wang, D.Q.; Mlacha, Y.P.; Mihayo, M.G.; Gavana, T.; Xiao, N.; Zhou, X.N.; Abdullah, S. Epidemiological characterization of malaria in rural southern Tanzania following China-Tanzania pilot joint malaria control baseline survey. Malar. J. 2018, 17, 292. [Google Scholar] [CrossRef]
- Shokoples, S.E.; Ndao, M.; Kowalewska-Grochowska, K.; Yanow, S.K. Multiplexed real-time PCR assay for discrimination of Plasmodium species with improved sensitivity for mixed infections. J. Clin. Microbiol. 2009, 47, 975–980. [Google Scholar] [CrossRef]
- World Health Organization. Haemoglobin Concentrations for the Diagnosis of Anaemia and Assessment of Severity. Available online: https://apps.who.int/iris/handle/10665/85839 (accessed on 1 December 2019).
- Desai, M.; Gutman, J.; L’Lanziva, A.; Otieno, K.; Juma, E.; Kariuki, S.; Ouma, P.; Were, V.; Laserson, K.; Katana, A.; et al. Intermittent screening and treatment or intermittent preventive treatment with dihydroartemisinin-piperaquine versus intermittent preventive treatment with sulfadoxine-pyrimethamine for the control of malaria during pregnancy in western Kenya: An open-label, three-group, randomised controlled superiority trial. Lancet 2015, 386, 2507–2519. [Google Scholar]
- Kakuru, A.; Jagannathan, P.; Muhindo, M.K.; Natureeba, P.; Awori, P.; Nakalembe, M.; Opira, B.; Olwoch, P.; Ategeka, J.; Nayebare, P.; et al. Dihydroartemisinin-Piperaquine for the Prevention of Malaria in Pregnancy. N. Engl. J. Med. 2016, 374, 928–939. [Google Scholar] [CrossRef]
- Madanitsa, M.; Kalilani, L.; Mwapasa, V.; van Eijk, A.M.; Khairallah, C.; Ali, D.; Pace, C.; Smedley, J.; Thwai, K.L.; Levitt, B.; et al. Scheduled Intermittent Screening with Rapid Diagnostic Tests and Treatment with Dihydroartemisinin-Piperaquine versus Intermittent Preventive Therapy with Sulfadoxine-Pyrimethamine for Malaria in Pregnancy in Malawi: An Open-Label Randomized Controlled Trial. PLoS Med. 2016, 13, e1002124. [Google Scholar]
- Ministry of Health, Community Development, Gender, Elderly and Children, Ministry of Health Zanzibar, National Bureau of Statistics, Office of Chief Government Statistician and ICF. Tanzania Demographic and Health Survey and Malaria Indicator Survey 2015–2016 Final Report. Available online: https://dhsprogram.com/publications/publication-fr321-dhs-final-reports.cfm (accessed on 4 December 2019).
- Bhatt, S.; Weiss, D.J.; Cameron, E.; Bisanzio, D.; Mappin, B.; Dalrymple, U.; Battle, K.E.; Moyes, C.L.; Henry, A.; Eckhoff, P.A.; et al. The effect of malaria control on Plasmodium falciparum in Africa between 2000 and 2015. Nature 2015, 526, 207–211. [Google Scholar] [CrossRef]
- Sherrard-Smith, E.; Griffin, J.T.; Winskill, P.; Corbel, V.; Pennetier, C.; Djenontin, A.; Moore, S.; Richardson, J.H.; Muller, P.; Edi, C.; et al. Systematic review of indoor residual spray efficacy and effectiveness against Plasmodium falciparum in Africa. Nat. Commun. 2018, 9, 4982. [Google Scholar] [CrossRef]
- Chaponda, E.B.; Chandramohan, D.; Michelo, C.; Mharakurwa, S.; Chipeta, J.; Chico, R.M. High burden of malaria infection in pregnant women in a rural district of Zambia: A cross-sectional study. Malar. J. 2015, 14, 380. [Google Scholar] [CrossRef]
- World Health organization. World Malaria Report 2019. Available online: https://www.who.int/publications-detail/world-malaria-report-2019 (accessed on 16 December 2019).
- Aguzie, I.O.N.; Ivoke, N.; Onyishi, G.C.; Okoye, I.C. Antenatal Practices Ineffective at Prevention of Plasmodium falciparum Malaria during Pregnancy in a Sub-Saharan Africa Region, Nigeria. Trop. Med. Infect. Dis. 2017, 2, 15. [Google Scholar] [CrossRef]
- Ouedraogo, S.; Bodeau-Livinec, F.; Briand, V.; Huynh, B.T.; Koura, G.K.; Accrombessi, M.M.; Fievet, N.; Massougbodji, A.; Deloron, P.; Cot, M. Malaria and gravidity interact to modify maternal haemoglobin concentrations during pregnancy. Malar. J. 2012, 11, 348. [Google Scholar] [CrossRef]
- Anchang-Kimbi, J.K.; Nkweti, V.N.; Ntonifor, H.N.; Apinjoh, T.O.; Tata, R.B.; Chi, H.F.; Achidi, E.A. Plasmodium falciparum parasitaemia and malaria among pregnant women at first clinic visit in the mount Cameroon Area. BMC Infect. Dis. 2015, 15, 10. [Google Scholar] [CrossRef]
- Di Renzo, G.C.; Spano, F.; Giardina, I.; Brillo, E.; Clerici, G.; Roura, L.C. Iron deficiency anemia in pregnancy. Womens Health (Lond.) 2015, 11, 891–900. [Google Scholar] [CrossRef]
- Agan, T.; Ekabua, J.; Udoh, A.; Ekanem, E.; Efiok, E.; Mgbekem, M. Prevalence of anemia in women with asymptomatic malaria parasitemia at first antenatal care visit at the University of Calabar Teaching Hospital, Calabar, Nigeria. Int. J. Womens Health 2010, 2, 229–233. [Google Scholar] [CrossRef]
- Kefiyalew, F.; Zemene, E.; Asres, Y.; Gedefaw, L. Anemia among pregnant women in Southeast Ethiopia: Prevalence, severity and associated risk factors. BMC Res. Notes 2014, 7, 771. [Google Scholar] [CrossRef]
- Hinderaker, S.G.; Olsen, B.E.; Bergsjo, P.; Lie, R.T.; Gasheka, P.; Kvale, G. Anemia in pregnancy in the highlands of Tanzania. Acta Obs. Gynecol. Scand. 2001, 80, 18–26. [Google Scholar] [CrossRef]
- Nair, M.; Knight, M.; Robinson, S.; Nelson-Piercy, C.; Stanworth, S.J.; Churchill, D. Pathways of association between maternal haemoglobin and stillbirth: Path-analysis of maternity data from two hospitals in England. BMJ Open 2018, 8, e020149. [Google Scholar] [CrossRef]
- Sukrat, B.; Wilasrusmee, C.; Siribumrungwong, B.; McEvoy, M.; Okascharoen, C.; Attia, J.; Thakkinstian, A. Hemoglobin concentration and pregnancy outcomes: A systematic review and meta-analysis. Biomed. Res. Int. 2013, 2013, 769057. [Google Scholar] [CrossRef]
- Vural, T.; Toz, E.; Ozcan, A.; Biler, A.; Ileri, A.; Inan, A.H. Can anemia predict perinatal outcomes in different stages of pregnancy? Pak. J. Med. Sci. 2016, 32, 1354–1359. [Google Scholar] [CrossRef]
- Berglund, S.K.; Torres-Espínola, F.J.; García-Valdés, L.; Segura, M.T.; Martínez-Zaldívar, C.; Padilla, C.; Rueda, R.; Pérez García, M.; McArdle, H.J.; Campoy, C. The impacts of maternal iron deficiency and being overweight during pregnancy on neurodevelopment of the offspring. Br. J. Nutr. 2017, 118, 533–540. [Google Scholar] [CrossRef]
- Beard, J.L. Why iron deficiency is important in infant development. J. Nutr. 2008, 138, 2534–2536. [Google Scholar] [CrossRef]
- Georgieff, M.K. The role of iron in neurodevelopment: Fetal iron deficiency and the developing hippocampus. Biochem. Soc. Trans. 2008, 36, 1267–1271. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics (n = 819) | n | Frequency (%) | |
|---|---|---|---|
| Maternal age | Mean age (SD), years | 26.5 (7.2) | |
| Adolescent (<20) years | 158 | 19.3 | |
| Young adult (20–34) years | 519 | 63.4 | |
| Adult (≥35) years | 142 | 17.3 | |
| Gravidity | Primigravida | 219 | 26.7 |
| Secundigravida | 181 | 22.1 | |
| Multigravida | 419 | 51.2 | |
| Parity (Number of live children) | Median (range) | 2 (0–9) | |
| Gestational age | Early ANC (≤20) weeks | 356 | 43.5 |
| Late ANC (≥21) weeks | 463 | 56.5 | |
| Insecticide treated bed net use | YES | 656 | 80.1 |
| NO | 163 | 19.9 | |
| Height | Median (range), cm | 151 (140–168) | |
| Weight | Median (range), kg | 54 (38–99) | |
| Body temperature | Median (range), °C | 37 (34–37.4) | |
| Body Mass Index (BMI) | Median (range), kg/cm2 | 23.8 (16.4–40.7) | |
| Characteristic | Asymptomatic Malaria n/N (%) | Univariate Analysis | Multivariate Analysis | ||
|---|---|---|---|---|---|
| OR (95% CI) | p Value | aOR (95% CI) | p Value | ||
| Age | 0.005 | 0.09 | |||
| Adolescent (16–19 years) | 73/158 (46.2) | 1.66 (1.17, 2.37) | 1.48 (0.94, 2.35) | ||
| Adult (≥20 years) | 225/661 (34) | 1 | 1 | ||
| Gravidity | 0.06 | ||||
| Primigravida | 94/219 (42.9) | 1.46 (1.06, 2.00) | 0.019 | 0.92 (0.85, 1.00) | |
| Multigravida | 204/600 (34) | 1 | 1 | ||
| Gestational age (Weeks) | |||||
| Early attendance to ANC (≤20 weeks) | 135/356 (37.9) | 1.12 (0.84, 1.50) | 0.42 | ||
| Late attendance to ANC (≥21 weeks) | 163/463 (35.2) | 1 | |||
| ITN use | |||||
| YES | 234/656 (35.7) | 0.85 (0.60, 1.21) | 0.36 | ||
| NO | 64/163 (39.2) | 1 | |||
| * BMI median (range) kg/m2 | 23.8 (16.4–40.7) | 0.98 (0.94, 1.02) | 0.31 | ||
| Anemia | |||||
| Severe & moderate anemia | 129/315 (41) | 1.49 (1.05, 2.10) | 0.024 | 1.39 (0.98, 1.97) | 0.07 |
| Mild anemia | 87/246 (35.4) | 1.17 (0.81, 1.70) | 0.40 | 1.13 (0.78, 1.64) | 0. 51 |
| No anemia | 82/258 (31.8) | 1 | 1 | ||
| Characteristic | Anemia n/N (%) | Univariate Analysis | Multivariate Analysis | ||
|---|---|---|---|---|---|
| OR (95% CI) | p Value | aOR (95% CI) | p Value | ||
| Age | |||||
| Adolescent (16–19 years) | 127/158 (80.4) | 2.14 (1.40, 3.28) | <0.001 | 1.35 (0.78, 2.32) | |
| Adult (≥20 years) | 434/661 (65.7) | 1 | 1 | 0.28 | |
| Gravidity | |||||
| Primigravida | 176/219 (80.4) | 2.29 (1.57, 3.32) | <0.001 | 1.96 (1.22, 3.13) | 0.005 |
| Multigravida | 385/600 (64.4) | 1 | 1 | ||
| Gestational age | |||||
| Early attendance to ANC (≤20 weeks) | 35/356 (66) | 0.82 (0.61, 1.10) | 0.18 | 0.72 (0.53, 0.98) | 0.035 |
| Late attendance to ANC (≥21 weeks) | 326/463 (70.4) | 1 | 1 | ||
| ITN use | |||||
| YES | 448/656 (68.3) | 0.96 (0.67, 1.39) | 0.84 | ||
| NO | 113/163 (69.3) | 1 | |||
| * BMI median (range) kg/m2 | 23.8 (16.4–40.7) | 0.97 (0.93, 1.01) | 0.11 | 0.97 (0.93, 1.01) | 0.19 |
| Characteristic | Univariate Analysis | Multivariate Analysis | ||||
|---|---|---|---|---|---|---|
| Beta Coefficient [95% CI] | t | p Value | Beta Coefficient [95% CI] | t | p Value | |
| Age (Years) | 0.03 (0.02, 0.04) | 4.36 | <0.001 | 0.01 (−0.01, 0.02) | 0.88 | 0.38 |
| * Gravidity | <0.001 | |||||
| Multigravida | 0.64 (0.42,0.86) | 5.77 | 0.53 (0.27, 0.80) | 3.95 | <0.001 | |
| Primigravida | 1 | 1 | ||||
| Gestational age (Weeks) | −0.01 (−0.03, 0.02) | −0.27 | 0.79 | |||
| * ITN use | 0.96 | |||||
| YES | 1 | |||||
| NO | −0.01 (−0.25,0.24) | −0.05 | ||||
| BMI | 0.04 (0.01, 0.07) | 3.05 | 0.002 | 0.03 (0.01, 0.06) | 2.49 | 0.013 |
| * Asymptomatic Malaria | 0.025 | |||||
| YES | −0.23 (−0.44, −0.03) | −0.17 (−0.37, 0.03) | ||||
| NO | 1 | −2.25 | 1 | 1.65 | 0.09 | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mlugu, E.M.; Minzi, O.; Kamuhabwa, A.A.R.; Aklillu, E. Prevalence and Correlates of Asymptomatic Malaria and Anemia on First Antenatal Care Visit among Pregnant Women in Southeast, Tanzania. Int. J. Environ. Res. Public Health 2020, 17, 3123. https://doi.org/10.3390/ijerph17093123
Mlugu EM, Minzi O, Kamuhabwa AAR, Aklillu E. Prevalence and Correlates of Asymptomatic Malaria and Anemia on First Antenatal Care Visit among Pregnant Women in Southeast, Tanzania. International Journal of Environmental Research and Public Health. 2020; 17(9):3123. https://doi.org/10.3390/ijerph17093123
Chicago/Turabian StyleMlugu, Eulambius M., Omary Minzi, Appolinary A. R. Kamuhabwa, and Eleni Aklillu. 2020. "Prevalence and Correlates of Asymptomatic Malaria and Anemia on First Antenatal Care Visit among Pregnant Women in Southeast, Tanzania" International Journal of Environmental Research and Public Health 17, no. 9: 3123. https://doi.org/10.3390/ijerph17093123
APA StyleMlugu, E. M., Minzi, O., Kamuhabwa, A. A. R., & Aklillu, E. (2020). Prevalence and Correlates of Asymptomatic Malaria and Anemia on First Antenatal Care Visit among Pregnant Women in Southeast, Tanzania. International Journal of Environmental Research and Public Health, 17(9), 3123. https://doi.org/10.3390/ijerph17093123