A Legal and Forensic Medicine Approach to Police Physical Intervention Techniques in High-Risk Situations

 ,
,  ,
,  and
and 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Materials and Methods
2.1. Training Manuals
2.2. Simulation of High-Risk Situations
- A hooking punch. In this first scenario, the opponent stood in front of the police and tried to punch him in the face.
- A knife blow. The second scenario recreated the typical situation where a criminal is holding a sharp knife. After the police officer asked him to throw the knife away and calm down, the criminal who is cornered, tries to stab the knife on the police abdomen.
- A blunt object blow. In this last situation the criminal tried to hit the policeman with a blunt object blow like a baseball bat.
3. Results and Discussion
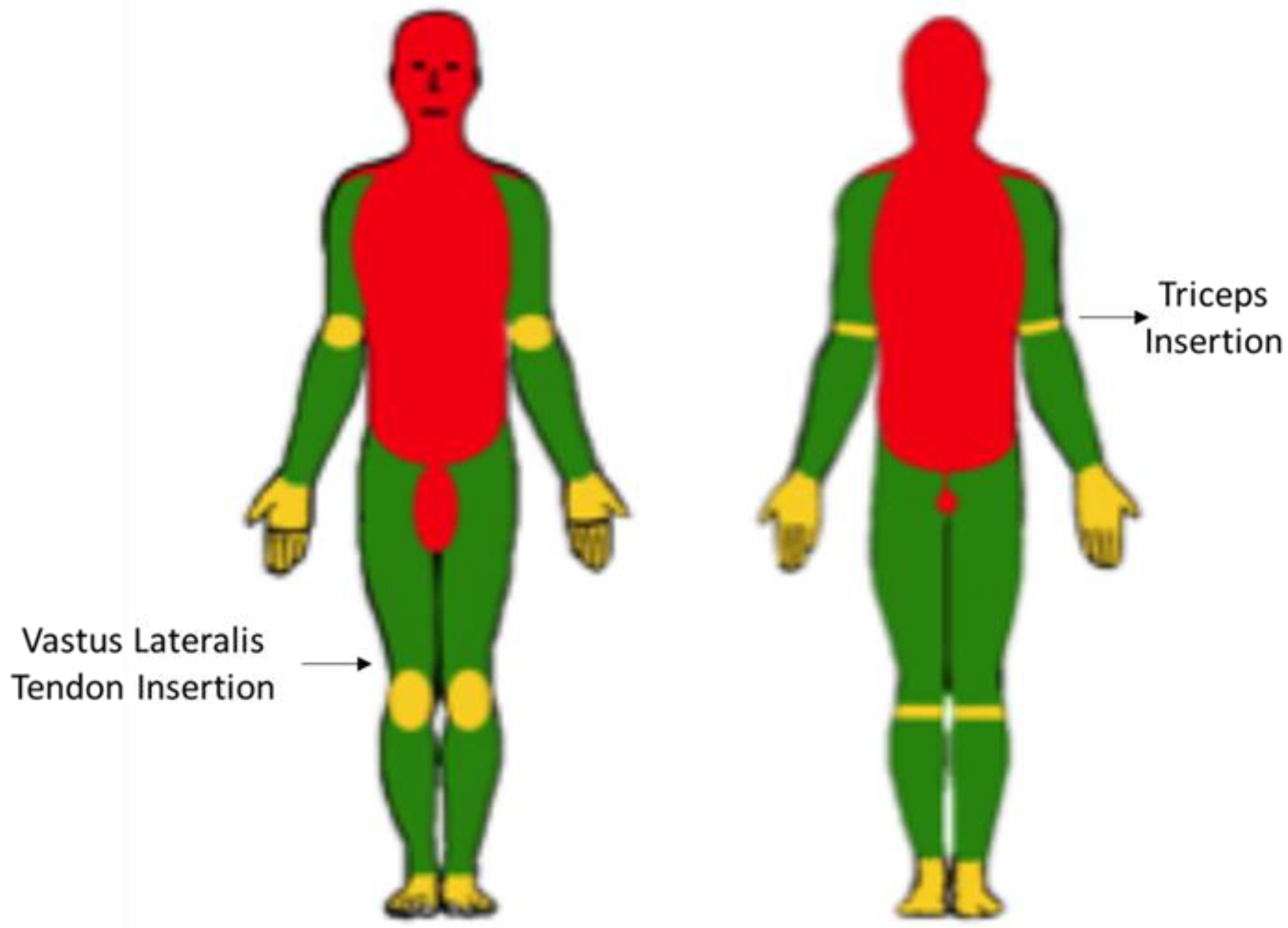
3.1. Injury-Based Analysis of Common Police PITs
3.2. The Principles of Congruence, Opportunity and Proportionality
3.3. Physical Intervention Techniques Based on Operational Tactical Procedures
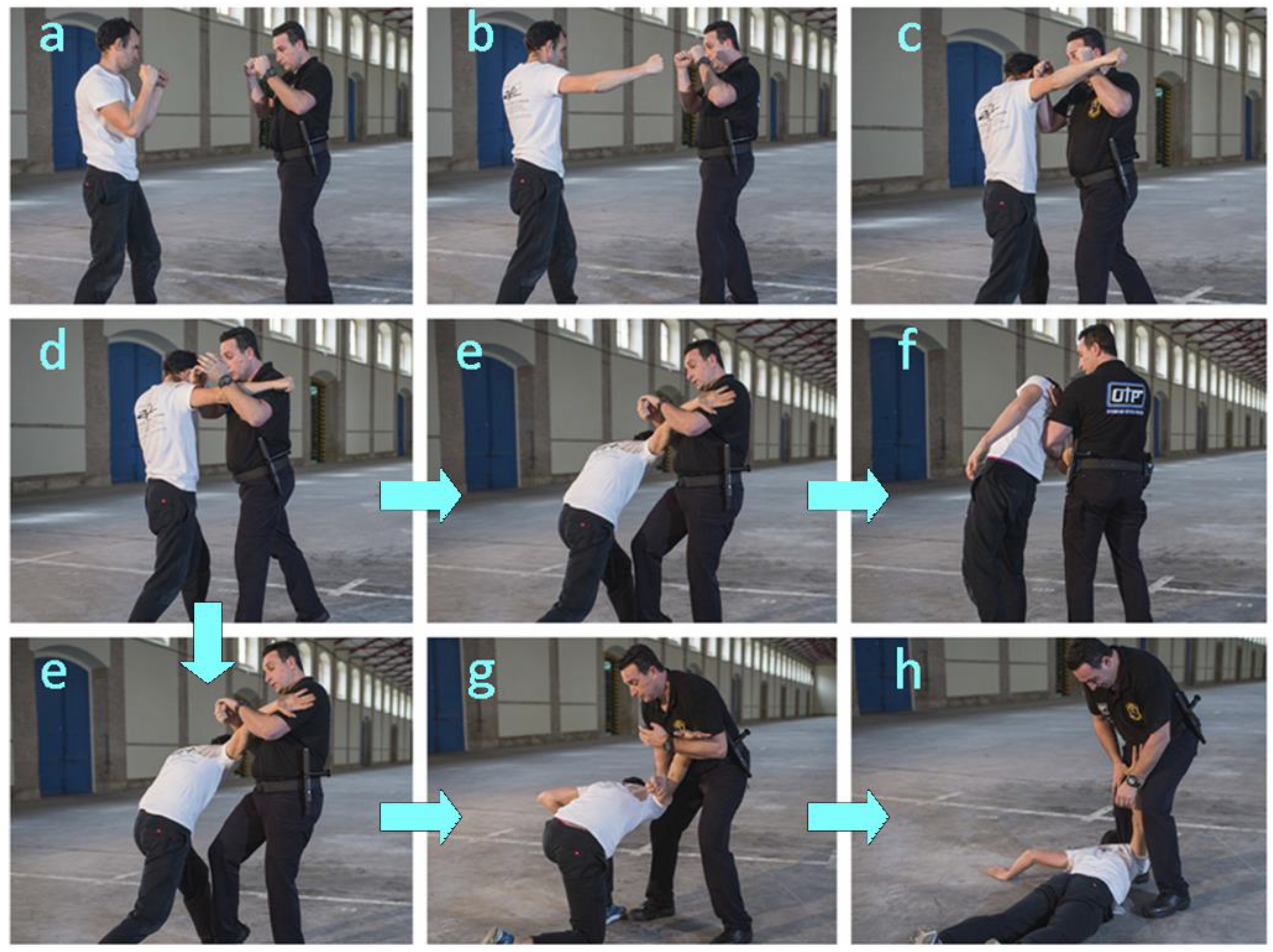
3.3.1. Technique 1. Response to a Hooked Punch
- –
- Step 1. The officer faces the opponent in the guard stance (Figure 2a).
- –
- –
- Step 3. The officer releases the arm he previously used to block the opponent’s arm (Figure 2d).
- –
- Step 4. The officer’s previously released arm is used to grab the opponent break his balance with the help of a knee blow on the opponent’s backward leg, in particular on the frontal area of the thigh (Figure 2e).
- –
- Step 5. The opponent’s is subdued in either of two different ways depending on his aggressiveness:
- 5A. While standing (Figure 2f). The officer controls the opponent by using his forearm to exert strong pressure on the opponent’s elbow and also to prop himself up in order to lower the elbow to his own hip level.
- 5B. On the ground (in one or two steps). The officer continues to control the opponent with the same forearm in order to lower it and keep it bent, still under control, at the officer’s knee level (Figure 2g) while exerting further pressure with the forearm to take the opponent to the ground (Figure 2h).
3.3.2. Technique 2. Response to a Knife Blow
- –
- Step 1. The officer adopts the guard stance while facing the opponent, who is holding a knife (Figure 3a).
- –
- Step 2. The officer uses one forearm to block the arm holding the knife (Figure 3b).
- –
- Step 3. The officer approaches the opponent and uses his free forearm to block the opponent’s free elbow (Figure 3c).
- –
- Step 4. Once the opponent is controlled, his balance is broken by kneeing on the backward leg (Figure 3d).
- –
- Step 5. Subduing the opponent on the ground. The officer controls the opponent by using his forearm to exert strong pressure on the opponent’s elbow while propping himself up in order to lower the elbow to his own hip level. Then, the officer continues to use his forearm in order to further lower the opponent until he reaches the ground (Figure 3e).
3.3.3. Technique 3. Response to a Blunt Object Blow
- –
- Step 1. The officer adopts the guard stance while facing the opponent, who is holding a blunt object as a weapon (Figure 4a).
- –
- Step 2. The officer approaches the opponent from a side, moves his left leg forward and uses his left forearm to block the opponent’s blow (Figure 4b).
- –
- Step 3. While grabbing the opponent with his left hand, the officer uses his right forearm to hit the opponent’s elbow (Figure 4c).
- –
- Step 4. The officer uses his right forearm to exert pressure on the opponent’s triceps in order to gradually drive him to the ground (Figure 4d).
- –
- Step 5. The opponent is subdued on the ground similarly as with Techniques 2 and 3 (Figure 4e).
4. Conclusions
5. Patents
Author Contributions
Funding
Conflicts of Interest
References
- Mckee, A.C.; Cantu, R.C.; Nowinski, C.J.; Hedley-Whyte, E.T.; Gavett, B.E.; Budson, A.E.; Santini, V.E.; Lee, H.S.; Kubilus, C.A.; Sern, R.A.; et al. Chronic traumatic encephalopathy in athletes: Progressive tauopathy after repetitive head injury. J. Neuropathol. Exp. Neurol. 2009, 68, 709–735. [Google Scholar] [CrossRef] [PubMed]
- Langlois, J.A.; Rutland-Brown, W.; Wald, M.M. The epidemiology and impact of traumatic brain injury: A brief overview. J. Head Trauma Rehab. 2006, 21, 375–378. [Google Scholar] [CrossRef] [PubMed]
- Thurman, D.J.; Branche, C.M.; Sniezek, J.E. The epidemiology of sports-related traumatic brain injuries in the United States: Recent developments. J. Head Trauma Rehab. 1998, 13, 1–8. [Google Scholar] [CrossRef]
- Salehi, A.; Zhang, J.H.; Obenaus, A. Response of the cerebral vasculature following traumatic brain injury. J. Cereb. Blood Flow Metab. 2017, 37, 2320–2339. [Google Scholar] [CrossRef] [PubMed]
- Logsdon, A.F.; Lucke-Wold, B.P.; Turner, R.C.; Huber, J.D.; Rosen, C.L.; Simpkins, J.W. Role of microvascular disruption in brain damage from traumatic brain injury. Compr. Physiol. 2015, 5, 1147–1160. [Google Scholar] [CrossRef] [PubMed]
- Saboe, L.A.; Reid, D.C.; Davis, L.A.; Warren, S.A.; Grace, M.G. Spine trauma and associated injuries. J. Trauma Inj. Infect. Crit. Care 1991, 31, 43–48. [Google Scholar] [CrossRef]
- Pickett, W.; Simpson, K.; Walker, J.; Brison, R.J. Traumatic spinal cord injury in Ontario, Canada. J. Trauma 2003, 55, 1070–1076. [Google Scholar] [CrossRef]
- Furlan, J.C.; Sakakibara, B.M.; Miller, W.C.; Krassioukov, A.V. Global incidence and prevalence of traumatic spinal cord injury. Can. J. Neurol. Sci. 2013, 40, 456–464. [Google Scholar] [CrossRef]
- Fakhry, S.M.; Jaques, P.F.; Proctor, H.J. Cervical vessel injury after blunt trauma. J. Vasc. Surg. 1988, 8, 501–508. [Google Scholar] [CrossRef]
- Phillips, A.A.; Krassioukov, A.V.; Ainslie, P.N.; Warburton, D.E.R. Baroreflex function after spinal cord injury. J. Neurotraum. 2012, 29, 2431–2445. [Google Scholar] [CrossRef]
- O’Kane, J.W. Syncope following neck trauma in a football player. Phys. Sportsmed. 2001, 29, 37–41. [Google Scholar] [CrossRef]
- Kochhar, T.; Back, D.L.; Mann, B.; Skinner, J. Risk of cervical injuries in mixed martial arts. Br. J. Sports Med. 2005, 39, 444–447. [Google Scholar] [CrossRef] [PubMed]
- Morley, C.A.; Sutton, R. Carotid sinus syncope. Int. J. Cardiol. 1984, 6, 287–293. [Google Scholar] [CrossRef]
- Conway, D.; Urquhart, C.S. Airway trauma. Anaesth. Intensive Care 2017, 18, 199–201. [Google Scholar] [CrossRef]
- Corneille, M.G.; Stewart, R.M.; Cohn, S.M. Upper airway injury and its management. Semin. Thorac. Cardiovasc. Surg. 2008, 20, 8–12. [Google Scholar] [CrossRef] [PubMed]
- Demetriades, D.; Salim, A.; Brown, C.; Martin, M.; Rhee, P. Neck injuries. Curr. Probl. Surg. 2007, 44, 13–85. [Google Scholar] [CrossRef]
- Erdogan, B.; Erdogan, M.O.; Colak, S.; Kibici, O.; Bozan, K.; Alper, B. An isolated hyoid bone fracture caused by blunt trauma to the neck. J. Pak. Med. Assoc. 2015, 65, 1233–1234. [Google Scholar]
- Jehng, Y.M.; Lee, F.T.T.; Pai, Y.C.; Choi, W.M. Hyoid bone fracture caused by blunt neck trauma. J. Acute Med. 2012, 2, 83–84. [Google Scholar] [CrossRef]
- Levine, E.; Taub, P.J. Hyoid bone fractures. Mt. Sinai J. Med. 2006, 73, 1015–1018. [Google Scholar]
- Moya, A.; Sutton, R.; Ammirati, F.; Blanc, J.J.; Brignole, M.; Dahm, J.B.; Deharo, J.C.; Gajek, J.; Gjesdal, K.; Krahn, A.; et al. Guidelines for the diagnosis and management of syncope (version 2009). Eur. Heart J. 2009, 30, 2631–2671. [Google Scholar] [CrossRef]
- Estañol, B.; Porras Betancourt, M.; Sánchez Torres, G.; Martínez Memije, R.; Infante, O.; Sentíes Madrid, H. Neural control of the peripheral circulation and blood pressure. Arch. Cardiol. Mex. 2009, 79 (Suppl. 2), 109–116. [Google Scholar]
- Wang, N.D.; Stevens, M.H.; Doty, D.B.; Hammond, E.H. Blunt chest trauma: An experimental model for heart and lung contusion. J. Trauma 2003, 54, 744–749. [Google Scholar] [CrossRef]
- Link, M.S. Commotio cordis: Ventricular fibrillation triggered by chest impact-induced abnormalities in repolarization. Circ. Arrhythm. Electrophysiol. 2012, 5, 425–432. [Google Scholar] [CrossRef]
- Link, M.S.; Wang, P.J.; Maron, B.J.; Estes, N.A., III. What is commotio cordis? Cardiol. Rev. 1999, 7, 265–269. [Google Scholar] [CrossRef]
- Shorr, R.M.; Crittenden, M.; Indeck, M.; Hartunian, S.L.; Rodríguez, A. Blunt thoracic trauma. Analysis of 515 patients. Ann. Surg. 1987, 206, 200–205. [Google Scholar] [CrossRef]
- Liman, S.T.; Kuzucu, A.; Tastepe, A.I.; Ulasan, G.N.; Topcu, S. Chest injury due to blunt trauma. Eur. J. Cardiothorac. Surg. 2003, 23, 374–378. [Google Scholar] [CrossRef]
- Freixinet Gilart, J.; Elena Ramírez Gil, M.; Gallardo Varela, G.; Moreno Casado, P. Chest trauma [Traumatismos torácicos]. Arch Bronconeumol. 2011, 47 (Suppl. 3), 9–14. [Google Scholar] [CrossRef]
- Lin, F.C.F.; Li, R.Y.; Tung, Y.W.; Jeng, K.C.; Tsai, S.C.S. Morbidity; mortality; associated injuries; and management of traumatic rib fractures. J. Chin. Med. Assoc. 2016, 79, 329–334. [Google Scholar] [CrossRef]
- Prachalias, A.A.; Kontis, E. Isolated abdominal trauma: Diagnosis and clinical management considerations. Curr. Opin. Crit. Care 2014, 20, 218–225. [Google Scholar] [CrossRef]
- Jordan, G.L., Jr.; Beall, A.C., Jr. Diagnosis and management of abdominal trauma. Curr. Probl. Surg. 1971, 8, 3–62. [Google Scholar] [CrossRef]
- Mercadante, S.; Nicosia, F. Celiac plexus block: A reappraisal. Regional Anesth. 1998, 23, 37–48. [Google Scholar] [CrossRef]
- De Froidmont, S.; Lobrinus, J.A.; Michaud, K.; Palmiere, C.; Augsburger, M.P.; Mangin, P.; Grabherr, S. Cardioinhibitory reflex due to a karate kick. Am. J. Forensic Med. Pathol. 2015, 36, 79–83. [Google Scholar] [CrossRef] [PubMed]
- Schrag, B.; Vaucher, P.; Bollmann, M.D.; Mangin, P. Death caused by cardioinhibitory reflex cardiac arrest—A systematic review of cases. Forensic Sci. Int. 2011, 207, 77–83. [Google Scholar] [CrossRef] [PubMed]
- Hess, D.S.; Hanlon, T.; Scheinman, M.; Budge, R.; Desai, J. Termination of ventricular tachycardia by carotid sinus massage. Circulation 1982, 65, 627–633. [Google Scholar] [CrossRef]
- Schrag, B.; Mangin, P.; Vaucher, P.; Bollmann, M.D. Death caused by cardioinhibitory reflex: What experts believe. Am. J. Forensic Med. Pathol. 2012, 33, 8–12. [Google Scholar] [CrossRef]
- Gaggioli, G.; Brignole, M.; Menozzi, C.; Bottoni, N.; Gianfranchi, L.; Oddone, D.; Lolli, G. Reappraisal of the vasodepressor reflex in carotid sinus syndrome. Am. J. Cardiol. 1995, 75, 518–521. [Google Scholar] [CrossRef]
- Lucena, J.S.; Rico, A.; Salguero, M.; Blanco, M.; Vázquez, R. Commotio cordis as a result of a fight: Report of a case considered to be imprudent homicide. Forensic Sci. Int. 2008, 177, e1–e4. [Google Scholar] [CrossRef]
- Bergqvist, D.; Hedelin, H.; Karlsson, G.; Lindblad, B.; Matzsch, T. Abdominal injury from sporting activities. Br. J. Sports Med. 1982, 16, 76–79. [Google Scholar] [CrossRef]
- Kazemi, M.; Shearer, H.; Young, S.C. Pre-competition habits and injuries in Taekwondo athletes. BMC Musculoskelet. Disord. 2005, 6, 26. [Google Scholar] [CrossRef]
- Kazemi, M.; Pieter, W. Injuries at a Canadian National Taekwondo Championships: A prospective study. BMC Musculoskelet. Disord. 2004, 5, 22. [Google Scholar] [CrossRef]
- Mithofer, K.; Lhowe, D.W.; Altman, G.T. Delayed presentation of acute compartment syndrome after contusion of the thigh. J. Orthop. Trauma. 2002, 16, 436–438. [Google Scholar] [CrossRef]
- Čierna, D.; Barrientos, M.; Agrasar, C.; Arriaza, R. Epidemiology of injuries in juniors participating in top-level karate competition: A prospective cohort study. Br. J. Sports Med. 2018, 52, 730–734. [Google Scholar] [CrossRef]
- Hübscher, M.; Zech, A.; Pfeifer, K.; Hänsel, F.; Vogt, L.; Banzer, W. Neuromuscular training for sports injury prevention: A systematic review. Med. Sci. Sports Exerc. 2010, 42, 413–421. [Google Scholar] [CrossRef]
- Vera-Jiménez, J.C. Manual Intervención Policial y Prevención de Riesgos—OTP. Available online: http://d-nb.info/1121789234 (accessed on 18 April 2020).
- Benito, J.M. Manual Básico de Procedimientos y Defensa Personal Policial I and Manual Básico de Procedimientos y Defensa Personal Policial ii. Cuerpo Nacional de Policía. División de Formación y Perfeccionamiento; Centro de Actualización y Perfeccionamiento. Available online: https://es.scribd.com/document/74168214/Manual-Defensa-Personal-Policial2 (accessed on 18 April 2020).
- Manual Defensa Personal Guardia Civil para la Academia de Guardias y Suboficiales de la Guardia Civil. Jefatura de Enseñanza; Ministerio del Interior: Baeza, Spain, 2010; Restricted access Manual.
- Plan Anual de Formación de la Escuela de Seguridad Pública de Andalucía Para el Curso Académico 2015. Available online: http://www.juntadeandalucia.es/organismos/justiciaeinterior/areas/policia/espa/paginas/plan-formacion-espa.html (accessed on 18 February 2020).
- Buschbacher, R.M. Martial arts. Phys. Med. Rehabil. Clin. N. Am. 1999, 10, 35–47. [Google Scholar] [CrossRef]
- Pieter, W. Martial arts injuries. Med. Sport Sci. 2005, 48, 59–73. [Google Scholar] [CrossRef]
- Hoover, E.J. Defensive tactics. In A Handbook for Law Enforcement Officers; FBI: Washington, DC, USA, 1951. Available online: https://es.scribd.com/doc/53113986/Defensa-Personal-FBI-Defensive-Tactics-Manual (accessed on 18 April 2020).
- Levine, D.; Whitman, J. Complete Krav Maga; Ulysses Press: Berkeley, CA, USA, 2016. [Google Scholar]
- MIEMIO—Ministerio del Interior de España Manual de Intervención Operativa. Ministerio del Interior; Guardia Civil: Baeza, Spain, 2014; Restricted access Manual.
- Vera Jiménez, J.C.; Fernández, F.; Ayuso, J.; Lorente, J.A. Evaluation of the police operational tactical procedures for reducing officer injuries resulting from physical interventions in problematic arrests. The case of the Municipal Police of Cádiz (Spain). Int. J. Occup. Med. Environ. Health 2020, 33, 35–43. [Google Scholar] [CrossRef]
- Vera-Jiménez, J.C.; Ferreiro-González, M.; Barbero, G.F.; Álvarez, J.Á.; Fernández-Zacarías, F.; Ayuso, J. OTP-PRL: An app for occupational risk prevention in policing activities. BMC Public Health 2019, 19, 1549. [Google Scholar] [CrossRef]
- Patents. Available online: https://patents.google.com/patent/ES2615602B2/es?oq=ES2615602B2 (accessed on 18 April 2020).




© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vera-Jiménez, J.C.; Lorente, J.A.; González-Herrera, L.; Álvarez, J.A.; Ferreiro-González, M.; Ayuso, J. A Legal and Forensic Medicine Approach to Police Physical Intervention Techniques in High-Risk Situations. Int. J. Environ. Res. Public Health 2020, 17, 2809. https://doi.org/10.3390/ijerph17082809
Vera-Jiménez JC, Lorente JA, González-Herrera L, Álvarez JA, Ferreiro-González M, Ayuso J. A Legal and Forensic Medicine Approach to Police Physical Intervention Techniques in High-Risk Situations. International Journal of Environmental Research and Public Health. 2020; 17(8):2809. https://doi.org/10.3390/ijerph17082809
Chicago/Turabian StyleVera-Jiménez, José C., José A. Lorente, Lucas González-Herrera, José A. Álvarez, Marta Ferreiro-González, and Jesús Ayuso. 2020. "A Legal and Forensic Medicine Approach to Police Physical Intervention Techniques in High-Risk Situations" International Journal of Environmental Research and Public Health 17, no. 8: 2809. https://doi.org/10.3390/ijerph17082809
APA StyleVera-Jiménez, J. C., Lorente, J. A., González-Herrera, L., Álvarez, J. A., Ferreiro-González, M., & Ayuso, J. (2020). A Legal and Forensic Medicine Approach to Police Physical Intervention Techniques in High-Risk Situations. International Journal of Environmental Research and Public Health, 17(8), 2809. https://doi.org/10.3390/ijerph17082809