Histological Effects of an Innovative 445 Nm Blue Laser During Oral Soft Tissue Biopsy

 ,
,  ,
,  ,
, 
 , and
, and 
Abstract
1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Deppe, H.; Horch, H.H. Current status of laser applications in oral and cranio-maxillofacial surgery. Med. Laser Appl. 2007, 22, 39–42. [Google Scholar] [CrossRef]
- Wigdor, H.A.; Walsh, J.T.; Featherstone, J.D.B.; Visuri, S.R.; Fried, D.; Waldvogel, J.L. Lasers in dentistry. Lasers Surg. Med. 1995, 16, 103–133. [Google Scholar] [CrossRef] [PubMed]
- Cadavid, A.M.H.; de Campos, W.G.; Aranha, A.C.C.; Lemos-Junior, C.A. Efficacy of photocoagulation of vascular malformations in the oral mucosa using Nd: YAG laser. J. Craniofac. Surg. 2018, 29, e614–e617. [Google Scholar] [CrossRef] [PubMed]
- Impellizzeri, A.; Palaia, G.; Horodynski, M.; Pergolini, D.; Vernucci, R.A.; Romeo, U.; Galluccio, G. CO2 laser for surgical exposure of impacted palatally canines. Dental Cadmos 2020. [Google Scholar] [CrossRef]
- Rizoiu, I.M.; Eversole, L.R.; Kimmel, A.I. Effects of an erbium, chromium: Yttrium, scandium, gallium, garnet laser on mucocutanous soft tissues. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 1996, 82, 386–395. [Google Scholar] [CrossRef]
- Suter, V.G.A.; Altermatt, H.J.; Bornstein, M.M. A randomized controlled clinical and histopathological trial comparing excisional biopsies of oral fibrous hyperplasias using CO2 and Er:YAG laser. Lasers Med. Sci. 2017, 32, 573–581. [Google Scholar] [CrossRef]
- Palaia, G.; Del Vecchio, A.; Impellizzeri, A.; Tenore, G.; Visca, P.; Libotte, F.; Russo, C.; Romeo, U. Histological ex vivo evaluation of peri-incisional thermal effect created by a new-generation CO2 superpulsed laser. Sci. World J. 2014, 2014, 345685. [Google Scholar] [CrossRef]
- Azma, E.; Safavi, N. Diode laser application in soft tissue oral surgery. J. Lasers Med. Sci. 2013, 4, 206. [Google Scholar] [CrossRef]
- Tirelli, G.; Boscolo Nata, F.; Bussani, R.; Gatto, A.; Quatela, E.; Rigo, S.; Piovesana, M. How we improve the transoral resection for oral and oropharyngeal cancer: The CO2 waveguide laser. Eur. Arch. Oto-Rhino-Laryngol. 2019, 276, 2301–2310. [Google Scholar] [CrossRef]
- Monteiro, L.; Delgado, M.L.; Garcês, F.; Machado, M.; Ferreira, F.; Martins, M.; Salazar, F.; Pacheco, J.J. A histological evaluation of the surgical margins from human oral fibrous-epithelial lesions excised with CO2 laser, diode laser, er:Yag laser, nd:Yag laser, electrosurgical scalpel and cold scalpel. Med. Oral Patol. Oral Cir. Bucal 2019, 24, e271. [Google Scholar] [CrossRef]
- Myers, M.L. The effect of laser irradiation on oral tissues. J. Prosthet. Dent. 1991, 66, 395–397. [Google Scholar] [CrossRef]
- Genovese, M.D.; Olivi, G. Laser in paediatric dentistry: Patient acceptance of hard and soft tissue therapy. Eur. J. Paediatr. Dent. 2008, 9, 13. [Google Scholar]
- Myers, T.D.; Sulewski, J.G. Evaluating dental lasers: What the clinician should know. Dent. Clin. N. Am. 2004, 48, 1127–1144. [Google Scholar] [CrossRef] [PubMed]
- Eversole, L.R. Laser artifacts and diagnostic biopsy. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 1997, 83, 639. [Google Scholar] [CrossRef]
- Convissar, R.A. Laser biopsy artifact. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 1997, 84, 458. [Google Scholar] [CrossRef]
- Tuncer, I.; Ozçakir-Tomruk, C.; Sencift, K.; Cöloǧlu, S. Comparison of conventional surgery and CO2 laser on intraoral soft tissue pathologies and evaluation of the collateral thermal damage. Photomed. Laser Surg. 2010, 28, 75–79. [Google Scholar] [CrossRef]
- Angiero, F.; Parma, L.; Crippa, R.; Benedicenti, S. Diode laser (808 nm) applied to oral soft tissue lesions: A retrospective study to assess histopathological diagnosis and evaluate physical damage. Lasers Med. Sci. 2012, 28, 75–79. [Google Scholar] [CrossRef]
- Romeo, U.; Russo, C.; Palaia, G.; Lo Giudice, R.; Del Vecchio, A.; Visca, P.; Migliau, G.; De Biase, A. Biopsy of different oral soft tissues lesions by KTP and diode laser: Histological evaluation. Sci. World J. 2014, 2014, 761704. [Google Scholar] [CrossRef]
- Vescovi, P.; Corcione, L.; Meleti, M.; Merigo, E.; Fornaini, C.; Manfredi, M.; Bonanini, M.; Govoni, P.; Rocca, J.P.; Nammour, S. Nd:YAG laser versus traditional scalpel. A preliminary histological analysis of specimens from the human oral mucosa. Lasers Med. Sci. 2010, 25, 685–691. [Google Scholar] [CrossRef]
- Romeo, U.; Libotte, F.; Palaia, G.; Del Vecchio, A.; Tenore, G.; Visca, P.; Nammour, S.; Polimeni, A. Histological in vitro evaluation of the effects of Er:YAG laser on oral soft tissues. Lasers Med. Sci. 2012, 27, 749–753. [Google Scholar] [CrossRef]
- Nakamura, S.; Senoh, M.; Nagahama, S.I.; Iwasa, N.; Matsushita, T.; Mukai, T. Blue InGaN-based laser diodes with an emission wavelength of 450 nm. Appl. Phys. Lett. 2000, 76, 22–24. [Google Scholar] [CrossRef]
- Palaia, G.; Tenore, G.; Tribolati, L.; Russo, C.; Gaimari, G.; Del Vecchio, A.; Romeo, U. Evaluation of wound healing and postoperative pain after oral mucosa laser biopsy with the aid of compound with chlorhexidine and sodium hyaluronate: A randomized double blind clinical trial. Clin. Oral Investig. 2019, 23, 3141–3151. [Google Scholar] [CrossRef] [PubMed]
- Mota-Ramírez, A.; Silvestre, F.J.; Simó, J.M. Oral biopsy in dental practice. Med. Oral Patol. Oral Cirugía Bucal 2007, 12, 504–510. [Google Scholar]
- Ma, G.; Sano, K.; Ikeda, H.; Inokuchi, T. Promotional effects of CO2 laser and scalpel incision on 4-NQO-induced premalignant lesions of mouse tongue. Lasers Surg. Med. 1999, 25, 207–212. [Google Scholar] [CrossRef]
- Awadallah, M.; Idle, M.; Patel, K.; Kademani, D. Management update of potentially premalignant oral epithelial lesions. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2018, 125, 628–636. [Google Scholar] [CrossRef] [PubMed]
- Issa, B.; Padilla, R.; Brennan, M.T. Diagnosis and management of mucosal lesions with the potential for malignant transformation. J. Calif. Dent. Assoc. 2013, 41, 343–348. [Google Scholar]
- Dong, Y.; Chen, Y.; Tao, Y.; Hao, Y.; Jiang, L.; Dan, H.; Zeng, X.; Chen, Q.; Zhou, Y. Malignant transformation of oral leukoplakia treated with carbon dioxide laser: A meta-analysis. Lasers Med. Sci. 2019, 34, 209–221. [Google Scholar] [CrossRef]
- Romeo, U.; Palaia, G.; Del Vecchio, A.; Tenore, G.; Gambarini, G.; Gutknecht, N.; De Luca, M. Effects of KTP laser on oral soft tissues. An in vitro study. Lasers Med. Sci. 2010, 25, 539–543. [Google Scholar] [CrossRef]
- De Maia, H.C.M.; Pinto, N.A.S.; Pereira, J.D.S.; de Medeiros, A.M.C.; da Silveira, É.J.D.; da Miguel, M.C.C. Potentially malignant oral lesions: Clinicopathological correlations. Einstein (Sao Paulo) 2016, 14, 35–40. [Google Scholar] [CrossRef]
- Vescovi, P.; Merigo, E.; Fornaini, C.; Rocca, J.P.; Nammour, S. Thermal increase in the oral mucosa and in the jawbone during Nd: YAG laser applications. Ex vivo study. Med. Oral Patol. Oral Cir. Bucal 2012, 17, e679. [Google Scholar] [CrossRef]
- Romanos, G.E.; Sacks, D.; Montanaro, N.; Delgado-Ruiz, R.; Calvo-Guirado, J.L.; Javed, F. Effect of Initiators on Thermal Changes in Soft Tissues Using a Diode Laser. Photomed. Laser Surg. 2018, 36, 386–390. [Google Scholar] [CrossRef] [PubMed]
- Jin, J.Y.; Lee, S.H.; Yoon, H.J. A comparative study of wound healing following incision with a scalpel, diode laser or Er, Cr:YSGG laser in guinea pig oral mucosa: A histological and immunohistochemical analysis. Acta Odontol. Scand. 2010, 68, 232–238. [Google Scholar] [CrossRef] [PubMed]
- Frigerio, A.; Tan, O.T. Laser applications for benign oral lesions. Lasers Surg. Med. 2015, 47, 643–650. [Google Scholar] [CrossRef] [PubMed]
- Vu, J.; Coleman, H.G.; Palme, C.E.; Riffat, F.; Schifter, M.; Zoellner, H. Diagnostic utility of microsurgical carbon dioxide laser excision of oral potentially malignant lesions vs incisional biopsy: A retrospective histopathological review. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2019, 127, 516–525. [Google Scholar] [CrossRef]
- Reichelt, J.; Winter, J.; Meister, J.; Frentzen, M.; Kraus, D. A novel blue light laser system for surgical applications in dentistry: Evaluation of specific laser-tissue interactions in monolayer cultures. Clin. Oral Investig. 2017, 21, 985–994. [Google Scholar] [CrossRef]
- Palaia, G.; Impellizzeri, A.; Tenore, G.; Caporali, F.; Visca, P.; Del Vecchio, A.; Galluccio, G.; Polimeni, A.; Romeo, U. Ex vivo histological analysis of the thermal effects created by a 445-nm diode laser in oral soft tissue biopsy. Clin. Oral Investig. 2019. [Google Scholar] [CrossRef]
- Isola, G.; Matarese, G.; Cervino, G.; Matarese, M.; Ramaglia, L.; Cicciù, M. Clinical efficacy and patient perceptions of pyogenic granuloma excision using diode laser versus conventional surgical techniques. J. Craniofac. Surg. 2018, 29, 2160–2163. [Google Scholar] [CrossRef]
- Tenore, G.; Palaia, G.; Mohsen, A.; Ambrogiano, S.; Di Gioia, C.R.T.; Dominiak, M.; Romeo, U. Could the super-pulsed CO2 laser be used for oral excisional biopsies? Adv. Clin. Exp. Med. 2019, 28, 1513–1517. [Google Scholar] [CrossRef]
- Suter, V.G.A.; Altermatt, H.J.; Bornstein, M.M. A randomized controlled trial comparing surgical excisional biopsies using CO2 laser, Er:YAG laser and scalpel. Int. J. Oral Maxillofac. Surg. 2020, 49, 99–106. [Google Scholar] [CrossRef]
- Braun, A.; Kettner, M.; Berthold, M.; Wenzler, J.S.; Heymann, P.G.B.; Frankenberger, R. Efficiency of soft tissue incision with a novel 445-nm semiconductor laser. Lasers Med. Sci. 2018, 33, 27–33. [Google Scholar] [CrossRef]
- Jiang, D.L.; Yang, Z.; Liu, G.X.; Wu, K.; Fan, J.; Wu, D.; Li, L.; Wang, X.; Guo, P.; Mu, L.; et al. A novel 450-nm blue laser system for surgical applications: Efficacy of specific laser-tissue interactions in bladder soft tissue. Lasers Med. Sci. 2019, 34, 807–813. [Google Scholar] [CrossRef] [PubMed]
- Fornaini, C.; Merigo, E.; Rocca, J.P.; Lagori, G.; Raybaud, H.; Selleri, S.; Cucinotta, A. 450 nm blue laser and oral surgery: Preliminary ex vivo study. J. Contemp. Dent. Pract. 2016, 17, 795–800. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient | Sex | Age | Medical History | Drugs | Smoke | Site | Clinical Suspicion |
|---|---|---|---|---|---|---|---|
| 1. | M | 15 | Nothing To Report | NO | NO | Vestibular interdental papilla | Pyogenic Granuloma |
| 2. | F | 63 | Celiac’s Disease, Uterine Fibromas | NO | NO | Tip of the tongue | Iperplafocal Fibrous Hyperplasiasia |
| 3. | F | 42 | Nothing To Report | Birth Control Pill | 3 per day for 25 years | Keratinized Vestibular Gingiva | Pyogenic Granuloma |
| 4. | M | 43 | Hypercholesterolemia, Kidney Stones, Psoriasis | Hypercholesterolemia Medication, Anti-Psoriatic | NO | Right buccal mucosa | Focal Fibrous Hyperplasia |
| 5. | F | 60 | Hypertension | Antihypertensive Drug | 25 per day for 47 years | Right buccal mucosa | Focal Fibrous Hyperplasia |
| 6. | F | 69 | Nothing To Report | NO | NO | Tip of the Tongue (2 lesions) | Focal Fibrous Hyperplasia |
| 7. | M | 63 | Pneumothorax, Inguinal Hernia | NO | 10 per day for 30 years | Soft palate | Squamous Papilloma |
| 8. | F | 60 | Hypertension, Sjogren’s syndrome | NO | NO | Hard palate | Squamous Papilloma |
| 9. | F | 72 | Hypertension, Chronic Ischemic Heart Disease, Obesity | Antihypertensive Drugs, Diuretic | NO | Right buccal mucosa– right upper arch | Focal Fibrous Hyperplasia |
| Case | Histological Diagnosis | Epithelial Thermal Effect (μm) | Connective Tissue Thermal Effect (μm) | Tissue Thermal Effect (μm) |
|---|---|---|---|---|
| 1. | Giant Cell Granuloma | 898.7 ± 311.96 | 217.5 ± 264.23 | 1116.2 ± 505.37 |
| 2. | Squamous Papilloma | 136.1 ± 311.96 | 181.7 ± 264.23 | 317.8 ± 505.37 |
| 3. | Pyogenic Granuloma | 831.5 ± 311.96 | 926.9 ± 264.23 | 1758.2 ± 505.37 |
| 4. | Focal Fibrous Hyperplasia | 690.8 ± 311.96 | 555.3 ± 264.23 | 1246.1 ± 505.37 |
| 5. | Focal Fibrous Hyperplasia | 1188 ± 311.96 | 585.5 ± 264.23 | 1773.5 ± 505.37 |
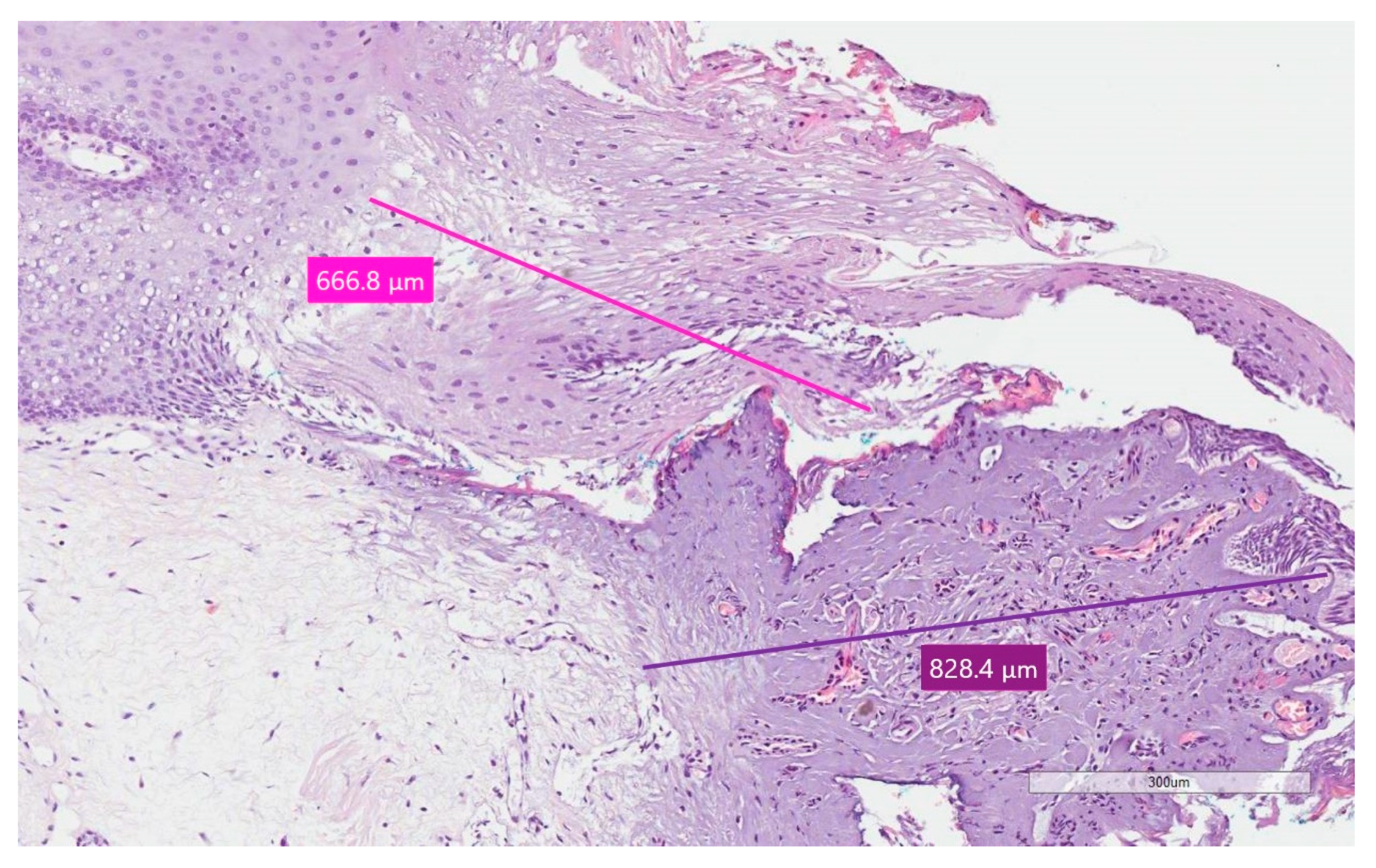
| 6.(1) | Pyogenic Granuloma | 666.8 ± 311.96 | 828.4 ± 264.23 | 1495.2 ± 505.37 |
| 6.(2) | Focal Fibrous Hyperplasia | 331.7 ± 311.96 | 266.1 ± 264.23 | 597.8 ± 505.37 |
| 7. | Squamous Papilloma | 477.1 ± 311.96 | 248.4 ± 264.23 | 725.5 ± 505.37 |
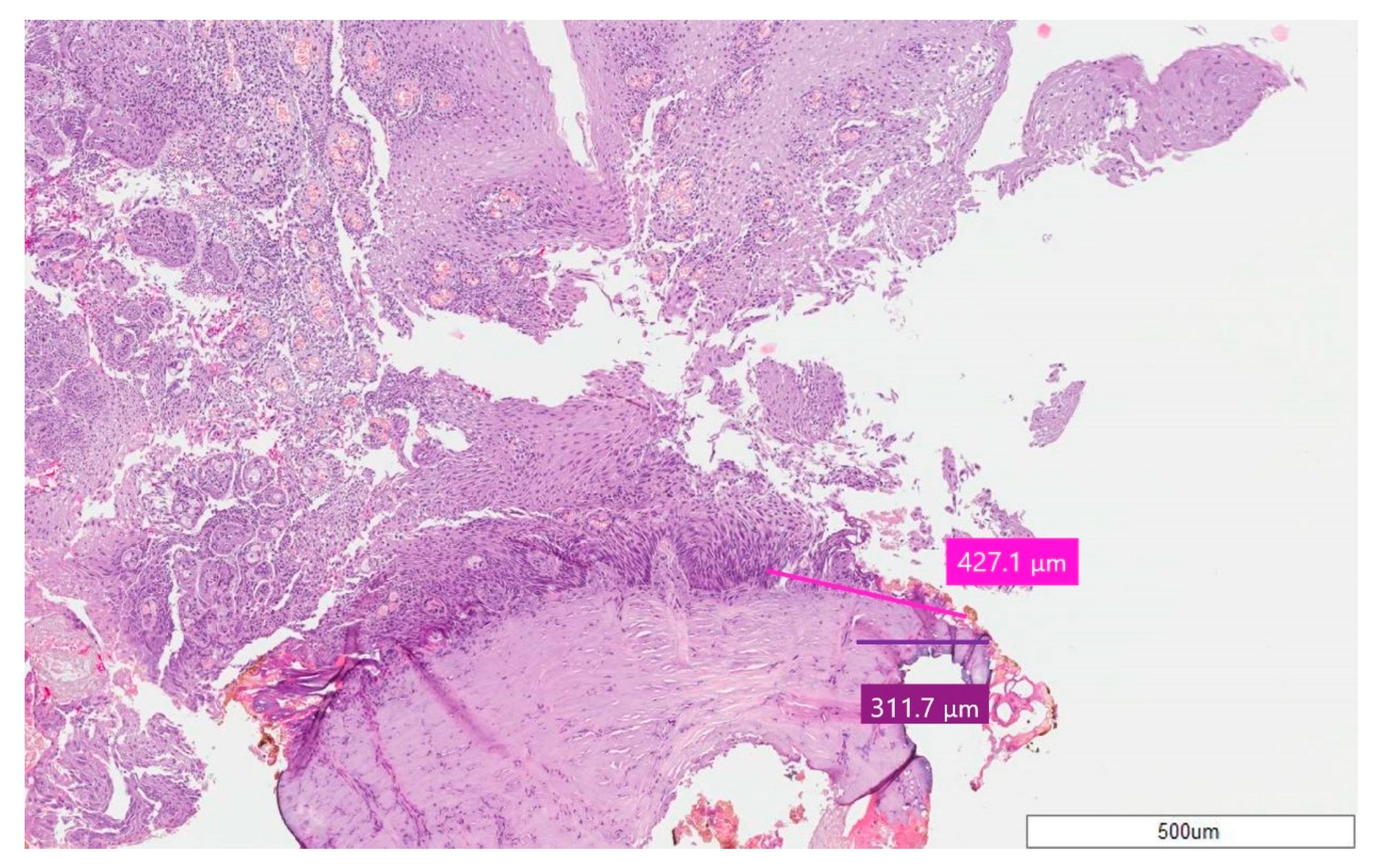
| 8. | Squamous Papilloma | 427.1 ± 311.96 | 311.7 ± 264.23 | 738.8 ± 505.37 |
| 9. | Focal Fibrous Hyperplasia | 861.5 ± 311.96 | 559.2 ± 264.23 | 1420.7 ± 505.37 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Palaia, G.; Pergolini, D.; D’Alessandro, L.; Carletti, R.; Del Vecchio, A.; Tenore, G.; Di Gioia, C.R.T.; Romeo, U. Histological Effects of an Innovative 445 Nm Blue Laser During Oral Soft Tissue Biopsy. Int. J. Environ. Res. Public Health 2020, 17, 2651. https://doi.org/10.3390/ijerph17082651
Palaia G, Pergolini D, D’Alessandro L, Carletti R, Del Vecchio A, Tenore G, Di Gioia CRT, Romeo U. Histological Effects of an Innovative 445 Nm Blue Laser During Oral Soft Tissue Biopsy. International Journal of Environmental Research and Public Health. 2020; 17(8):2651. https://doi.org/10.3390/ijerph17082651
Chicago/Turabian StylePalaia, Gaspare, Daniele Pergolini, Leonardo D’Alessandro, Raffaella Carletti, Alessandro Del Vecchio, Gianluca Tenore, Cira Rosaria Tiziana Di Gioia, and Umberto Romeo. 2020. "Histological Effects of an Innovative 445 Nm Blue Laser During Oral Soft Tissue Biopsy" International Journal of Environmental Research and Public Health 17, no. 8: 2651. https://doi.org/10.3390/ijerph17082651
APA StylePalaia, G., Pergolini, D., D’Alessandro, L., Carletti, R., Del Vecchio, A., Tenore, G., Di Gioia, C. R. T., & Romeo, U. (2020). Histological Effects of an Innovative 445 Nm Blue Laser During Oral Soft Tissue Biopsy. International Journal of Environmental Research and Public Health, 17(8), 2651. https://doi.org/10.3390/ijerph17082651