National Monitoring for Menstrual Health and Hygiene: Is the Type of Menstrual Material Used Indicative of Needs Across 10 Countries?


Abstract
1. Introduction
The Present Study
2. Materials and Methods
2.1. Measures
2.1.1. Menstrual Material Use
2.1.2. Menstrual Material Needs
2.2. Analyses
2.3. Ethical Approvals
3. Results
3.1. Menstrual Material Use Across Settings
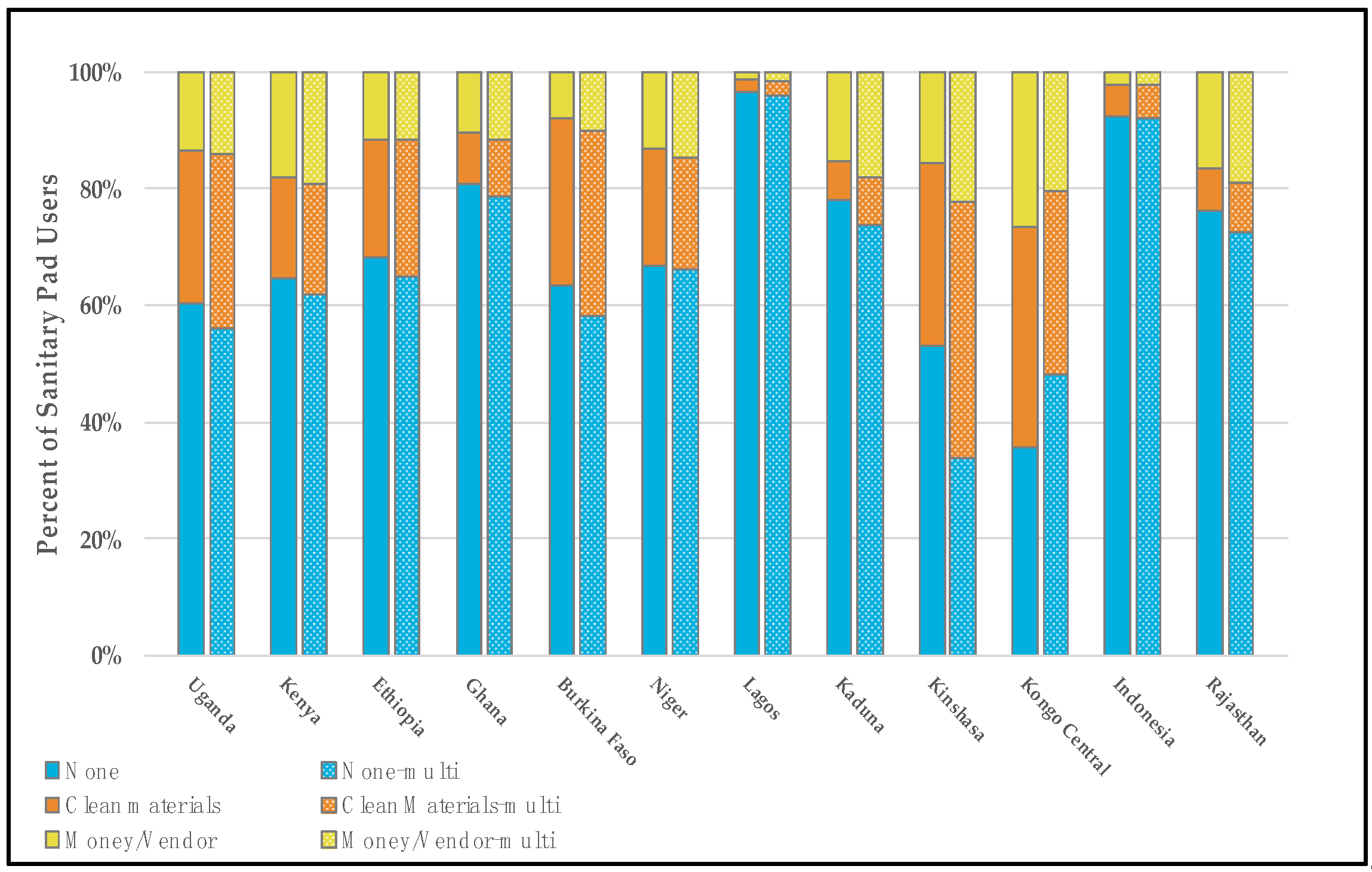
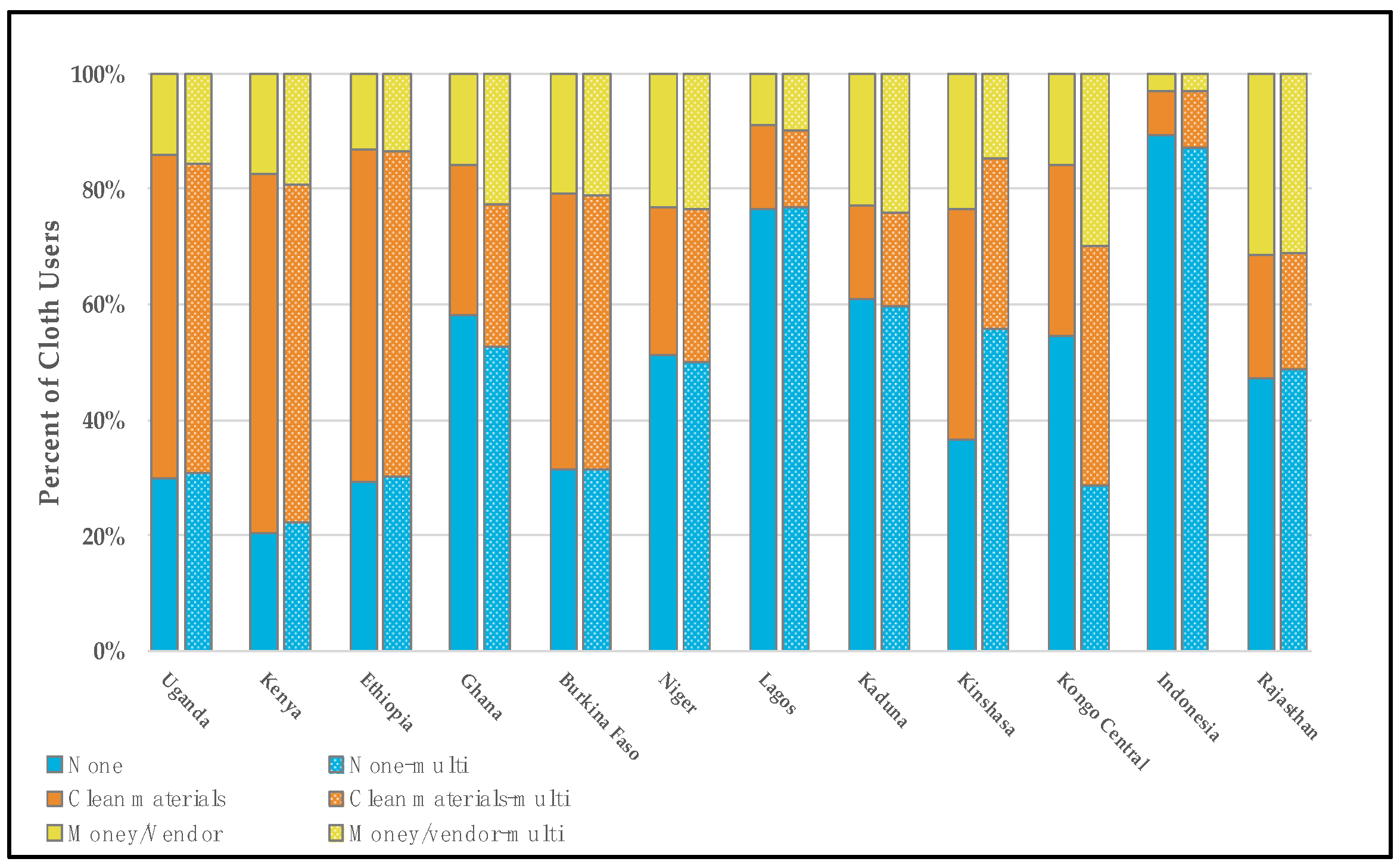
3.2. Menstrual Material Needs by the Type of Menstrual Material Used
3.3. Misrepresentaton of Material Needs by Socio-Demographic Group
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- UNICEF. Guidance on Menstrual Health and Hygiene; UNICEF: New York, NY, USA, 2019. [Google Scholar]
- Sommer, M.; Caruso, B.A.; Sahin, M.; Calderon, T.; Cavill, S.; Mahon, T.; Phillips-Howard, P.A. A Time for Global Action: Addressing Girls’ Menstrual Hygiene Management Needs in Schools. PLOS Med. 2016, 13, e1001962–e1001970. [Google Scholar] [CrossRef] [PubMed]
- Hennegan, J.; Shannon, A.K.; Rubli, J.; Schwab, K.J.; Melendez-Torres, G.J. Women’s and girls’ experiences of menstruation in low-and middle-income countries: A systematic review and qualitative metasynthesis. PLoS Med. 2019, 16, e1002803–e1002842. [Google Scholar] [CrossRef] [PubMed]
- Tellier, S.; Hyttel, M. Menstrual Health Management in East and Southern Africa: a Review Paper; UNFPA: Johannesburg, South Africa, 2017. [Google Scholar]
- Geertz, A.; Iyer, L.; Kasen, P.; Mazzola, F.; Peterson, K. An Opportunity to Address Menstrual Health and Gender Equity; FSG: Boston, MA, USA, 2016. [Google Scholar]
- Weiss-Wolf, J.U.S. Policymaking to Address Menstruation: Advancing an Equity Agenda. Wm Mary J Women L 2019, 25, 493–525. [Google Scholar]
- Rwanda Scraps Tax on Sanitary Pads. East Afr. 2019. Available online: https://www.theeastafrican.co.ke/business/Rwanda-scraps-tax-on-sanitary-pads/2560-5382040-12x2gf7z/index.html (accessed on 8 February 2020).
- SA Joins Growing List of Countries with Zero Tax on Sanitary Pads. IOL Bus. Rep. 2018. Available online: https://www.iol.co.za/business-report/economy/sa-joins-growing-list-of-countries-with-zero-tax-on-sanitary-pads-17682368 (accessed on 8 February 2020).
- Berger, M. Germany Has Slashed Its Tax on Tampons. Many other Countries still Tax them as ‘luxury’ Items. Wash. Post. 2019. Available online: https://www.washingtonpost.com/world/2019/11/09/germany-has-slashed-its-tax-tampons-many-other-countries-still-tax-them-luxury-items/ (accessed on 8 February 2020).
- Bobel, C. Making Menstruation Matter in the Global South: Mapping a Critical History. In The Managed Body: Developing Girls and Menstrual Health in the Global South; Palgrave Macmillan: London, UK, 2019; pp. 69–109. [Google Scholar]
- Hennegan, J. Inserting informed choice into global menstrual product use and provision. Lancet Public Health 2019, 4, e361–e362. [Google Scholar] [CrossRef]
- Khomani, N. Scotland to Offer Free Sanitary Products to all Students in World First. The Guardian. 2018. Available online: https://www.theguardian.com/uk-news/2018/aug/24/scotland-to-offer-free-sanitary-products-to-all-students-in-world-first (accessed on 8 February 2020).
- Garg, R.; Goyal, S.; Gupta, S. India moves towards menstrual hygiene: subsidized sanitary napkins for rural adolescent girls-issues and challenges. Matern. Child Health J. 2012, 16, 767–774. [Google Scholar] [CrossRef] [PubMed]
- Free sanitary pads for adolescent schoolgirls. Himal. Times. 2020. Available online: https://thehimalayantimes.com/kathmandu/free-sanitary-pads-for-adolescent-schoolgirls/ (accessed on 8 February 2020).
- Kenya’s schoolgirls to get free sanitary pads from government. BBC News. 2017. Available online: https://www.bbc.com/news/world-africa-40365691 (accessed on 8 February 2020).
- Sommer, M.; Zulaika, G.; Schmitt, M.; Gruer, C. Monitoring Menstrual Health and Hygiene Monitoring and Measuring Menstruation; Meeting Report; Columbia University and WSSCC: New York, NY, USA; Geneva, Switzerland, 2019. [Google Scholar]
- Sommer, M.; Schmitt, M.L.; Ogello, T.; Mathenge, P.; Mark, M.; Clatworthy, D.; Khandakji, S.; Ratnayake, R. Pilot testing and evaluation of a toolkit for menstrual hygiene management in emergencies in three refugee camps in Northwest Tanzania. J. Int. Humanit. Action 2018, 3, 6–19. [Google Scholar] [CrossRef]
- Home-PMA Data. Available online: https://www.pmadata.org/ (accessed on 8 February 2020).
- Zimmerman, L.; Olson, H.; Tsui, A.; Radloff, S. PMA2020: Rapid Turn-Around Survey Data to Monitor Family Planning Service and Practice in Ten Countries. Stud. Fam. Plann. 2017, 48, 293–303. [Google Scholar] [CrossRef] [PubMed]
- Home-UNICEF MICS. Available online: https://mics.unicef.org/ (accessed on 8 February 2020).
- Khan, S.M.; Bain, R.E.S.; Lunze, K.; Unalan, T.; Beshanski-Pedersen, B.; Slaymaker, T.; Johnston, R.; Hancioglu, A. Optimizing household survey methods to monitor the Sustainable Development Goals targets 6.1 and 6.2 on drinking water, sanitation and hygiene: A mixed-methods field-test in Belize. PLOS ONE 2017, 12, e0189089–e0189106. [Google Scholar] [CrossRef] [PubMed]
- The DHS Program-Quality Information to Plan, Monitor and Improve Population, Health, and Nutrition Programs. Available online: https://dhsprogram.com/ (accessed on 8 February 2020).
- Hennegan, J.; Brooks, D.J.; Schwab, K.J.; Melendez-Torres, G.J. Measurement in the study of menstrual health and hygiene: A systematic review and audit. SocArXiv 2019. Available online: https://osf.io/preprints/socarxiv/n8j5w/ (accessed on 8 February 2020).
- Joshi, D.; Buit, G.; González-Botero, D. Menstrual hygiene management: education and empowerment for girls? Waterlines 2015, 34, 51–67. [Google Scholar] [CrossRef]
- Mahajan, T. Imperfect Information in Menstrual Health and the Role of Informed Choice. Indian J. Gend. Stud. 2019, 26, 59–78. [Google Scholar] [CrossRef]
- UNICEF. Guide to Menstrual Hygiene Materials; UNICEF: New York, NY, USA, 2019. [Google Scholar]
- Nyaga, V.N. METAPREG: Stata Module to Compute Fixed and Random Effects Meta-Analysis and Meta-Regression of Proportions; Statistical Software Components S458693; Boston College Department of Economics: Boston, MA, USA, 2019. [Google Scholar]
- Hennegan, J.; Nansubuga, A.; Smith, C.; Redshaw, M.; Akullo, A.; Schwab, K.J. Measuring menstrual hygiene experience: development and validation of the Menstrual Practice Needs Scale (MPNS-36) in Soroti, Uganda. BMJ Open 2020, 10, e034461–e034477k. [Google Scholar] [CrossRef] [PubMed]
- Sommer, M.; Hirsch, J.S.; Nathanson, C.; Parker, R.G. Comfortably, safely, and without shame: Defining menstrual hygiene management as a public health issue. Am. J. Public Health 2015, 105, 1302–1311. [Google Scholar] [CrossRef] [PubMed]
- Farage, M.A.; Farage, M.A.; Miller, K.W.; Davis, A. Cultural aspects of menstruation and menstrual hygiene in adolescents. Expert Rev. Obstet. Gynecol. 2011, 6, 127–139. [Google Scholar] [CrossRef]
- Wallace, M. Rollins College Rollins Scholarship Online the Impact of Globalization on the Perceptions and Practices of Menstruation among Indigenous Women in Peru. Bachelor of Arts Honors Program Thesis, Rollins College, Orlando, FL, USA, 2017. [Google Scholar]
- Hennegan, J.; Shannon, A.K.; Schwab, K.J. Wealthy, urban, educated. Who is represented in population surveys of women’s menstrual hygiene management? Reprod. Health Matters 2018, 26, 36–46. [Google Scholar] [CrossRef] [PubMed]
- The World Bank Data: GNI per Capita, Atlas Method (current US$). Available online: https://data.worldbank.org/indicator/NY.GNP.PCAP.CD (accessed on 8 February 2020).
- van Eijk, A.M.; Zulaika, G.; Lenchner, M.; Mason, L.; Sivakami, M.; Nyothach, E.; Unger, H.; Laserson, K.; Phillips-Howard, P.A. Menstrual cup use, leakage, acceptability, safety, and availability: a systematic review and meta-analysis. Lancet Public Health 2019, 4, e376–e393. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Menstrual Material | Uganda | Kenya | Ethiopia | Ghana | Burkina Faso | Niger | Lagos, Nigeria | Kaduna, Nigeria | Kinshasa, DRC | Kongo Central, DRC | Indonesia | Rajasthan |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| (n = 2709) | (n = 4364) | (n = 4784) | (n = 2837) | (n = 2158) | (n = 1913) | (n = 1169) | (n = 1993) | (n = 2081) | (n = 1109) | (n = 8117) | (n = 5023) | |
| Grouped single-response material categories (% of respondents) | ||||||||||||
| Pads only | 52.2 | 77.5 | 34.0 | 82.7 | 13.6 | 9.7 | 74.7 | 27.4 | 73.3 | 20.8 | 87.7 | 39.1 |
| Cloth only | 30.6 | 9.0 | 38.4 | 8.6 | 58.0 | 59.8 | 4.0 | 55.7 | 3.6 | 29.5 | 7.3 | 49.0 |
| Cotton wool only | 1.6 | 2.5 | 1.2 | 0.3 | 13.2 | 12.1 | 1.2 | 0.3 | 0.8 | 6.8 | 0.1 | 0.3 |
| Pads, cloth, cotton wool | 12.5 | 7.8 | 7.0 | 3.4 | 4.1 | 1.8 | 2.6 | 8.9 | 1.9 | 8.3 | 3.0 | 10.4 |
| Pads, cloth, cotton wool, other | 1.2 | 2.3 | 2.5 | 3.4 | 1.8 | 2.5 | 9.5 | 4.4 | 11.1 | 15.4 | 0.2 | 0.2 |
| Other 1 | 2.0 | 1.0 | 16.9 | 1.5 | 9.3 | 14.2 | 8.2 | 3.4 | 9.3 | 19.2 | 1.8 | 1.0 |
| Multi-response material categories (% of cases) | ||||||||||||
| Pads | 64.3 | 86.1 | 39.8 | 89.3 | 15.8 | 9.9 | 85.5 | 37.4 | 84.0 | 33.9 | 90.7 | 49.2 |
| Tampons | 0.2 | 1.2 | 0.3 | 1.2 | 0.8 | 0.9 | 0.6 | 0.0 | 1.9 | 5.6 | 0.1 | 0.1 |
| Cloth | 41.9 | 14.1 | 47.3 | 12.0 | 63.1 | 63.6 | 6.5 | 67.6 | 7.4 | 40.4 | 10.3 | 59.4 |
| Cotton wool | 5.1 | 7.3 | 3.0 | 1.0 | 15.4 | 13.7 | 2.6 | 1.2 | 2.2 | 17.1 | 0.3 | 1.4 |
| Paper | 0.6 | 2.2 | 0.2 | 3.3 | 3.9 | 0.2 | 17.1 | 4.6 | 15.3 | 25.1 | 0.2 | 0.1 |
| Foam | 0.4 | 0.5 | 0.8 | 0.3 | 1.2 | 8.6 | 0.5 | 0.34 | 0.5 | 5.1 | 0.0 | 0.1 |
| Natural materials | 0.3 | 0.1 | 2.2 | 0.6 | 0.1 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.1 |
| None | 1.3 | 0.4 | 11.1 | 0.1 | 3.7 | 4.3 | 0.0 | 1.1 | 0.3 | 2.7 | 1.7 | 0.9 |
| Bucket | 0.2 | |||||||||||
| Other 2 | 1.2 | 0.0 | 4.9 | 0.8 | 2.3 | 3.6 | 0.1 | 1.7 | 4.5 | 2.7 | 0.1 | 0.1 |
| Menstrual Material | Self-Reported Menstrual Material Needs Pooled Proportion (as Percent) (95% CI) | ||
|---|---|---|---|
| None | Absorbent | Money or Vendor | |
| Menstrual Material (grouped) | |||
| Pads only | 73.4 (61.2–82.8) | 14.1 (8.7–22.0) | 10.4 (6.6–16.0) |
| Cloth only | 49.2 (36.3–62.1) | 31.1 (21.4–42.8) | 16.3 (11.9–21.8) |
| Cotton wool only | 63.8 (52.8–73.5) | 24.2 (17.5–32.4) | 14.2 (10.8–18.4) |
| Pads, cloth, cotton wool | 50.6 (40.8–60.3) | 25.9 (17.9–35.9) | 19.1 (13.4–26.6) |
| Pads, cloth, cotton wool, other | 47.6 (30.4–65.4) | 30.8 (20.2–44.0) | 16.9 (10.2–26.9) |
| Other 1 | 61.4 (47.5–73.6) | 27.0 (17.4–39.3) | 9.2 (6.2–13.5) |
| Menstrual Material (multi-response) | |||
| Pads | 70.6 (57.5–80.9) | 15.6 (9.6–24.3) | 11.5 (7.4–17.5) |
| Cloth | 48.1 (35.9–60.6) | 30.7 (21.6–41.7) | 17.3 (12.6–23.4) |
| Cotton wool | 64.8 (51.8–75.9) | 20.6 (13.7–29.9) | 14.5 (10.1–20.5) |
| Paper | 55.2 (29.6–78.2) | 25.1 (14.6–39.6) | 14.9 (7.7–26.9) |
| All others 2 | 53.0 (41.3–64.5) | 33.6 (24.1–44.6) | 11.7 (8.6–15.7) |
| Socio-Demo- Graphic Group | Uganda | Kenya | Ethiopia | Ghana | Burkina Faso | Niger | Lagos, Nigeria | Kaduna, Nigeria | Kinshasa, DRC | Kongo Central, DRC | Indonesia | Rajasthan | Pooled Proportion |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| (n = 1415) | (n = 3359) | (n = 2533) | (n = 23,356) | (n = 446) | (n = 403) | (n = 871) | (n = 595) | (n = 1624) | (n = 367) | (n = 7143) | (n = 1840) | ||
| % | % | % | % | % | % | % | % | % | % | % | % | (95% CI) | |
| Age | |||||||||||||
| 15–19 | 40.8 | 38.8 | 37.2 | 21.0 | 46.7 | 34.9 | 4.3 | 29.4 | 50.9 | 62.4 | 9.6 | 31.6 | 26.5 (15.2–42.1) |
| 20–24 | 34.3 | 33.4 | 29.0 | 19.6 | 31.8 | 45.6 | 2.1 | 22.2 | 46.6 | 72.1 | 7.8 | 27.5 | 27.2 (17.2–40.3) |
| 25–34 | 38.9 | 34.4 | 28.5 | 19.7 | 41.8 | 26.3 | 2.8 | 16.6 | 43.6 | 70.4 | 8.1 | 19.2 | 25.0 (15.4–37.9) |
| 35+ | 46.0 | 34.3 | 26.7 | 17.4 | 18.0 | 16.2 | 4.4 | 17.0 | 47.0 | 49.8 | 6.5 | 11.7 | 20.8 (13.3–31.2) |
| Education | |||||||||||||
| None | 49.5 | 40.6 | 43.4 | 31.1 | 57.8 | 47.9 | 0.0 | 25.4 | 54.7 | 49.7 | 13.0 | 29.7 | 35.6 (26.7–45.5) |
| Primary | 51.9 | 42.3 | 40.6 | 29.0 | 38.7 | 37.6 | 3.0 | 13.6 | 49.2 | 65.0 | 11.1 | 32.6 | 31.4 (20.9–44.2) |
| Secondary | 32.2 | 34.7 | 25.5 | 18.2 | 31.9 | 31.5 | 4.1 | 24.8 | 48.0 | 65.3 | 7.4 | 24.6 | 25.6 (16.7–37.1) |
| Higher | 17.2 | 17.9 | 9.6 | 3.1 | 19.4 | 9.9 | 2.9 | 18.3 | 40.4 | 50.9 | 3.5 | 13.2 | 12.8 (7.4–21.3) |
| Wealth | |||||||||||||
| 1 (lowest) | 71.3 | 53.0 | 62.5 | 41.3 | 21.0 | 100 | 8.5 | 31.0 | 61.0 | 65.5 | 14.6 | 50.6 | 45.9 (29.2–63.6) |
| 2 | 56.1 | 45.3 | 41.2 | 20.8 | 66.1 | 96.7 | 6.0 | 29.4 | 51.2 | 89.7 | 11.3 | 40.6 | 43.6 (25.6–63.5) |
| 3 | 42.3 | 41.0 | 52.8 | 18.0 | 58.5 | 77.1 | 2.1 | 34.3 | 49.5 | 60.8 | 9.4 | 34.6 | 35.3 (21.0–5.29) |
| 4 | 33.6 | 33.4 | 43.6 | 16.3 | 62.4 | 42.4 | 1.1 | 21.0 | 38.9 | 67.8 | 4.9 | 22.2 | 26.2 (14.3–42.9) |
| 5 (highest) | 24.1 | 16.9 | 21.9 | 6.1 | 20.5 | 25.6 | 2.6 | 19.6 | 44.7 | 58.3 | 3.1 | 14.2 | 16.8 (9.7–27.5) |
| Rurality | |||||||||||||
| Urban | 25.7 | 25.9 | 22.6 | 13.4 | 26.7 | 22.7 | 9.3 | 6.7 | 13.4 | 17.1 (12.4–23.0) | |||
| Rural | 46.1 | 40.9 | 46.9 | 28.3 | 62.3 | 58.9 | 37.7 | 9 | 35.8 | 38.5 (27.3–51.1) | |||
| TOTAL | 39.2 | 35.4 | 31.4 | 19.4 | 36.5 | 33.2 | 3.5 | 21.9 | 47.0 | 63.3 | 7.7 | 18.8 | 26.4 (17.1–38.5) |
| Socio- Demo-Graphic Group | Uganda | Kenya | Ethiopia | Ghana | Burkina Faso | Niger | Lagos, Nigeria | Kaduna, Nigeria | Kinshasa, DRC | Kongo Central, DRC | Indonesia | Rajasthan | Pooled Proportion |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| (n = 1737) | (n = 3767) | (n = 2816) | (n = 2542) | (n = 526) | (n = 451) | (n = 997) | (n = 788) | (n = 1778) | (n = 535) | (n = 7403) | (n = 2341) | ||
| % | % | % | % | % | % | % | % | % | % | % | % | (95% CI) | |
| Age | |||||||||||||
| 15–19 | 45.5 | 41.0 | 42.4 | 23.2 | 53.3 | 36.4 | 4.8 | 34.9 | 56.2 | 66.7 | 9.8 | 34.8 | 34.2 (23.1–47.2) |
| 20–24 | 38.0 | 35.1 | 32.2 | 20.6 | 34.1 | 46.1 | 2.3 | 22.9 | 52.0 | 69.4 | 8.2 | 30.9 | 28.6 (17.9–42.4) |
| 25–34 | 43.6 | 37.8 | 30.7 | 22.0 | 45.2 | 27.7 | 3.4 | 22.1 | 49.4 | 69.8 | 8.2 | 22.3 | 28.0 (17.7–41.2) |
| 35+ | 49.3 | 37.9 | 28.8 | 19.8 | 26.3 | 16.6 | 4.7 | 20.9 | 49.3 | 57.9 | 7.1 | 18.6 | 23.2 (15.3–33.5) |
| Education | |||||||||||||
| None | 49.4 | 44.9 | 38.9 | 34.6 | 56.6 | 48.2 | 6.1 | 28.1 | 50.1 | 49.4 | 13.0 | 31.5 | 37.3 (29.5–45.9) |
| Primary | 56.7 | 45.7 | 44.7 | 31.2 | 47.5 | 36.1 | 2.4 | 26.3 | 59.0 | 66.3 | 11.8 | 36.3 | 35.6 (23.7–49.6) |
| Secondary | 35.4 | 37.0 | 28.8 | 19.8 | 38.2 | 32.3 | 4.3 | 27.4 | 51.8 | 69.1 | 7.5 | 28.0 | 28.0 (18.1–40.6) |
| Higher | 19.4 | 18.7 | 11.2 | 4.0 | 19.8 | 13.6 | 3.8 | 22.6 | 43.8 | 46.9 | 3.8 | 15.8 | 14.4 (8.7–23.0) |
| Wealth | |||||||||||||
| 1 (lowest) | 73.1 | 55.4 | 68.2 | 44.8 | 45.6 | 82.7 | 8.5 | 43.0 | 65.3 | 70.2 | 15.0 | 47.5 | 49.6 (34.8–64.5) |
| 2 | 60.9 | 48.9 | 44.2 | 22.2 | 68.7 | 96.7 | 6.2 | 43.2 | 54.3 | 79.2 | 11.8 | 40.6 | 44.8 (28.1–62.7) |
| 3 | 47.8 | 43.9 | 56.6 | 20.3 | 66.3 | 78.4 | 2.7 | 46.9 | 55.8 | 55.4 | 9.7 | 38.2 | 38.5 (23.7–55.9) |
| 4 | 38.8 | 36.0 | 44.5 | 17.8 | 59.2 | 44.6 | 2.2 | 25.8 | 42.1 | 67.3 | 5.1 | 27.5 | 29.0 (17.1–44.6) |
| 5 (highest) | 24.7 | 17.6 | 23.9 | 6.3 | 32.32 | 26.4 | 2.6 | 19.1 | 50.4 | 63.6 | 3.1 | 15.4 | 18.5 (10.3–30.8) |
| Rurality | |||||||||||||
| Urban | 27.8 | 26.8 | 24.7 | 14.7 | 29.0 | 25.0 | 9.7 | 6.7 | 15.6 | 18.4 (13.3–25.0) | |||
| Rural | 50.8 | 44.4 | 49.5 | 31.3 | 67.5 | 58.9 | 41.9 | 9.6 | 39.0 | 41.7 (29.9–54.6) | |||
| TOTAL | 43.7 | 38.2 | 35.0 | 21.4 | 41.6 | 34.0 | 3.9 | 26.3 | 51.8 | 65.7 | 8.0 | 27.38 | 29.3 (19.0–42.2) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Smith, A.D.; Muli, A.; Schwab, K.J.; Hennegan, J. National Monitoring for Menstrual Health and Hygiene: Is the Type of Menstrual Material Used Indicative of Needs Across 10 Countries? Int. J. Environ. Res. Public Health 2020, 17, 2633. https://doi.org/10.3390/ijerph17082633
Smith AD, Muli A, Schwab KJ, Hennegan J. National Monitoring for Menstrual Health and Hygiene: Is the Type of Menstrual Material Used Indicative of Needs Across 10 Countries? International Journal of Environmental Research and Public Health. 2020; 17(8):2633. https://doi.org/10.3390/ijerph17082633
Chicago/Turabian StyleSmith, Annie D., Alfred Muli, Kellogg J. Schwab, and Julie Hennegan. 2020. "National Monitoring for Menstrual Health and Hygiene: Is the Type of Menstrual Material Used Indicative of Needs Across 10 Countries?" International Journal of Environmental Research and Public Health 17, no. 8: 2633. https://doi.org/10.3390/ijerph17082633
APA StyleSmith, A. D., Muli, A., Schwab, K. J., & Hennegan, J. (2020). National Monitoring for Menstrual Health and Hygiene: Is the Type of Menstrual Material Used Indicative of Needs Across 10 Countries? International Journal of Environmental Research and Public Health, 17(8), 2633. https://doi.org/10.3390/ijerph17082633