Sexually Harassing Behaviors from Patients or Clients and Care Workers’ Mental Health: Development and Validation of a Measure

 , and
, and 
Abstract
1. Introduction
1.1. Conceptualization of Sexual Harassment
1.2. The Effect of Sexual Harassment on Employees’ Mental Health
1.3. Measurement of Sexual Harassment from an Extraorganizational Perspective
2. Study 1: Item Generation and Item Review
2.1. Method
2.1.1. Ethics Approval and Consent to Participate
2.1.2. Sample and Procedure
2.2. Results
3. Study 2: Item Reduction and Factorial Structure
3.1. Method
3.1.1. Sample and Procedure
3.1.2. Measures
3.1.3. Statistical Analyses
3.2. Results
3.2.1. Item Difficulty
3.2.2. Exploratory Factor Analysis (EFA)
4. Study 3: Validation of the Factorial Structure and Relationships with Employee Mental Health
4.1. Method
4.1.1. Sample and Procedure
4.1.2. Measures
4.1.3. Statistical Analyses
4.2. Results
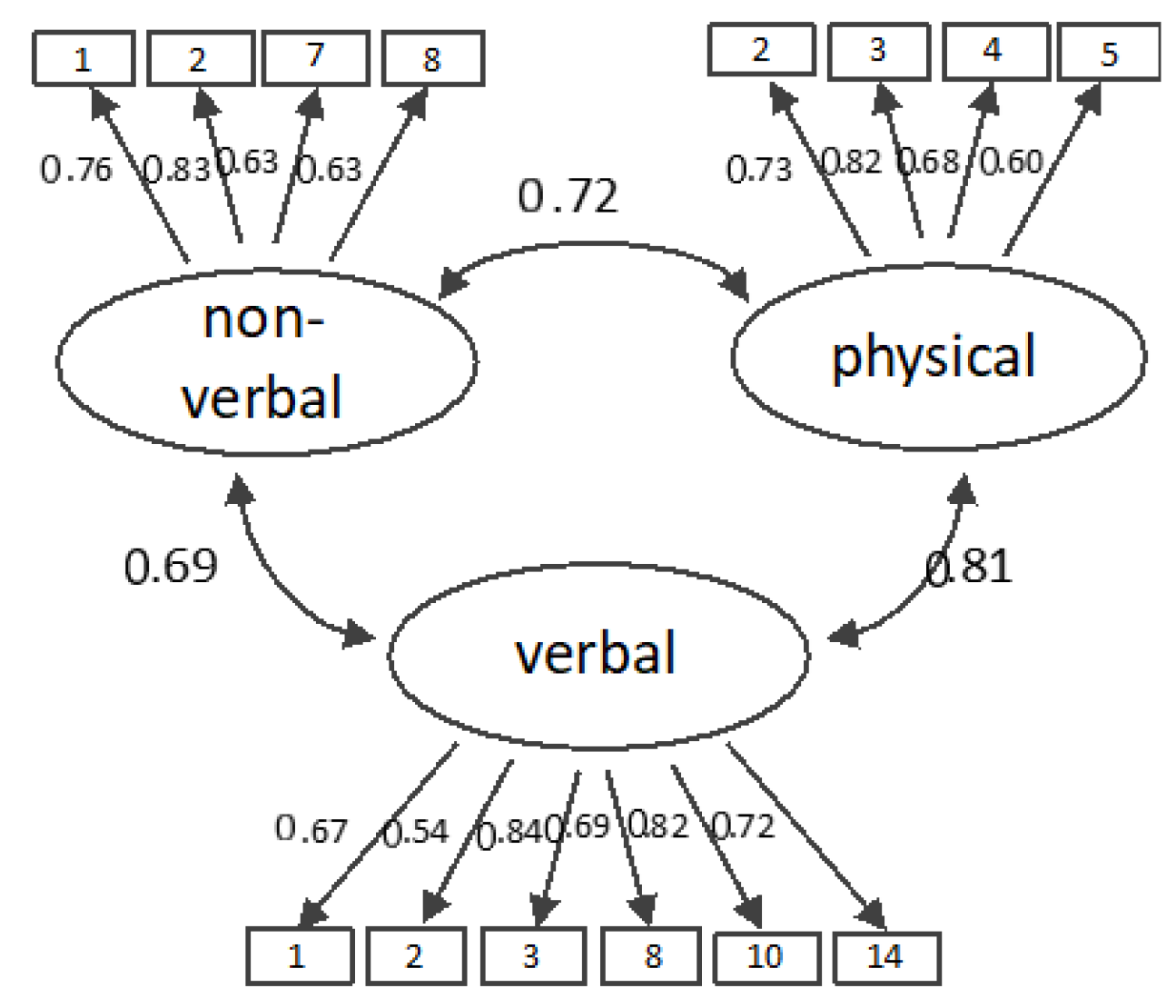
4.2.1. Confirmatory Factor Analysis (CFA)
4.2.2. Correlations between Sexual Harassment and Employee Well-Being
5. Discussion
5.1. Future Directions
5.2. Practical Implications
5.3. Limitations
6. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Data Availability
References
- Quick, J.C.; McFadyen, M. Sexual harassment: Have we made any progress? J. Occup. Health Psychol. 2017, 22, 286–298. [Google Scholar] [CrossRef] [PubMed]
- Barling, J.; Rogers, A.G.; Kelloway, E.K. Behind closed doors: In-home workers’ experience of sexual harassment and workplace violence. J. Occup. Health Psychol. 2001, 6, 255–269. [Google Scholar] [CrossRef] [PubMed]
- Fitzgerald, L.F.; Gelfand, M.J.; Drasgow, F. Measuring sexual harassment: Theoretical and psychometric advances. Basic Appl. Soc. Psychol. 1995, 17, 425–445. [Google Scholar] [CrossRef]
- Nielsen, M.B.D.; Kjær, S.; Aldrich, P.T.; Madsen, I.E.; Friborg, M.K.; Rugulies, R.; Folker, A.P. Sexual harassment in care work - Dilemmas and consequences: A qualitative investigation. Int. J. Nurs. Stud. 2017, 70, 122–130. [Google Scholar] [CrossRef] [PubMed]
- Lengnick-Hall, M.L. Sexual harassment research: A methodological critique. Pers. Psychol. 1995, 48, 841–864. [Google Scholar] [CrossRef]
- Willness, C.R.; Steel, P.; Lee, K. A meta-analysis of the antecedents and consequences of workplace sexual harassment. Pers. Psychol. 2007, 60, 127–162. [Google Scholar] [CrossRef]
- Fitzgerald, L.F.; Shullman, S.L.; Bailey, N.; Richards, M.; Swecker, J.; Gold, Y.; Ormerod, M.; Weitzman, L. The incidence and dimensions of sexual harassment in academia and the workplace. J. Vocat. Behav. 1988, 32, 152–175. [Google Scholar] [CrossRef]
- Schröttle, D.M.; Meshkova, K.; Lehmann, C. Umgang Mit Sexueller Belästigung am Arbeitsplatz—Lösungsstrategien und Maßnahmen zur Intervention; Antidiskriminierungsstelle des Bundes: Berling, Germany, 2019. [Google Scholar]
- Cortina, L.M.; Berdahl, J.L. Sexual harassment in organizations: A decade of research in review. In The Sage Handbook of Organizational Behavior; Barling, J., Cooper, C.L., Eds.; Sage: Thousand Oaks, CA, USA, 2008; pp. 469–497. [Google Scholar]
- Good, L.; Cooper, R. ‘But it’s your job to be friendly’: Employees coping with and contesting sexual harassment from customers in the service sector. Gend. Work Organ. 2016, 23, 447–469. [Google Scholar] [CrossRef]
- Yagil, D. When the customer is wrong: A review of research on aggression and sexual harassment in service encounters. Aggr. Violent Behav. 2008, 13, 141–152. [Google Scholar] [CrossRef]
- Friborg, M.K.; Hansen, J.V.; Aldrich, P.T.; Folker, A.P.; Kjær, S.; Nielsen, M.B.D.; Rugulies, R.; Madsen, I.E. Workplace sexual harassment and depressive symptoms: A cross-sectional multilevel analysis comparing harassment from clients or customers to harassment from other employees amongst 7603 Danish employees from 1041 organizations. BMC Public Health 2017, 17, 675. [Google Scholar] [CrossRef]
- Hanson, G.C.; Perrin, N.A.; Moss, H.; Laharnar, N.; Glass, N. Workplace violence against homecare workers and its relationship with workers health outcomes: A cross-sectional study. BMC Public Health 2015, 15, 11. [Google Scholar] [CrossRef] [PubMed]
- Fitzgerald, L.F.; Swan, S.; Magley, V.J. But was it really sexual harassment? Legal, behavioral, and psychological definitions of the workplace victimization of women. In Sexual Harassment: Theory, Research, and Treatment; O’Donohue, W., Ed.; Allyn & Bacon: Needham Heights, MA, USA, 1997; pp. 5–28. [Google Scholar]
- European Commission. Commission Recommendation of 27 November 1991 on the Protection of the Dignity of Women and Men at Work; European Commission: Brussels, Belgium, 1991. [Google Scholar]
- Barling, J.; Dekker, I.; Loughlin, C.A.; Kelloway, E.K.; Fullagar, C.; Johnson, D. Prediction and replication of the organizational and personal consequences of workplace sexual harassment. J. Manag. Psychol. 1996, 11, 4–25. [Google Scholar] [CrossRef]
- Cantisano, G.T.; Domínguez, J.F.M.; Depolo, M. Perceived sexual harassment at work: Meta-analysis and structural model of antecedents and consequences. Span. J. Psychol. 2008, 11, 207–218. [Google Scholar] [CrossRef] [PubMed]
- Chan, D.K.-S.; Chow, S.Y.; Lam, C.B.; Cheung, S.F. Examining the job-related, psychological, and physical outcomes of workplace sexual harassment: A meta-analytic review. Psychol. Women Q. 2008, 32, 362–376. [Google Scholar] [CrossRef]
- Fitzgerald, L.F.; Drasgow, F.; Hulin, C.L.; Gelfand, M.J.; Magley, V.J. Antecedents and consequences of sexual harassment in organizations: A test of an integrated model. J. Appl. Psychol. 1997, 82, 578–589. [Google Scholar] [CrossRef] [PubMed]
- Magley, V.J.; Hulin, C.L.; Fitzgerald, L.F.; DeNardo, M. Outcomes of self-labeling sexual harassment. J. Appl. Psychol. 1999, 84, 390–402. [Google Scholar] [CrossRef]
- Wasti, S.A.; Bergman, M.E.; Glomb, T.M.; Drasgow, F. Test of the cross-cultural generalizability of a model of sexual harassment. J. Appl. Psychol. 2000, 85, 766–778. [Google Scholar] [CrossRef]
- Larsen, S.E.; Fitzgerald, L.F. PTSD symptoms and sexual harassment: The role of attributions and perceived control. J. Interp. Viol. 2011, 26, 2555–2567. [Google Scholar] [CrossRef]
- Schneider, K.T.; Swan, S.; Fitzgerald, L.F. Job-related and psychological effects of sexual harassment in the workplace: Empirical evidence from two organizations. J. Appl. Psychol. 1997, 82, 401–415. [Google Scholar] [CrossRef]
- Gettman, H.J.; Gelfand, M.J. When the customer shouldn’t be king: Antecedents and consequences of sexual harassment by clients and customers. J. Appl. Psychol. 2007, 92, 757–770. [Google Scholar] [CrossRef]
- Krøjer, J.; Lehn-Christiansen, S.; Nielsen, M.L. Sexual harassment of newcomers in elder care-an institutional practice? Nord. J. Work. Life Stud. 2014, 4, 81–96. [Google Scholar] [CrossRef]
- Spector, P.E.; Zhou, Z.E.; Che, X.X. Nurse exposure to physical and nonphysical violence, bullying, and sexual harassment: A quantitative review. Int. J. Nurs. Stud. 2014, 51, 72–84. [Google Scholar] [CrossRef] [PubMed]
- Koss, M.P. Changed lives: The psychological impact of sexual harassment. In Ivory Power: Sexual Harassment on Campus; Paludi, M.A., Ed.; SUNY series in the psychology of women; State University of New York Press: Albany, NY, USA, 1990; pp. 73–92. [Google Scholar]
- Bronner, G.; Peretz, C.; Ehrenfeld, M. Sexual harassment of nurses and nursing students. J. Adv. Nurs. 2003, 42, 637–644. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Constitution of the World Health Organization; World Health Organization: New York, NY, USA, 2006. [Google Scholar]
- Keyes, C.L. Promoting and protecting mental health as flourishing: A complementary strategy for improving national mental health. Am. Psychol. 2007, 62, 95–108. [Google Scholar]
- Rousseau, V.; Aubé, C.; Chiocchio, F.; Boudrias, J.-S.; Morin, E.M. Social interactions at work and psychological health: The role of leader–member exchange and work group integration. J. Appl. Soc. Psychol. 2008, 38, 1755–1777. [Google Scholar]
- Wright, T.A.; Emich, K.J.; Klotz, D. The many ‘faces’ of well-being. In Research Handbook on Work and Well-Being; Burke, R.J., Page, K.M., Eds.; Edward Elgar Publishing: Cheltenham, UK, 2017; pp. 37–58. [Google Scholar]
- Diener, E. Subjective well-being. Psychol. Bull. 1984, 95, 542–575. [Google Scholar]
- Karademas, E.C. Positive and negative aspects of well-being: Common and specific predictors. Pers. Individ. Differ. 2007, 43, 277–287. [Google Scholar]
- Dormann, C.; Zapf, D. Social stressors at work, irritation, and depressive symptoms: Accounting for unmeasured third variables in a multi-wave study. J. Occup. Organ. Psychol. 2002, 75, 33–58. [Google Scholar] [CrossRef]
- Anti-Discrimination Agency of Germany (Antidiskriminierungsstelle des Bundes). Sexuelle Belästigung am Arbeitsplatz: Ergebnisse Einer Repräsentativen Umfrage unter Beschäftigten in Deutschland; [Sexual Harassment at the Workplace: Results of a Representative Survey among Employees in Germany] 2015; Anti-Discrimination Agency of Germany: Berlin, Germany, 2015. [Google Scholar]
- Huang, J.L.; Curran, P.G.; Keeney, J.; Poposki, E.M.; DeShon, R.P. Detecting and deterring insufficient effort responding to surveys. J. Bus. Psychol. 2012, 27, 99–114. [Google Scholar]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2019. [Google Scholar]
- Maslach, C.; Jackson, S.E. The measurement of experienced burnout. J. Organ. Behav. 1981, 2, 99–113. [Google Scholar]
- Enzmann, D.; Kleiber, D. Helfer-Leiden: Stress und Burnout in psychosozialen Berufen; Asanger: Heidelberg, Germany, 1989. [Google Scholar]
- Maslach, C.; Schaufeli, W.B.; Leiter, M.P. Job burnout. Annu. Rev. Psychol. 2001, 52, 397–422. [Google Scholar] [PubMed]
- Radloff, L.S. The CES-D scale: A self-report depression scale for research in the general population. Appl. Psychol. Meas. 1977, 1, 385–401. [Google Scholar]
- Hautzinger, M.; Bailer, M. Allgemeine Depressions-Skala (ADS) [General Depression Scale]; Beltz: Weinheim, Germany, 1993. [Google Scholar]
- Mohr, G.; Müller, A.; Rigotti, T.; Aycan, Z.; Tschan, F. The assessment of psychological strain in work contexts. Eur. J. Psychol. Assess. 2006, 22, 198–206. [Google Scholar]
- Mohr, G.; Müller, A. Psychosomatische Beschwerden im nichtklinischen Kontext. Zs. Soz. Items Skalen 2014. [Google Scholar] [CrossRef]
- Bech, P. Measuring the dimension of psychological general well-being by the WHO-5. Qual. Life Newsl. 2004, 32, 15–16. [Google Scholar]
- Brähler, E.; Mühlan, H.; Albani, C.; Schmidt, S. Teststatistische Prüfung und Normierung der deutschen Versionen des EUROHIS-QOL Lebensqualität-Index und des WHO-5 Wohlbefindens-Index [Statistical examination and standardization of the German versions of the EUROHIS-QOL life-quality index and the WHO-5 well-being index]. Diagnostica 2007, 53, 83–96. [Google Scholar]
- Kristensen, T.S.; Hannerz, H.; Høgh, A.; Borg, V. The Copenhagen Psychosocial Questionnaire − A tool for the assessment and improvement of the psychosocial work environment. Scand. J. Work. Environ. Health 2005, 31, 438–449. [Google Scholar]
- Nübling, M.; Stößel, U.; Hasselhorn, H.M.; Michaelis, M.; Hofmann, F. Methoden zur Erfassung psychischer Belastungen. Erprobung eines Messinstrumentes (COPSOQ); Bundesanstalt für Arbeitsschutz Arbeitsmedizi: Dortmund, Germany, 2005. [Google Scholar]
- Rosseel, Y. Lavaan: An R package for structural equation modeling. J. Stat. Softw. 2012, 48, 1–36. [Google Scholar]
- Bearden, W.O.; Sharma, S.; Teel, J.E. Sample size effects on chi square and other statistics used in evaluating causal models. J. Mark. Res. 1982, 19, 425–430. [Google Scholar]
- Hu, L.; Bentler, P.M. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct. Equ. Model. Multidiscip. J. 1999, 6, 1–55. [Google Scholar]
- Semmer, N.; Zapf, D.; Greif, S. ‘Shared job strain’: A new approach for assessing the validity of job stress measurements. J. Occup. Organ. Psychol. 1996, 69, 293–310. [Google Scholar] [CrossRef]
- Pina, A.; Gannon, T.A. An overview of the literature on antecedents, perceptions and behavioural consequences of sexual harassment. J. Sex. Aggress. 2012, 18, 209–232. [Google Scholar] [CrossRef]
- Bakker, A.B.; Demerouti, E. The job demands-resources model: State of the art. J. Manag. Psychol. 2007, 22, 309–328. [Google Scholar] [CrossRef]
- Archibald, C. Sexuality and dementia in residential care - whose responsibility? Sex. Relatsh. Ther. 2002, 17, 301–309. [Google Scholar] [CrossRef]
- Semmer, N.K. Job stress interventions and the organization of work. Scand. J. Work. Environ. Health 2006, 32, 515–527. [Google Scholar] [CrossRef]
- Biron, C.; Gatrell, C.; Cooper, C.L. Autopsy of a failure: Evaluating process and contextual issues in an organizational-level work stress intervention. Int. J. Stress Manag. 2010, 17, 135–158. [Google Scholar] [CrossRef]
- Erdogan, B.; Enders, J. Support from the top: Supervisors’ perceived organizational support as a moderator of leader-member exchange to satisfaction and performance relationships. J. Appl. Psychol. 2007, 92, 321–330. [Google Scholar] [CrossRef]
- Zapf, D.; Dormann, C.; Frese, M. Longitudinal studies in organizational stress research: A review of the literature with reference to methodological issues. J. Occup. Health Psychol. 1996, 1, 145–169. [Google Scholar] [CrossRef]
- Podsakoff, P.M.; MacKenzie, S.B.; Lee, J.-Y.; Podsakoff, N.P. Common method biases in behavioral research: A critical review of the literature and recommended remedies. J. Appl. Psychol. 2003, 88, 879–903. [Google Scholar] [CrossRef]
- Semmer, N.K.; Grebner, S.; Elfering, A. Beyond self-report: Using observational, physiological, and situation-based measures in research on occupational stress. In Emotional and Physiological Processes and Positive Intervention Strategies; Research in Occupational Stress and Well-being; Perrewe, P.L., Ganster, D.C., Eds.; Emerald Group Publishing Limited: Amsterdam, The Netherlands, 2003; pp. 205–263. [Google Scholar]


{kind=link}
| Title | Initial Set of 16 Items | Final Set of 14 Items | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Item | Item Wording | % “never” | 1 | 2 | 3 | h2 | 1 | 2 | 3 | h2 |
| Nonverbal 1 | I have witnessed sexual acts (e.g., masturbation). | 48.0 | 0.80 | 0.69 | 0.81 | 0.69 | ||||
| Nonverbal 2 | I have witnessed sexual gestures. | 32.4 | 0.69 | 0.71 | 0.69 | 0.69 | ||||
| Nonverbal 3 | I have been leered/stared at. | 33.0 | 0.52 | 0.32 | 0.63 | |||||
| Nonverbal 4 | Someone has unnecessarily exposed themselves in front of me. | 67.6 | 0.68 | 0.59 | 0.67 | 0.57 | ||||
| Nonverbal 5 | I have witnessed sexual harassment/violence among patients/clients/residents. | 65.4 | 0.79 | 0.56 | 0.78 | 0.57 | ||||
| Verbal 1 | I have been whistled at. | 49.2 | 0.77 | 0.55 | 0.71 | 0.53 | ||||
| Verbal 2 | I have received repeated requests for dates. | 75.4 | 0.62 | 0.45 | 0.61 | 0.46 | ||||
| Verbal 3 | I have been sexually complimented. | 34.6 | 0.88 | 0.74 | 0.84 | 0.73 | ||||
| Verbal 4 | I have been told suggestive/offensive stories or jokes. | 35.2 | 0.56 | 0.50 | 0.57 | 0.52 | ||||
| Verbal 5 | I have been exposed to verbal sexual innuendo. | 42.5 | 0.63 | 0.70 | 0.62 | 0.71 | ||||
| Verbal 6 | I have been asked intrusive or personal questions by a client (e.g., requests for body measurements, relationship status, sexual preferences). | 62.0 | 0.66 | 0.55 | 0.68 | 0.59 | ||||
| Physical 1 | I have experienced someone unnecessarily close/breaking personal boundaries. | 34.1 | 0.43 | 0.36 | 0.57 | |||||
| Physical 2 | I have been hugged in a way that made me feel uncomfortable. | 65.4 | 0.76 | 0.66 | 0.72 | 0.63 | ||||
| Physical 3 | I have been petted or patted in a way that made me feel uncomfortable. | 63.7 | 0.85 | 0.77 | 0.84 | 0.75 | ||||
| Physical 4 | I have been touched in a way that made me feel uncomfortable. | 71.0 | 0.75 | 0.62 | 0.76 | 0.64 | ||||
| Physical 5 | I have been kissed in a way that made me feel uncomfortable. | 82.1 | 0.67 | 0.40 | 0.67 | 0.43 | ||||
| Eigenvalue | 7.98 | 1.73 | 1.14 | 6.85 | 1.69 | 1.13 | ||||
| Variance accounted for (%) | 49.90 | 10.84 | 7.11 | 48.92 | 12.06 | 8.08 | ||||
| Verbal 7 | I have been targeted for rumors of sexual promiscuity. | 87.7 | ||||||||
| Verbal 8 | I have been exposed to insults that targeted my sexual orientation. | 90.5 | ||||||||
| Verbal 9 | I have been offered money for sex. | 92.7 | ||||||||
| Physical 6 | I have been cornered or placed in a position that was difficult to get out of. | 95.0 | ||||||||
| Scale | M | SD | α |
|---|---|---|---|
| Nonverbal sexual harassment | 1.95 | 1.04 | 0.86 |
| Verbal sexual harassment | 2.04 | 1.02 | 0.89 |
| Physical sexual harassment | 1.49 | 0.78 | 0.85 |
| Variables | M | SD | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 Nonverbal SH | 1.45 | 0.69 | (0.79) | ||||||||
| 2 Verbal SH | 1.69 | 0.83 | 0.57 *** | (0.86) | |||||||
| 3 Physical SH | 1.38 | 0.65 | 0.60 *** | 0.67 *** | (0.80) | ||||||
| 4 Emotional exhaustion | 2.98 | 1.29 | 0.21 *** | 0.21 *** | 0.26 *** | (0.94) | |||||
| 5 Strain | 2.61 | 1.27 | 0.16 ** | 0.13 * | 0.18 ** | 0.53 *** | (0.89) | ||||
| 6 Depressive symptoms | 2.38 | 1.30 | 0.27 *** | 0.26 *** | 0.27 *** | 0.64 *** | 0.53 *** | (0.94) | |||
| 7 Psychosomatic complaints | 2.32 | 0.83 | 0.25 *** | 0.27 *** | 0.25 *** | 0.67 *** | 0.46 *** | 0.74 *** | (0.88) | ||
| 8 Positive well-being | 3.26 | 0.89 | −0.24 *** | −0.21 *** | −0.28 *** | −0.56 *** | −0.46 *** | −0.64 *** | −0.63 *** | (0.92) | |
| 9 Job satisfaction | 3.55 | 0.87 | −0.15* | −0.09 | −0.24 *** | −0.56 *** | −0.35 *** | −0.49 *** | −0.47 *** | 0.54 *** | (0.91) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vincent-Höper, S.; Adler, M.; Stein, M.; Vaupel, C.; Nienhaus, A. Sexually Harassing Behaviors from Patients or Clients and Care Workers’ Mental Health: Development and Validation of a Measure. Int. J. Environ. Res. Public Health 2020, 17, 2570. https://doi.org/10.3390/ijerph17072570
Vincent-Höper S, Adler M, Stein M, Vaupel C, Nienhaus A. Sexually Harassing Behaviors from Patients or Clients and Care Workers’ Mental Health: Development and Validation of a Measure. International Journal of Environmental Research and Public Health. 2020; 17(7):2570. https://doi.org/10.3390/ijerph17072570
Chicago/Turabian StyleVincent-Höper, Sylvie, Mareike Adler, Maie Stein, Claudia Vaupel, and Albert Nienhaus. 2020. "Sexually Harassing Behaviors from Patients or Clients and Care Workers’ Mental Health: Development and Validation of a Measure" International Journal of Environmental Research and Public Health 17, no. 7: 2570. https://doi.org/10.3390/ijerph17072570
APA StyleVincent-Höper, S., Adler, M., Stein, M., Vaupel, C., & Nienhaus, A. (2020). Sexually Harassing Behaviors from Patients or Clients and Care Workers’ Mental Health: Development and Validation of a Measure. International Journal of Environmental Research and Public Health, 17(7), 2570. https://doi.org/10.3390/ijerph17072570