Spatial Variability of Heat-Related Mortality in Barcelona from 1992–2015: A Case Crossover Study Design

 , , , , ,
, , , , ,  ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population and Characteristics
2.2. Urban Climate Model (UrbClim)
2.3. Exposure Definition and Lags Structures
2.4. Statistical Method/Analysis
3. Results
3.1. Heat-Related Mortality in Barcelona
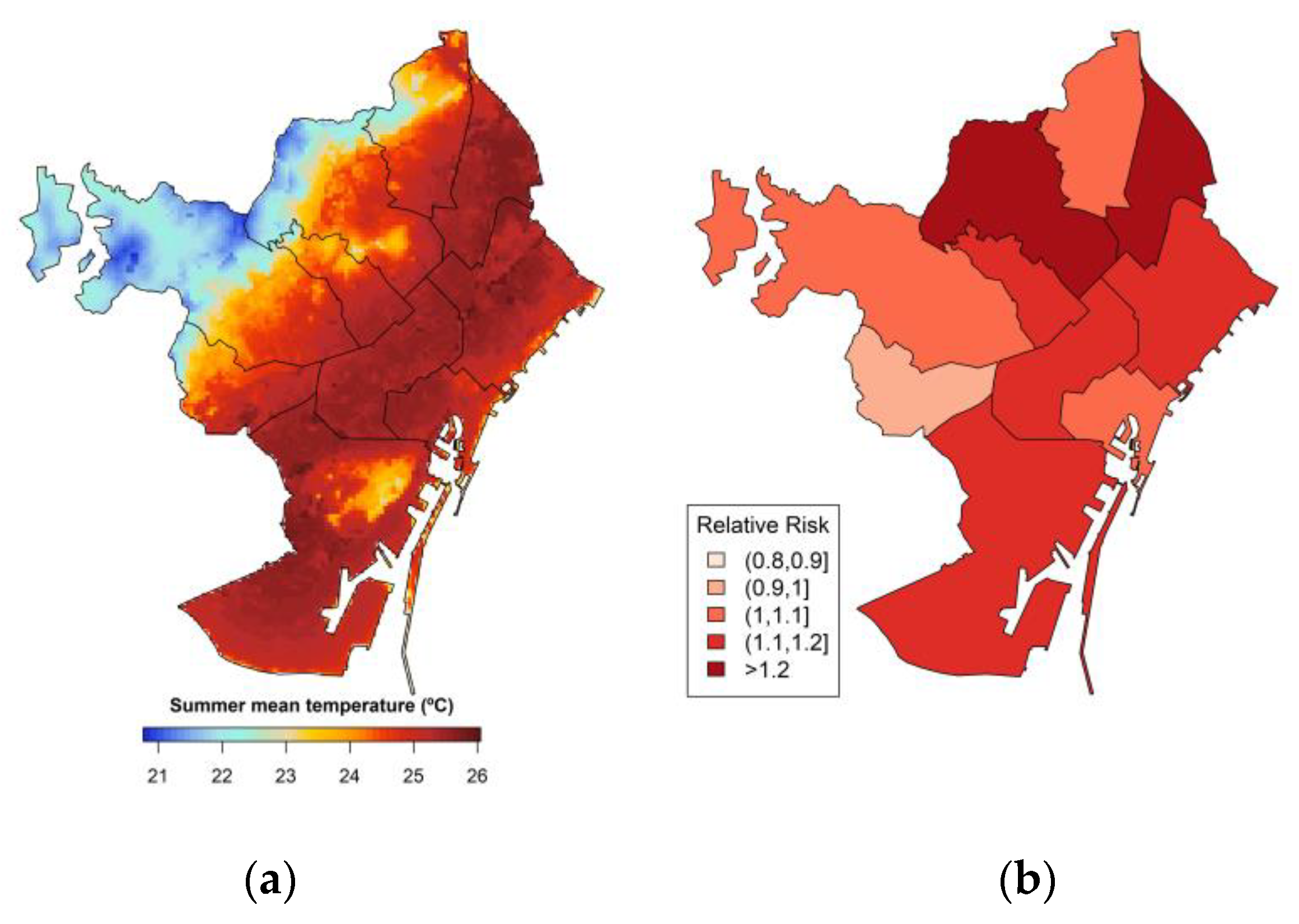
3.2. The Spatial Distribution of Heat-Related Mortality by District
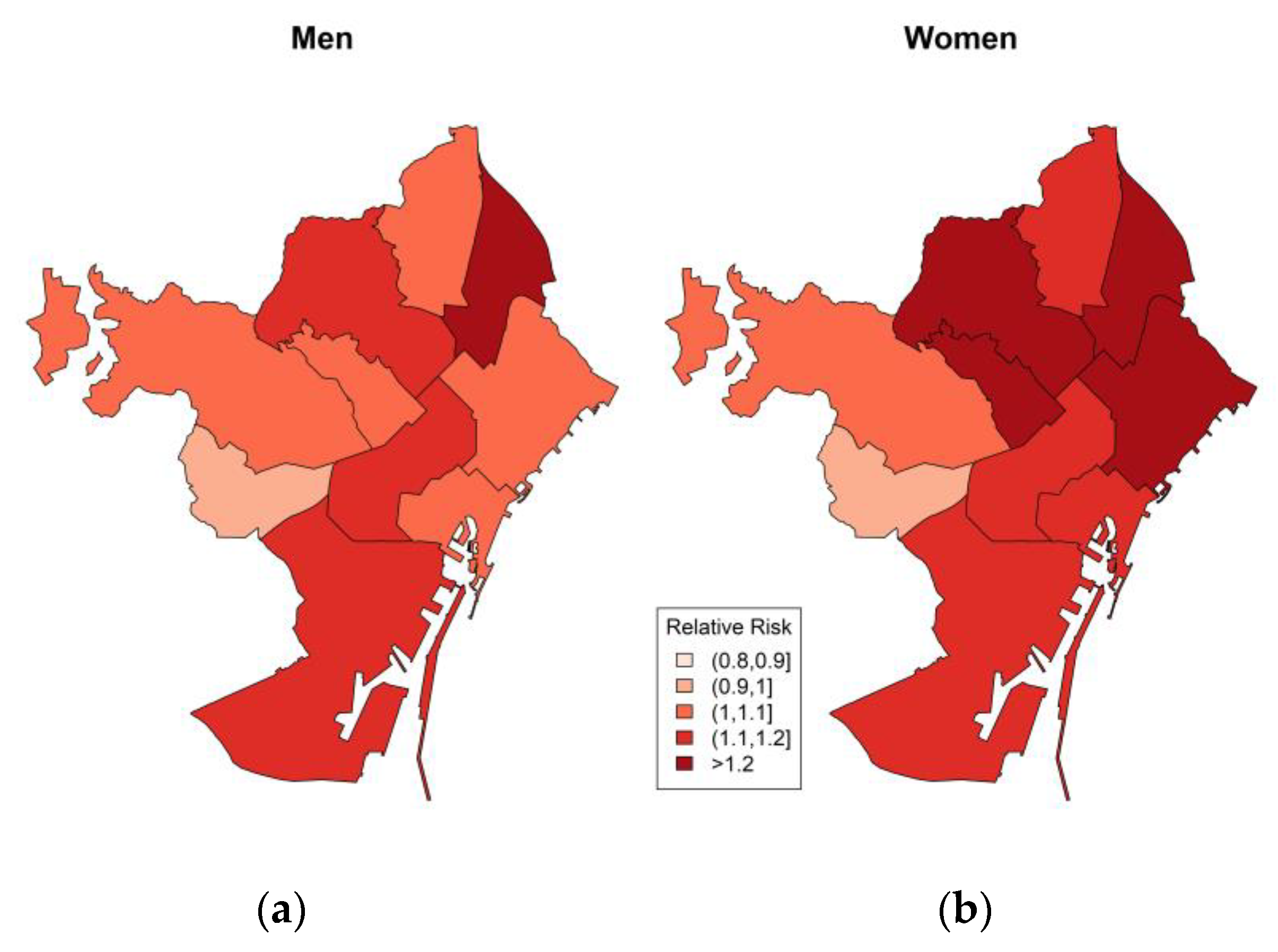
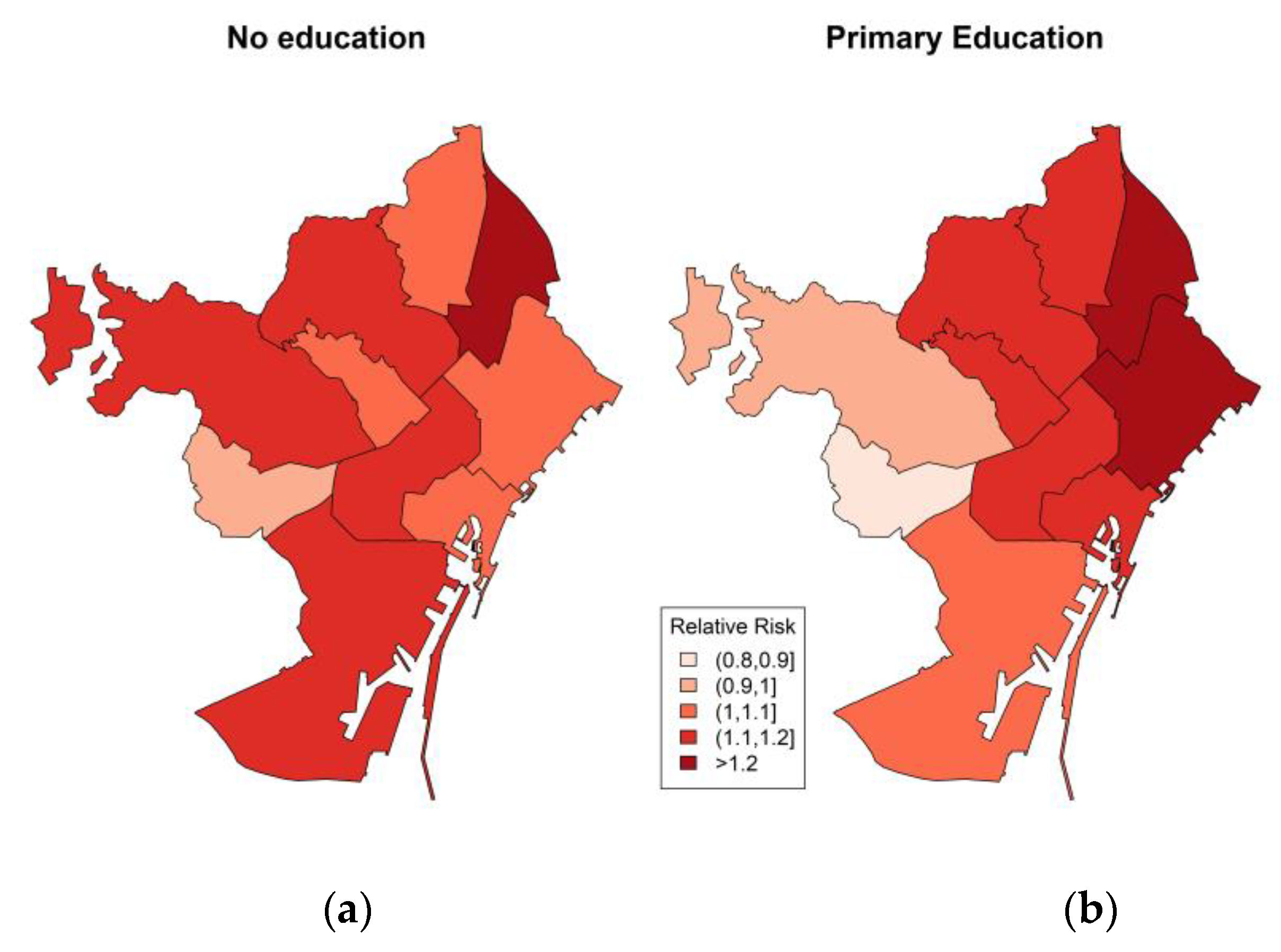
3.3. The Spatial Distribution of Heat-Related Mortality Results Stratified by Age, Sex and Education
4. Discussion
4.1. Summary of Main Results
4.2. Spatial Differences by Age, Sex and Education
4.3. Socio-Economic and Built Environmental Factors
5. Strengths and Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Barnett, A.; Morawska, L. Virtual Special Issue: “The Impact of Temperature on Human Health: New Insights”; Faculty of Health, Institute of Health and Biomedical Innovation, Science and Engineering Faculty, Queensland University of Technology: Brisbane, Australia, 2015. [Google Scholar]
- Howe, P.D.; Marlon, J.; Wang, X.; Leiserowitz, A. Public perceptions of the health risks of extreme heat across US states, counties, and neighborhoods. Proc. Natl. Acad. Sci. USA 2019, 116, 6743–6748. [Google Scholar] [CrossRef] [PubMed]
- Guo, Y.; Gasparrini, A.; Li, S.; Sera, F.; Cabrera, A.M.V.; Coelho, M.; Saldiva, P.H.; Lavigne, E.; Tawatsupa, B.; Punnasiri, K.; et al. Quantifying excess deaths related to heatwaves under climate change scenarios: A multicountry time series modelling study. PLoS Med. 2018, 15, e1002629. [Google Scholar] [CrossRef] [PubMed]
- Guo, Y.; Gasparrini, A.; Armstrong, B.G.; Tawatsupa, B.; Tobias, A.; Lavigne, E.; Coelho, M.; Pan, X.; Kim, H.; Hashizume, M.; et al. Heat Wave and Mortality: A Multicountry, Multicommunity Study. Environ. Heal. Perspect. 2017, 125, 087006. [Google Scholar] [CrossRef] [PubMed]
- Marí-Dell’Olmo, M.; Tobias, A.; Gómez-Gutiérrez, A.; Rodríguez-Sanz, M.; De Olalla, P.G.; Camprubí, E.; Gasparrini, A.; Borrell, C. Social inequalities in the association between temperature and mortality in a South European context. Int. J. Public Heal. 2018, 64, 27–37. [Google Scholar] [CrossRef] [PubMed]
- Borrell, C.; Marí-Dell’Olmo, M.; Rodríguez-Sanz, M.; Garcia-Olalla, P.; Caylà, J.A.; Benach, J.; Muntaner, C. Socioeconomic position and excess mortality during the heat wave of 2003 in Barcelona. Eur. J. Epidemiology 2006, 21, 633–640. [Google Scholar] [CrossRef]
- Bell, M.; O’Neill, M.S.; Ranjit, N.; Borja-Aburto, V.H.; A Cifuentes, L.; Gouveia, N. Vulnerability to heat-related mortality in Latin America: A case-crossover study in São Paulo, Brazil, Santiago, Chile and Mexico City, Mexico. Int. J. Epidemiology 2008, 37, 796–804. [Google Scholar] [CrossRef]
- Dang, T.N.; Van, D.Q.; Kusaka, H.; Seposo, X.; Honda, Y. Green Space and Deaths Attributable to the Urban Heat Island Effect in Ho Chi Minh City. Am. J. Public Heal. 2017, 108, S137–S143. [Google Scholar] [CrossRef]
- Johnson, D.P.; Wilson, J.S. The socio-spatial dynamics of extreme urban heat events: The case of heat-related deaths in Philadelphia. Appl. Geogr. 2009, 29, 419–434. [Google Scholar] [CrossRef]
- Kalkstein, L.S.; Davis, R.E. Weather and Human Mortality: An Evaluation of Demographic and Interregional Responses in the United States. Ann. Assoc. Am. Geogr. 1989, 79, 44–64. [Google Scholar] [CrossRef]
- Smoyer, K.E. Putting risk in its place: Methodological considerations for investigating extreme event health risk. Soc. Sci. Med. 1998, 47, 1809–1824. [Google Scholar] [CrossRef]
- Asumadu-Sakyi, A.; Barnett, A.; Thai, P.; Jayaratne, E.; Miller, W.; Thompson, M.H.; Roghani, R.; Morawska, L.; Roughani, R. The relationship between indoor and outdoor temperature in warm and cool seasons in houses in Brisbane, Australia. Energy Build. 2019, 191, 127–142. [Google Scholar] [CrossRef]
- Hu, K.; Guo, Y.; Hochrainer-Stigler, S.; Liu, W.; See, L.; Yang, X.; Zhong, J.; Fei, F.; Chen, F.; Zhang, Y.; et al. Evidence for Urban–Rural Disparity in Temperature–Mortality Relationships in Zhejiang Province, China. Environ. Heal. Perspect. 2019, 127, 37001. [Google Scholar] [CrossRef] [PubMed]
- Madrigano, J.; McCormick, S.; Kinney, P.L. The Two Ways of Assessing Heat-Related Mortality and Vulnerability. Am. J. Public Heal. 2015, 105, 2212–2213. [Google Scholar] [CrossRef]
- Wan, Z. New refinements and validation of the MODIS Land-Surface Temperature/Emissivity products. Remote. Sens. Environ. 2008, 112, 59–74. [Google Scholar] [CrossRef]
- De Ridder, K.; Lauwaet, D.; Maiheu, B. UrbClim – A fast urban boundary layer climate model. Urban Clim. 2015, 12, 21–48. [Google Scholar] [CrossRef]
- Lauwaet, D.; De Ridder, K.; Saeed, S.; Brisson, E.; Chatterjee, F.; Van Lipzig, N.; Maiheu, B.; Hooyberghs, H. Assessing the current and future urban heat island of Brussels. Urban Clim. 2016, 15, 1–15. [Google Scholar] [CrossRef]
- Xu, Y.; Dadvand, P.; Barrera-Gómez, J.; Sartini, C.; Marí-Dell’Olmo, M.; Borrell, C.; Medina-Ramón, M.; Sunyer, J.; Basagaña, X. Differences on the effect of heat waves on mortality by sociodemographic and urban landscape characteristics. J. Epidemiology Community Heal. 2013, 67, 519–525. [Google Scholar] [CrossRef] [PubMed]
- Mendelsohn, R.; Dinar, A.; Williams, L. The distributional impact of climate change on rich and poor countries. Environ. Dev. Econ. 2006, 11, 159–178. [Google Scholar] [CrossRef]
- Laaidi, K.; Zeghnoun, A.; Dousset, B.; Bretin, P.; Vandentorren, S.; Giraudet, E.; Beaudeau, P. The Impact of Heat Islands on Mortality in Paris during the August 2003 Heat Wave. Environ. Heal. Perspect. 2011, 120, 254–259. [Google Scholar] [CrossRef]
- García-Díez, M.; Lauwaet, D.; Hooyberghs, H.; Ballester, J.; De Ridder, K.; Rodo, X. Advantages of using a fast urban boundary layer model as compared to a full mesoscale model to simulate the urban heat island of Barcelona. Geosci. Model Dev. 2016, 9, 4439–4450. [Google Scholar] [CrossRef]
- Martinez, G.S.; Gimeno, L.; Hooyberghs, H.; Lauwaet, D.; De Ridder, K.; Linares, C.; Carmona, R.; Ortiz, C.; Kendrovski, V.; Aerts, R.; et al. Heat and health in Antwerp under climate change: Projected impacts and implications for prevention. Environ. Int. 2017, 111, 135–143. [Google Scholar] [CrossRef] [PubMed]
- Hashizume, M.; Wagatsuma, Y.; Hayashi, T.; Saha, S.K.; Streatfield, K.; Yunus, M. The effect of temperature on mortality in rural Bangladesh—a population-based time-series study. Int. J. Epidemiology 2009, 38, 1689–1697. [Google Scholar] [CrossRef] [PubMed]
- Levy, D.; Lumley, T.; Sheppard, L.; Kaufman, J.D.; Checkoway, H. Referent Selection in Case-Crossover Analyses of Acute Health Effects of Air Pollution. Epidemiology 2001, 12, 186–192. [Google Scholar] [CrossRef] [PubMed]
- Lu, Y.; Zeger, S.L. On the equivalence of case-crossover and time series methods in environmental epidemiology. Biostatistics 2006, 8, 337–344. [Google Scholar] [CrossRef] [PubMed]
- Stafoggia, M.; Forastiere, F.; Agostini, D.; Biggeri, A.; Bisanti, L.; Cadum, E.; Caranci, N.; Donato, F.K.D.; De Lisio, S.; De Maria, M.; et al. Vulnerability to Heat-Related Mortality. Epidemiology 2006, 17, 315–323. [Google Scholar] [CrossRef] [PubMed]
- Heaton, M.J.; Olenick, C.R.; Wilhelmi, O. Age-specific distributed lag models for heat - related mortality. Environmetrics 2019, 30, e2561. [Google Scholar] [CrossRef]
- Hondula, D.M.; Davis, R.E.; Leisten, M.J.; Saha, M.V.; Veazey, L.M.; Wegner, C.R. Fine-scale spatial variability of heat-related mortality in Philadelphia County, USA, from 1983-2008: A case-series analysis. Environ. Heal. 2012, 11, 16. [Google Scholar] [CrossRef]
- Achebak, H.; Devolder, D.; Ballester, J. Heat-related mortality trends under recent climate warming in Spain: A 36-year observational study. PLoS Med. 2018, 15, e1002617. [Google Scholar] [CrossRef]
- Curriero, F.C.; Heiner, K.S.; Samet, J.M.; Zeger, S.L.; Strug, L.; Patz, J.A. Temperature and mortality in 11 cities of the eastern United States. Am. J. Epidemiology 2002, 155, 80–87. [Google Scholar] [CrossRef]
- Gronlund, C.J. Racial and Socioeconomic Disparities in Heat-Related Health Effects and Their Mechanisms: A Review. Curr. Epidemiology Rep. 2014, 1, 165–173. [Google Scholar] [CrossRef]
- O’Neill, M.S.; Zanobetti, A.; Schwartz, J. Disparities by race in heat-related mortality in four US cities: The role of air conditioning prevalence. J. Hered. 2014, 82, 191–197. [Google Scholar] [CrossRef] [PubMed]
- Medina-Ramón, M.; Zanobetti, A.; Cavanagh, D.P.; Schwartz, J. Extreme Temperatures and Mortality: Assessing Effect Modification by Personal Characteristics and Specific Cause of Death in a Multi-City Case-Only Analysis. Environ. Heal. Perspect. 2006, 114, 1331–1336. [Google Scholar] [CrossRef] [PubMed]
- Taylor, J.; Wilkinson, P.; Davies, M.; Armstrong, B.; Chalabi, Z.; Mavrogianni, A.; Symonds, P.; Oikonomou, E.; Bohnenstengel, S.I. Mapping the effects of urban heat island, housing, and age on excess heat-related mortality in London. Urban Clim. 2015, 14, 517–528. [Google Scholar] [CrossRef]
- Von Klot, S.; Paciorek, C.; Melly, S.; Coull, B.; Dutton, J.; Schwartz, J. Association of Temperature at Residence Vs Central Site Temperature with Mortality in Eastern Massachusetts—A Case Crossover Analysis. Epidemiology 2009, 20, S75. [Google Scholar] [CrossRef]
- Lee, M.; Shi, L.; Zanobetti, A.; Schwartz, J.D. Study on the association between ambient temperature and mortality using spatially resolved exposure data. Environ. Res. 2016, 151, 610–617. [Google Scholar] [CrossRef] [PubMed]
- Spangler, K.R.; Weinberger, K.; Wellenius, G.A. Suitability of gridded climate datasets for use in environmental epidemiology. J. Expo. Sci. Environ. Epidemiology 2018, 29, 777–789. [Google Scholar] [CrossRef]
- Kuras, E.R.; Richardson, M.B.; Calkins, M.; Ebi, K.L.; Hess, J.J.; Kintziger, K.W.; Jagger, M.A.; Middel, A.; Scott, A.A.; Spector, J.T.; et al. Opportunities and Challenges for Personal Heat Exposure Research. Environ. Heal. Perspect. 2017, 125, 085001. [Google Scholar] [CrossRef]
- Royé, D.; Íñiguez, C.; Tobías, A. Comparison of temperature–mortality associations using observed weather station and reanalysis data in 52 Spanish cities. Environ. Res. 2020, 183, 109237. [Google Scholar] [CrossRef]
- Nelson, J.K.; Brewer, C.A. Evaluating data stability in aggregation structures across spatial scales: revisiting the modifiable areal unit problem. Cartogr. Geogr. Inf. Sci. 2015, 44, 1–16. [Google Scholar] [CrossRef]
- Rodríguez-Sanz, M.; Gotsens, M.; Marí-Dell’Olmo, M.; Borrell, C. Trends in mortality inequalities in an urban area: The influence of immigration. Int. J. Equity Heal. 2019, 18, 37. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | n | % |
|---|---|---|
| Sex | ||
| Men | 51,556 | 48.84 |
| Women | 54,003 | 51.16 |
| Total | 105,559 | 100 |
| Age | ||
| <79 | 48,788 | 46.22 |
| ≥80 | 56,771 | 53.78 |
| Total | 105,559 | 100 |
| Education * | ||
| No Education | 32,894 | 46.92 |
| With Education | 37,216 | 53.08 |
| Total | 70,110 | 100 |
| Temperature Variables | Mean | Std. Dev. | Minimum | Maximum |
|---|---|---|---|---|
| Mean Temperature | 25.25 | 2.90 | 13.24 | 34.05 |
| Maximum Temperature | 28.39 | 3.23 | 14.51 | 40.52 |
| Minimum Temperature | 22.05 | 2.99 | 10.00 | 30.71 |
| Percentile 70th of mean temperature | 26.90 | 4.44 | 22.63 | 27.63 |
| Percentile 30th of mean temperature | 23.78 | 0.452 | 19.57 | 24.54 |
| Characteristics | Lag 0–3 days | |
|---|---|---|
| Relative Risk | 95% CI | |
| All-cause mortality | 1.13 | 1.10–1.16 |
| Sex | ||
| Men | 1.10 | 1.06–1.14 |
| Women | 1.16 | 1.12–1.21 |
| Age | ||
| <79 | 1.08 | 1.04–1.12 |
| ≥80 | 1.18 | 1.13–1.22 |
| Education * | ||
| No Education | 1.10 | 1.05–1.15 |
| With Education | 1.13 | 1.08–1.18 |
| District Name | Lag 0–3 days | ||
|---|---|---|---|
| Relative Risk | 95% CI | ||
| Cuitat Vella | 1.09 | 0.99 | 1.21 |
| Eixample | 1.17 | 1.10 | 1.24 |
| Sants-Montjuïc | 1.12 | 1.03 | 1.21 |
| Les Corts | 0.95 | 0.83 | 1.08 |
| Sarrià-Sant Gervasi | 1.04 | 0.95 | 1.15 |
| Gràcia | 1.14 | 1.04 | 1.26 |
| Horta-Guinardó | 1.20 | 1.10 | 1.31 |
| Nou-Barris | 1.08 | 0.99 | 1.18 |
| Sant Andreu | 1.25 | 1.14 | 1.38 |
| Sant Martí | 1.14 | 1.06 | 1.23 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ingole, V.; Marí-Dell’Olmo, M.; Deluca, A.; Quijal, M.; Borrell, C.; Rodríguez-Sanz, M.; Achebak, H.; Lauwaet, D.; Gilabert, J.; Murage, P.; et al. Spatial Variability of Heat-Related Mortality in Barcelona from 1992–2015: A Case Crossover Study Design. Int. J. Environ. Res. Public Health 2020, 17, 2553. https://doi.org/10.3390/ijerph17072553
Ingole V, Marí-Dell’Olmo M, Deluca A, Quijal M, Borrell C, Rodríguez-Sanz M, Achebak H, Lauwaet D, Gilabert J, Murage P, et al. Spatial Variability of Heat-Related Mortality in Barcelona from 1992–2015: A Case Crossover Study Design. International Journal of Environmental Research and Public Health. 2020; 17(7):2553. https://doi.org/10.3390/ijerph17072553
Chicago/Turabian StyleIngole, Vijendra, Marc Marí-Dell’Olmo, Anna Deluca, Marcos Quijal, Carme Borrell, Maica Rodríguez-Sanz, Hicham Achebak, Dirk Lauwaet, Joan Gilabert, Peninah Murage, and et al. 2020. "Spatial Variability of Heat-Related Mortality in Barcelona from 1992–2015: A Case Crossover Study Design" International Journal of Environmental Research and Public Health 17, no. 7: 2553. https://doi.org/10.3390/ijerph17072553
APA StyleIngole, V., Marí-Dell’Olmo, M., Deluca, A., Quijal, M., Borrell, C., Rodríguez-Sanz, M., Achebak, H., Lauwaet, D., Gilabert, J., Murage, P., Hajat, S., Basagaña, X., & Ballester, J. (2020). Spatial Variability of Heat-Related Mortality in Barcelona from 1992–2015: A Case Crossover Study Design. International Journal of Environmental Research and Public Health, 17(7), 2553. https://doi.org/10.3390/ijerph17072553