CB-Art Interventions Implemented with Mental Health Professionals Working in a Shared War Reality: Transforming Negative Images and Enhancing Coping Resources


Abstract
1. Introduction
The Current Study
2. Methods
2.1. CB-Art Intervention Description
2.2. Sample
2.3. Measures
2.3.1. Distress Level
2.3.2. Compositional Elements
2.3.3. Statistical Analyses
3. Results
3.1. Pre–Post SUDS Scores
3.2. Compositional Characteristics of the Mhps’ Drawings and Their Explanatory Narratives
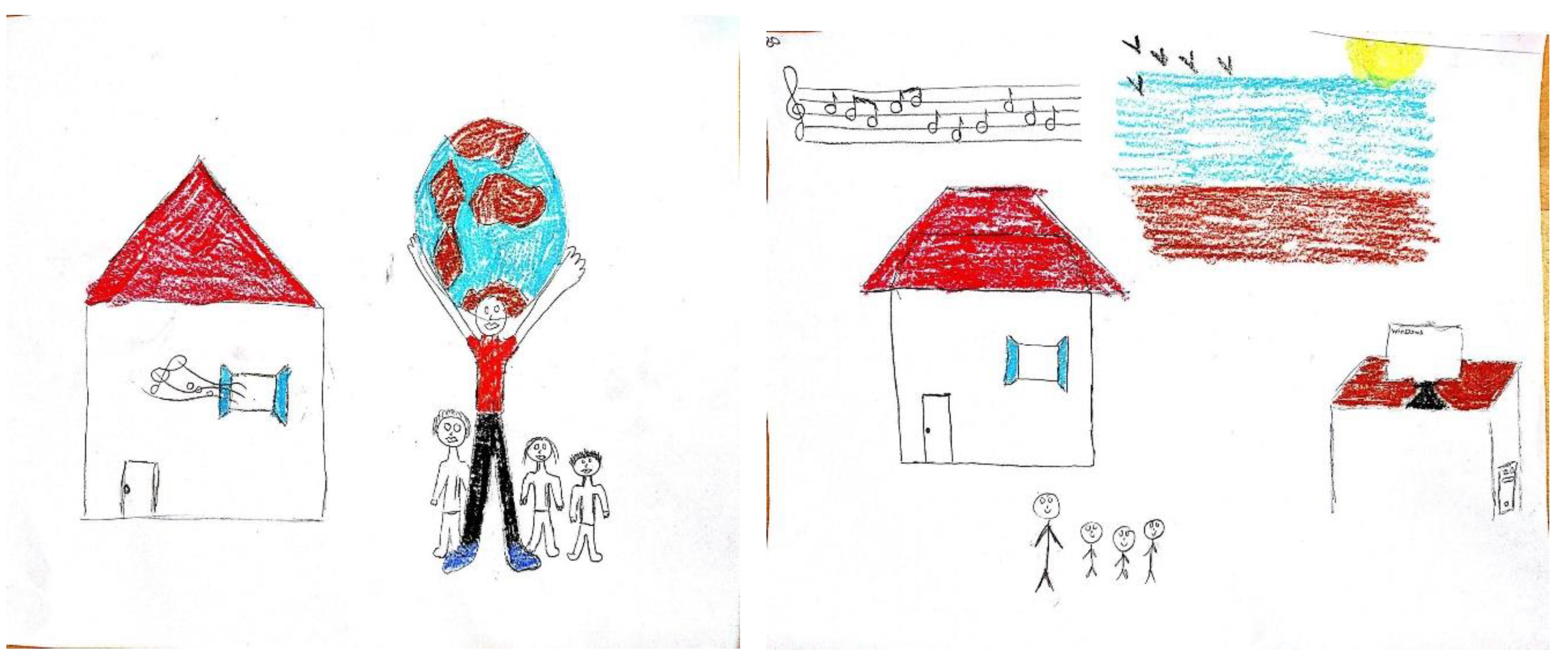
Illustrative Examples of the Drawings
3.3. SUDS-Difference Scores by the Selected Format of the Integrated Drawing and Compositional Transformations
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Israel Ministry of Foreign Affairs. The 2014 Gaza Conflict: Factual and Legal Aspects. Jerusalem: Ministry of Foreign Affairs. 2015. Available online: https://mfa.gov.il/MFA/ForeignPolicy/IsraelGaza2014/Pages/2014-Gaza-Conflict-Factual-and-Legal-Aspects.aspx (accessed on 30 January 2020).
- Baum, N. Professionals’ double exposure in the shared traumatic reality of wartime: Contributions to professional growth and stress. Br. J. Soc. Work 2014, 44, 2113–2134. [Google Scholar] [CrossRef]
- Saakvitne, K. Shared trauma: The therapists’ increased vulnerability. Psychoanal. Dialogues 2002, 12, 443–450. [Google Scholar] [CrossRef]
- Tosone, C.; Nuttman-Shwartz, O.; Stephens, T. Shared trauma: When the professional is personal. Clin. Soc. Work J. 2012, 40, 231–239. [Google Scholar] [CrossRef]
- Dekel, R.; Baum, N. Intervention in a shared traumatic reality: A new challenge for social workers. Br. J. Soc. Work 2010, 40, 1927–1944. [Google Scholar] [CrossRef]
- Freedman, S.A.; Mashiach, R.T. Shared trauma reality in war: Mental health therapists’ experience. PLoS ONE 2018, 13, e0191949. [Google Scholar]
- Cohen, E.; Roer-Strier, D.; Menachem, M.; Fingher-Amitai, S.; Israeli, N. “Common-Fate”: Therapists’ benefits and perils in conducting child therapy following the shared traumatic reality of war. Clin. Soc. Work J. 2014, 43, 77–88. [Google Scholar] [CrossRef]
- Finklestein, M.; Stein, E.; Greene, T.; Bronstein, I.; Solomon, Z. Posttraumatic stress disorder and vicarious trauma in mental health professionals. Health Soc. Work 2015, 40, e25–e31. [Google Scholar] [CrossRef]
- Dekel, R.; Hantman, S.; Ginzburg, K.; Solomon, Z. The cost of caring? Social workers in hospitals confront ongoing terrorism. Br. J. Soc. Work 2007, 37, 1247–1261. [Google Scholar] [CrossRef]
- Lev-Wiesel, R.; Goldblat, H.; Eisikovits, Z.; Admi, H. Growth in the shadow of war: The case of social workers and nurses working in a shared war reality. Br. J. Soc. Work 2009, 39, 1154–1174. [Google Scholar] [CrossRef]
- Pruginin, I.; Segal-Engelchin, D.; Isralowitz, R.; Reznik, A. Shared war reality effects on the professional quality of life of mental health professionals. Isr. J. Health Policy Res. 2016, 5, 17. [Google Scholar] [CrossRef][Green Version]
- Ben-Ezra, M.; Palgi, Y.; Wolf, J.J.; Shrira, A. Psychiatric symptoms and psychosocial functioning among hospital personnel during the Gaza War: A repeated cross-sectional study. Psychiatry Res. 2011, 189, 392–395. [Google Scholar] [CrossRef] [PubMed]
- Ben-Ezra, M.; Palgi, Y.; Wolf, J.J.; Shrira, A.; Hamama-Raz, Y. Somatization and psychiatric symptoms among hospital nurses exposed to war stressors. Isr J. Psychiatry Relat Sci. 2013, 50, 182–187. [Google Scholar] [PubMed]
- Abu-El-Noor, N.I.; Aljeesh, Y.I.; Radwan, A.S.; Abu-El-Noor, M.K.; Qddura, I.A.I.; Khadoura, K.J.; Alnawajha, S.K. Post-Traumatic Stress Disorder among health care providers following the Israeli attacks against Gaza Strip in 2014: A call for immediate policy actions. Arch. Psychiatr. Nurs. 2016, 30, 185–191. [Google Scholar] [CrossRef] [PubMed]
- Shamia, N.A.; Thabet, A.A.M.; Vostanis, P. Exposure to war traumatic experiences, Post-Traumatic Stress Disorder and post-traumatic growth among nurses in Gaza. J. Psychiatr. Ment. Health Nurs. 2015, 22, 749–755. [Google Scholar] [CrossRef] [PubMed]
- Shamai, M.; Ron, P. Helping direct and indirect victims of national terror: Experiences of Israeli social workers. Qual Health Res. 2009, 19, 42–54. [Google Scholar] [CrossRef] [PubMed]
- Somer, E.; Buchbinder, E.; Peled-Avram, M.; Ben-Yizhack, Y. The stress and coping of Israeli emergency room social workers following terrorist attacks. Qual. Health Res. 2004, 14, 1077–1093. [Google Scholar] [CrossRef] [PubMed]
- Dekel, R.; Nuttman-Shwartz, O.; Lavi, T. Shared traumatic reality and boundary theory: How mental health professionals cope with the home/work conflict during continuous security threats. J. Couple Relatsh. Ther. 2016, 15, 121–134. [Google Scholar] [CrossRef]
- Lavi, T.; Nuttman-Shwartz, O.; Dekel, R. Therapeutic intervention in a continuous shared traumatic reality: An example from the Israeli–Palestinian conflict. Br. J. Soc. Work 2015, 47, 919–935. [Google Scholar] [CrossRef]
- Tosone, C. Therapeutic intimacy: A post-9/11 perspective. Smith Coll. Stud. Soc. Work 2006, 76, 89–98. [Google Scholar] [CrossRef]
- Mitchell, J.T.; Everly, G.S., Jr. Critical incident stress management and critical incident stress debriefings: Evolutions, effects and outcomes. In Psychological Debriefing: Theory, Practice and Evidence; Raphael, B., Wilson, J.P., Eds.; Cambridge University Press: Cambridge, UK, 2000; pp. 71–90. [Google Scholar]
- Wilson, J.; Sigman, M. Theoretical perspectives of traumatic stress. In Psychological Debriefing: Theory, Practice and Evidence; Raphael, B., Wilson, J.P., Eds.; Cambridge University Press: Cambridge, UK, 2000; pp. 58–68. [Google Scholar]
- Kenardy, J.A.; Webster, R.A.; Lewin, T.J.; Carr, V.J.; Hazell, P.L.; Carter, G.L. Stress debriefing and patterns of recovery following a natural disaster. J. Trauma. Stress 1996, 9, 37–49. [Google Scholar] [CrossRef]
- Huss, E.; Hafford-Letchfield, T. Using art to illuminate social workers’ stress. J. Soc. Work 2019, 19, 751–768. [Google Scholar] [CrossRef]
- Huss, E.; Sarid, O.; Cwikel, J. Using art as a self-regulating tool in a war situation: A model for social workers. Health Soc. Work 2010, 35, 201–209. [Google Scholar] [CrossRef] [PubMed]
- Huss, E.; Sarid, O. Visually transforming artwork and guided imagery as a way to reduce work related stress: A quantitative pilot study. Arts Psychother. 2014, 41, 409–412. [Google Scholar] [CrossRef]
- Lazarus, R.S.; Folkman, S. Stress, Appraisal, and Coping; Springer: New York, NY, USA, 1984. [Google Scholar]
- Rosal, M. Cognitive Behavioral Art Therapy. In Approaches to Art Therapy: Theory and Technique; Rubin, J., Ed.; Brunner and Routledge: New York, NY, USA, 2001; pp. 210–225. [Google Scholar]
- Rubin, J. Introduction. In Approaches to Art Therapy: Theory and Technique; Brunner and Routledge: New York, NY, USA, 2016; pp. 1–15. [Google Scholar]
- Simon, M.; Graham, A. Self-Healing Through Visual and Verbal Art Therapy; Jessika Kingsley: Philadelphia, PA, USA, 2005. [Google Scholar]
- Wilkinson, R.A.; Chilton, G. Positive art therapy: Linking positive psychology to art therapy theory, practice, and research. J. Am. Art Ther. Assoc. 2013, 30, 4–11. [Google Scholar] [CrossRef]
- Sarid, O.; Huss, E. Image formation and image transformation. Arts Psychother. 2011, 38, 252–255. [Google Scholar] [CrossRef]
- Sarid, O.; Cwikel, J.; Czamanski-Cohen, J.; Huss, E. Treating women with perinatal mood and anxiety disorders (PMADs) with a hybrid cognitive behavioral and art therapy treatment (CB-ART). Arch. Women’s Ment. Health 2017, 20, 229–231. [Google Scholar] [CrossRef]
- Wolpe, J. The Practice of Behavior Therapy; Pergamon Press: New York, NY, USA, 1969. [Google Scholar]
- Segal-Engelchin, D.; Sarid, O. Brief intervention effectiveness on stress among Nepalese people indirectly exposed to the Nepal earthquake. Int. J. Ment. Health Addict. 2016, 14, 1–5. [Google Scholar] [CrossRef]
- Sarid, O.; Huss, E. Trauma and acute stress disorder: A comparison between cognitive behavioral intervention and art therapy. Arts Psychother. 2010, 37, 8–12. [Google Scholar] [CrossRef]
- Huss, E.; Samson, T. Drawing on the arts to enhance salutogenic coping with health-related stress and loss. Front. Psychol. 2018, 9, 1612. [Google Scholar] [CrossRef]
- Rollins, J.A. Tell me about it: Drawing as a communication tool for children with cancer. J. Pediatric Oncol. Nurs. 2005, 22, 203–221. [Google Scholar] [CrossRef]
- Edwards, M. Jungian Analytic Art Therapy. In Approaches to Art Therapy: Theory and Technique; Rubin, J., Ed.; Brunner and Routledge: New York, NY, USA, 2001; pp. 81–94. [Google Scholar]
- Goodnow, J. Children’s Drawings; Harvard University Press: Cambridge, MA, USA, 1997. [Google Scholar]
- Khellog, R. Analyzing Childrens Art; Mayfeilds Publishing Company: California, CA, USA, 1993. [Google Scholar]
- Wadeson, H. The anti-assessment devils advocate. J. Am. Art Ther. Assoc. 2002, 19, 37–41. [Google Scholar]
- Kaplan, F. Now and future ethno-cultural issues. J. Am. Art Ther. Soc. 2000, 19, 65–79. [Google Scholar]
- Ntoumanis, N.; Edmunds, J.; Duda, J.L. Understanding the coping process from a self-determination theory perspective. Br. J. Health Psychol. 2009, 14, 249–260. [Google Scholar] [CrossRef] [PubMed]
- Tedeschi, R.G.; Calhoun, L.G. Posttraumatic growth: Conceptual foundations and empirical evidence. Psychol. Inq. 2004, 15, 1–18. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristics | n | % or Mean (SD) |
|---|---|---|
| Age | 37.5 (12.5) | |
| 23–35 | 26 | 52.0 |
| 36–54 | 19 | 38.0 |
| 55 and above | 5 | 10.0 |
| Gender | ||
| Male | 7 | 14.0 |
| Female | 43 | 86.0 |
| Marital status | ||
| Single | 16 | 32.0 |
| Married | 23 | 46.0 |
| Cohabiting | 9 | 18.0 |
| Divorced/Separated | 2 | 4.0 |
| Has children | ||
| Yes | 26 | 52.0 |
| No | 24 | 48.0 |
| Country of birth | ||
| Israel | 41 | 82.0 |
| Other (US, Europe, FSU) | 9 | 18.0 |
| Religion | ||
| Jewish | 49 | 96.0 |
| Muslim | 2 | 4.0 |
| Degree of religiosity | ||
| Secular | 36 | 72.0 |
| Traditional or religious | 14 | 28.0 |
| Education | ||
| Academic-B.A. degree | 36 | 72.0 |
| Academic-M.A. degree | 14 | 28.0 |
| Perceived financial situation | ||
| Bad | 4 | 8.0 |
| Fair | 26 | 52.0 |
| Good or very good | 20 | 40.0 |
| SUDS Score Mean (SD) | Paired Sample t-Test | |
|---|---|---|
| SUDS score at t1 | 5.97 (2.22) | |
| SUDS score at t2 | 4.46 (1.98) | |
| Mean difference | 1.51 (1.39) | 7.41 ** |
| Drawings | |||
|---|---|---|---|
| Stress Drawing (%) | Resources Drawing (%) | Integrated Drawing (%) | |
| Background | |||
| No background | 49.0 | 37.3 | 29.4 |
| Had background | 51.0 | 62.7 | 76.6 |
| Number of objects | |||
| One | 25.5 | 7.8 | 9.8 |
| Several | 74.5 | 92.2 | 90.2 |
| Object placement | |||
| Center of the drawing | 37.3 | 19.6 | 13.7 |
| All over the drawing | 62.7 | 80.4 | 86.3 |
| Object size | |||
| Large-medium | 54.9 | 54.9 | 45.1 |
| Small or mixed | 45.1 | 45.1 | 54.9 |
| Colors | |||
| Black | |||
| None or minor | 52.9 | 96.1 | 78.4 |
| Dominant or only | 47.1 | 3.9 | 21.6 |
| Green | |||
| None or minor | 92.2 | 68.6 | 66.7 |
| Dominant or only | 7.8 | 31.4 | 33.3 |
| Grey | |||
| None or minor | 88.2 | 98.0 | 94.1 |
| Dominant or only | 11.8 | 2.0 | 5.9 |
| SUDS-Difference Mean (SD) | Independent Sample t-Test | |
|---|---|---|
| Selected format for the integrative drawing | 1.828 * | |
| Stress drawing | −0.92 (0.86) | |
| Resources drawing or a new drawing | −1.73 (0.15) | |
| Shape transformation | 0.150 | |
| Addition of shapes | −1.50 (1.40) | |
| Change or omission of shapes | −1.60 (1.51) | |
| Color transformation | −0.78 | |
| Yes | −1.59 (1.36) | |
| No | −1.20 (1.54) | |
| Size transformation | −1.786 * | |
| Reduction of initial size | −1.87 (1.22) | |
| Maintenance of initial size | −1.13 (1.48) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Segal-Engelchin, D.; Achdut, N.; Huss, E.; Sarid, O. CB-Art Interventions Implemented with Mental Health Professionals Working in a Shared War Reality: Transforming Negative Images and Enhancing Coping Resources. Int. J. Environ. Res. Public Health 2020, 17, 2287. https://doi.org/10.3390/ijerph17072287
Segal-Engelchin D, Achdut N, Huss E, Sarid O. CB-Art Interventions Implemented with Mental Health Professionals Working in a Shared War Reality: Transforming Negative Images and Enhancing Coping Resources. International Journal of Environmental Research and Public Health. 2020; 17(7):2287. https://doi.org/10.3390/ijerph17072287
Chicago/Turabian StyleSegal-Engelchin, Dorit, Netta Achdut, Efrat Huss, and Orly Sarid. 2020. "CB-Art Interventions Implemented with Mental Health Professionals Working in a Shared War Reality: Transforming Negative Images and Enhancing Coping Resources" International Journal of Environmental Research and Public Health 17, no. 7: 2287. https://doi.org/10.3390/ijerph17072287
APA StyleSegal-Engelchin, D., Achdut, N., Huss, E., & Sarid, O. (2020). CB-Art Interventions Implemented with Mental Health Professionals Working in a Shared War Reality: Transforming Negative Images and Enhancing Coping Resources. International Journal of Environmental Research and Public Health, 17(7), 2287. https://doi.org/10.3390/ijerph17072287