The Effects of Short-Term and Long-term Hearing Changes on Music Exposure: A Systematic Review and Meta-Analysis


Abstract
1. Introduction
2. Materials and Methods
2.1. Strategy for Systematic Search
2.2. Selection Criteria
2.3. Selection Process for Studies and Data Extraction
2.4. Assessment of the Quality of the Studies
2.5. Statistical Analysis
3. Results
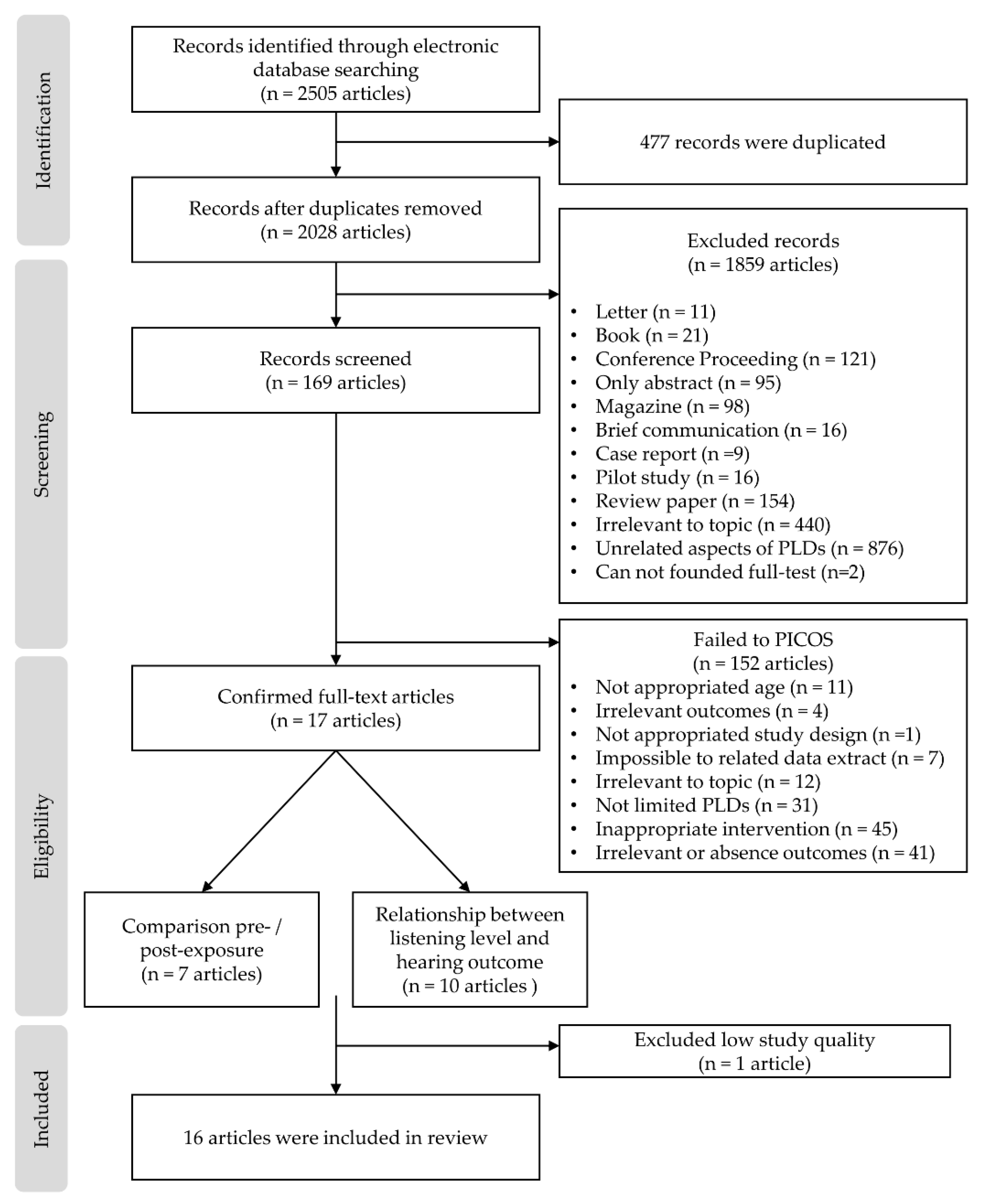
3.1. Selection Outcomes
3.2. Study Characteristics
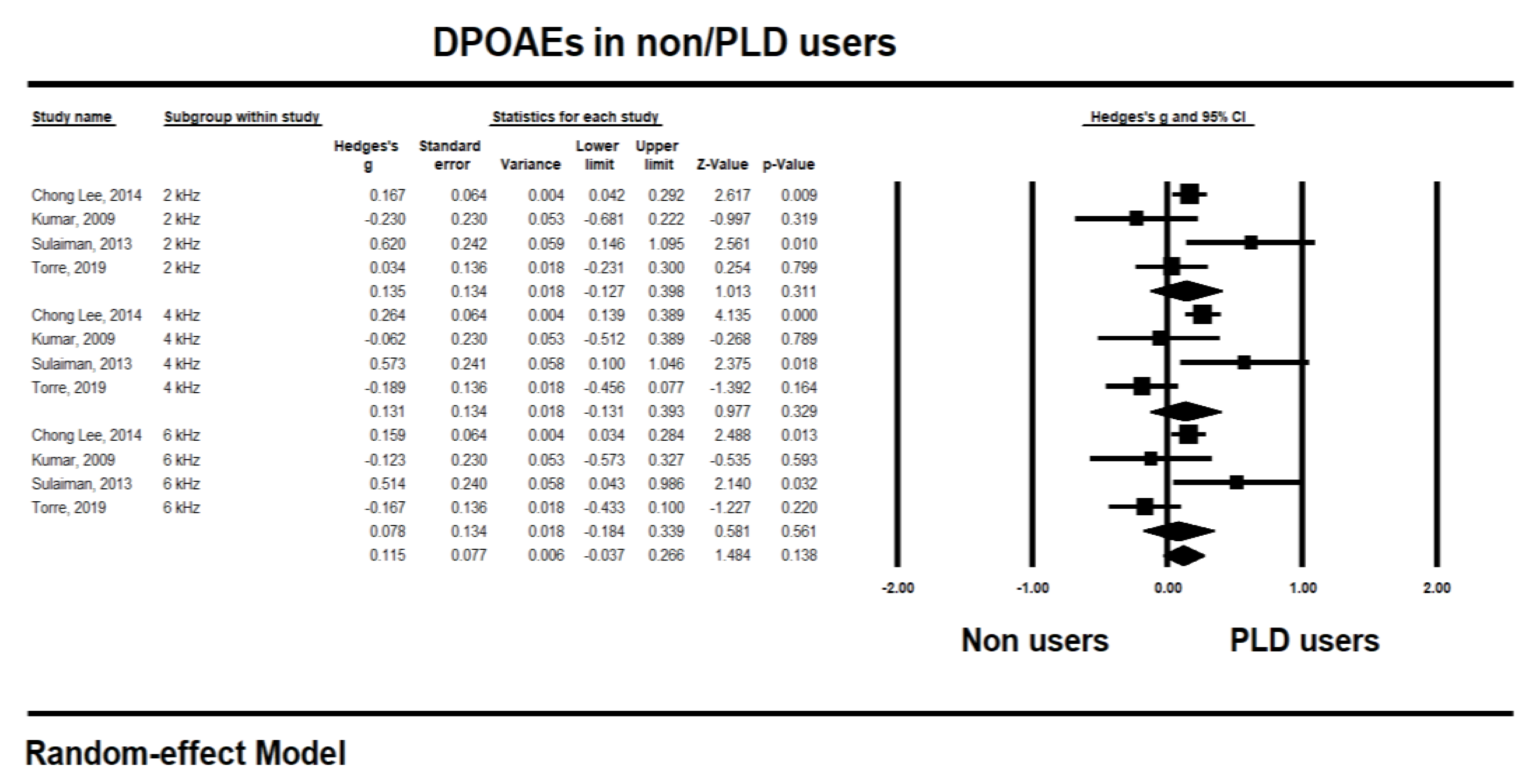
3.3. Meta-Analysis of Music Exposure Effects with Subgroup Analysis
4. Discussion
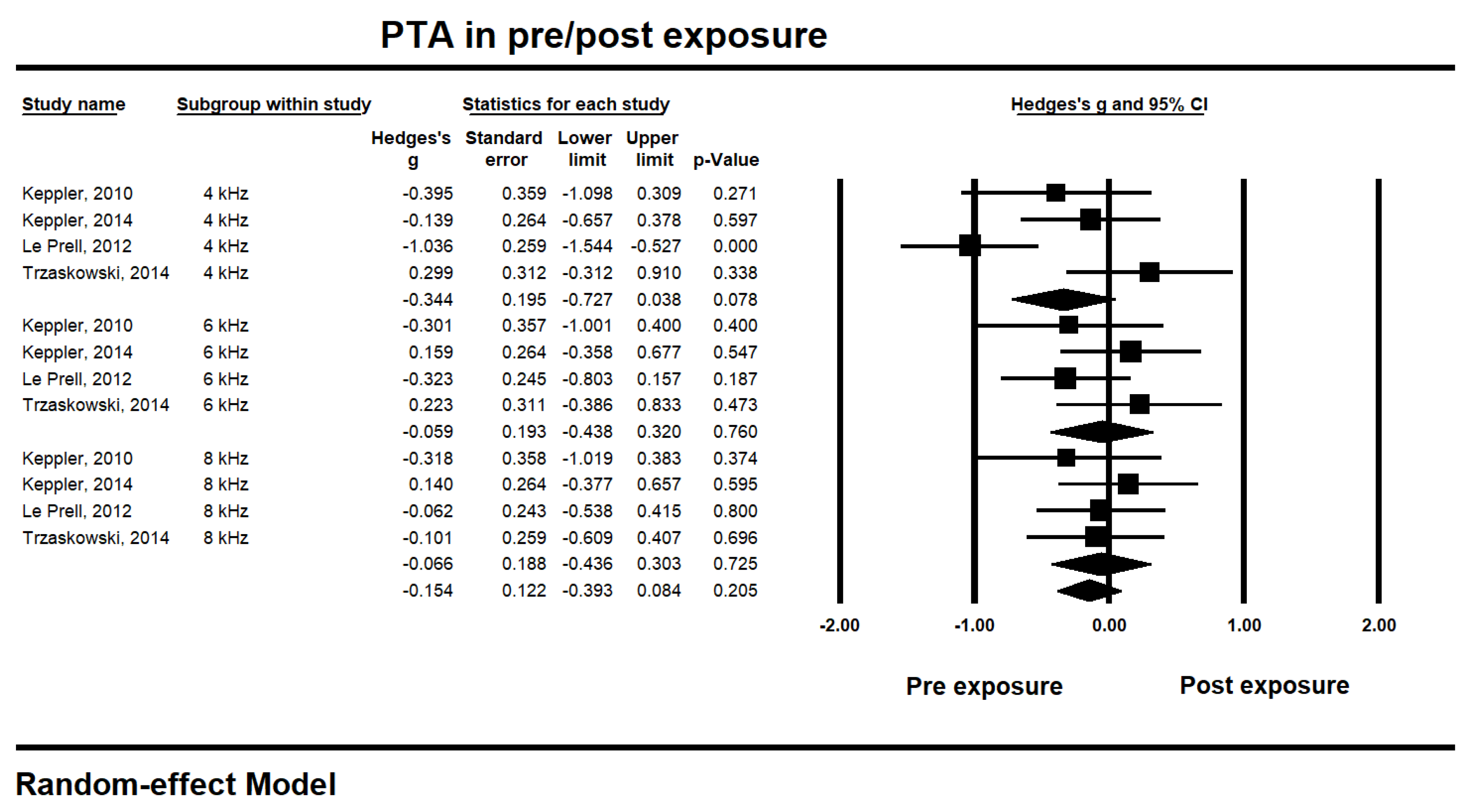
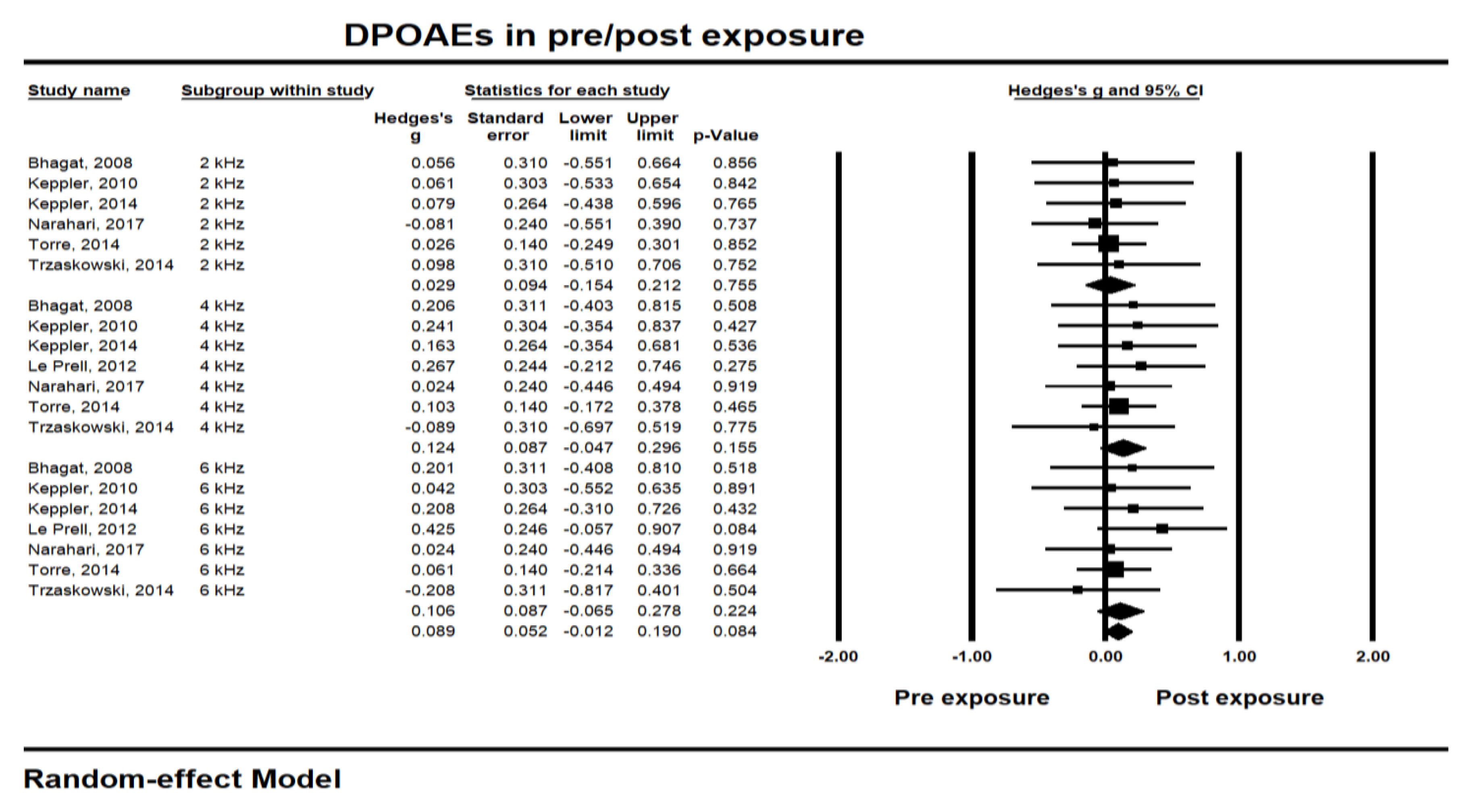
4.1. Short-term Hearing Changes Due to Music Exposure
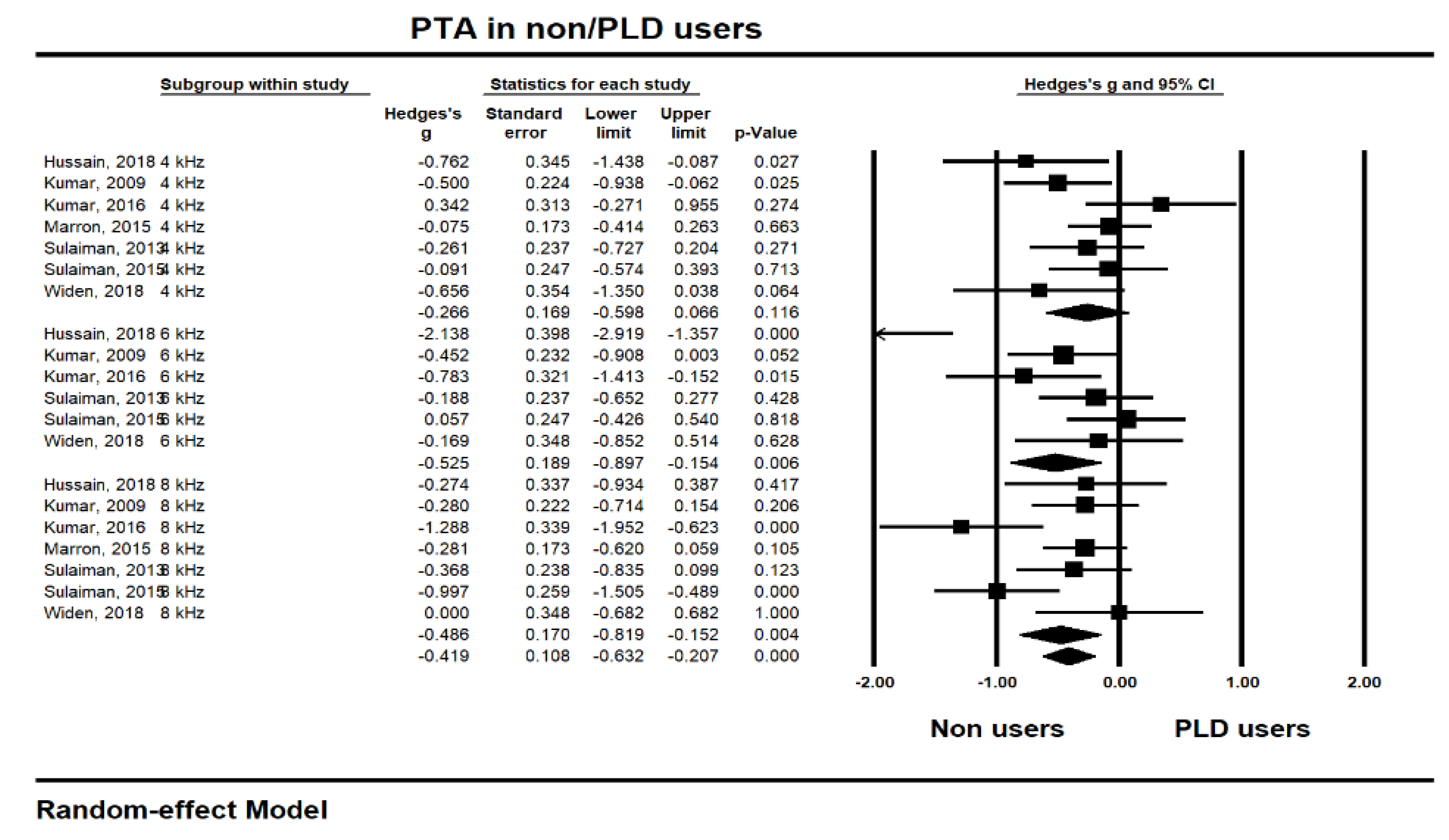
4.2. Long-term Hearing Changes Due to Music Exposure
4.3. Limitation of the Study
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Appendix A. Search Strategy in Keywords
References
- Scientific Committee on Emerging and Newly Identified Health Risks (2008) Potential Health Risks of Exposure to Noise From Personal Music Players and Mobile Phones Including A Music Playing Function -Preliminary Report. Available online: https://ec.europa.eu/health/ph_risk/committees/04_scenihr/docs/scenihr_o_017.pdf (accessed on 3 January 2020).
- Meyer-Bisch, C. Epidemiological evaluation of hearing damage related to strongly amplified music (personal cassette players, discotheques, rock concerts)-high-definition audiometric survey on 1364 subjects. Audiology 1996, 35, 121–142. [Google Scholar] [CrossRef]
- Serra, M.R.; Biassoni, E.C.; Richter, U.; Minoldo, G.; Franco, G.; Abraham, S.A.; Joeks, S.; Yacci, M.R. Recreational noise exposure and its effects on the hearing of adolescents. Part I: An interdisciplinary long-term study Exposición a ruido recreativo y sus efectos en la audición de los adolescentes. Parte I: un estudio interdisciplinario a largo plazo. Int. J. Audiol. 2005, 44, 65–73. [Google Scholar]
- Danhauer, J.L.; Johnson, C.E.; Byrd, A.; DeGood, L.; Meuel, C.; Pecile, A.; Koch, L.L. Survey of college students on iPod use and hearing health. J. Am. Adm. Audiol. 2009, 20, 5–27. [Google Scholar]
- Sulaiman, A.H.; Seluakumaran, K.; Husain, R. Hearing risk associated with the usage of personal listening devices among urban high school students in Malaysia. Public Health 2013, 127, 710–715. [Google Scholar]
- Punch, J.L.; Elfenbein, J.L.; James, R.R. Targeting hearing health messages for users of personal listening devices. Am. J. Audiol. 2011, 20, 69–82. [Google Scholar] [CrossRef]
- Ralli, M.; Greco, A.; de Vincentiis, M. Hearing Loss Following Unsafe Listening Practices in Children, Teenagers and Young Adults: An Underestimated Public Health Threat. Int. J. High Risk Behav. Addict. 2018, 7, 1–2. [Google Scholar] [CrossRef]
- Breinbauer, H.A.; Anabalón, J.L.; Gutierrez, D.; Cárcamo, R.; Olivares, C.; Caro, J. Output capabilities of personal music players and assessment of preferred listening levels of test subjects: Outlining recommendations for preventing music-induced hearing loss. The Laryngoscope 2012, 122, 2549–2556. [Google Scholar]
- Sulaiman, A.H.; Husain, R.; Seluakumaran, K. Evaluation of early hearing damage in personal listening device users using extended high-frequency audiometry and otoacoustic emissions. Eur. Arch. Oto-Rhino-L. 2013, 271, 1463–1470. [Google Scholar] [CrossRef]
- Serra, M.R.; Biassoni, E.C.; Hinalaf, M.; Abraham, M.; Pavlik, M.; Villalobo, J.P.; Curet, C.; Joeks, S.; Yacci, R.M.; Righetti, A. Hearing and loud music exposure in 14–15 years old adolescents. Noise Health 2014, 16, 320–330. [Google Scholar] [CrossRef]
- Jiang, W.; Zhao, F.; Guderley, N.; Manchaiah, V. Daily music exposure dose and hearing problems using personal listening devices in adolescents and young adults: A systematic review. Int. J. Audiol. 2016, 55, 197–205. [Google Scholar] [CrossRef]
- Le Clercq, C.M.; Van Ingen, G.; Ruytjens, L.; van der Schroeff, M.P. Music-induced hearing loss in children, adolescents, and young adults: a systematic review and meta-analysis. Otolog.Neurotol. 2016, 37, 1208–1216. [Google Scholar] [CrossRef] [PubMed]
- Zhao, F.; Manchaiah, V.K.; French, D.; Price, S.M. Music exposure and hearing disorders: An overview. Inte. J. Autol. 2010, 49, 54–64. [Google Scholar] [CrossRef] [PubMed]
- Figueiredo, R.R.; de Azevedo, A.A.; de Oliveira, P.M.; Amorim, S.P.V.; Rios, A.G.; Baptista, V. Incidence of tinnitus in mp3 player users. Braz. J. Otorhinolaryngol. 2011, 77, 293–298. [Google Scholar] [CrossRef]
- Kujawa, S.G.; Liberman, M.C. Acceleration of age-related hearing loss by early noise exposure: Evidence of a misspent youth. J. Neurosci. 2016, 26, 2115–2123. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Ann. Intern. Med. 2009, 151, 264–269. [Google Scholar] [CrossRef]
- Davies, S. The importance of PROSPERO to the National Institute for Health Research. Syst. Rev. 2012, 1. [Google Scholar] [CrossRef]
- Henshaw, H.; Ferguson, M.A. Efficacy of individual computer-based auditory training for people with hearing loss: A systematic review of the evidence. PloS one 2013, 8, e62836. [Google Scholar] [CrossRef]
- Stang, A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur. J. Epidemiol. 2010, 25, 603–605. [Google Scholar] [CrossRef]
- Le Prell, C.G.; Dell, S.; Hensley, B.; Hall, J.W., III; Campbell, K.C.; Antonelli, P.J.; Green, G.E.; Miller, M.J.; Guire, K. Digital music exposure reliably induces temporary threshold shift (TTS) in normal hearing human subjects. Ear and hearing 2012, 33, e44–e58. [Google Scholar] [CrossRef]
- Lee, G.J.C.; Lim, M.Y.; Kuan, A.Y.W.; Teo, J.H.W.; Tan, H.G.; Low, W.K. Relationship between leisure noise exposure and otoacoustic emissions in a young Asian population. Int. J.Audiol. 2014, 53, 462–468. [Google Scholar] [CrossRef]
- Torre, P.; Reed, M.B. Risk Factors for Distortion Product Otoacoustic Emissions in Young Adults. Appl. Sci. 2019, 9, 1608. [Google Scholar] [CrossRef]
- Bhagat, S.P.; Davis, A.M. Modification of otoacoustic emissions following ear-level exposure to MP3 player music. Int. J. Audiol. 2008, 47, 751–760. [Google Scholar] [CrossRef]
- Kumar, A.; Mathew, K.; Alexander, S.A.; Kiran, C. Output sound pressure levels of personal music systems and their effect on hearing. Noise Health 2009, 11, 132–140. [Google Scholar] [CrossRef] [PubMed]
- Keppler, H.; Dhooge, I.; Maes, L.; D’haenens, W.; Bockstael, A.; Philips, B.; Swinnen, F.; Vinck, B. Short-term auditory effects of listening to an MP3 player. Arch. Otolaryngol. Head Neck Surg. 2010, 136, 538–548. [Google Scholar] [CrossRef] [PubMed]
- Sulaiman, A.H.; Husain, H.; Seluakumaran, K. Hearing Risk among Young Personal Listening Device Users: Effects at High-Frequency and Extended High-Frequency Audiogram Thresholds. J. Int. Adv. Otol. 2015, 11, 104–109. [Google Scholar] [CrossRef]
- Keppler, H.; Dhooge, I.; Maes, L.; Bockstael, A.; Philips, B.; Swinnen, F.; Vinck, B. Evaluation of the olivocochlear efferent reflex strength in the susceptibility to temporary hearing deterioration after music exposure in young adults. Noise health 2014, 16, 108–115. [Google Scholar]
- Torre, P.; Grace, J. Changes in distortion product otoacoustic emission components after music exposure. J. Am. Acad. Audiol. 2014, 25, 804–813. [Google Scholar] [CrossRef]
- Trzaskowski, B.; Jędrzejczak, W.W.; Piłka, E.; Cieślicka, M.; Skarżyński, H. Otoacoustic Emissions before and after Listening to Music on a Personal Player. Med. Sci. Monit. 2014, 20, 1426–1431. [Google Scholar]
- Hutchinson Marron, K.; Marchiondo, K.; Stephenson, S.; Wagner, S.; Cramer, I.; Wharton, T.; Hughes, M.; Sproat, B.; Alessio, H. College students’ personal listening device usage and knowledge. Int. J. Audiol. 2015, 54, 384–390. [Google Scholar] [CrossRef]
- Kumar, U.A.; Deepashree, S.R. Personal music systems and hearing. J. Laryngol Otol. 2016, 130, 717–729. [Google Scholar] [CrossRef]
- Narahari, P.G.; Bhat, J.; Nambi, A.; Arora, A. Impact of usage of personal music systems on oto-acoustic emissions among medical students. Noise Health 2017, 19, 222–226. [Google Scholar] [CrossRef] [PubMed]
- Hussain, T.; Chou, C.; Zettner, E.; Torre, P.; Hans, S.; Gauer, J.; Markgraf, M.; Nquyen, Q.T. Early Indication of Noise-Induced Hearing Loss in Young Adult Users of Personal Listening Devices. Ann.Rhino. Laryngol. 2018, 127, 703–709. [Google Scholar] [CrossRef] [PubMed]
- Widén, S.E.; Möller, C.; Kähäri, K. Headphone listening habits, hearing thresholds and listening levels in Swedish adolescents with severe to profound HL and adolescents with normal hearing. Int. J. Audiol. 2018, 57, 730–736. [Google Scholar] [CrossRef] [PubMed]
- McNeill, K.; Keith, S.E.; Feder, K.; Konkle, A.T.; Michaud, D.S. MP3 player listening habits of 17 to 23 year old university students. J. Acoust. Soc. Am. 2010, 128, 646–653. [Google Scholar] [CrossRef]
- World Health Organization. Environmental Noise Guidelines for the European Region. 2018. Available online: https://apps.who.int/iris/bitstream/handle/10665/279952/9789289053563eng.pdf?sequence=1&isAllowed=y (accessed on 10 February 2020).







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| PICOS | Content Category |
|---|---|
| Participants | Young adults using PLDs |
| Intervention | Device exposure intensity and/or time |
| Control | Comparison to a control group or repeated measures (pre- and post-PLDs exposure comparison). |
| Outcomes | 1+ audiometry outcomes (PTA, OAEs, and EHF) and/or hearing symptoms |
| Study Designs | Cohort studies, cross-sectional studies, and repeated measures |
| Authors | Quality Assessment per the Newcastle–Ottawa Scale | |||
|---|---|---|---|---|
| Selection | Comparability | Outcome | Total | |
| Bhagat, 2008 [23] | 2 | 1 | 3 | Fair (6) |
| Kumar, 2009 [24] | 3 | 1 | 2 | Fair (6) |
| Keppler, 2010 [22] | 3 | 1 | 2 | Fair (6) |
| McNeill, 2010 [23] | 1 | 1 | 1 | Poor (3) |
| Le Prell, 2012 [20] | 3 | 1 | 3 | Good (7) |
| Lee, 2014 [21] | 4 | 2 | 2 | Good (8) |
| Sulaiman, 2013 [9] | 4 | 1 | 2 | Good (7) |
| Sulaiman, 2015 [26] | 3 | 1 | 2 | Fair (6) |
| Keppler, 2014 [27] | 3 | 1 | 2 | Fair (6) |
| Torre, 2014 [28] | 3 | 1 | 2 | Fair (6) |
| Trzaskowski, 2014 [29] | 2 | 1 | 3 | Fair (6) |
| Marron, 2015 [30] | 3 | 1 | 2 | Fair (6) |
| Kumar, 2016 [31] | 3 | 1 | 2 | Fair (6) |
| Narahari, 2017 [32] | 3 | 1 | 2 | Fair (6) |
| Hussain, 2018 [33] | 3 | 1 | 2 | Fair (6) |
| Widén, 2018 [34] | 3 | 1 | 1 | Fair (5) |
| Torre, 2019 [22] | 3 | 2 | 2 | Good (7) |
| Authors (Publication Date) | Subjects (Ages) | Method | Main Outcomes | ||
|---|---|---|---|---|---|
| Study Design | ExposureIntensity | Exposure Time (min) | |||
| Bhagat and Davis (2008) [23] | 20 young adults (18–38 y) | Hearing statuses were measured pre, post (30 min), and recovery (48 h) from time of music exposure PTA OAEs (DPOAEs, SOAEs) | 85 dBC ± 3 dB | 30 | Although the hearing thresholds did not change, the changes in DPOAEs and SSOAEs were early warning signs of the harmful effects of high levels of music exposure on cochlear functioning. |
| Keppler and Bockstael (2010) [25] | Noise exposure group 15 young adults (19–28 y), Control group 28 young adults (19–28 y) | Audiometric results of both groups were compared PTA OAEs (DPOAEs, TEOAEs) | LAeq,1h 92.41 dBA LAeq,8h 83.38 dBA | 60 | In the noise exposure group, the PTA and TEOAE amplitudes changed significantly between pre- and post-exposure. However, these patterns were not found for the DPOAE amplitudes. |
| Le Prell et al. (2012) [20] | 33 young adults (18–27 y) | Hearing status was measured pre, post (15min, 75min, 135min, 195min), and recovery (following 1 day and 1 week) after music exposure PTA OAEs (DPOAEs) | 94.5 dBA (n = 10) 99.6 dBA (n = 11) 100.3 dBA (n =12) | 240 | Changes in hearing thresholds showed a notched configuration, largest at 4 kHz. After music exposure, small, but reliable, temporary threshold shifts were found, but these threshold shifts quickly recovered during the first 3 h after music exposure. |
| Keppler et al., (2014) [27] | 28 young adults (19–30 y) | Hearing status was measured pre- and post- (immediately, 30 min) exposure PTA OAEs (DPOAEs, TEOAEs) | Based on LAeq,1h 82.52 dBA (n = 2) 87.46 dBA (n = 2) 92.25 dBA (n =12) 98.70 dBA (n = 12) | 60 | The authors reported that no clear relationship exists between temporary hearing deterioration and the amount of efferent suppression. |
| Torre and Grace (2014) [28] | Noise exposure group 101 young adults (18–30 y), Control group 21 young adults | Audiometric results for both groups were compared for pre- and post- (immediate) exposure DPOAE absolute levels and generator and characteristic frequency component levels were noted | 50.8 dBA (n = 7) 56.6 dBA (n = 56) 58.8 dBA (n = 14) 62.3 dBA (n = 24) | 60 | Based on the lower listening levels, DPOAEs showed very little or indeed no significant change after music exposure. |
| Trzaskowski et al. (2014) [29] | 20 young adults (22–27 y) | Audiological tests were conducted pre-, post (immediately), and recovery (24 h) after music exposure PTA OAEs (DPOAEs, TEOAEs) | 86.6 dBA | 30 | No statistically significant changes were found in OAE and PTA following 30min of music exposure. |
| Narahari et al. (2017) [32] | 34 young adults (17–21 y) | DPOAEs at pre- and post- (2 h) music exposure were analyzed | 98.29 dBSPL | 120 | The DPOAEs were affected immediately post music exposure, especially at 8 kHz or higher. |
| Authors (Publication Date) | Subjects (Ages) | Method | Main Results | |||
|---|---|---|---|---|---|---|
| Study Design | Exposure Intensity | UseTime | UsePeriod (yr) | |||
| Kumar el al. (2009) [24] | PLD user group 70 young adults (17–24 y) Non-PLD group (control) 30 young adults | After dividing into two groups based on the questionnaire, the audiological results of both groups were compared. PLL in quiet and noisy conditions PTA OAEs (DPOAEs) | 76 dBA LAeq,8h | 1.5 h/day | >2 yr | No significant differences were found at PTA and DPOAE for either group. In terms of a correlation analysis, a positive correlation exists between PTA and PLLs, and a negative correlation exists between DPOAEs and PLLs. |
| Sulaiman et al. (2013) [9] | PLD user group 35 young adults (18–30 y) Non-PLD group (control) 35 young adults | After dividing into two groups based on the interviews, hearing status was compared. Interviews (hearing symptoms) PLLs in blinded volume setting PTA, EHFs OAEs (DPOAEs, TEOAEs) | 81.3 dBA (76.2 dBA LAeq,8h) | 2.7 h/day | 3.2 yr | In EHFs, the mean hearing thresholds of PLD users were significantly higher, while conventional PTA users did not have typical characteristics of NIHL. OAE (DPOAE, TEOAE) amplitudes in PLD users were reduced compared to those in the non-PLD group. |
| Lee et al. (2014) [21] | High-risk group DPOAEs (n = 279) TEOAEs (n = 325) Others group (ear) D POAEs (n = 2097) TEOAEs (n = 2462) | A listening habit survey was conducted, and the subjects were assigned to each group. Based on the group, the OAE results were compared between the two groups. Listening habit survey PLLs OAEs (DPOAEs, TEOAEs) | 95.5 dBA | 2.9 h/day | 5.5 yr | • OAE (DPOAE, TEOAE) levels in high-risk group were significantly depressed. Specifically, TEOAE levels were lower at 4 kHz, and DPOAE levels decreased at 1, 2, 3, and 4 kHz. |
| Marron et al. (2015) [30] | 180 young adults (17–25 y) | Based on three questionnaires, PLL and PTA results of the subjects were analyzed. 3 questionnaires PTA PLLs | 73 dBA | 9.51 h/week | 10–12 yr | Listeners who use their PLDs for more than 7.5 h a week exhibited a statistically significantly worse hearing threshold. |
| Sulaiman e al. (2015) [26] | PLD user group 228 young adults (18–30 y) Non-PLD group (the control) 54 young adults | Audiological results were compared by group, PLL, and hearing symptoms. Interview (habits, symptoms) PTA, EHFs PLLs | 70.1 dBA (62.4 dBA LAeq,8h) | 2.2 h/day | 3.15 yr | In the PLD user group, 20.1% had >75 dBA (LAeq,8h), while 4.4% had >85 dBA, which can cause hearing damage. The subjects who listened to their devices at more than 75 dBA showed a significantly higher hearing threshold and incidence of hearing symptoms. |
| Kumar and Deepashree (2016) [31] | PLD user group 30 young adults (15–30 y) Non-PLD group 30 young adults | When comparing the two groups, the effects of PLD use on hearing were evaluated. Questionnaire for group assignment PLLs PTA, EHFs OAEs (TEOAEs) | 87.97 dBA LAeq | 2 h/day | > 2 yr | Subjects who listened to PLDs at higher than 80 dBA (LAeq) showed poorer EHF thresholds and decreased TEOAE amplitude. |
| Hussain et al. (2018) [33] | 50 young adults (19–39 y) High-risk group (subgroup) 11 young adults who listened to their devices at over 91 dBA | Based on the questionnaire, hearing status and listening preferences were compared. Questionnaire PLLs in quiet and noisy condition PTA | 85.5 dBA (All subjects), 96.2 dBA (High-risk subgroup) | 2 h/day | 6.1 yr | PLL and hearing thresholds were significantly correlated. In addition, the high-risk subgroup of subjects revealed poorer hearing thresholds at 4khz and 6 kHz. |
| Widén et al. (2018) [34] | 279 young adults (17 y) | Based on the questionnaire, output levels and hearing statuses were compared.QuestionnairePLLsPTA | 83 dBA LAeq | 1.99 h/day | 3.7 yr | • Subjects who listened at more than 85 dBA showed higher hearing thresholds. |
| Torre and Reed (2019) [22] | 216 young adults (college-aged, mean age, 20.95) | As measured for questionnaire-related PLDs and objective and subjective outcomes, the effects of DPOAEs were analyzed. Questionnaire (listening habits) OAEs (DPOAEs) | 73.0 dBA LAeq | 1 h/day | - | • In a subjective volume setting, 35% of subjects reported loud or very loud, but the measured PLLs were not considered hazardous. •There was no association between PLLs and DPOAEs, regardless of gender. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
You, S.; Kong, T.H.; Han, W. The Effects of Short-Term and Long-term Hearing Changes on Music Exposure: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2020, 17, 2091. https://doi.org/10.3390/ijerph17062091
You S, Kong TH, Han W. The Effects of Short-Term and Long-term Hearing Changes on Music Exposure: A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health. 2020; 17(6):2091. https://doi.org/10.3390/ijerph17062091
Chicago/Turabian StyleYou, Sunghwa, Tae Hoon Kong, and Woojae Han. 2020. "The Effects of Short-Term and Long-term Hearing Changes on Music Exposure: A Systematic Review and Meta-Analysis" International Journal of Environmental Research and Public Health 17, no. 6: 2091. https://doi.org/10.3390/ijerph17062091
APA StyleYou, S., Kong, T. H., & Han, W. (2020). The Effects of Short-Term and Long-term Hearing Changes on Music Exposure: A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health, 17(6), 2091. https://doi.org/10.3390/ijerph17062091