Active Travel of Czech and Polish Adolescents in Relation to Their Well-Being: Support for Physical Activity and Health

 ,
,  , and
, and
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants and Settings
2.2. Measurements
2.2.1. Subjective Estimation of Weekly PA
2.2.2. Subjective Estimation of Sedentary Behaviours (Passive Commuting and Sitting)
2.2.3. Self-Reported Well-Being
2.3. Data Analysis
2.4. Ethical Statement
3. Results
3.1. The Associations Between Active Travel and Well-Being
3.2. The Association Between Active Travel Recommendation and Well-Being
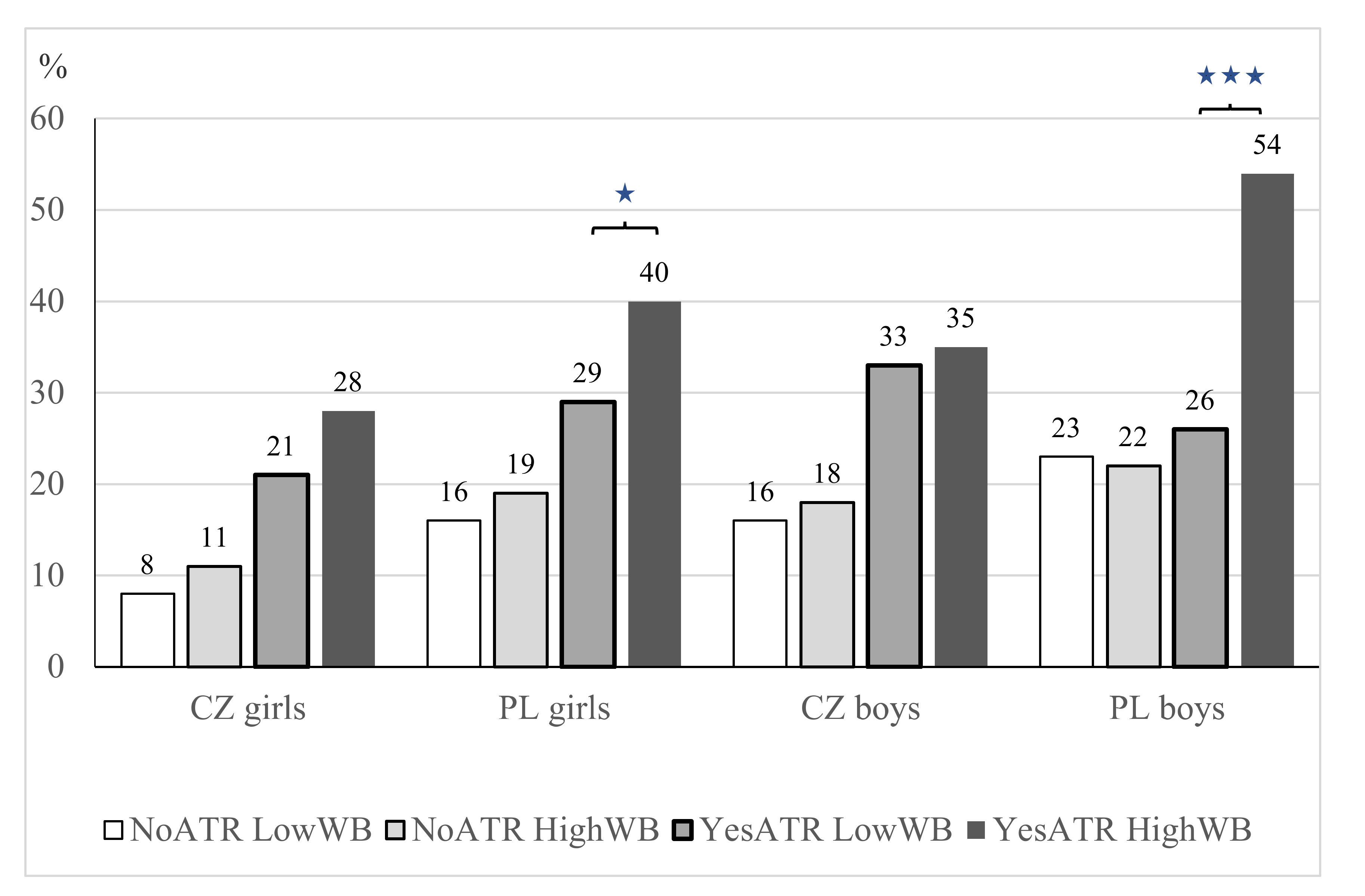
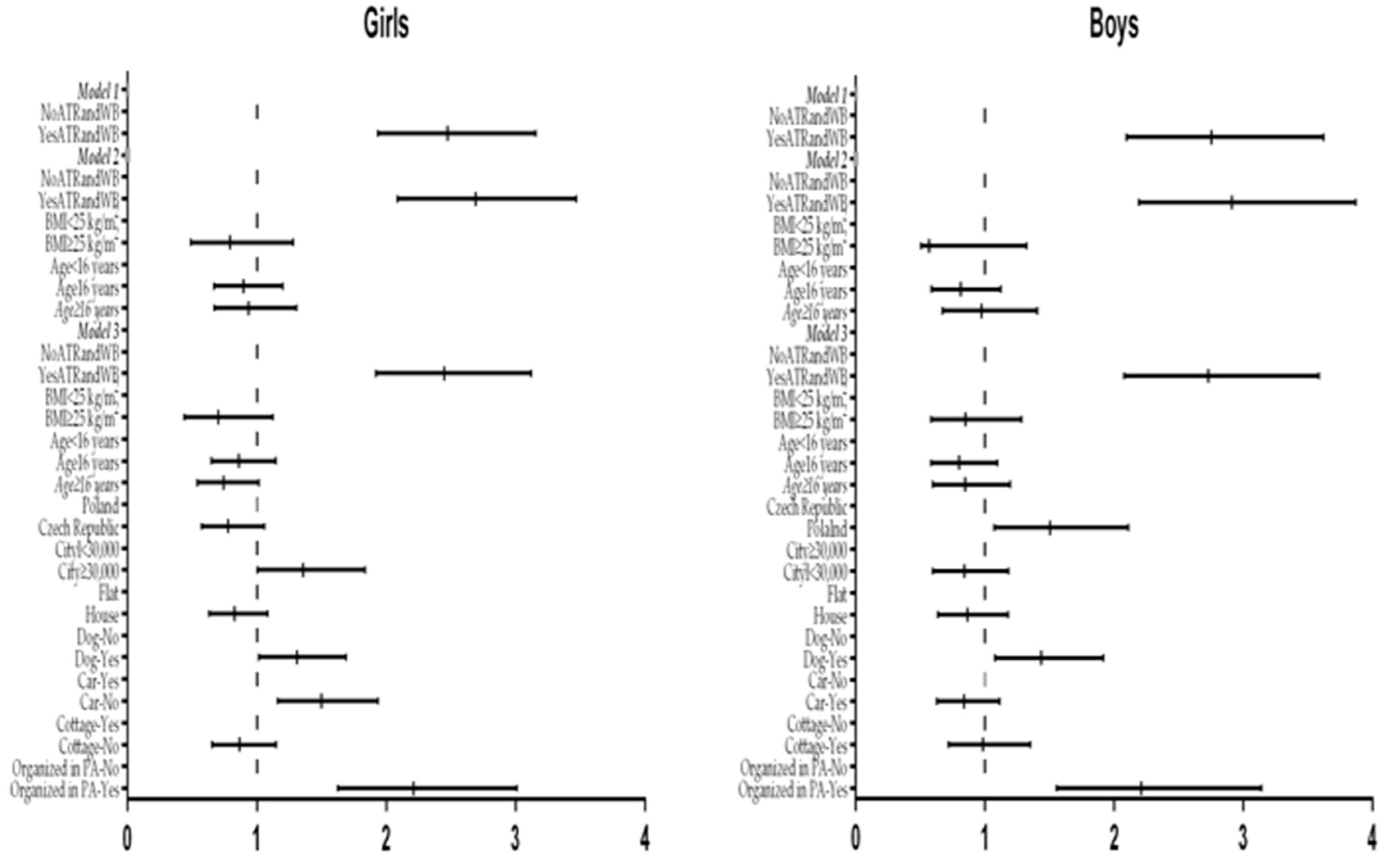
3.3. Odds of Meeting the Weekly PA Recommendations According to Meeting the Active Travel Recommendations and Level of Well-Being
3.4. The Associations Between Sedentary Behaviour (Commuting and Sitting) and Well-Being
4. Discussion
4.1. The Active Travel Recommendation and Well-Being in the Structure of the Weekly PA
4.2. The Association Between Active Travel and Well-Being
4.3. The Associations Between Sedentary Behaviour and Well-Being
4.4. Active Travel in the Context of the Policy
4.5. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Booth, V.M.; Rowlands, A.V.; Dollman, J. Physical activity temporal trends among children and adolescents. J. Sci. Med. Sport 2015, 18, 418–425. [Google Scholar] [CrossRef] [PubMed]
- Dygrýn, J.; Mitáš, J.; Gába, A.; Rubín, L.; Frömel, K. Changes in active commuting to school in Czech adolescents in different types of built environment across a 10-year period. Int. J. Environ. Res. Public Health 2015, 12, 12988–12998. [Google Scholar] [CrossRef] [PubMed]
- Katzmarzyk, P.T.; Denstel, K.N.; Beals, K.; Bolling, C.; Wright, C.; Crouter, S.E.; McKenzie, T.L.; Pate, R.R.; Saelens, B.E.; Staiano, A.E.; et al. Results from the United States of America’s 2016 Report card on physical activity for children and youth. J. Phys. Act. Health 2016, 13, S307–S313. [Google Scholar] [CrossRef] [PubMed]
- Rothman, L.; Macpherson, A.K.; Ross, T.; Buliung, R.N. The decline in active school transportation (AST): A systematic review of the factors related to AST and changes in school transport over time in North America. Prev. Med. 2018, 111, 314–322. [Google Scholar] [CrossRef] [PubMed]
- Ton, D.; Duives, D.C.; Cats, O.; Hoogendoorn-Lanser, S.; Hoogendoorn, S.P. Cycling or walking? Determinants of mode choice in the Netherlands. Transp. Res. Part A Policy Pract. 2019, 123, 7–23. [Google Scholar] [CrossRef]
- Burns, R.D.; Pfledderer, C.D.; Brusseau, T.A. Active transport, not device use, associates with self-reported school week physical activity in adolescents. Behav. Sci. 2019, 9, 32. [Google Scholar] [CrossRef]
- Mandic, S.; Hopkins, D.; Bengoechea, E.G.; Flaherty, C.; Williams, J.; Sloane, L.; Moore, A.; Spence, J.C. Adolescents’ perceptions of cycling versus walking to school: Understanding the New Zealand context. J. Transp. Health 2017, 4, 294–304. [Google Scholar] [CrossRef]
- Pérez, K.; Olabarria, M.; Rojas-Rueda, D.; Santamariňa-Rubio, E.; Borrell, C.; Nieuwenhuijsen, M. The health and economic benefits of active transport policies in Barcelona. J. Transp. Health 2017, 4, 316–324. [Google Scholar] [CrossRef]
- Larouche, R.; Faulkner, G.E.J.; Fortier, M.; Tremblay, M.S. Active transportation and adolescents’ health: The Canadian Health Measures Survey. Am. J. Prev. Med. 2014, 46, 507–515. [Google Scholar] [CrossRef]
- Mueller, N.; Rojas-Rueda, D.; Cole-Hunter, T.; de Nazelle, A.; Dons, E.; Gerike, R.; Götschi, T.; Panis, L.I.; Kahlmeier, S.; Nieuwenhuijsen, M. Health impact assessment of active transportation: A systematic review. Prev. Med. 2015, 76, 103–114. [Google Scholar] [CrossRef]
- Rojas-Rueda, D.; de Nazelle, A.; Andersen, Z.J.; Braun-Fahrländer, C.; Bruha, J.; Bruhova-Foltynova, H.; Desqueyroux, H.; Praznoczy, C.; Ragettli, M.S.; Tainio, M.; et al. Health impacts of active transportation in Europe. PLoS ONE 2016, 11, e0149990. [Google Scholar] [CrossRef] [PubMed]
- Fang, K.; Handy, S. Skateboarding for transportation: Exploring the factors behind an unconventional mode choice among university skateboard commuters. Transportation 2019, 46, 263–283. [Google Scholar] [CrossRef]
- Aubert, S.; Barnes, J.D.; Abdeta, C.; Nader, P.A.; Adeniyi, A.F.; Agular-Farias, N.; Tenesaca, D.S.A.; Bhawra, J.; Brazo-Sayavera, J.; Cardon, G.; et al. Global Matrix 3.0 Physical activity report card grades for children and youth: Results and analysis from 49 countries. J. Phys. Act. Health 2018, 15, S251–S273. [Google Scholar] [CrossRef] [PubMed]
- McGrath, L.J.; Hopkins, W.G.; Hinckson, E.A. Associations of objectively measured built-environment attributes with youth moderate–vigorous physical activity: A systematic review and meta-analysis. Sports Med. 2015, 45, 841–865. [Google Scholar] [CrossRef] [PubMed]
- Carver, A.; Timperio, A.F.; Hesketh, K.D.; Ridgers, N.D.; Salmon, J.L.; Crawford, D.A. How is active transport associated with children’s and adolescents’ physical activity over time? Int. J. Behav. Nutr. Phys. Act. 2011, 8, 126. [Google Scholar] [CrossRef] [PubMed]
- Dumith, S.C.; Gigante, D.P.; Domingues, M.R.; Kohl III, H.W. Physical activity change during adolescence: A systematic review and a pooled analysis. Int. J. Epidemiol. 2011, 40, 685–698. [Google Scholar] [CrossRef]
- Katzmarzyk, P.T.; Lee, I.-M.; Martin, C.K.; Blair, S.N. Epidemiology of physical activity and exercise training in the United States. Prog. Cardiovasc. Dis. 2017, 60, 3–10. [Google Scholar] [CrossRef]
- WHO. Regional Office for Europe. Physical Activity in Adolescents. 2016. Available online: http://www.euro.who.int/__data/assets/pdf_file/0018/303480/HBSC-No.7_factsheet_Physical.pdf?ua=1 (accessed on 22 March 2019).
- U.S. Department of Health and Human Services. Healthy People 2020. 2010. Available online: https://www.cdc.gov/nchs/healthy_people/hp2020.htm (accessed on 22 March 2019).
- Easton, S.; Ferrari, E. Children’s travel to school—The interaction of individual, neighbourhood and school factors. Transp. Policy 2015, 44, 9–18. [Google Scholar] [CrossRef]
- Garnham-Lee, K.P.; Falconer, C.L.; Sherar, L.B.; Taylor, I.M. Evidence of moderation effects in predicting active transport to school. J. Public Health 2016, 39, 153–162. [Google Scholar] [CrossRef]
- Rodríguez-López, C.; Salas-Fariňa, Z.M.; Villa-González, E.; Borges-Cosic, M.; Herrador-Colmenero, M.; Medina-Casaubón, J.; Ortega, F.B.; Chillón, P. The threshold distance associated with walking from home to school. Health Educ. Behav. 2017, 44, 857–866. [Google Scholar] [CrossRef]
- Chillón, P.; Panter, J.; Corder, K.; Jones, A.P.; Van Sluijs, E.M.F. A longitudinal study of the distance that young people walk to school. Health Place 2015, 31, 133–137. [Google Scholar] [CrossRef] [PubMed]
- Duncan, S.; White, K.; Mavoa, S.; Steward, T.; Hinckson, E.; Schofield, G. Active transport, physical activity, and distance between home and school in children and adolescents. J. Phys. Act. Health 2016, 13, 447–453. [Google Scholar] [CrossRef] [PubMed]
- Hubáčková, R.; Groffik, D.; Skrzypnik, L.; Frömel, K. Physical activity and inactivity in primary and secondary school boys’ and girls’ daily program. Acta Gymnica 2016, 46, 193–200. [Google Scholar] [CrossRef]
- Mitáš, J.; Sas-Nowosielski, K.; Groffik, D.; Frömel, K. The safety of the neighborhood environment and physical activity in Czech and Polish adolescents. Int. J. Environ. Res. Public Health 2018, 15, 126. [Google Scholar] [CrossRef] [PubMed]
- Gropp, K.; Janssen, I.; Pickett, W. Active transportation to school in Canadian youth: Should injury be a concern? Inj. Prev. 2013, 19, 64–67. [Google Scholar] [CrossRef]
- Denstel, K.D.; Broyles, S.T.; Larouche, R.; Sarmiento, O.L.; Barreira, T.V.; Chaput, J.-P.; Church, T.S.; Fogelholm, M.; Hu, G.; Kuriyan, R.; et al. Active school transport and weekday physical activity in 9–11-year-old children from 12 countries. Int. J. Obes. Suppl. 2015, 5, S100–S106. [Google Scholar] [CrossRef]
- Aparicio-Ugarriza, R.; Mielgo-Ayuso, J.; Ruiz, E.; Ávila, J.M.; Aranceta-Bartrina, J.; Gil, Á.; Ortega, R.M.; Serra-Majem, L.; Varela-Moreiras, G.; González-Gross, M. Active commuting, physical activity, and sedentary behaviors in children and adolescents from Spain: Findings from the ANIBES Study. Int. J. Environ. Res. Public Health 2020, 17, 668. [Google Scholar] [CrossRef]
- Sirard, J.R.; Slater, M.E. Walking and bicycling to school: A review. Am. J. Lifestyle Med. 2008, 2, 372. [Google Scholar] [CrossRef]
- Pucher, J.; Buehler, R. At the frontiers of cycling: Policy innovations in the Netherlands, Denmark, and Germany. World Transp. Pol. Pract. 2007, 13, 8–57. [Google Scholar]
- Molina-Garcia, J.; Garcia-Massó, X.; Estevan, I.; Queralt, A. Built environment, psychosocial factors and active commuting to school in adolescents: Clustering a self-organizing map analysis. Int. J. Environ. Res. Public Health 2019, 16, 83. [Google Scholar] [CrossRef]
- Lubans, D.R.; Plotnikoff, R.C.; Lubans, N.J. Review: A systematic review of the impact of physical activity programmes on social and emotional well-being in at-risk youth. Child Adolesc. Ment. Health 2012, 17, 2–13. [Google Scholar] [CrossRef]
- Doré, I.; Sylvester, B.; Sabiston, C.; Sylvestre, M.-P.; O’Loughlin, J.; Brunet, J.; Bélanger, M. Mechanisms underpinning the association between physical activity and mental health in adolescence: A 6-year study. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 9. [Google Scholar] [CrossRef] [PubMed]
- Sallis, J.F.; Owen, N.; Fisher, E.B. Ecological models of health behaviour. In Health Behavior and Health Education. Theory, Research and Practice, 4th ed.; Glanz, K., Rimer, B.K., Viswanath, K., Eds.; Jossey-Bass: San Francisco, CA, USA, 2008; Volume 20, pp. 465–485. [Google Scholar]
- Durayappah, A. The 3P model: A general theory of subjective well-being. J. Happiness Stud. 2011, 12, 681–716. [Google Scholar] [CrossRef]
- Craig, C.L.; Marshall, A.L.; Sjöström, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelung, U.; Yngve, A.; Sallis, J.F.; et al. International physical activity questionnaire: 12-country reliability and validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef] [PubMed]
- Bauman, A.; Ainsworth, B.E.; Sallis, J.F.; Hagströmer, M.; Craig, C.L.; Bull, F.C.; Pratt, M.; Venugopal, K.; Chau, J.; Sjöström, M.; et al. The descriptive epidemiology of sitting. A 20-country comparison using the International Physical Activity Questionnaire (IPAQ). Am. J. Prev. Med. 2011, 41, 228–235. [Google Scholar] [CrossRef]
- Hagströmer, M.; Bergman, P.; De Bourdeaudhuij, I.; Ortega, F.B.; Ruiz, J.R.; Manios, Y.; Rey-López, J.P.; Phillipp, K.; von Berlepsch, J.; Sjöström, M.; et al. Concurrent validity of a modified version of the International Physical Activity Questionnaire (IPAQ-A) in European adolescents: The HELENA Study. Int. J. Obes. 2008, 32, S42–S48. [Google Scholar] [CrossRef]
- Ottevaere, C.; Huybrechts, I.; De Bourdeaudhuij, I.; Sjöström, M.; Ruiz, J.R.; Ortega, F.B.; Hagströmer, M.; Widhalm, K.; Molnár, D.; Moreno, L.A.; et al. Comparison of the IPAQ-A and Actigraph in relation to VO2max among European adolescents: The HELENA study. J. Sci. Med. Sport 2011, 14, 317–324. [Google Scholar] [CrossRef]
- Cull, A.; Sprangers, M.; Bjordal, K.; Aaronson, N.; West, K.; Bottomley, A. EORTC Quality of Life Group Translation Procedure, 2nd ed.; EORTC Quality of Life Unit: Brussels, Belgium, 2002. [Google Scholar]
- Fromel, K.; Kudlacek, M.; Groffik, D.; Svozil, Z.; Simunek, A.; Garbaciak, W. Promoting healthy lifestyle and well-being in adolescents through outdoor physical activity. Int. J. Environ. Res. Public Health 2017, 14, 533. [Google Scholar] [CrossRef]
- Cerin, E.; Cain, K.L.; Oyeymi, A.L.; Owen, N.; Conway, T.L.; Cochrane, T.; Van Dyck, D.; Schipperijn, J.; Mitas, J.; Toftager, M.; et al. Correlates of agreement between accelerometry and self-reported physical activity. Med. Sci. Sports Exerc. 2016, 48, 1075–1084. [Google Scholar] [CrossRef]
- U.S. Department of Health and Human Services. Physical Activity Guidelines for Americans, 2nd ed.; U.S. Department of Health and Human Services: Washington, DC, USA, 2018.
- Kohl, H.W., 3rd; Craig, C.L.; Lambert, E.V.; Inoue, S.; Alkandari, J.R.; Leetongin, G.; Kahlmeier, S. The pandemic of physical inactivity: Global action for public health. Lancet 2012, 380, 294–305. [Google Scholar] [CrossRef]
- Slingerland, M.; Borghouts, L.B.; Hesselink, M.K.C. Physical activity energy expenditure in Dutch adolescents: Contribution of active transport to school, physical education, and leisure time activities. J. Sch. Health 2012, 82, 225–232. [Google Scholar] [CrossRef] [PubMed]
- Valois, R.F.; Zullig, K.J.; Huebner, E.S.; Drane, J.W. Physical activity behaviors and perceived life satisfaction among public high school adolescents. J. Sch. Health 2004, 74, 59–65. [Google Scholar] [CrossRef] [PubMed]
- González-Carrasco, M.; Casas, F.; Malo, S.; Viňas, F.; Dinisman, T. Changes with age in subjective well-being through the adolescent years: Differences by gender. J. Happiness Stud. 2017, 18, 63–88. [Google Scholar] [CrossRef]
- Eddolls, W.T.B.; McNarry, M.A.; Lester, L.; Winn, C.O.N.; Stratton, G.; Mackintosh, K.A. The association between physical activity, fitness and body mass index on mental well-being and quality of life in adolescents. Qual. Life Res. 2018, 27, 2313–2320. [Google Scholar] [CrossRef]
- Wiium, N.; Säfvenbom, R. Participation in organized sports and self-organized physical activity: Associations with developmental factors. Int. J. Environ. Res. Public Health 2019, 16, 585. [Google Scholar] [CrossRef]
- Greenleaf, C.; Boyer, E.M.; Petrie, T.A. High school sport participation and subsequent psychological well-being and physical activity: The mediating influences of body image, physical competence, and instrumentality. Sex Roles 2009, 61, 714–726. [Google Scholar] [CrossRef]
- Xu, H.; Wen, L.M.; Rissel, C. The relationships between active transport to work or school and cardiovascular health or body weight: A systematic review. Asia Pac. J. Public Health 2013, 25, 298–315. [Google Scholar] [CrossRef]
- Sun, Y.; Liu, Y.; Tao, F.-B. Associations between active commuting to school, body fat, and mental well-being: Population-based, cross-sectional study in China. J. Adolesc. Health 2015, 57, 679–685. [Google Scholar] [CrossRef]
- Ruiz-Ariza, A.; de la Torre-Cruz, M.J.; Redecillas-Peiró, M.T.; Martínez-López, E.J. Influence of active commuting on happiness, well-being, psychological distress and body shape in adolescents. Gac. Sanit. 2015, 29, 454–457. [Google Scholar] [CrossRef]
- Martínez-López, E.J.; Hita-Contreras, F.; Moral-García, J.E.; Grao-Cruces, A.; Ruiz, J.R.; Redecillas-Peiró, M.T.; Martínez-Amat, A. Association of low weekly physical activity and sedentary lifestyle with self-perceived health, pain, and well-being in a Spanish teenage population. Sci. Sports 2015, 30, 342–351. [Google Scholar] [CrossRef]
- Gill, D.L.; Chang, Y.-K.; Murphy, K.M.; Speed, K.M.; Hammond, C.C.; Rodriguez, E.A.; Lyu, M.; Shang, Y.-T. Quality of life assessment for physical activity and health promotion. Appl. Res. Qual. Life 2011, 6, 181–200. [Google Scholar] [CrossRef]
- Bowler, D.E.; Buyung-Ali, L.M.; Knight, T.M.; Pullin, A.S. A systematic review of evidence for the added benefits to health of exposure to natural environments. BMC Public Health 2010, 10, 456. [Google Scholar] [CrossRef] [PubMed]
- Coon, J.T.; Boddy, K.; Stein, K.; Whear, R.; Barton, J.; Depledge, M.H. Does participating in physical activity in outdoor natural environments have a greater effect on physical and mental wellbeing than physical activity indoors? A systematic review. Environ. Sci. Technol. 2011, 45, 1761–1772. [Google Scholar] [CrossRef] [PubMed]
- Larouche, R.; Mammen, G.; Rowe, D.A.; Faulkner, G. Effectiveness of active school transport interventions: A systematic review and update. BMC Public Health 2018, 18, 206. [Google Scholar] [CrossRef]
- Verhoeven, H.; Ghekiere, A.; Van Cauwenberg, J.; Van Dyck, D.; De Bourdeaudhuij, I.; Clarys, P.; Deforche, B. Which physical and social environmental factors are most important for adolescents’ cycling for transport? An experimental study using manipulated photographs. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 108. [Google Scholar] [CrossRef]
- Larsen, L.R.; Troelsen, J.; Kirkegaard, K.L.; Riiskjær, S.; Krølner, R.; Østergaard, L.; Kristensen, P.L.; Møller, N.C.; Christensen, B.F.N.; Jensen, J.-O.; et al. Results from Denmark’s 2016 report card on physical activity for children and youth. J. Phys. Act. Health 2016, 13, S137–S142. [Google Scholar] [CrossRef]
- Elinder, L.S.; Sundblom, E.; Rosendahl, K.I. Low physical activity is a predictor of thinness and low self-rated health: Gender differences in a Swedish cohort. J. Adolesc. Health 2011, 48, 481–486. [Google Scholar] [CrossRef]
- Breidablik, H.J.; Meland, E.; Lydersen, S. Self-rated health during adolescence: Stability and predictors of change (Young-HUNT study, Norway). Eur. J. Public Health 2009, 19, 73–78. [Google Scholar] [CrossRef]
- Villa-González, E.; Barranco-Ruiz, Y.; Evenson, K.R.; Chillón, P. Systematic review of interventions for promoting active school transport. Prev. Med. 2018, 111, 115–134. [Google Scholar] [CrossRef]
- Chen, S.; Gu, X. Toward active living: Comprehensive school physical activity program research and implications. Quest 2018, 70, 191–212. [Google Scholar] [CrossRef]
- Sallis, J.F.; Bull, F.; Guthold, R.; Heath, G.W.; Inoue, S.; Kelly, P.; Oyeyemi, A.L.; Perez, L.G.; Richards, J.; Hallal, P.C.; et al. Progress in physical activity over the Olympic quadrennium. Lancet 2016, 388, 1325–1336. [Google Scholar] [CrossRef]
- McDonald, N.C.; Steiner, R.L.; Palmer, W.M.; Bullock, A.N.; Sisiopiku, V.P.; Lytle, B.F. Costs of school transportation: Quantifying the fiscal impacts of encouraging walking and bicycling for school travel. Transportation 2016, 43, 159–175. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristics | n | Age (Years) | Weight (kg) | Height (cm) | BMI (kg·m-2) | ||||
|---|---|---|---|---|---|---|---|---|---|
| M | SD | M | SD | M | SD | M | SD | ||
| Girls CZ | 931 | 16.77 | 1.18 | 59.49 | 9.26 | 167.50 | 6.42 | 21.18 | 2.95 |
| Boys CZ | 531 | 16.74 | 1.22 | 70.35 | 11.85 | 179.06 | 7.86 | 21.92 | 3.37 |
| Girls PL | 764 | 16.26 | 0.77 | 56.95 | 8.79 | 166.10 | 6.07 | 20.62 | 2.85 |
| Boys PL | 579 | 16.21 | 0.74 | 67.02 | 13.37 | 176.63 | 7.74 | 21.41 | 3.65 |
| Physical Activity | Girls | Boys | H | p | η2 | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Low WB (n = 678) | High WB (n = 1017) | Low WB (n = 325) | High WB (n = 785) | ||||||||
| Mdn (IQR) | M (SD) | Mdn (IQR)) | M (SD) | Mdn (IQR) | M (SD) | Mdn (IQR)) | M (SD) | ||||
| Cycling transportation (MET-min/week) | 0 (0) | 181 (703) | 0 (60) | 272 (827) | 0 (120) | 308 (763) | 0 (360) | 462 (1104) | 66.34 b,c,d | ˂0.001 | 0.037* |
| Walking transportation (MET-min/week) | 57 8(1122) | 910 (989) | 578 (1139) | 981 (1074) | 462 (990) | 874 (1061) | 495 (990) | 906 (1058) | 10.07 | 0.018 | 0.004 |
| Total transportation (MET-min/week) | 693 (1116) | 1090 (1217) | 743 (1424) | 1253 (1333) | 675 (1544) | 1181 (1312) | 792 (1679) | 1368 (1587) | 7.90 | 0.048 | 0.003 |
| Total physical activity (MET-min/week) | 3485 (4274) | 4388 (3354) | 4102 (5103) | 5094 (3645) | 4212 (5362) | 5122 (3787) | 5014 (4051) | 5808 (4051) | 47.76 a,b,c,d | ˂0.001 | 0.037* |
| Country | Gender | Well-being | Passive Commuting and Sitting | χ 2 | p | w | |||
|---|---|---|---|---|---|---|---|---|---|
| Low | High | ||||||||
| n | % | n | % | ||||||
| Czech Republic | Girls: | Low | 117 | 24.4 | 48 | 48.5 | 23.41 | <0.001 | 0.201 * |
| High | 363 | 75.6 | 51 | 51.5 | |||||
| Boys | Low | 124 | 29.3 | 36 | 34.6 | 0.79 | 0.375 | 0.039 | |
| High | 300 | 71.7 | 71 | 66.4 | |||||
| Poland | Girls: | Low | 258 | 43.8 | 85 | 48.6 | 1.24 | 0.265 | 0.041 |
| High | 331 | 56.2 | 90 | 51.4 | |||||
| Boys | Low | 233 | 33.6 | 102 | 42.9 | 6.56 | 0.010 | 0.084 | |
| High | 460 | 66.4 | 136 | 57.1 | |||||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Frömel, K.; Groffik, D.; Mitáš, J.; Dygrýn, J.; Valach, P.; Šafář, M. Active Travel of Czech and Polish Adolescents in Relation to Their Well-Being: Support for Physical Activity and Health. Int. J. Environ. Res. Public Health 2020, 17, 2001. https://doi.org/10.3390/ijerph17062001
Frömel K, Groffik D, Mitáš J, Dygrýn J, Valach P, Šafář M. Active Travel of Czech and Polish Adolescents in Relation to Their Well-Being: Support for Physical Activity and Health. International Journal of Environmental Research and Public Health. 2020; 17(6):2001. https://doi.org/10.3390/ijerph17062001
Chicago/Turabian StyleFrömel, Karel, Dorota Groffik, Josef Mitáš, Jan Dygrýn, Petr Valach, and Michal Šafář. 2020. "Active Travel of Czech and Polish Adolescents in Relation to Their Well-Being: Support for Physical Activity and Health" International Journal of Environmental Research and Public Health 17, no. 6: 2001. https://doi.org/10.3390/ijerph17062001
APA StyleFrömel, K., Groffik, D., Mitáš, J., Dygrýn, J., Valach, P., & Šafář, M. (2020). Active Travel of Czech and Polish Adolescents in Relation to Their Well-Being: Support for Physical Activity and Health. International Journal of Environmental Research and Public Health, 17(6), 2001. https://doi.org/10.3390/ijerph17062001