Development and Validation of the Scale for Partnership in Care—for Family (SPIC-F)


Abstract
1. Introduction
2. Methods
2.1. Study Participants
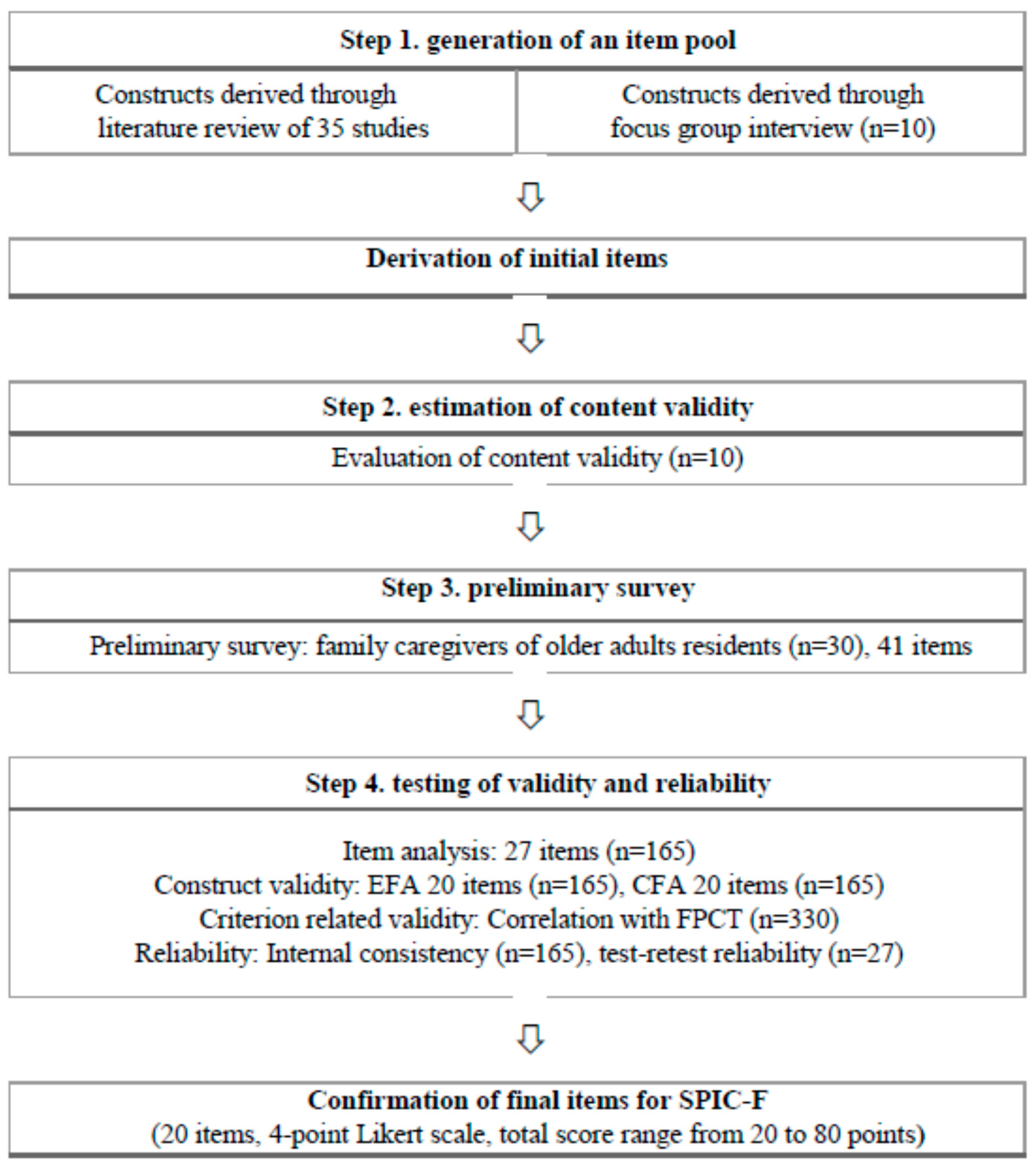
2.2. Development of Instrument
2.2.1. Item Generation
2.2.2. Content Validity
2.2.3. Preliminary Study
2.3. Data Collection and Ethical Considerations
2.4. Instrument
2.5. Statistical Analysis
3. Results
3.1. Validity and Reliability Testing
3.1.1. Participant Characteristics
3.1.2. Item Analysis
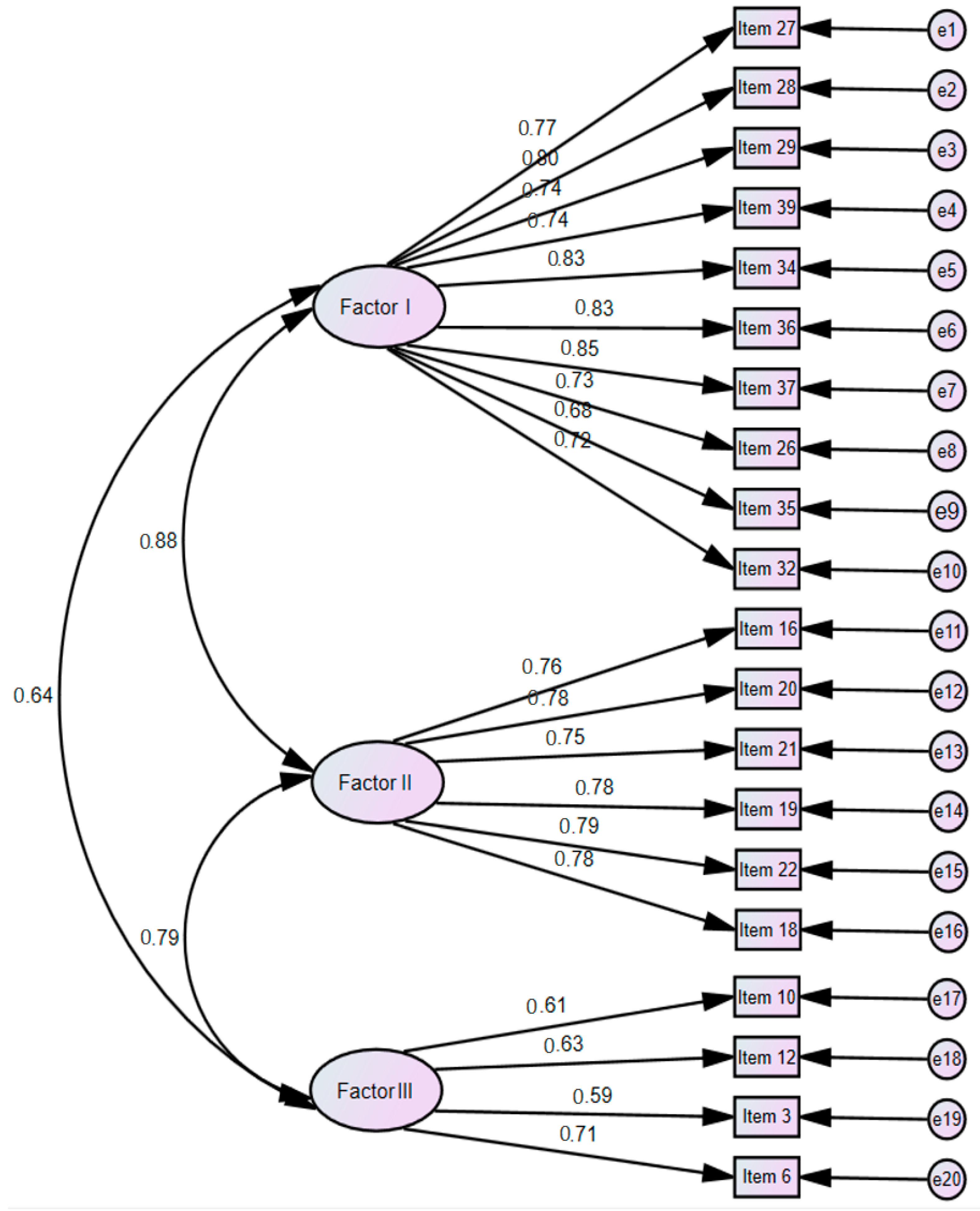
3.1.3. Construct Validity
EFA
CFA
3.1.4. Criterion Validity
3.1.5. Reliability
3.2. Finalization of Scale
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A. SPIC-F Scale

{kind=link}
{kind=link}
| Item | Strongly Disagree | Disagree | Agree | Strongly Agree |
|---|---|---|---|---|
| Professional caring and support | ||||
| 1. Staff encourage the family to visit the facility. | ① | ② | ③ | ④ |
| 2. Staff positively support family involvement in providing care (e.g., conversation, taking a walk, meal assistance, etc.). | ① | ② | ③ | ④ |
| 3. Staff welcome the family when they visit the facility. | ① | ② | ③ | ④ |
| 4. Staff inform the family about the regulations and the policies of the facility before he or she is admitted. | ① | ② | ③ | ④ |
| 5. Staff respect and support the families’ decision-making on the older adults residing in the facility. | ① | ② | ③ | ④ |
| 6. Staff provide appropriate care on the condition of the older adults residing in the facility. | ① | ② | ③ | ④ |
| 7. Staff provide care while maintaining the dignity of the older adults residing in the facility. | ① | ② | ③ | ④ |
| 8. Staff inform the family about the condition or changes in the condition of the older adults residing in the facility. | ① | ② | ③ | ④ |
| 9. Staff are sensitive to changes in the state of the older adults residing in the facility. | ① | ② | ③ | ④ |
| 10. Staff involve families when planning care for the older adults residing in the facility. | ① | ② | ③ | ④ |
| Cooperative relationship and information sharing | ||||
| 11. Staff and I communicate smoothly regarding caring for the older adult. | ① | ② | ③ | ④ |
| 12. Staff and I discuss the range of roles that each other should take in caring for the older adult. | ① | ② | ③ | ④ |
| 13. Staff and I respect each other’s knowledge and experience with regard to caring for the older adults residing in the facility. | ① | ② | ③ | ④ |
| 14. Staff and I understand and sympathize with each other’s difficulties in caring for the older adults residing in the facility. | ① | ② | ③ | ④ |
| 15. Staff and I find solutions together when problems occur regarding the older adults residing in the facility. | ① | ② | ③ | ④ |
| 16. Staff and I share a common goal in caring for the older adults residing in the facility. | ① | ② | ③ | ④ |
| Participation in care | ||||
| 17. I am involved in the care of the older adult residing in the facility. | ① | ② | ③ | ④ |
| 18. I pay enough attention to the older adult residing in the facility. | ① | ② | ③ | ④ |
| 19. I provide staff with information on the characteristics of the older adult before he or she is admitted. | ① | ② | ③ | ④ |
| 20. I actively participate when the staff ask for cooperation regarding the older adult residing in the facility. | ① | ② | ③ | ④ |
References
- United Nations. World Population Prospects 2019: Highlights: Report; United Nations, Department of Economic and Social Affairs, Population Division: New York, NY, USA, 2019. [Google Scholar]
- Economic and Social Commission for Asia and the Pacific. Population Ageing in East and North-East Asia. Available online: https://www.unescap.org/ageing-asia/countries (accessed on 1 March 2020).
- World Health Organization. Global Dementia Observatory. Available online: http://apps.who.int/gho/data/node.dementia (accessed on 1 March 2020).
- Centers for Disease Control and Prevention. About Chronic Diseases. Available online: https://www.cdc.gov/chronicdisease/about/index.htm (accessed on 1 March 2020).
- Jang, H.Y.; Yi, M. Hermeneutic phenomenological study on caring experience of spouses of elderly people with dementia at home. J. Korean Acad. Nurs. 2017, 47, 367–379. [Google Scholar] [CrossRef] [PubMed]
- National Institute on Aging. Caregiving. Available online: https://www.nia.nih.gov/health/caregiving (accessed on 3 March 2020).
- Alzheimer’s Disease International. World Alzheimer Report 2019: Attitudes to Dementia. Available online: https://www.alz.co.uk/research/world-report-2019 (accessed on 3 March 2020).
- Cooper, C.; Balamurali, T.B.S.; Livingston, G. A systematic review of the prevalence and covariates of anxiety in caregivers of people with dementia. Int. Psychogeriatr. 2007, 19, 175–195. [Google Scholar] [CrossRef] [PubMed]
- Kwon, S.H.; Tae, Y.S. The experience of adult Korean children caring for parents institutionalized with dementia. J. Korean Acad. Nurs. 2014, 44, 41–54. [Google Scholar] [CrossRef] [PubMed]
- Majerovitz, D.S. Predictors of burden and depression among nursing home family caregivers. Aging Ment. Health 2007, 11, 323–329. [Google Scholar] [CrossRef]
- Chang, Y.P.; Schneider, J.K. Decision-making process of nursing home placement among Chinese family caregivers. Perspect. Psychiatr. Care 2010, 46, 108–118. [Google Scholar] [CrossRef]
- Mast, M.E. To use or not to use: A literature review of factors that influence family caregivers’ use of support services. J. Gerontol. Nurs. 2013, 39, 20–28. [Google Scholar] [CrossRef]
- Gaugler, J.E. Family involvement in residential long-term care: A synthesis and critical review. Aging. Ment. Health 2005, 9, 105–118. [Google Scholar] [CrossRef]
- Bauer, M. Staff–family relationships in nursing home care: A typology of challenging behaviours. Int. J. Older People Nurs. 2007, 2, 213–218. [Google Scholar] [CrossRef]
- Choi, H. A comparative study on perceptions and expectations of families and care workers on elder care services in nursing facilities. J. Fam. Cult. 2010, 22, 1–31. [Google Scholar] [CrossRef]
- Janzen, W. Long-term care for older adults: The role of the family. J. Gerontol. Nurs. 2001, 27, 36–43. [Google Scholar] [CrossRef]
- Ryan, A.A.; Scullion, H.F. Nursing home placement: An exploration of the experiences of family carers. J. Adv. Nurs. 2000, 32, 1187–1195. [Google Scholar] [CrossRef] [PubMed]
- Robison, J.; Curry, L.; Gruman, C.; Porter, M.; Henderson, C.R.; Pillemer, K. Partners in caregiving in a special care environment: Cooperative communication between staff and families on dementia units. Gerontologist 2007, 47, 504–515. [Google Scholar] [CrossRef] [PubMed]
- Utley-Smith, Q.; Colón-Emeric, C.S.; Lekan-Rutledge, D.; Ammarell, N.; Bailey, D.; Corazzini, K.; Piven, M.L.; Anderson, R.A. Staff perceptions of staff-family interactions in nursing homes. J. Aging Stud. 2009, 23, 168–177. [Google Scholar] [CrossRef] [PubMed]
- Casey, A. Partnership nursing: Influences on involvement of informal carers. J. Adv. Nurs. 1995, 22, 1058–1062. [Google Scholar] [CrossRef]
- Espezel, H.J.; Canam, C.J. Parent–nurse interactions: Care of hospitalized children. J. Adv. Nurs. 2003, 44, 34–41. [Google Scholar] [CrossRef]
- Kawik, L. Nurses’ and parents’ perceptions of participation and partnership in caring for a hospitalized child. Br. J. Nurs. 1996, 5, 430–434. [Google Scholar] [CrossRef]
- Lee, P. What does partnership in care mean for children’s nurses? J. Clin. Nurs. 2007, 16, 518–526. [Google Scholar] [CrossRef]
- Casey, A. A partnership with child and family. Sr. Nurse 1988, 8, 8–9. [Google Scholar]
- Farrell, M. Partnership in care: Paediatric nursing model. Br. J. Nurs. 1992, 1, 175–176. [Google Scholar] [CrossRef]
- Wiggins, M.S. The partnership care delivery model. JONA J. Nurs. Adm. 2006, 36, 341–345. [Google Scholar] [CrossRef]
- Wiggins, M.S. The partnership care delivery model: An examination of the core concept and the need for a new model of care. J. Nurs. Manag. 2008. 16, 629–638.
- Coyne, I.; Cowley, S. Challenging the philosophy of partnership with parents: A grounded theory study. Int. J. Nurs. Stud. 2007, 44, 893–904. [Google Scholar] [CrossRef] [PubMed]
- Power, N.; Franck, L. Parent participation in the care of hospitalized children: A systematic review. J. Adv. Nurs. 2008, 62, 622–641. [Google Scholar] [CrossRef] [PubMed]
- Haesler, E.; Bauer, M.; Nay, R. Recent evidence on the development and maintenance of constructive staff–family relationships in the care of older people–a report on a systematic review update. Int. J. Evid. Based Healthc. 2010, 8, 45–74. [Google Scholar] [CrossRef] [PubMed]
- Jones, J.A.; Barry, M. Developing a scale to measure trust in health promotion partnerships. Health Promot. Int. 2011, 26, 484–491. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.C.; Boren, D.; Solem, S.L. The Kim Alliance Scale: Development and preliminary testing. Clin. Nurs. Res. 2001, 10, 314–331. [Google Scholar] [CrossRef]
- Kiriake, A.; Moriyama, M. Development and testing of the partnership scale for primary family caregivers caring for patients with dementia. J. Fam. Nurs. 2016, 22, 339–367. [Google Scholar] [CrossRef]
- Hinkin, T.R. A brief tutorial on the development of measures for use in survey questionnaires. Organ Res. Methods 1998, 1, 104–121. [Google Scholar] [CrossRef]
- Anderson, J.C.; Gerbing, D.W. Structural equation modeling in practice: A review and recommended two-step approach. Psychol. Bull. 1988, 103, 411–413. [Google Scholar] [CrossRef]
- DeVellis, R.F. Scale Development: Theory and Applications, 3rd ed.; SAGE Publications: Thousand Oaks, CA, USA, 2012. [Google Scholar]
- Morgado, F.F.R.; Meireles, J.F.F.; Neves, C.M.; Amaral, A.C.S.; Ferreira, M.E.C. Scale development: Ten main limitations and recommendations to improve future research practices. Psicol. Reflexão Crítica 2018, 30, 1–20. [Google Scholar] [CrossRef]
- Hinkin, T.R. A review of scale development practices in the study of organizations. J. Manag. 1995, 21, 967–988. [Google Scholar] [CrossRef]
- Kapuscinski, A.N.; Masters, K.S. The current status of measures of spirituality: A critical review of scale development. Psycholog. Relig. Spiritual. 2010, 2, 191–205. [Google Scholar] [CrossRef]
- Kreuger, R.A. Focus Group: A Practical Guide for Applied Research, 2nd ed.; SAGE Publications: Thousand Oaks, CA, USA, 1994. [Google Scholar]
- Morgan, D.L. Focus Groups as Qualitative Research, 2nd ed.; SAGE Publications: Thousand Oaks, CA, USA, 1997. [Google Scholar]
- Hsieh, H.F.; Shannon, S.E. Three approaches to qualitative content analysis. Qual. Health Res. 2005, 15, 1277–1288. [Google Scholar] [CrossRef] [PubMed]
- Streiner, D.L.; Norman, G.R. Health Measurement Scales: A Practical Guide to Their Development and Use; Oxford University Press: London, UK, 2008. [Google Scholar]
- Maas, M.; Buckwalter, K. Final Report: Phase II Nursing Evaluation Research: Alzheimer’s Care Unit; National Institutes of Health: Rockville, MD, USA, 1990.
- Park, M. Korean family caregivers’ perceptions of care in dementia care units. J. Korean Acad. Nurs. 2002, 32, 967–976. [Google Scholar] [CrossRef]
- Jablonski, R.A.; Reed, D.; Maas, M.L. Care intervention for older adults with Alzheimer’s disease and related dementias: Effect of family involvement on cognitive and functional outcomes in nursing homes. J. Gerontol. Nurs. 2005, 31, 38–48. [Google Scholar] [CrossRef] [PubMed]
- Maas, M.L.; Reed, D.; Park, M.; Specht, J.P.; Schutte, D.; Kelley, L.S.; Swanson, E.A.; Trip-Reimer, T.; Buckwalte, K.C. Outcomes of family involvement in care intervention for caregivers of individuals with dementia. Nurs. Res. 2004, 53, 76–86. [Google Scholar] [CrossRef] [PubMed]
- Specht, J.P.; Kelley, L.S.; Manion, P.; Maas, M.L.; Reed, D.; Rantz, M.J. Who’s the boss? Family/staff partnership in care of persons with dementia. Nurs. Adm. Q. 2000, 24, 64–77. [Google Scholar] [CrossRef]
- Field, A. Discovering Statistics Using IBM SPSS Statistics: And Sex and Drugs and Rock ‘n’ Roll, 4th ed.; Sage: London, UK, 2013. [Google Scholar]
- Hair, J.F.; Black, W.C.; Babin, B.J.; Anderson, R.E. Multivariate Data Analysis: A Global Perspective, 7th ed.; Pearson Prentice Hall: Upper Saddle River, NJ, USA, 2010. [Google Scholar]
- Yu, J.P. The Concept and Understanding of Structural Equation Modeling; Hannare Publishing Co.: Seoul, Korea, 2012; pp. 160–370. [Google Scholar]
- Heo, J. Structural Equation Modeling with AMOS; Hannarae Publishing Co.: Seoul, Korea, 2013. [Google Scholar]
- Bagozzi, R.P.; Yi, Y. On the evaluation of structural equation models. J. Acad. Mark. Sci. 1988, 16, 74–94. [Google Scholar] [CrossRef]
- Port, C.L.; Zimmerman, S.; Williams, C.S.; Dobbs, D.; Preisser, J.S.; Williams, S.W. Families filling the gap: Comparing family involvement for assisted living and nursing home residents with dementia. Gerontologist 2004, 45, 87–95. [Google Scholar] [CrossRef]
- Chrisman, N.J.; Senturia, K.; Tang, G.; Gheisar, B. Qualitative process evaluation of urban community work: A preliminary view. Health Ed. Behav. 2002, 29, 232–248. [Google Scholar] [CrossRef]
- Johnson, B.; Abraham, M. Partnering with Patients, Residents, and Families: A Resource for Leaders of Hospitals, Ambulatory Care Settings, and Long-Term Care Communities; Institute for Patient-and Family-Centered Care: Bethesda, MD, USA, 2012. [Google Scholar]


| Variables | Category | Total | Group A for EFA (n = 165) | Group B for CFA (n = 165) | t or χ2 (p) |
|---|---|---|---|---|---|
| n (%) or Mean ± SD | |||||
| Age (year) | 53.67 ± 11.04 | 54.85 ± 10.44 | 52.50 ± 11.51 | 1.94 (0.053) | |
| Gender | Female | 205 (62.1) | 105 (63.6) | 100 (60.6) | 0.32 (0.570) |
| Male | 125 (37.9) | 60 (36.4) | 65 (39.4) | ||
| Education | ≤Middle school | 19 (5.7) | 8 (4.8) | 11 (6.7) | 0.51 (0.773) |
| High school | 90 (27.3) | 45 (27.3) | 45 (27.3) | ||
| ≥College | 221 (67.0) | 112 (67.9) | 109 (66.0) | ||
| Perceived economic status | Good | 28 (8.5) | 16 (9.7) | 12 (7.3) | 3.40 (0.183) |
| Moderate | 265 (80.3) | 126 (76.4) | 139 (84.2) | ||
| Poor | 37 (11.2) | 23 (13.9) | 14 (8.5) | ||
| Perceived health status | Good | 43 (13.0) | 23 (13.9) | 20 (12.1) | 0.40 (0.817) |
| Moderate | 151 (45.8) | 73 (44.3) | 78 (47.3) | ||
| Poor | 136 (41.2) | 69 (41.8) | 67 (40.6) | ||
| Perceived stress status | Low | 96 (29.1) | 46 (27.9) | 50 (30.3) | 0.24 (0.628) |
| High | 234 (70.9) | 119 (72.1) | 115 (69.7) | ||
| Size of facilities | ≤29 beds | 28 (8.5) | 11 (6.7) | 17 (10.3) | 3.55 (0.170) |
| 30–99 beds | 132 (40.0) | 61 (37.0) | 71 (43.0) | ||
| ≥100 beds | 170 (51.5) | 93 (56.3) | 77 (46.7) | ||
| Relationship to older adult resident | Spouse | 16 (4.8) | 8 (4.8) | 8 (4.8) | 5.24 (0.388) |
| Adult child | 198 (60.0) | 105 (63.6) | 93 (56.4) | ||
| Daughter-in-law | 59 (17.9) | 30 (18.2) | 29 (17.6) | ||
| Son-in-law | 23 (7.0) | 11 (6.7) | 12 (7.3) | ||
| Others | 34 (10.3) | 11 (6.7) | 23 (13.9) | ||
| Duration of caring at home (month) | 53.52 ± 89.85 | 51.47 ± 86.13 | 55.56 ± 93.65 | −0.41 (0.680) | |
| Factor/Item Contents | Mean ± SD | Factor Loadings | Commonality | Explained Variance (%) | ITC | Cron- Bach’s α If Item Deleted | Cron- Bach’s α | ICC (95%CI) (n = 27) | AVE | CCR | ||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | ||||||||||
| Factor 1 | 30.4 | 0.93 | 0.80 (0.57–0.91) | 0.79 | 0.97 | |||||||
| 27. Staff encourage the family to visit the facility. | 3.08 ± 0.75 | 0.79 | 0.18 | 0.16 | 0.68 | 0.70 | 0.95 | |||||
| 28. Staff positively support family involvement in providing care (e.g., conversation, taking a walk, meal assistance, etc.). | 3.26 ± 0.58 | 0.78 | 0.20 | 0.19 | 0.69 | 0.74 | 0.95 | |||||
| 29. Staff welcome the family when they visit the facility. | 3.28 ± 0.69 | 0.75 | 0.26 | 0.17 | 0.66 | 0.70 | 0.95 | |||||
| 39. Staff inform the family about the regulations and the policies of the facility before he or she is admitted. | 3.31 ± 0.59 | 0.74 | 0.18 | 0.22 | 0.64 | 0.70 | 0.95 | |||||
| 34. Staff respect and support the families’ decision-making on the older adults residing in the facility. | 3.22 ± 0.60 | 0.71 | 0.40 | 0.17 | 0.69 | 0.77 | 0.94 | |||||
| 36. Staff provide appropriate care on the condition of the older adults residing in the facility. | 3.23 ± 0.58 | 0.71 | 0.46 | 0.17 | 0.74 | 0.79 | 0.94 | |||||
| 37. Staff provide care while maintaining the dignity of the older adults residing in the facility. | 3.20 ± 0.61 | 0.70 | 0.35 | 0.26 | 0.68 | 0.77 | 0.95 | |||||
| 26. Staff inform the family about the condition or changes in the condition of the older adults residing in the facility. | 3.35 ± 0.59 | 0.67 | 0.40 | 0.19 | 0.65 | 0.74 | 0.95 | |||||
| 35. Staff are sensitive to changes in the state of the older adults residing in the facility. | 3.10 ± 0.69 | 0.67 | 0.34 | 0.00 | 0.56 | 0.63 | 0.95 | |||||
| 32. Staff involve families when planning care for the older adults residing in the facility. | 2.95 ± 0.68 | 0.63 | 0.31 | 0.06 | 0.50 | 0.65 | 0.95 | |||||
| Factor 2 | 22.1 | 0.91 | 0.71 (0.36–0.87) | 0.81 | 0.96 | |||||||
| 16. Staff and I communicate smoothly regarding caring for the older adult. | 3.28 ± 0.60 | 0.32 | 0.77 | 0.22 | 0.76 | 0.74 | 0.95 | |||||
| 20. Staff and I discuss the range of roles that each other should take in caring for the older adult. | 3.14 ± 0.64 | 0.33 | 0.77 | 0.22 | 0.75 | 0.73 | 0.95 | |||||
| 21. Staff and I respect each other’s knowledge and experience with regard to caring for the older adults residing in the facility. | 3.30 ± 0.57 | 0.36 | 0.70 | 0.30 | 0.70 | 0.71 | 0.95 | |||||
| 19. Staff and I understand and sympathize with each other’s difficulties in caring for the older adults residing in the facility. | 3.29 ± 0.57 | 0.49 | 0.69 | 0.15 | 0.73 | 0.75 | 0.95 | |||||
| 22. Staff and I find solutions together when problems occur regarding the older adults residing in the facility. | 3.32 ± 0.60 | 0.34 | 0.68 | 0.26 | 0.65 | 0.72 | 0.95 | |||||
| 18. Staff and I share a common goal in caring for the older adults residing in the facility. | 3.30 ± 0.63 | 0.39 | 0.67 | 0.32 | 0.71 | 0.75 | 0.95 | |||||
| Factor 3 | 13.3 | 0.74 | 0.85 (0.67–0.93) | 0.68 | 0.89 | |||||||
| 10. I am involved in the care of the older adult residing in the facility. | 3.24 ± 0.61 | 0.10 | 0.09 | 0.81 | 0.67 | 0.44 | 0.95 | |||||
| 12. I pay enough attention to the older adult residing in the facility. | 3.27 ± 0.51 | 0.21 | 0.15 | 0.77 | 0.66 | 0.48 | 0.95 | |||||
| 3. I provide staff with information on the characteristics of the older adult before he or she is admitted. | 3.48 ± 0.57 | 0.13 | 0.39 | 0.64 | 0.57 | 0.50 | 0.95 | |||||
| 6. I actively participate when the staff ask for cooperation regarding the older adult residing in the facility. | 3.52 ± 0.57 | 0.19 | 0.36 | 0.56 | 0.48 | 0.51 | 0.95 | |||||
| Total | 65.8 | 0.95 | 0.83 (0.62–0.92) | |||||||||
| KMO = 0.94, Bartlett’s test: χ2 = 2252.85 (p < 0.001) | ||||||||||||
| Measurement | SPIC-F | Factor 1 | Factor 2 | Factor 3 |
|---|---|---|---|---|
| r (p) | r (p) | r (p) | r (p) | |
| FPCT | 0.64 (<0.001) | 0.68 (<0.001) | 0.55 (<0.001) | 0.28 (<0.001) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jang, H.-Y.; Song, E.-O. Development and Validation of the Scale for Partnership in Care—for Family (SPIC-F). Int. J. Environ. Res. Public Health 2020, 17, 1882. https://doi.org/10.3390/ijerph17061882
Jang H-Y, Song E-O. Development and Validation of the Scale for Partnership in Care—for Family (SPIC-F). International Journal of Environmental Research and Public Health. 2020; 17(6):1882. https://doi.org/10.3390/ijerph17061882
Chicago/Turabian StyleJang, Hye-Young, and Eun-Ok Song. 2020. "Development and Validation of the Scale for Partnership in Care—for Family (SPIC-F)" International Journal of Environmental Research and Public Health 17, no. 6: 1882. https://doi.org/10.3390/ijerph17061882
APA StyleJang, H.-Y., & Song, E.-O. (2020). Development and Validation of the Scale for Partnership in Care—for Family (SPIC-F). International Journal of Environmental Research and Public Health, 17(6), 1882. https://doi.org/10.3390/ijerph17061882