Long-Term Subjective Outcomes of Barbed Reposition Pharyngoplasty for Obstructive Sleep Apnea Syndrome Treatment

 ,
, 
 ,
,  ,
,  ,
,  ,
,  ,
,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Enrollment of the Patients and Inclusion/Exclusion Criteria
2.2. Patient’s Characteristics
2.3. Investigated Parameters
2.4. Statistical Analysis
3. Results
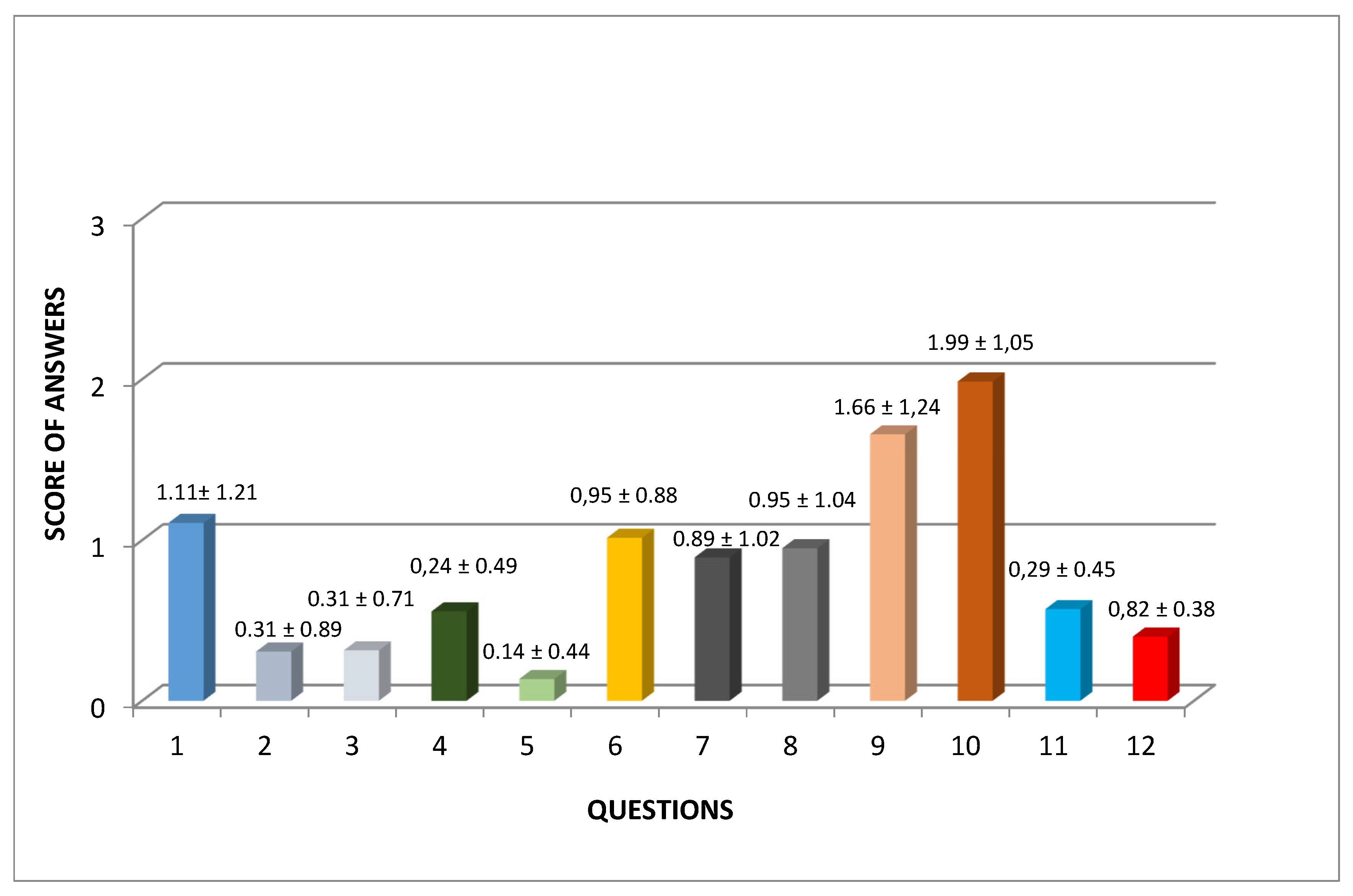
3.1. PPOPS Results
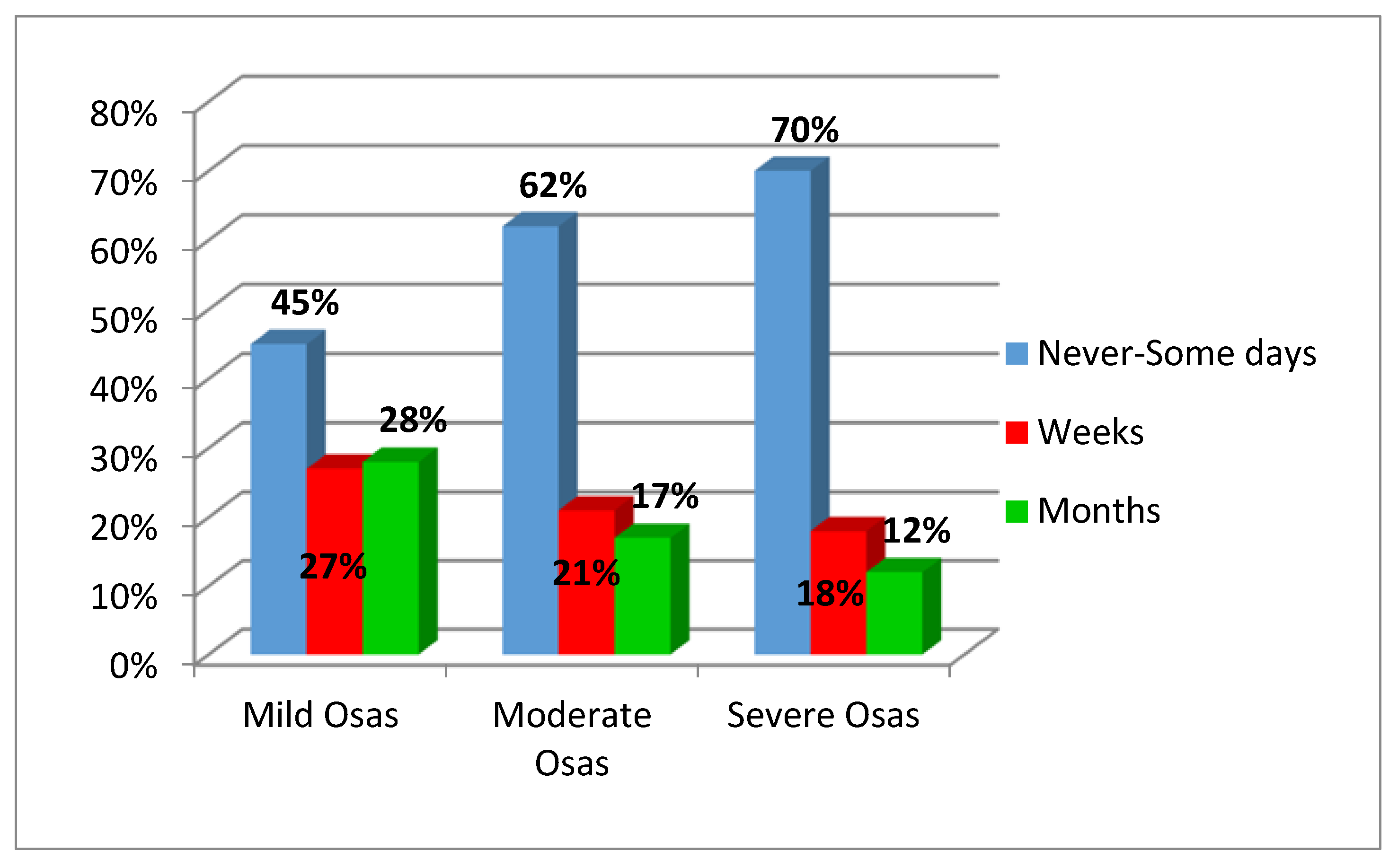
3.2. Swallowing Problems
3.3. Rhinolalia
3.4. Nose Regurgitation
3.5. Loss of Weight
3.6. Foreign Body Sensation in the Throat
3.7. Sticky Mucus in the Throat
3.8. Painful Sensation
3.9. Discourage Others from Undergoing the Procedure?
3.10. Preoperative and Postoperative AHI
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Young, T.; Peppard, P.E.; Gottlieb, D.J. Epidemiology of obstructive sleep apnea: A population health perspective. Am. J. Respir. Crit. Care Med. 2002, 165, 1217–1239. [Google Scholar] [CrossRef]
- Iannella, G.; Vicini, C.; Colizza, A.; Meccariello, G.; Polimeni, A.; Greco, A.; de Vincentiis, M.; de Vito, A.; Cammaroto, G.; Gobbi, R.; et al. Aging effect on sleepiness and apneas severity in patients with obstructive sleep apnea syndrome: A meta-analysis study. Eur. Arch. Otorhinolaryngol. 2019, 276, 3549–3556. [Google Scholar] [CrossRef] [PubMed]
- Veasey, S.C.; Rosen, I.M. Obstructive Sleep Apnea in Adults. N. Engl. J. Med. 2019, 11, 1442–1449. [Google Scholar] [CrossRef] [PubMed]
- Bonsignore, M.R.; Marrone, O.; Fanfulla, F. Sleep Apnea, Sleepiness, and Driving Risk. Sleep Med. Clin. 2019, 14, 431–439. [Google Scholar] [CrossRef]
- Magliulo, G.; de Vincentiis, M.; Iannella, G.; Ciofalo, A.; Manno, A.; Pasquariello, B.; Angeletti, D.; Pace, A.; Gulotta, G.; Polimeni, A. Eustachian tube evaluation in patients with obstructive sleep apnea syndrome. Acta Otolaryngol. 2018, 138, 159–164. [Google Scholar] [CrossRef] [PubMed]
- Vicini, C.; Meccariello, G.; Montevecchi, F.; De Vito, A.; Frassineti, S.; Gobbi, R.; Pelucchi, S.; Iannella, G.; Magliulo, G.; Cammaroto, G. Effectiveness of barbed repositioning pharyngoplasty for the treatment of obstructive sleep apnea (OSA): A prospective randomized trial. Sleep Breath. 2019, 1–8, [Epub ahead of print]. [Google Scholar] [CrossRef] [PubMed]
- Chi, J.C.; Chiang, R.P.; Chou, T.Y.; Shu, C.H.; Shiao, A.S.; Lin, C.M. The role of lateral pharyngoplasty in obstructive sleep apnea syndrome. Eur. Arch. Otorhinolaryngol. 2015, 272, 489–496. [Google Scholar] [CrossRef] [PubMed]
- Dizdar, D.; Civelek, Ş.; Çaliş, Z.A.; Dizdar, S.K.; Coşkun, B.U.; Vural, A. Comparative Analysis of Lateral Pharyngoplasty and Uvulopalatopharyngoplasty Techniques with Polisomnography and Epworth Sleepiness Scales. J. Craniofacial Surg. 2015, 26, e647–e651. [Google Scholar] [CrossRef]
- Vicini, C.; Hendawy, E.; Campanini, A.; Eesa, M.; Bahgat, A.; AlGhamdi, S.; Meccariello, G.; De Vito, A.; Montevecchi, F.; Mantovani, M. Barbed Reposition Pharyngoplasty (BRP) for OSAHS: A feasibility, safety, efficacy and teachability pilot study. “We are on the giant’s shoulders”. Eur. Arch. Otorhinolaryngol. 2015, 272, 3065–3070. [Google Scholar] [CrossRef]
- Montevecchi, F.; Meccariello, G.; Firinu, E.; Rashwan, M.S.; Arigliani, M.; De Benedetto, M.; Palumbo, A.; Bahgat, Y.; Bahgat, A.; Lugo Saldana, R.; et al. Prospective multicentre study on barbed reposition pharyngoplasty standing alone or as a part of multilevel surgery for sleep apnoea. Clin. Otolaryngol. 2018, 43, 483–488. [Google Scholar] [CrossRef]
- Madkikar, N.; Pandey, S.; Ghaisas, V. Multi Level Single Stage: Barbed Reposition Pharyngoplasty and Nasal Surgery in Treatment of OSA-Our Experience. Indian J. Otolaryngol. Head Neck Surg. 2019, 71, 309–314. [Google Scholar] [CrossRef]
- Pang, K.P.; Vicini, C.; Montevecchi, F.; Piccin, O.; Chandra, S.; Yang, H.C.; Agrawal, V.; Chung, J.C.; Chan, Y.H.; Pang, S.B.; et al. Long-term complications of palate surgery: A multicenter study of 217 patients. Laryngoscope 2019. [Epub ahead of print]. [Google Scholar] [CrossRef] [PubMed]
- Grover, R.; Barnett, A.; Rampazzo, A.; Papay, F.; Gharb, B.B. Outcomes of Sphincter Pharyngoplasty in the Cleft Population. J. Craniofacial Surg. 2018, 29, 908–913. [Google Scholar] [CrossRef] [PubMed]
- Li, H.Y.; Lee, L.A.; Fang, T.J.; Lin, W.N.; Lin, W.Y. Evaluation of velopharyngeal function after relocation pharyngoplasty for obstructive sleep apnea. Laryngoscope 2010, 120, 1069–1073. [Google Scholar] [CrossRef] [PubMed]
- Corradi, A.M.B.; Valarelli, L.P.; Grechi, T.H.; Eckeli, A.L.; Aragon, D.C.; Küpper, D.S.; Almeida, L.A.; Sander, H.H.; Trawitzki, L.V.; Valera, F.C. Swallowing evaluation after surgery for obstructive sleep apnea syndrome: Uvulopalatopharyngoplasty vs. expansion pharyngoplasty. Eur. Arch. Otorhinolaryngol. 2018, 275, 1023–1030. [Google Scholar] [CrossRef]
- Wischhusen, J.; Qureshi, U.; Camacho, M. Laser-assisted uvulopalatoplasty (LAUP) complications and side effects: A systematic review. Nat. Sci. Sleep 2019, 27, 59–67. [Google Scholar] [CrossRef]
- Rashwan, M.S.; Montevecchi, F.; Firinua, E. Let’s know from our patients: PPOPS score for palate surgery evaluation/a pilot study. Eur. Arch. Otorhinolaryngol. 2018, 275, 287–291. [Google Scholar] [CrossRef]
- Ruehland, W.R.; Rochford, P.D.; O’Donoghue, F.J.; Pierce, R.J.; Singh, P.; Thornton, A.T. The new AASM criteria for scoring hypopneas: Impact on the apnea hypopnea index. Sleep Res. Soc. 2009, 32, 150–157. [Google Scholar] [CrossRef]
- Heinzer, R.; Petitpierre, N.J.; Marti-Soler, H.; Haba-Rubio, J. Incidence and characteristics of positional sleep apnea in the HypnoLaus population-based cohort. Sleep Med. 2018, 48, 157–162. [Google Scholar] [CrossRef]
- Iannella, G.; Vicini, C.; Polimeni, A.; Greco, A.; Gobbi, R.; Montevecchi, F.; De Vito, A.; Meccariello, G.; Cammaroto, G.; D’Agostino, G.; et al. Laryngopharyngeal Reflux Diagnosis in Obstructive Sleep Apnea Patients Using the Pepsin Salivary Test. Int. J. Environ. Res. Public Health 2019, 16, 2056. [Google Scholar] [CrossRef]
- Magliulo, G.; Iannella, G.; Ciofalo, A.; Polimeni, A.; De Vincentiis, M.; Pasquariello, B.; Montevecchi, F.; Vicini, C. Nasal pathologies in patients with obstructive sleep apnoea. Acta Otorhinolaryngol. Ital. 2019, 39, 250–256. [Google Scholar] [CrossRef] [PubMed]
- Vicini, C.; De Vito, A.; Iannella, G.; Gobbi, R.; Corso, R.M.; Montevecchi, F.; Polimeni, A.; De Vincentiis, M.; Meccariello, G.; D’agostino, G.; et al. The aging effect on upper airways collapse of patients with obstructive sleep apnea syndrome. Eur. Arch. Otorhinolaryngol. 2018, 275, 2983–2990. [Google Scholar] [CrossRef]
- Staderini, E.; De Luca, M.; Candida, E.; Rizzo, M.I.; Rajabtork Zadeh, O.; Bucci, D.; Zama, M.; Lajolo, C.; Cordaro, M.; Gallenzi, P. Lay People Esthetic Evaluation of Primary Surgical Repair on Three-Dimensional Images of Cleft Lip and Palate Patients. Medicina 2019, 55, 576. [Google Scholar] [CrossRef] [PubMed]
- Modica, D.M.; Lorusso, F.; Presti, G.; Fasola, S.; Gallina, S. Our Assessment Using Palate Postoperative Problems Score (PPOPS): Tool for the Evaluation of Results in Palatal Surgery Techniques. Indian J. Otolaryngol. Head Neck Surg. 2019, 71, 766–770. [Google Scholar] [CrossRef] [PubMed]
- Goh, Y.H.; Mark, I.; Fee, W.E., Jr. Quality of life 17 to 20 years after uvulopalatopharyngoplasty. Laryngoscope 2007, 117, 503–506. [Google Scholar] [CrossRef] [PubMed]
- Tang, J.A.; Salapatas, A.M.; Bonzelaar, L.B.; Friedman, M. Long-Term Incidence of Velopharyngeal Insufficiency and Other Sequelae following Uvulopalatopharyngoplasty. Otolaryngol. Head Neck Surg. 2017, 156, 606–610. [Google Scholar] [CrossRef] [PubMed]
- Värendh, M.; Berg, S.; Andersson, M. Long-term follow-up of patients operated with Uvulopalatopharyngoplasty from 1985 to 1991. Respir. Med. 2012, 106, 1788–1793. [Google Scholar] [CrossRef][Green Version]



{kind=link}
{kind=link}
| Name____________________________________ | Age____ | |||
|---|---|---|---|---|
| Date and type of operation______________________________________________ Date of questionnaire and examination____________________________________ | ||||
| QUESTIONS | SCORE | |||
| 0 | 1 | 2 | 3 | |
| (1) Did you have any swallowing problems after surgery | Never | Days | Weeks | Months |
| (2) The problems resolved | Spontaneously | With a doctor | With the speechterapist | Unresolved |
| (3) Residual difficulty in swallowing | No | Mild | Moderate | Severe |
| (4) Residual nasal tone of voice | No | Mild | Moderate | Severe |
| (5) Residual regurgitation of liquid into the nose | Never | Rarely | Often | Always |
| (6) Any weight loss recorded after surgery | No | Mild | Moderate | Severe |
| (7) Any foreign body sensation in the throat | No | Mild | Moderate | Severe |
| (8) Do you feel sticky mucus in the throat | No | Mild | Moderate | Severe |
| (9) Painful sensation in the throat at rest | No | Mild | Moderate | Severe |
| (10) Painful sensation in the throat while swallowing | No | Mild | Moderate | Severe |
| (11) Do you have different ad a worse feeling in the throat after surgery | No | Mild | Moderate | Severe |
| (12) Do you discourage the procedure to others | No | Mild | Moderate | Severe |
| Total Score_______ | ||||
| Item for each score from 0 to 3 | ||||
| Total Score 0/36 | ||||
| Number of Patients | Percentage | |
|---|---|---|
| Sex | ||
| Female | 10 | 7% |
| Male | 130 | 93% |
| Age | ||
| <40 | 33 | 24% |
| 40–65 | 94 | 67% |
| >65 | 13 | 9% |
| OSA severity | ||
| Mild | 53 | 38% |
| Moderate | 29 | 21% |
| Severe | 49 | 35% |
| BMI | ||
| <25 | 31 | 26% |
| 25–30 | 62 | 51% |
| >30 | 28 | 23% |
| Type of surgery | ||
| BRP and nasal surgery | 130 | 93% |
| Only BRP surgery | 10 | 7% |
| Days of hospitalization | ||
| <2 | 16 | 11% |
| 3–6 | 103 | 74% |
| >6 | 21 | 15% |
| ITEM | Never N/% | Days N/% | Weeks N/% | Months N/% |
|---|---|---|---|---|
| Swallowing problems in the postoperative period | 69/49 | 15/11 | 29/21 | 27/19 |
| No N/% | Mild N/% | Moderate N/% | Severe N/% | |
| Residual Swallowing difficult (PPOPS evaluation) | 127/91 | 11/8 | 2/1 | 0/0 |
| Rhinolalia (PPOPS evaluation) | 129/92 | 8/6 | 3/2 | 0/0 |
| Never N/% | Rarely N/% | Often N/% | Always N/% | |
| Nose regurgitation (PPOPS evaluation) | 138/98 | 1/1 | 1/1 | 0/0 |
| 0–5 Kg N/% | 6–20 Kg N/% | |||
| Weight loss (PPOPS evaluation) | 90/64 | 50/36 | ||
| No N/% | Mild N/% | Moderate N/% | Severe N/% | |
| Foreign body in throat after surgery | 67/48 | 34/24 | 27/19 | 12/9 |
| Sticky mucus in throat | 119/85 | 18/13 | 3/2 | 0/0 |
| Pain in throat at rest after surgery | 92/66 | 14/10 | 20/14 | 28/20 |
| Pain in throat during swallowing after surgery | 41/29 | 15/11 | 34/24 | 50/36 |
| YES N/% | NO N/% | I don’t know N/% | ||
| Discourage others to procedure? (PPOPS evaluation) | 22/16 | 108/77 | 10/7 | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Iannella, G.; Vallicelli, B.; Magliulo, G.; Cammaroto, G.; Meccariello, G.; De Vito, A.; Greco, A.; Pelucchi, S.; Sgarzani, R.; Corso, R.M.; et al. Long-Term Subjective Outcomes of Barbed Reposition Pharyngoplasty for Obstructive Sleep Apnea Syndrome Treatment. Int. J. Environ. Res. Public Health 2020, 17, 1542. https://doi.org/10.3390/ijerph17051542
Iannella G, Vallicelli B, Magliulo G, Cammaroto G, Meccariello G, De Vito A, Greco A, Pelucchi S, Sgarzani R, Corso RM, et al. Long-Term Subjective Outcomes of Barbed Reposition Pharyngoplasty for Obstructive Sleep Apnea Syndrome Treatment. International Journal of Environmental Research and Public Health. 2020; 17(5):1542. https://doi.org/10.3390/ijerph17051542
Chicago/Turabian StyleIannella, Giannicola, Bianca Vallicelli, Giuseppe Magliulo, Giovanni Cammaroto, Giuseppe Meccariello, Andrea De Vito, Antonio Greco, Stefano Pelucchi, Rossella Sgarzani, Ruggero Massimo Corso, and et al. 2020. "Long-Term Subjective Outcomes of Barbed Reposition Pharyngoplasty for Obstructive Sleep Apnea Syndrome Treatment" International Journal of Environmental Research and Public Health 17, no. 5: 1542. https://doi.org/10.3390/ijerph17051542
APA StyleIannella, G., Vallicelli, B., Magliulo, G., Cammaroto, G., Meccariello, G., De Vito, A., Greco, A., Pelucchi, S., Sgarzani, R., Corso, R. M., Napoli, G., Bianchi, G., Cocuzza, S., Maniaci, A., & Vicini, C. (2020). Long-Term Subjective Outcomes of Barbed Reposition Pharyngoplasty for Obstructive Sleep Apnea Syndrome Treatment. International Journal of Environmental Research and Public Health, 17(5), 1542. https://doi.org/10.3390/ijerph17051542