Hybrid Methodology to Improve Health Status Utility Values Derivation Using EQ-5D-5L and Advanced Multi-Criteria Techniques

Abstract
1. Introduction
2. Current Issues
3. Materials and Methods
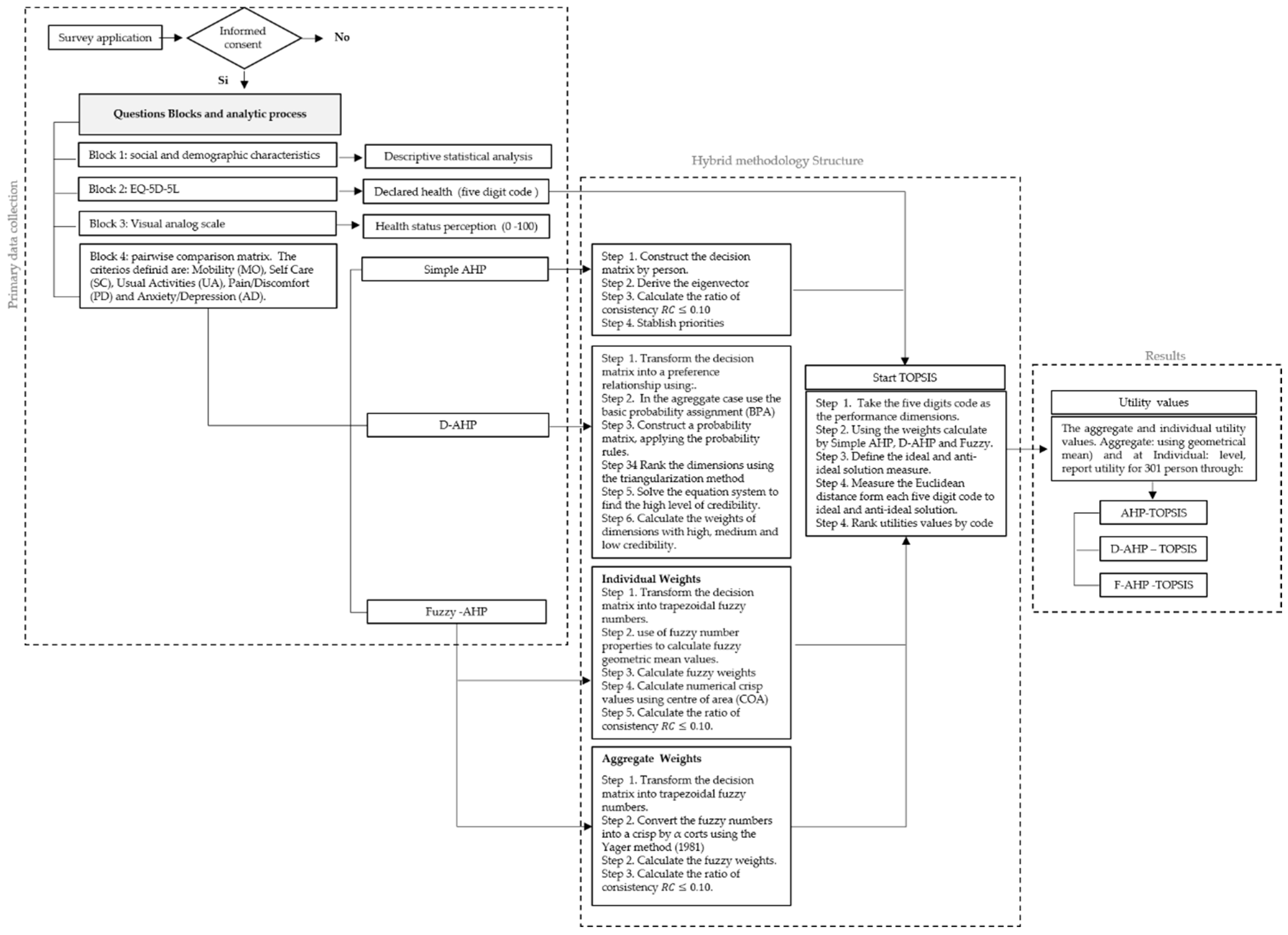
3.1. Study Design
3.2. The Proposed Model
3.2.1. Analytic Hierarchy Process (AHP)
3.2.2. AHP with a D-Number Extended Fuzzy Preference Relation (D-AHP)
- Calculated the sum by rows.
- Deleted the row and column with the highest number derived in step . The first to be removed represented the most preferred dimension, and so on.
- Repeated (i) and (ii) until the probability matrix was empty.
- Constructed a new R matrix, considering the order of the eliminated rows called
3.2.3. Fuzzy AHP (F-AHP)

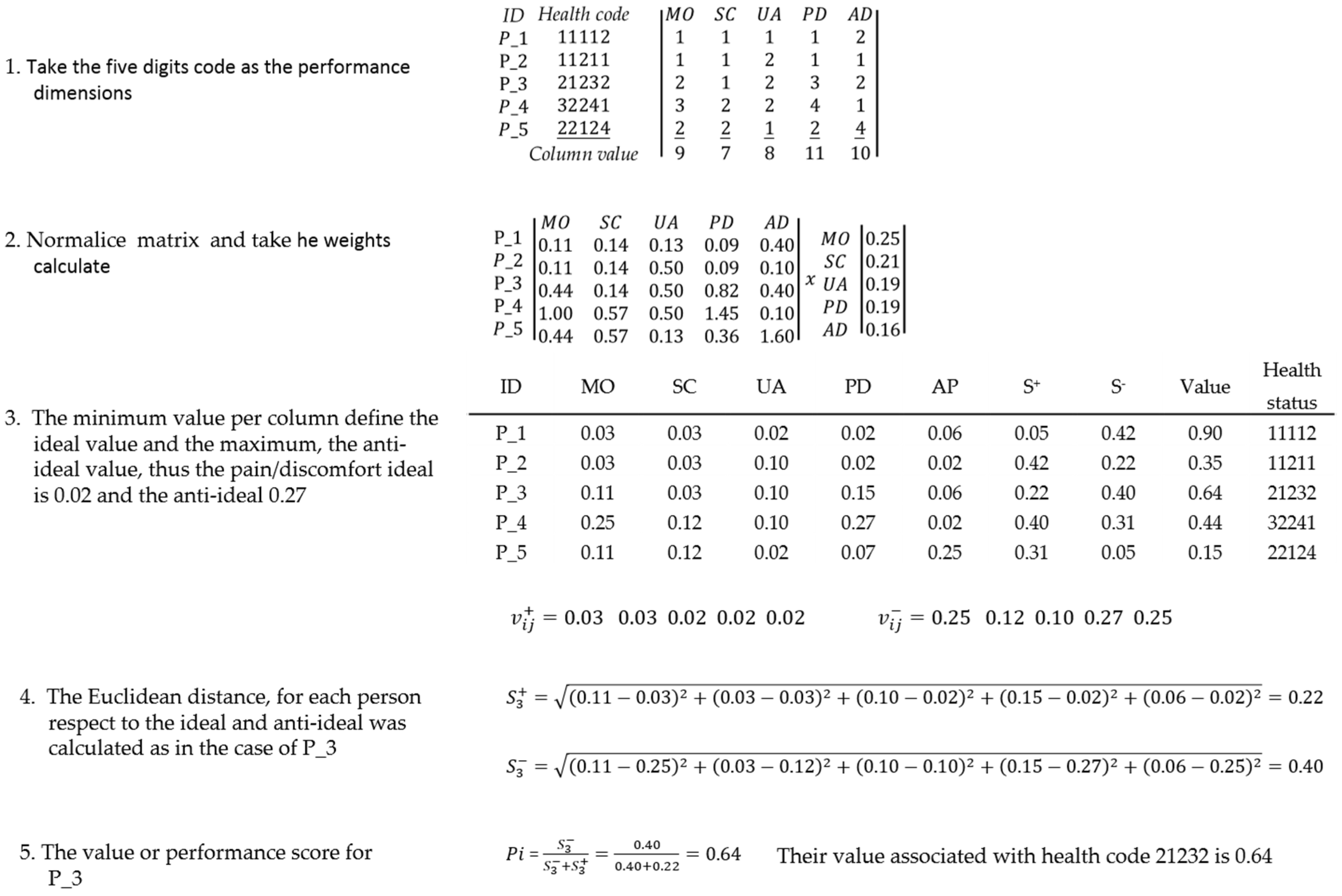
3.2.4. The Technique for Order Performance by Similarity to the Ideal Solution (TOPSIS)
3.2.5. Numerical Example
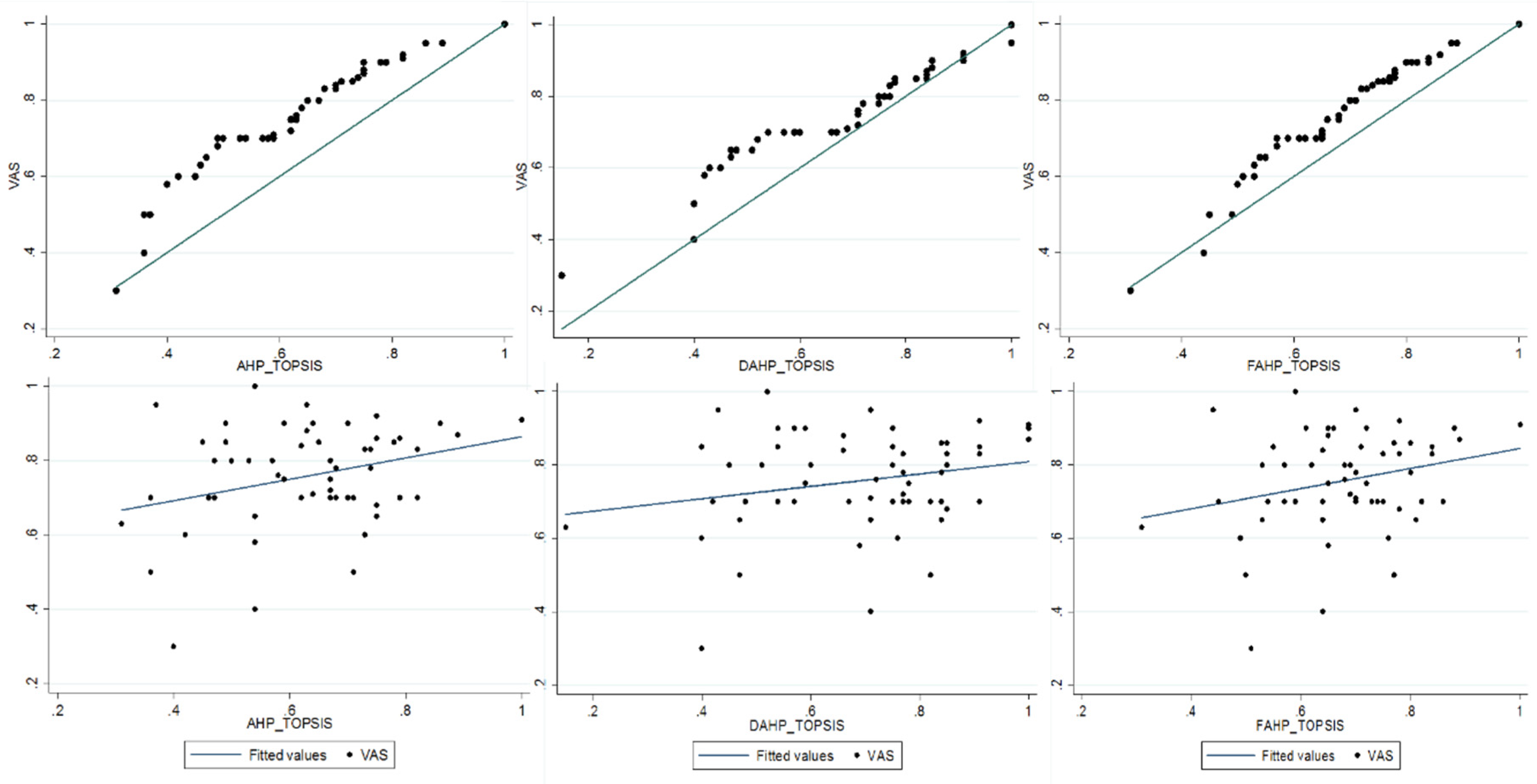
4. Results and Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Wang, P.; Hammer, P. Assumptions of decision-making models in AGI. In International Conference on Artificial General Intelligence; Springer: Cham, The Switzerland, 2015. [Google Scholar]
- Torrance, G.W.; Thomas, W.H.; Sackett, D.L. A Utility Maximization Model for evaluation of health care programs. Health Serv. Res. 1972, 7, 118–133. [Google Scholar] [PubMed]
- Torrance, G.W. Toward a utility theory foundation for health status index models. Health Serv. Res. 1976, 11, 349–369. [Google Scholar] [PubMed]
- Dolan, P.; Gudex, C.; Kind, P.; Williams, A. Valuing health states: A comparison of methods. J. Health Econ. 1996, 15, 209–231. [Google Scholar] [CrossRef]
- Feeny, D. Response to Lenert and Kaplan: The utility approach to assessing health-related quality of life. Med. Care 2000, 38, 51–154. [Google Scholar] [CrossRef]
- Kopec, J.A.; Schultz, S.E.; Goel, V.; Williams, J.I. Can the health utilities index measure change? Med. Care 2001, 39, 562–574. [Google Scholar] [CrossRef]
- Dolan, P.; Kahneman, D. Interpretations of utility and their implications for the valuation of health. Econ. J. 2008, 118, 215–234. [Google Scholar] [CrossRef]
- Facey, K.; Boivin, A.; Gracia, J.; Hansen, H.P.; Scalzo, A.L.; Mossman, J.; Single, A. Patients’ perspectives in health technology assessment: A route to robust evidence and fair deliberation. Int. J. Technol. Assess. Health Care 2010, 26, 334–340. [Google Scholar] [CrossRef]
- Karimi, M.; Brazier, J.; Paisley, S. How do individuals value health states? A qualitative investigation. Soc. Sci. Med. 2017, 172, 80–88. [Google Scholar] [CrossRef]
- MacKillop, E.; Sheard, S. Quantifying life: Understanding the history of Quality-Adjusted Life-Years (QALYs). Soc. Sci. Med. 2018, 211, 359–366. [Google Scholar] [CrossRef]
- Lipman, S.A.; Brouwer, W.B.; Attema, A.E. The corrective approach: Policy implications of recent developments in QALY measurement based on prospect theory. Value Health 2019, 22, 816–821. [Google Scholar] [CrossRef]
- Lipman, S.A.; Brouwer, W.B.; Attema, A.E. QALYs without bias? Nonparametric correction of time trade-off and standard gamble weights based on prospect theory. Health Econ. 2019, 28, 843–854. [Google Scholar] [CrossRef] [PubMed]
- Bernoulli, D. Exposition of a New Theory on the Measurement of Risk. Econometrica 1954, 22, 23–36. [Google Scholar] [CrossRef]
- Patrick, D.L.; Starks, H.E.; Cain, K.C.; Uhlmann, R.F.; Pearlman, R.A. Measuring preferences for health states worse than death. Med. Decis. Mak. 1994, 14, 9–18. [Google Scholar] [CrossRef]
- Robinson, A.; Spencer, A. Exploring challenges to TTO utilities: Valuing states worse than dead. Health Econ. 2006, 15, 393–402. [Google Scholar] [CrossRef] [PubMed]
- Devlin, N.J.; Tsuchiya, A.; Buckingham, K.; Tilling, C. A uniform time trade off method for states better and worse than dead: Feasibility study of the ‘lead time’ approach. Health Econ. 2011, 20, 348–361. [Google Scholar] [CrossRef] [PubMed]
- Janssen, M.F.; Szende, A.; Cabases, J.; Ramos-Goñi, J.M.; Vilagut, G.; König, H.H. Population norms for the EQ-5D-3L: A cross-country analysis of population surveys for 20 countries. Eur. J. Health Econ. 2018, 20, 1–12. [Google Scholar] [CrossRef]
- Xie, F.; Pullenayegum, E.; Gaebel, K.; Bansback, N.; Bryan, S.; Ohinmaa, A.; Poissant, L.; Johnson, J.A. How different are composite and traditional TTO valuations of severe EQ-5D-5L states? Qual. Life Res. 2016, 25, 2101–2108. [Google Scholar] [CrossRef]
- Ramos-Goñi, J.M.; Pinto-Prades, J.L.; Oppe, M.; Cabasés, J.M.; Serrano-Aguilar, P.; Rivero-Arias, O. Valuation and modeling of EQ-5D-5L health states using a hybrid approach. Med. Care 2017, 55, 51–58. [Google Scholar] [CrossRef]
- Oppe, M.; Rand-Hendriksen, K.; Shah, K.; Ramos-Goñi, J.M.; Luo, N. EuroQol protocols for time trade-off valuation of health outcomes. Pharmacoeconomics 2016, 34, 993–1004. [Google Scholar] [CrossRef]
- Busschbach, J.J.; McDonnell, J.; Essink-Bot, M.L.; van Hout, B.A. Estimating parametric relationships between health description and health valuation with an application to the EuroQol EQ-5D. J. Health Econ. 1999, 18, 551–571. [Google Scholar] [CrossRef]
- Dolan, P.; Stalmeier, P.F. The validity of time trade-off values in calculating QALYs: Constant proportional time trade-off versus the proportional heuristic. J. Health Econ. 2003, 22, 445–458. [Google Scholar] [CrossRef]
- Rowen, J.E.B.D.; Lloyd, A.; Karimi, M. Future directions in valuing benefits for estimating QALYs: Is time up for the EQ-5D? Value Health 2019, 22, 62–68. [Google Scholar]
- Dolan, P.; Olsen, J.A.; Menzel, P.; Richardson, J. An inquiry into the different perspectives that can be used when eliciting preferences in health. Health Econ. 2003, 12, 545–551. [Google Scholar] [CrossRef] [PubMed]
- Janssen, B.M.; Oppe, M.; Versteegh, M.M.; Stolk, E.A. Introducing the composite time trade-off: A test of feasibility and face validity. Eur. J. Health Econ. 2013, 14, 5–13. [Google Scholar] [CrossRef]
- Lamers, L.M. The transformation of utilities for health states worse than death: Consequences for the estimation of EQ-5D value sets. Med Care 2007, 45, 238–244. [Google Scholar] [CrossRef]
- Craig, B.M.; Rand, K.; Bailey, H.; Stalmeier, P.F. Quality-Adjusted Life-Years without Constant Proportionality. Value Health 2018, 21, 1124–1131. [Google Scholar] [CrossRef]
- von Neumann, J.; Morgenstern, O. Theory of Games and Economic Behavior, 2nd ed.; Princeton University Press: Princeton, NJ, USA, 1947. [Google Scholar]
- World Health Organization (WHO). Health Definition. In Proceedings of the International Health Conference, New York, NY, USA, 19 June–22 July 1946; pp. 19–22. [Google Scholar]
- Kahneman, D.; Tversky, A. Prospect Theory: An Analysis of Decision under Risk. Econometrica 1979, 47, 263–291. [Google Scholar] [CrossRef]
- Dolan, J.G.; Isselhardt, B.J.; Cappuccio, J.D. The analytic hierarchy process in medical decision making: A tutorial. Med Decis. Mak. 1989, 9, 40–50. [Google Scholar] [CrossRef]
- Dolan, J.G. Are patients capable of using the analytic hierarchy process and willing to use it to help make clinical decisions? Med Decis. Mak. 1995, 15, 76–80. [Google Scholar] [CrossRef]
- Danner, M.; Hummel, J.M.; Volz, F.; van Manen, J.G.; Wiegard, B.; Dintsios, C.M.; Bastian, H.; Gerber, A.; IJzerman, M.J. Integrating patients’ views into health technology assessment: Analytic hierarchy process (AHP) as a method to elicit patient preferences. Int. J. Technol. Assess. Health Care 2011, 27, 369–375. [Google Scholar] [CrossRef]
- Glaize, A.; Duenas, A.; di Martinelly, C.; Fagnot, I. Healthcare decision-making applications using multicriteria decision analysis: A scoping review. J. Multi-Criteria Decis. Anal. 2019, 26, 62–83. [Google Scholar] [CrossRef]
- Janssen, I.M.; Gerhardus, A.; Schröer-Günther, M.A.; Scheibler, F. A descriptive review on methods to prioritize outcomes in a health care context. Health Expect. 2015, 18, 1873–1893. [Google Scholar] [CrossRef] [PubMed]
- Oliveira, M.D.; Mataloto, I.; Kanavos, P. Multi-criteria decision analysis for health technology assessment: Addressing methodological challenges to improve the state of the art. Eur. J. Health Econ. 2019, 20, 891–918. [Google Scholar] [CrossRef] [PubMed]
- Dyer, J.S. Maut—Multiattribute Utility Theory. In Multiple Criteria Decision Analysis: State of the Art Surveys; Springer: New York, NY, USA, 2005; pp. 265–292. [Google Scholar]
- von Winterfeldt, D.; Edwards, W. Decision Analysis and Behavioral Research; Cambridge University Press: Cambridge, UK, 1986. [Google Scholar]
- Saaty, T.L. A scaling method for priorities in hierarchical structures. J. Math. Psychol. 1977, 15, 234–281. [Google Scholar] [CrossRef]
- Saaty, T.L. How to make a decision: The analytic hierarchy process. Eur. J. Oper. Res. 1990, 40, 9–26. [Google Scholar] [CrossRef]
- Costa, C.A.B.; Corte, J.; Vansnick, J. On the mathematical foundation of MACBETH. In Multiple Criteria Decision Analysis: State of the Art Surveys; Greco, S., Ehrgott, M., Figueira, J.R., Eds.; Springer: New York, NY, USA, 2005; pp. 421–463. [Google Scholar]
- Hwang, C.L.; Yoon, K. Methods for Multiple Attribute Decision Making; Cap 3, Multiple Attribute Decision Making; Springer: Berlin/Heidelberg, Germany, 1981. [Google Scholar]
- Roy, B.; Słowiński, R. Questions guiding the choice of a multicriteria decision aiding method. EURO J. Decis. Process. 2013, 1, 69–97. [Google Scholar] [CrossRef]
- Németh, B.; Molnár, A.; Bozóki, S.; Wijaya, K.; Inotai, A.; Campbell, J.D.; Kaló, Z. Comparison of weighting methods used in multicriteria decision analysis frameworks in healthcare with focus on low-and middle-income countries. J. Comp. Eff. Res. 2019, 8, 195–204. [Google Scholar] [CrossRef]
- Gutknecht, M.; Schaarschmidt, M.L.; Danner, M.; Otten, M.; Augustin, M. How to weight patient-relevant treatment goals for assessing treatment benefit in psoriasis: Preference elicitation methods vs. rating scales. Arch. Dermatol. Res. 2018, 310, 567–577. [Google Scholar] [CrossRef]
- Garau, M.; Hampson, G.; Devlin, N.; Mazzanti, N.A.; Profico, A. Applying a multicriteria decision analysis (MCDA) approach to elicit Stakeholders’ preferences in Italy: The case of Obinutuzumab for rituximab-refractory indolent non-Hodgkin lymphoma (iNHL). PharmacoEconomics-Open 2018, 2, 153–163. [Google Scholar] [CrossRef]
- Kamiński, B.; Jakubczyk, M. Comparing the crisp and fuzzy approaches to modelling preferences towards health states. Mult. Criteria Decis. Mak. 2017, 12, 75–89. [Google Scholar] [CrossRef]
- Gerlinger, C.; Bamber, L.; Leverkus, F.; Schwenke, C.; Haberland, C.; Schmidt, G.; Endrikat, J. Comparing the EQ-5D-5L utility index based on value sets of different countries: Impact on the interpretation of clinical study results. BMC Res. Note 2019, 12, 18–23. [Google Scholar] [CrossRef] [PubMed]
- Tavakol, M.; Dennick, R. Making sense of Cronbach’s alpha. Int. J. Med Educ. Editor. 2011, 2, 53–55. [Google Scholar] [CrossRef] [PubMed]
- Bland, J.M.; Altman, D.G. Statistics notes: Cronbach’s alpha. BMJ 1997, 314, 314. [Google Scholar] [CrossRef] [PubMed]
- Haddad, M.; Sanders, D. Selection of discrete multiple criteria decision making methods in the presence of risk and uncertainty. Oper. Res. Perspect. 2018, 5, 357–370. [Google Scholar] [CrossRef]
- Mikhailov, L. A fuzzy programming method for deriving priorities in the analytic hierarchy process. J. Oper. Res. Soc. 2000, 51, 341–349. [Google Scholar] [CrossRef]
- Krejčí, J.; Stoklasa, J. Aggregation in the analytic hierarchy process: Why weighted geometric mean should be used instead of weighted arithmetic mean. Expert Syst. Appl. 2018, 114, 97–106. [Google Scholar] [CrossRef]
- Dempster, A.P. A generalization of Bayesian inference. J. R. Stat. Soc. Ser. B (Methodol.) 1968, 30, 205–232. [Google Scholar] [CrossRef]
- Shafer, G. Perspectives on the theory and practice of belief functions. Int. J. Approx. Reason. 1990, 4, 323–362. [Google Scholar] [CrossRef]
- Dutta, P. Modeling of variability and uncertainty in human health risk assessment. MethodsX 2017, 4, 76–85. [Google Scholar] [CrossRef]
- Deng, Y. D numbers: Theory and applications. J. Inf. Comput. Sci. 2012, 9, 2421–2428. [Google Scholar]
- Deng, X.; Hu, Y.; Deng, Y.; Mahadevan, S. Supplier selection using AHP methodology extended by D numbers. Expert Syst. Appl. 2014, 41, 156–167. [Google Scholar] [CrossRef]
- Herrera-Viedma, E.; Herrera, F.; Chiclana, F.; Luque, M. Some issues on consistency of fuzzy preference relations. Eur. J. Oper. Res. 2004, 154, 98–109. [Google Scholar] [CrossRef]
- Zadeh, L.A. Fuzzy sets. Inf. Control 1965, 8, 338–353. [Google Scholar] [CrossRef]
- Bellman, R.E.; Zadeh, L.A. Decision-making in a fuzzy environment. Manag. Sci. 1970, 17, B141. [Google Scholar] [CrossRef]
- van Laarhoven, P.J.; Pedrycz, W. A fuzzy extension of Saaty’s priority theory. Fuzzy Sets Syst. 1983, 11, 229–241. [Google Scholar] [CrossRef]
- Yager, R.R. A Procedure for Ordering Fuzzy Subsets of the Unit Interval. Inf. Sci. 1981, 24, 143–161. [Google Scholar] [CrossRef]
- Zheng, G.; Zhu, N.; Tian, Z.; Chen, Y.; Sun, B. Application of a trapezoidal fuzzy AHP method for work safety evaluation and early warning rating of hot and humid environments. Saf. Sci. 2012, 50, 228–239. [Google Scholar] [CrossRef]
- Yoon, K.P.; Kim, W.K. The behavioral TOPSIS. Expert Syst. Appl. 2017, 89, 266–272. [Google Scholar] [CrossRef]
- Golany, B.; Kress, M. A multicriteria evaluation of methods for obtaining weights from ratio-scale matrices. Eur. J. Oper. Res. 1993, 69, 210–220. [Google Scholar] [CrossRef]
- Lal, A.; Mohebi, M.; Sweeney, R.; Moodie, M.; Peeters, A.; Carter, R. R Equity weights for socioeconomic position: Two methods—survey of stated preferences and epidemiological data. Value Health 2019, 22, 247–253. [Google Scholar] [CrossRef]
- Sen, A. Why health equity? Health Econ. 2002, 11, 659–666. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Scale | Numerical Rating | Reciprocal (Decimal) | Fuzzy Trapezoidal | Fuzzy Reciprocal (Inverse) | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Equal importance | 1 | 1 (1000) | (1, 1, 1, 1) | (1, 1, 1, 1) | ||||||
| Moderate importance | 3 | 1/3 (0.33) | (2, 5/2, 7/2, 4) | (1/4, 2/7, 2/5, 1/2) | ||||||
| Strong importance | 5 | 1/5 (0.20) | (4, 9/2,11/2,6) | (1/6, 2/11, 2/9,1/4) | ||||||
| Very strong importance | 7 | 1/7 (0.14) | (6, 18/2, 15/2, 8) | (1/8, 2/15, 2/13, 1/6) | ||||||
| Extreme importance | 9 | 1/9 (0.11) | (8,17/2, 9, 9) | (1/9, 1/9, 2/17, 1/8) | ||||||
| Intermediate values between two adjacent judgments | 2 | 1/2 (0.50) | ||||||||
| 4 | 1/4 (0.25) | |||||||||
| 6 | 1/6 (0.17) | |||||||||
| 8 | 1/8 (0.13) | |||||||||
| Size matrix | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 |
| Random consistency (RC) | 0 | 0 | 0.58 | 0.9 | 1.12 | 1.24 | 1.32 | 1.41 | 1.45 | 1.49 |
| Characteristics | n (%) | |
|---|---|---|
| Sex | Female | 132 (43.5) |
| Male | 169 (56.15) | |
| Age | 18–21 | 76 (25.25) |
| 22–47 | 77 (25.58) | |
| 48–66 | 79 (26.25) | |
| 67–90 | 69 (22.92) | |
| Education levels | Primary | 29 (9.63) |
| Secondary | 38 (12.62) | |
| Bachelor degree | 50 (16.61) | |
| Bachelor student | 105 (34.88) | |
| Professional technician | 11 (3.65) | |
| Technologist | 17 (5.65) | |
| Master degree | 39 (12.96) | |
| Ph.D. | 12 (3.99) | |
| Wage | <1 minimum wage | 78 (25.91) |
| 1 < minimum wage < 2 | 104 (34.55) | |
| >3 minimum wage | 119 (39.53) | |
| Social-economic status | 1 (lowest) | 7 (2.33) |
| 2 | 51 (16.94) | |
| 3 | 113 (37.54) | |
| 4 | 63 (20.93) | |
| 5 | 51 (16.94) | |
| 6 (highest) | 16 (5.32) | |
| Health program | Yes | 93 (30.90) |
| No | 206 (68.44) | |
| Mobility | No problems | 246 (81.73) |
| Slight problems | 32 (10.63) | |
| Moderate problems | 18 (5.98) | |
| Severe problems | 5 (1.66) | |
| Self-care | No problems | 298 (99) |
| Slight problems | 3 (1) | |
| Usual activities | No problems | 253 (84.05) |
| Slight problems | 39 (12.96) | |
| Moderate problems | 8 (2.66) | |
| Severe problems | 1 (0.33) | |
| Pain/discomfort | No pain or discomfort | 172 (57.14) |
| Slight pain or discomfort | 78 (25.91) | |
| Moderate pain or discomfort | 45 (14.95) | |
| Severe pain or discomfort | 5 (1.66) | |
| Extreme pain or discomfort | 1 (0.33) | |
| Anxiety/depression | No anxiety or depression | 183 (60.80) |
| Slight anxiety or depression | 74 (24.58) | |
| Moderately anxiety or depression | 38 (12.62) | |
| Severely anxiety or depression | 4 (1.33) | |
| Extremely anxiety or depression | 2 (0.66) | |
| Models | Dimensions | TOPSIS | ||||||
|---|---|---|---|---|---|---|---|---|
| AHP | MO | SC | UA | PD | AP | a | Ideal (S+) | Anti-ideal (S−) |
| MO | 1 | 1.5 | 1.2 | 1.2 | 1.6 | 0.25 | 0.01 | 0.04 |
| SC | 0.7 | 1 | 1.2 | 0.8 | 1.1 | 0.19 | 0.01 | 0.03 |
| UA | 0.8 | 0.9 | 1 | 1 | 1.3 | 0.19 | 0.01 | 0.03 |
| PD | 0.8 | 1.2 | 1 | 1 | 1.3 | 0.21 | 0.01 | 0.02 |
| AP | 0.6 | 0.9 | 0.8 | 0.8 | 1 | 0.16 | 0.01 | 0.03 |
| D-AHP | MO | SC | AU | PD | AP | b | (S+) | (S−) |
| MO | 0.5 | 0.6 | 0.6 | 0.6 | 0.6 | 0.39 | 0.01 | 0.06 |
| SC | 0.5 | 0.5 | 0.5 | 0.5 | 0.6 | 0.27 | 0.01 | 0.03 |
| UA | 0.4 | 0.5 | 0.5 | 0.5 | 0.5 | 0.22 | 0 | 0.04 |
| PD | 0.5 | 0.5 | 0.5 | 0.5 | 0.5 | 0.12 | 0.01 | 0.03 |
| AP | 0.4 | 0.4 | 0.4 | 0.4 | 0.5 | 0 | 0 | 0 |
| F-AHP | MO | SC | UA | PD | AD | c | (S+) | (S−) |
| MO | 1 | 1.4 | 1.1 | 1 | 1.3 | 0.23 | 0.01 | 0.04 |
| SC | 0.8 | 1 | 1.1 | 0.9 | 1 | 0.19 | 0.01 | 0.03 |
| UA | 0.9 | 0.9 | 1 | 0.9 | 1 | 0.18 | 0.01 | 0.03 |
| PD | 1 | 1.1 | 1.2 | 1 | 1.2 | 0.21 | 0.01 | 0.02 |
| AP | 0.8 | 0.1 | 0.9 | 0.9 | 1 | 0.18 | 0.01 | 0.03 |
| Health Status | n | VAS | AHP-TOPSIS | D-AHP-TOPSIS | F-AHP-TOPSIS | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean | Min | Max | SD | Mean | Min | Max | SD | Mean | Min | Max | SD | Mean | Min | Max | SD | ||
| 11111 | 102 | 0.88 | 0.5 | 1.00 | 0.12 | 0.87 | 0.82 | 0.96 | 0.02 | 0.89 | 0.85 | 0.90 | 0.01 | 0.86 | 0.83 | 0.91 | 0.02 |
| 11121 | 35 | 0.86 | 0.5 | 1.00 | 0.11 | 0.85 | 0.72 | 0.91 | 0.04 | 0.85 | 0.67 | 0.90 | 0.05 | 0.86 | 0.84 | 0.91 | 0.02 |
| 11112 | 33 | 0.84 | 0.5 | 1.00 | 0.12 | 0.84 | 0.71 | 0.90 | 0.05 | 0.86 | 0.69 | 0.90 | 0.04 | 0.87 | 0.83 | 0.91 | 0.02 |
| 11122 | 15 | 0.86 | 0.6 | 0.95 | 0.11 | 0.82 | 0.76 | 0.91 | 0.04 | 0.84 | 0.69 | 0.89 | 0.05 | 0.87 | 0.84 | 0.91 | 0.02 |
| 11113 | 12 | 0.87 | 0.7 | 1.00 | 0.10 | 0.85 | 0.77 | 0.92 | 0.04 | 0.86 | 0.78 | 0.89 | 0.03 | 0.86 | 0.83 | 0.90 | 0.02 |
| 11131 | 9 | 0.84 | 0.7 | 0.90 | 0.07 | 0.81 | 0.68 | 0.88 | 0.06 | 0.80 | 0.72 | 0.89 | 0.05 | 0.87 | 0.83 | 0.90 | 0.03 |
| 21121 | 9 | 0.81 | 0.3 | 0.95 | 0.22 | 0.83 | 0.76 | 0.87 | 0.04 | 0.83 | 0.79 | 0.87 | 0.03 | 0.86 | 0.83 | 0.89 | 0.03 |
| 11222 | 5 | 0.88 | 0.7 | 1.00 | 0.13 | 0.84 | 0.78 | 0.90 | 0.05 | 0.84 | 0.82 | 0.87 | 0.02 | 0.86 | 0.84 | 0.88 | 0.02 |
| 11123 | 4 | 0.75 | 0.5 | 1.00 | 0.21 | 0.84 | 0.80 | 0.88 | 0.03 | 0.85 | 0.79 | 0.89 | 0.04 | 0.87 | 0.84 | 0.89 | 0.02 |
| 11211 | 4 | 0.80 | 0.55 | 1.00 | 0.23 | 0.87 | 0.81 | 0.94 | 0.06 | 0.87 | 0.84 | 0.89 | 0.02 | 0.87 | 0.85 | 0.88 | 0.01 |
| 11212 | 4 | 0.93 | 0.9 | 1.00 | 0.05 | 0.82 | 0.74 | 0.89 | 0.07 | 0.84 | 0.79 | 0.88 | 0.04 | 0.85 | 0.84 | 0.86 | 0.01 |
| 21232 | 4 | 0.84 | 0.8 | 0.90 | 0.05 | 0.76 | 0.71 | 0.81 | 0.04 | 0.76 | 0.72 | 0.81 | 0.05 | 0.82 | 0.80 | 0.84 | 0.02 |
| 31131 | 4 | 0.74 | 0.65 | 0.80 | 0.08 | 0.71 | 0.62 | 0.79 | 0.09 | 0.67 | 0.56 | 0.73 | 0.08 | 0.77 | 0.74 | 0.90 | 0.03 |
| 11132 | 3 | 0.70 | 0.5 | 0.90 | 0.20 | 0.81 | 0.71 | 0.88 | 0.09 | 0.81 | 0.76 | 0.87 | 0.05 | 0.74 | 0.72 | 0.76 | 0.02 |
| 42352 | 1 | 0.63 | 0.61 | 0.62 | 0.73 | ||||||||||||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vásquez, J.; Botero, S. Hybrid Methodology to Improve Health Status Utility Values Derivation Using EQ-5D-5L and Advanced Multi-Criteria Techniques. Int. J. Environ. Res. Public Health 2020, 17, 1423. https://doi.org/10.3390/ijerph17041423
Vásquez J, Botero S. Hybrid Methodology to Improve Health Status Utility Values Derivation Using EQ-5D-5L and Advanced Multi-Criteria Techniques. International Journal of Environmental Research and Public Health. 2020; 17(4):1423. https://doi.org/10.3390/ijerph17041423
Chicago/Turabian StyleVásquez, Johanna, and Sergio Botero. 2020. "Hybrid Methodology to Improve Health Status Utility Values Derivation Using EQ-5D-5L and Advanced Multi-Criteria Techniques" International Journal of Environmental Research and Public Health 17, no. 4: 1423. https://doi.org/10.3390/ijerph17041423
APA StyleVásquez, J., & Botero, S. (2020). Hybrid Methodology to Improve Health Status Utility Values Derivation Using EQ-5D-5L and Advanced Multi-Criteria Techniques. International Journal of Environmental Research and Public Health, 17(4), 1423. https://doi.org/10.3390/ijerph17041423