Shift Work and Prostate Cancer: An Updated Systematic Review and Meta-Analysis

 , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Selection Criteria
2.2. Search Strategy and Study Selection
2.3. Data Extraction and Quality Evaluation
2.4. Data Synthesis and Analysis
3. Results
3.1. Study Selection
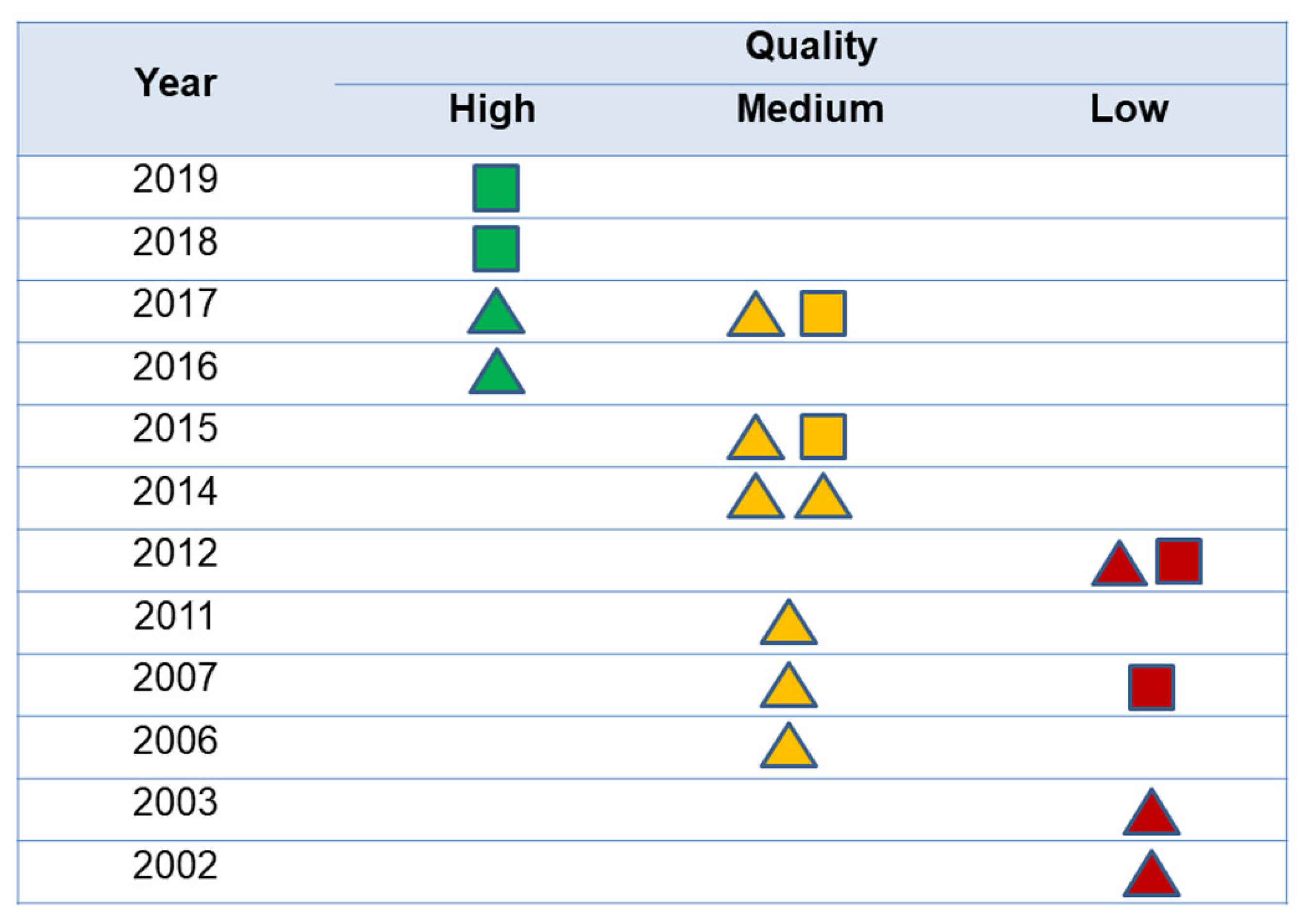
3.2. Methodological Evaluation of the Studies: Identification of Systematic Bias
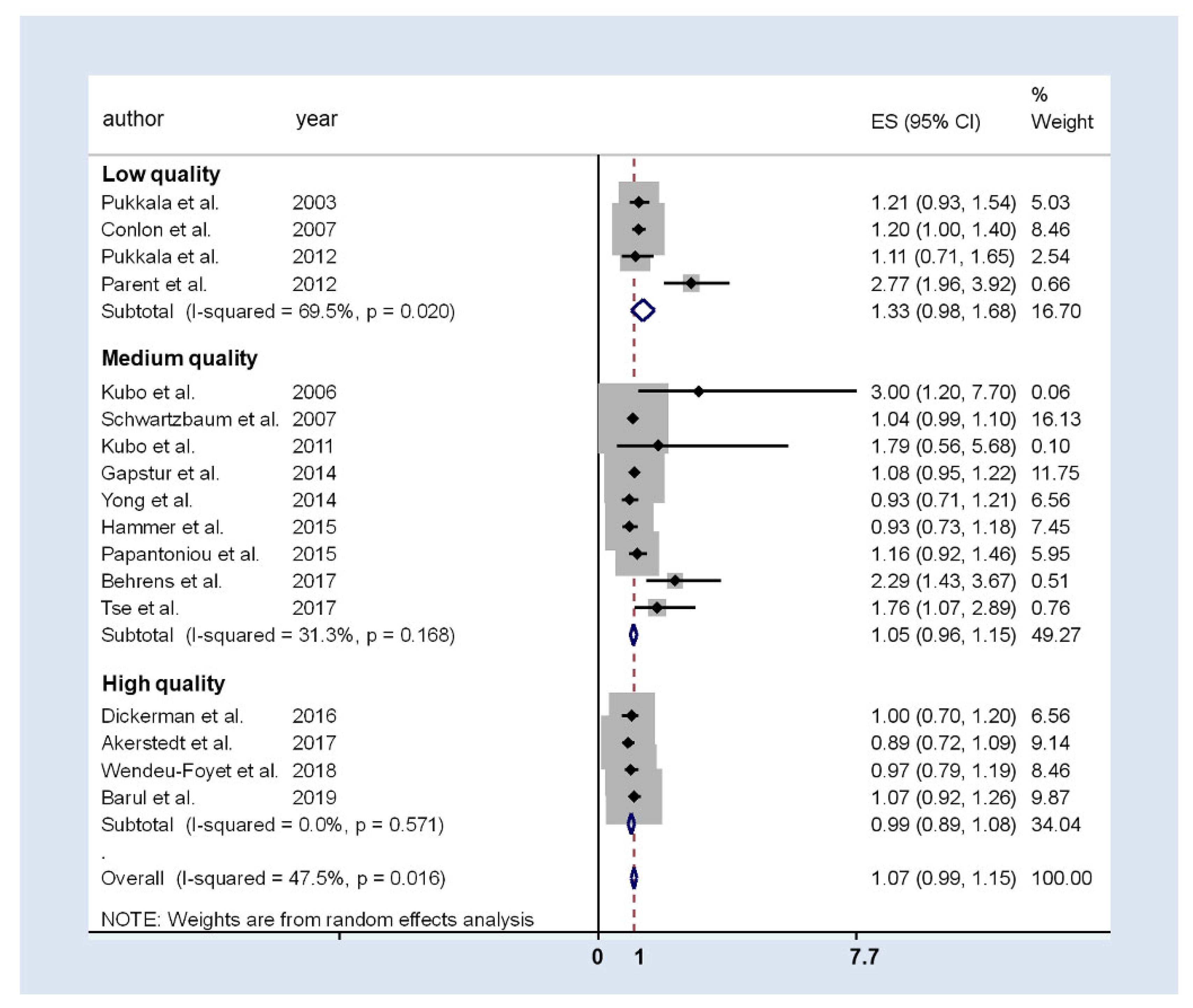
3.3. Association between Shift Work and Prostate Cancer: Meta-Analysis Results
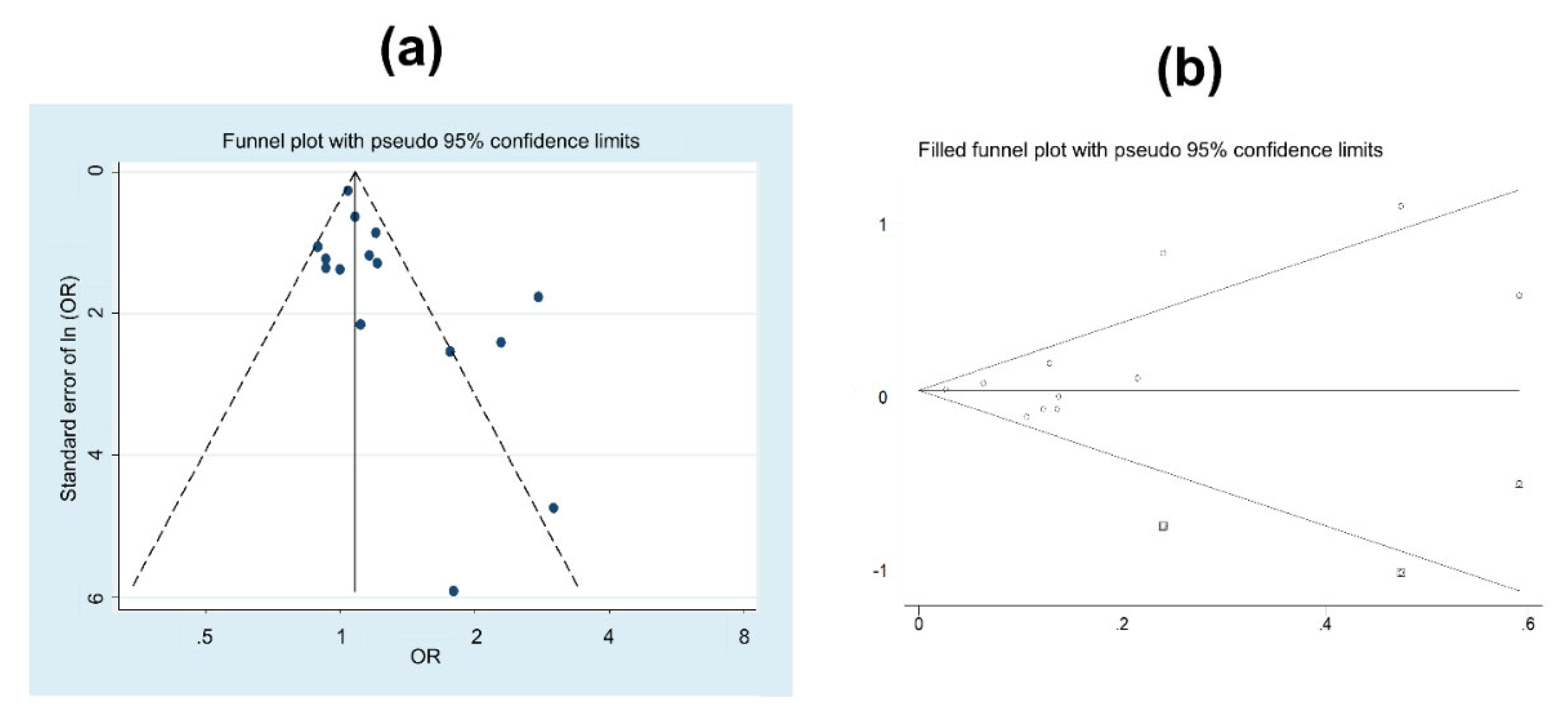
3.4. Publication Bias
4. Discussion
4.1. Methodology of the Studies
4.2. Discussion of the Results
Design
Methodological Quality of Studies
Exposure Variables
Stratified Analysis
Publication Bias
4.3. Strengths and limitations of the meta-analysis
4.4. Consequences and Applicability of the Results
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- International Agency for Research on Cancer (IARC). Global Cancer Observatory; 2018; Available online: https://gco.iarc.fr/ (accessed on 10 September 2019).
- Bray, F.; Ren, J.S.; Masuyer, E.; Ferlay, J. Global estimates of cancer prevalence for 27 sites in the adult population in 2008. Int. J. Cancer 2013, 132, 1133–1145. [Google Scholar] [CrossRef] [PubMed]
- International Agency for Research on Cancer/WHO. List of Classifications by Cancer Sites with Sufficient or Limited Evidence in Humans; 2018; Available online: https://monographs.iarc.fr/wp-content/uploads/2018/07/Table4.pdf (accessed on 10 July 2019).
- Mancuso, N.; Gayther, S.; Gusev, A.; Zheng, W.; Penney, K.L.; Kote-Jarai, Z.; Eeles, R.; Freedman, M.; Haiman, C.; Pasaniuc, B. Large-scale transcriptome-wide association study identifies new prostate cancer risk regions. Nat. Commun. 2018, 9, 4079. [Google Scholar] [CrossRef] [PubMed]
- Bostwick, D.G.; Burke, H.B.; Djakiew, D.; Euling, S.; Ho, H.; Landolph, J.; Morrison, H.; Sonawane, B.; Shifflett, T.; Waters, D.J.; et al. Human prostate cancer risk factors. Cancer 2004, 101, 2371–2490. [Google Scholar] [CrossRef]
- Cooperberg, M.R.; Chan, J.M. Epidemiology of prostate cancer. World J. Urol. 2017, 35, 849. [Google Scholar] [CrossRef] [PubMed]
- Jemal, A.; Siegel, R.; Ward, E.; Hao, Y.; Xu, J.; Thun, M.J. Cancer statistics, 2009. CA Cancer J. Clin. 2009, 59, 225–249. [Google Scholar] [CrossRef]
- Center, M.M.; Jemal, A.; Lortet-Tieulent, J.; Ward, E.; Ferlay, J.; Brawley, O.; Bray, F. International variation in prostate cancer incidence and mortality rates. Eur. Urol. 2012, 61, 1079–1092. [Google Scholar] [CrossRef]
- Chen, M.; Luo, Y.; Yang, S.; Xu, L.; Li, N.; Li, H.; Qu, S. Association of diabetes mellitus with prostate cancer grade and prostate-specific antigen in Chinese biopsy population. Diabetes Res. Clin. Pract. 2018, 141, 80–87. [Google Scholar] [CrossRef]
- Dagnelie, P.C.; Schuurman, A.G.; Goldbohm, R.A.; Van Den Brandt, P.A. Diet, anthropometric measures and prostate cancer risk: A review of prospective cohort and intervention studies. BJU Int. 2004, 93, 1139–1150. [Google Scholar] [CrossRef]
- Markozannes, G.; Tzoulaki, I.; Karli, D.; Evangelou, E.; Ntzani, E.; Gunter, M.J.; Norat, T.; Ioannidis, J.P.; Tsilidis, K.K. Diet, body size, physical activity and risk of prostate cancer: An umbrella review of the evidence. Eur. J. Cancer 2016, 69, 61–69. [Google Scholar] [CrossRef]
- Wilson, K.M.; Giovannucci, E.L.; Mucci, L.A. Lifestyle and dietary factors in the prevention of lethal prostate cancer. Asian J. Androl. 2012, 14, 365–374. [Google Scholar] [CrossRef]
- Straif, K.; Baan, R.; Grosse, Y.; Secretan, B.; El Ghissassi, F.; Bouvard, V.; Altieri, A.; Benbrahim-Tallaa, L.; Cogliano, V. Carcinogenicity of shift-work, painting, and fire-fighting. Lancet Oncol. 2007, 8, 1065–1066. [Google Scholar] [CrossRef]
- Krstev, S.; Knutsson, A. Occupational risk factors for prostate cancer: A meta-analysis. J. Cancer Prev. 2019, 24, 91–111. [Google Scholar] [CrossRef] [PubMed]
- Loomis, D.; Guha, N.; Hall, A.L.; Straif, K. Identifying occupational carcinogens: An update from the IARC Monographs. Occup. Environ. Med. 2018, 75, 593–603. [Google Scholar] [CrossRef] [PubMed]
- Aumayr-Pintar, C.; Boehmer, S.; Bremermann, M. Developments in Working Life in Europe: EurWORK Annual Review 2014 (EUROFOUND). 2015. Available online: https://www.eurofound.europa.eu/sites/default/files/ef_comparative_analytical_report/field_ef_documents/ef1551en_1.pdf (accessed on 10 September 2019).
- Nappo, N. Is there an association between working conditions and health? An analysis of the Sixth European Working Conditions Survey data. PLoS ONE 2019, 14, e0211294. [Google Scholar] [CrossRef] [PubMed]
- Ward, E.M.; Germolec, D.; Kogevinas, M.; McCormick, D.; Vermeulen, R.; Anisimov, V.N.; Aronson, K.J.; Bhatti, P.; Cocco, P.; Costa, G.; et al. Carcinogenicity of night shift work. Lancet Oncol. 2019, 20, 1058–1059. [Google Scholar] [CrossRef]
- Papantoniou, K.; Castano-Vinyals, G.; Espinosa, A.; Aragonés, N.; Pérez-Gómez, B.; Adanaz, E.; Altzibar, J.M.; Sanchez, V.M.; Gómez-Acebo, I.; Llorca, J.; et al. Breast cancer risk and night shift work in a case-control study in a Spanish population. Eur. J. Epidemiol. 2016, 31, 867–878. [Google Scholar] [CrossRef] [PubMed]
- Papantoniou, K.; Castano-Vinyals, G.; Espinosa, A.; Turner, M.C.; Alonso-Aguado, M.H.; Martin, V.; Aragonés, N.; Pérez-Gómez, B.; Pozo, B.M.; Gómez-Acebo, I.; et al. Shift work and colorectal cancer risk in the MCC-Spain case-control study. Scand. J. Work Environ. Health 2017, 43, 250–259. [Google Scholar] [CrossRef]
- Schernhammer, E.S.; Laden, F.; Speizer, F.E.; Willett, W.C.; Hunter, D.J.; Kawachi, I.; Colditz, G.A. Rotating night shifts and risk of breast cancer in women participating in the nurses’ health study. J. Natl. Cancer Inst. 2001, 93, 1563–1568. [Google Scholar] [CrossRef]
- Blask, D.E. Melatonin, sleep disturbance and cancer risk. Sleep Med. Rev. 2009, 13, 257–264. [Google Scholar] [CrossRef]
- Haus, E.L.; Smolensky, M.H. Shift work and cancer risk: Potential mechanistic roles of circadian disruption, light at night, and sleep deprivation. Sleep Med. Rev. 2013, 17, 273–284. [Google Scholar] [CrossRef]
- Lamia, K.A. Ticking time bombs: Connections between circadian clocks and cancer. F1000Research 2017, 6, 1910. [Google Scholar] [CrossRef] [PubMed]
- Parent, M.E.; El-Zein, M.; Rousseau, M.C.; Pintos, J.; Siemiatycki, J. Night work and the risk of cancer among men. Am. J. Epidemiol. 2012, 176, 751–759. [Google Scholar] [CrossRef] [PubMed]
- Yong, M.; Blettner, M.; Emrich, K.; Nasterlack, M.; Oberlinner, C.; Hammer, G.P. A retrospective cohort study of shift work and risk of incident cancer among German male chemical workers. Scand. J. Work Environ. Health 2014, 40, 502–510. [Google Scholar] [CrossRef] [PubMed]
- Du, H.B.; Bin, K.Y.; Liu, W.H.; Yang, F.S. Shift work, night work, and the risk of prostate cancer: A meta-analysis based on 9 cohort studies. Medicine 2017, 96, e8537. [Google Scholar] [CrossRef]
- Gan, Y.; Li, L.; Zhang, L.; Yan, S.; Gao, C.; Hu, S.; Qiao, Y.; Tang, S.; Wang, C.; Lu, Z. Association between shift work and risk of prostate cancer: A systematic review and meta-analysis of observational studies. Carcinogenesis 2018, 39, 87–97. [Google Scholar] [CrossRef]
- Rao, D.; Yu, H.; Bai, Y.; Zheng, X.; Xie, L. Does night-shift work increase the risk of prostate cancer? A systematic review and meta-analysis. Onco-Targets Ther. 2015, 8, 817–826. [Google Scholar]
- Liu, W.; Zhou, Z.; Dong, D.; Sun, L.; Zhang, G. Sex Differences in the Association between Night Shift Work and the Risk of Cancers: A Meta-Analysis of 57 Articles. Dis. Markers 2018, 2018, 7925219. [Google Scholar] [CrossRef]
- Mancio, J.; Leal, C.; Ferreira, M.; Norton, P.; Lunet, N. Does the association of prostate cancer with night-shift work differ according to rotating vs. fixed schedule? A systematic review and meta-analysis. Prostate Cancer Prostatic Dis. 2018, 21, 337–344. [Google Scholar] [CrossRef]
- Wendeu-Foyet, M.G.; Menegaux, F. Circadian Disruption and Prostate Cancer Risk: An Updated Review of Epidemiological Evidences. Cancer Epidemiol. Biomark. Prev. 2017, 26, 985–991. [Google Scholar] [CrossRef]
- Salamanca-Fernández, E.; Rodríguez-Barranco, M.; Guevara, M.; Ardanaz, E.; Olry de Labry Lima, A.; Sánchez, M.J. Night-shift work and breast and prostate cancer risk: Updating the evidence from epidemiological studies. An. Sist. Sanit. Navar. 2018, 41, 211–226. [Google Scholar]
- Murad, M.H.; Asi, N.; Alsawas, M.; Alahdab, F. New evidence pyramid. Evid. Based Med. 2017, 21, 125–127. [Google Scholar] [CrossRef] [PubMed]
- Akerstedt, T.; Narusyte, J.; Svedberg, P.; Kecklund, G.; Alexanderson, K. Night work and prostate cancer in men: A Swedish prospective cohort study. BMJ Open 2017, 7, e015751. [Google Scholar] [CrossRef] [PubMed]
- Behrens, T.; Rabstein, S.; Wichert, K.; Erbel, R.; Eisele, L.; Arendt, M.; Dragano, N.; Brüning, T.; Jöckel, K.H. Shift work and the incidence of prostate cancer: A 10-year follow-up of a German population-based cohort study. Scand. J. Work Environ. Health 2017, 43, 560–568. [Google Scholar] [CrossRef] [PubMed]
- Dickerman, B.A.; Markt, S.C.; Koskenvuo, M.; Hublin, C.; Pukkala, E.; Mucci, L.A.; Kaprio, J. Sleep disruption, chronotype, shift work, and prostate cancer risk and mortality: A 30-year prospective cohort study of Finnish twins. Cancer Causes Control 2016, 27, 1361–1370. [Google Scholar] [CrossRef]
- Tse, L.A.; Lee, P.M.Y.; Ho, W.M.; Lam, A.T.; Lee, M.K.; Ng, S.S.M.; He, Y.; Leung, K.S.; Hartle, J.C.; Hu, H.; et al. Bisphenol A and other environmental risk factors for prostate cancer in Hong Kong. Environ. Int. 2017, 107, 1–7. [Google Scholar] [CrossRef]
- Barul, C.; Richard, H.; Parent, M.E. Night-Shift Work and Risk of Prostate Cancer: Results from a Canadian Case-Control Study, the Prostate Cancer and Environment Study. Am. J. Epidemiol. 2019, 188, 1801–1811. [Google Scholar] [CrossRef]
- Wendeu-Foyet, M.G.; Bayon, V.; Cenee, S.; Tretarre, B.; Rebillard, X.; Cancel-Tassin, G.; Cussenot, O.; Lamy, P.J.; Faraut, B.; Ben Khedeher, S.; et al. Night work and prostate cancer risk: Results from the EPICAP Study. Occup. Environ. Med. 2018, 75, 573–581. [Google Scholar] [CrossRef]
- Erren, T.C.; Falaturi, P.; Morfeld, P.; Knauth, P.; Reiter, R.J.; Piekarski, C. Shift work and cancer: The evidence and the challenge. Dtsch. Arztebl. Int. 2010, 107, 657–662. [Google Scholar]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleiinen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. PLoS Med. 2009, 6, e1000100. [Google Scholar] [CrossRef]
- Wells, G.A.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses. 2013. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 10 July 2019).
- Cohen, J. A coefficient of agreement for nominal scales. Educ. Psychol. Meas. 1960, 20, 37–46. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [PubMed]
- Borenstein, M.; Hedges, L.V.; Higgins, J.P.; Rothstein, H.R. A basic introduction to fixed-effect and random-effects models for meta-analysis. Res. Synth. Methods 2010, 1, 97–111. [Google Scholar] [CrossRef] [PubMed]
- Egger, M.; Davey Smith, G.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [PubMed]
- Conlon, M.; Lightfoot, N.; Kreiger, N. Rotating shift work and risk of prostate cancer. Epidemiology 2007, 18, 182–183. [Google Scholar] [CrossRef] [PubMed]
- Papantoniou, K.; Castano-Vinyals, G.; Espinosa, A.; Aragonés, N.; Pérez-Gómez, B.; Burgos, J.; Gómez-Acebo, I.; Llorca, J.; Peiró, R.; Jiménez-Moleón, J.J.; et al. Night shift work, chronotype and prostate cancer risk in the MCC-Spain case-control study. Int. J. Cancer 2015, 137, 1147–1157. [Google Scholar] [CrossRef] [PubMed]
- Gapstur, S.M.; Diver, W.R.; Stevens, V.L.; Carter, B.D.; Teras, L.R.; Jacobs, E.J. Work schedule, sleep duration, insomnia, and risk of fatal prostate cancer. Am. J. Prev. Med. 2014, 46, S26–S33. [Google Scholar] [CrossRef]
- Hammer, G.P.; Emrich, K.; Nasterlack, M.; Blettner, M.; Yong, M. Shift Work and Prostate Cancer Incidence in Industrial Workers: A Historical Cohort Study in a German Chemical Company. Dtsch. Arztebl. Int. 2015, 112, 463–470. [Google Scholar]
- Kubo, T.; Ozasa, K.; Mikami, K.; Wakai, K.; Fujino, Y.; Watanabe, Y.; Miki, T.; Nakao, M.; Hayashi, K.; Suzuki, K.; et al. Prospective cohort study of the risk of prostate cancer among rotating-shift workers: Findings from the Japan collaborative cohort study. Am. J. Epidemiol. 2006, 164, 549–555. [Google Scholar] [CrossRef]
- Pukkala, E.; Aspholm, R.; Auvinen, A.; Eliasch, H.; Gundestrup, M.; Haldorsen, T.; Hammar, N.; Hrafnkelsson, J.; Kyyrönen, P.; Linnersjö, A.; et al. Incidence of cancer among Nordic airline pilots over five decades: Occupational cohort study. BMJ 2002, 325, 567. [Google Scholar] [CrossRef]
- Pukkala, E.; Aspholm, R.; Auvinen, A.; Eliasch, H.; Gundestrup, M.; Haldorsen, T.; Hammar, N.; Hrafnkelsson, J.; Kyyrönen, P.; Linnersjö, A.; et al. Cancer incidence among 10,211 airline pilots: A Nordic study. Aviat. Space Environ. Med. 2003, 74, 699–706. [Google Scholar]
- Pukkala, E.; Helminen, M.; Haldorsen, T.; Hammar, N.; Kojo, K.; Linnesjö, A. Cancer incidence among Nordic airline cabin crew. Int. J. Cancer 2012, 131, 2886–2897. [Google Scholar] [CrossRef] [PubMed]
- Schwartzbaum, J.; Ahlbom, A.; Feychting, M. Cohort study of cancer risk among male and female shift workers. Scand. J. Work Environ. Health 2007, 33, 336–343. [Google Scholar] [CrossRef] [PubMed]
- Kubo, T.; Oyama, I.; Nakamura, T.; Kunimoto, M.; Kadowaki, K.; Otomo, H.; Fujino, Y.; Fujimoto, N.; Matsumoto, T.; Matsuda, S. Industry-based retrospective cohort study of the risk of prostate cancer among rotating-shift workers. Int. J. Urol. 2011, 18, 206–211. [Google Scholar] [CrossRef]
- Ijaz, S.; Verbeek, J.; Seidler, A.; Lindbohm, M.L.; Ojajärvi, A.; Orsini, N.; Costa, G.; Neuvonen, K. Nigh-shift work and breast cancer—A systematic review and meta-analysis. Scand. J. Work Environ. Health 2013, 39, 431–447. [Google Scholar] [CrossRef] [PubMed]
- Ioannidis, J.P. Why most published research findings are false. PLoS Med. 2005, 2, e124. [Google Scholar] [CrossRef]
- Palma-Perez, S.; Delgado-Rodriguez, M. Practical considerations on detection of publication bias. Gac. Sanit. 2006, 20, 10–16. [Google Scholar]
- Geng, Q.; Zhang, Q.E.; Wang, F.; Zheng, W.; Ng, C.H.; Ungvari, G.S.; Wang, G.; Xiang, Y.T. Comparison of comorbid depression between irritable bowel syndrome and inflammatory bowel disease: A meta-analysis of comparative studies. J. Affect. Disord. 2018, 237, 37–46. [Google Scholar] [CrossRef]
- He, X.; Yang, K.; Wang, H.; Chen, X.; Wu, H.; Yao, L.; Ma, S. Expression and clinical significance of surviving in ovarian cancer: A meta-analysis. PLoS ONE 2018, 13, e0194463. [Google Scholar] [CrossRef]
- Cordina-Duverger, E.; Menegaux, F.; Popa, A.; Rabstein, S.; Harth, V.; Pesch, B.; Brüning, T.; Fritschi, L.; Glass, D.C.; Heyworth, J.S.; et al. Night shift work and breast cancer: A pooled analysis of population-based case–control studies with complete work history. Eur. J. Epidemiol. 2018, 33, 369–379. [Google Scholar] [CrossRef]
- Dal-Re, R.; Delgado, M.; Bolumar, F. Registration of observational studies: It is time to comply with the Declaration of Helsinki requirement. Gac. Sanit. 2015, 29, 228–231. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study, Year | Country | Population Analyzed | Sample Size | Exposure Variable/s | Outcome Ascertainment Source | Adjustment Variables | Total Quality Score 1 |
|---|---|---|---|---|---|---|---|
| Cohort Studies | |||||||
| Pukkala et al. 2002 2 | Nordic countries | Pilots cohort (1943–1997) | 10,032 | Airline-related shift work | National population-based cancer registries | Age, number of block hours in long haul aircraft, country, estimation radiation dose | 5 |
| Pukkala et al. 2003 | Nordic countries | Pilots cohort (1943–1997) | 10,051 | Airline-related shift work | National population-based cancer registries | Age, number of block hours in long haul aircraft, country, estimation radiation dose, altitude | 5 |
| Kubo et al. 2006 | Japan | Industry workers (1988–1997) | 14,052 | Night and rotating work | PC recorded by national registries | Age, FHPC, study area surveyed, BMI, smoking, alcohol drinking, job type, PA at work, workplace, perceived stress, EL, MS | 7 |
| Schwartzbaum et al. 2007 | Sweden | Industry workers (1960–1989) | 2,102,126 | Shift work | National population-based cancer registry | Age, socioeconomic status, occupational position and country of residence | 7 |
| Kubo et al. 2011 | Japan | Industry workers (1981–2009) | 4995 | Shift work | Health insurance records | Age, BMI, alcohol intake, smoking, PA and MS | 7 |
| Pukkala et al. 2012 | Nordic countries | Flight cabin workers (1947–1997) | 1559 | Airline-related shift work | National population-based cancer registry | Age, sex, country, time since first employment | 5 |
| Gapstur et al. 2014 | United States | Volunteers from general population (1982–2010) | 294,440 | Night and rotating work | Mortality by PC recorded by the National Death Index | Age, race, EL, BMI, smoking history, FHPC, frequent or painful urination | 7 |
| Yong et al. 2014 | Germany | Chemical industry workers (2000–2009) | 27,828 | Shift work | Regional population-based cancer registry | Age, smoking status, job level, and employment duration | 6 |
| Hammer et al. 2015 | Germany | Chemical industry workers (2000–2009) | 27,828 | Shift work | Regional population-based cancer registry | Age, occupational task, and duration of employment | 7 |
| Dickerman et al. 2016 | Finland | Twins cohort (1981–2012) | 11,370 | Night and rotating work | National population-based cancer registry (histologically verified). | Age, EL, BMI, PA, social class, smoking status, alcohol use, snoring, zygosity | 8 |
| Akerstedt et al. 2017 | Sweden | Twins cohort (1998–2003) | 12,322 | Night and rotating work | National population-based cancer registry | Age, EL, tobacco use, alcohol use, PA, BMI, have children, coffee use and previous cancer | 8 |
| Behrens et al. 2017 | Germany | Population from highly industrialized zone (2000–2014) | 1757 | Night and rotating work | Incident primary PC reported in the survey and subsequently evaluated in patient records. | Smoking status, FHPC, EL, equivalent income | 7 |
| Case-control studies | |||||||
| Conlon et al. 2007 | Canada | General population (1995–1998) | 2392: 760 cases, 1632 controls | Full-time rotating shift work | PC registry-identified cases | Age and FHPC | 5 |
| Parent et al. 2012 | Canada | General population (1979–1985) | 912: 400 cases, 512 controls | Night shift work | Incident PC and other cancers, pathologically confirmed | Age, ancestry, EL, family income, respondent status, smoking, alcohol, BMI, farming, PA | 5 |
| Papantoniou et al. 2015 | Spain | Hospital cases. Ambulatory controls, (2008–2013) | 2483: 1095 cases, 1388 controls | Night shift work | Incident PC, histologically confirmed | Age, center, EL, FHPC, PA, smoking status, past sun exposure and meat consumption | 7 |
| Tse et al. 2017 | China | Hospital cohort (2011–2016) | 833: 431 cases, 402 controls. | Night shift work | Incident prostate cancer, confirmed by histology | Age, MS, employment, FHPC, consumption of deep-fried food and pickled vegetable, green tea drinking habits, bisphenol A exposure | 6 |
| Wendeu-Foyet et al. 2018 | France | General population (2012–2013) | 1698: 819 cases, 879 controls | Night and rotating work | Incident prostate cancer, confirmed by histology | Age, ethnic origin, FHPC, BMI, EL, PA, sleep duration, Gleason score, chronotype | 8 |
| Barul et al. 2019 | Canada | General population (2005–2012) | 3869: 1904 cases, 1965 controls | Night and rotating work | Incident prostate cancer, confirmed by histology | Age, ethnic origin (ancestry) and EL. Lifestyle and occupational variables were not included according to a Directed Acyclic Graph. | 9 |
| Subgroup Items | Number 1 | Pooled Results | Heterogeneity (I2), % | p-Value of Heterogeneity |
|---|---|---|---|---|
| Exposure variable | ||||
| Rotating shift work exclusively | 7 | 1.05 (1.00–1.10) | 0.0 | 0.460 |
| Night-fixed work exclusively | 3 | 1.81 (0.86–2.76) | 81.2 | 0.005 |
| Both | 6 | 1.01 (0.87–1.16) | 46.0 | 0.099 |
| Study design | ||||
| Cohort | 11 | 1.03 (0.96–1.10) | 18.9 | 0.264 |
| Case-control | 5 | 1.28 (0.98–1.58) | 68.7 | 0.007 |
| Study quality | ||||
| High | 4 | 0.99 (0.80–1.17) | 0.0 | 0.108 |
| Medium | 9 | 1.06 (0.99–1.12) | 31.3 | 0.331 |
| Low | 3 | 1.52 (0.87–2.18) | 69.5 | 0.008 |
| Region of the study | ||||
| Nordic European countries | 5 | 1.03 (0.98–1.08) | 0.0 | 0.431 |
| Central-Southern European countries | 5 | 1.02 (0.85–1.18) | 44.5 | 0.125 |
| Asian countries | 3 | 1.84 (1.01–2.67) | 0.0 | 0.771 |
| United States and Canada | 3 | 1.19 (0.97–1.41) | 75.4 | 0.007 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rivera-Izquierdo, M.; Martínez-Ruiz, V.; Castillo-Ruiz, E.M.; Manzaneda-Navío, M.; Pérez-Gómez, B.; Jiménez-Moleón, J.J. Shift Work and Prostate Cancer: An Updated Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2020, 17, 1345. https://doi.org/10.3390/ijerph17041345
Rivera-Izquierdo M, Martínez-Ruiz V, Castillo-Ruiz EM, Manzaneda-Navío M, Pérez-Gómez B, Jiménez-Moleón JJ. Shift Work and Prostate Cancer: An Updated Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health. 2020; 17(4):1345. https://doi.org/10.3390/ijerph17041345
Chicago/Turabian StyleRivera-Izquierdo, Mario, Virginia Martínez-Ruiz, Elena Mercedes Castillo-Ruiz, Miriam Manzaneda-Navío, Beatriz Pérez-Gómez, and José Juan Jiménez-Moleón. 2020. "Shift Work and Prostate Cancer: An Updated Systematic Review and Meta-Analysis" International Journal of Environmental Research and Public Health 17, no. 4: 1345. https://doi.org/10.3390/ijerph17041345
APA StyleRivera-Izquierdo, M., Martínez-Ruiz, V., Castillo-Ruiz, E. M., Manzaneda-Navío, M., Pérez-Gómez, B., & Jiménez-Moleón, J. J. (2020). Shift Work and Prostate Cancer: An Updated Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health, 17(4), 1345. https://doi.org/10.3390/ijerph17041345