Dose–Response Relationship between Physical Workload and Specific Shoulder Diseases—A Systematic Review with Meta-Analysis

 ,
,  ,
,  ,
, 
Abstract
1. Introduction
2. Materials and Methods
- the aim of deriving a dose-response relationship
- the investigation of the risk for rotator cuff syndrome, in addition to the original investigation of the risks for “specific shoulder diseases” by van der Molen and colleagues [8]
- a sex-specific analysis to estimate and compare risks for women and men.
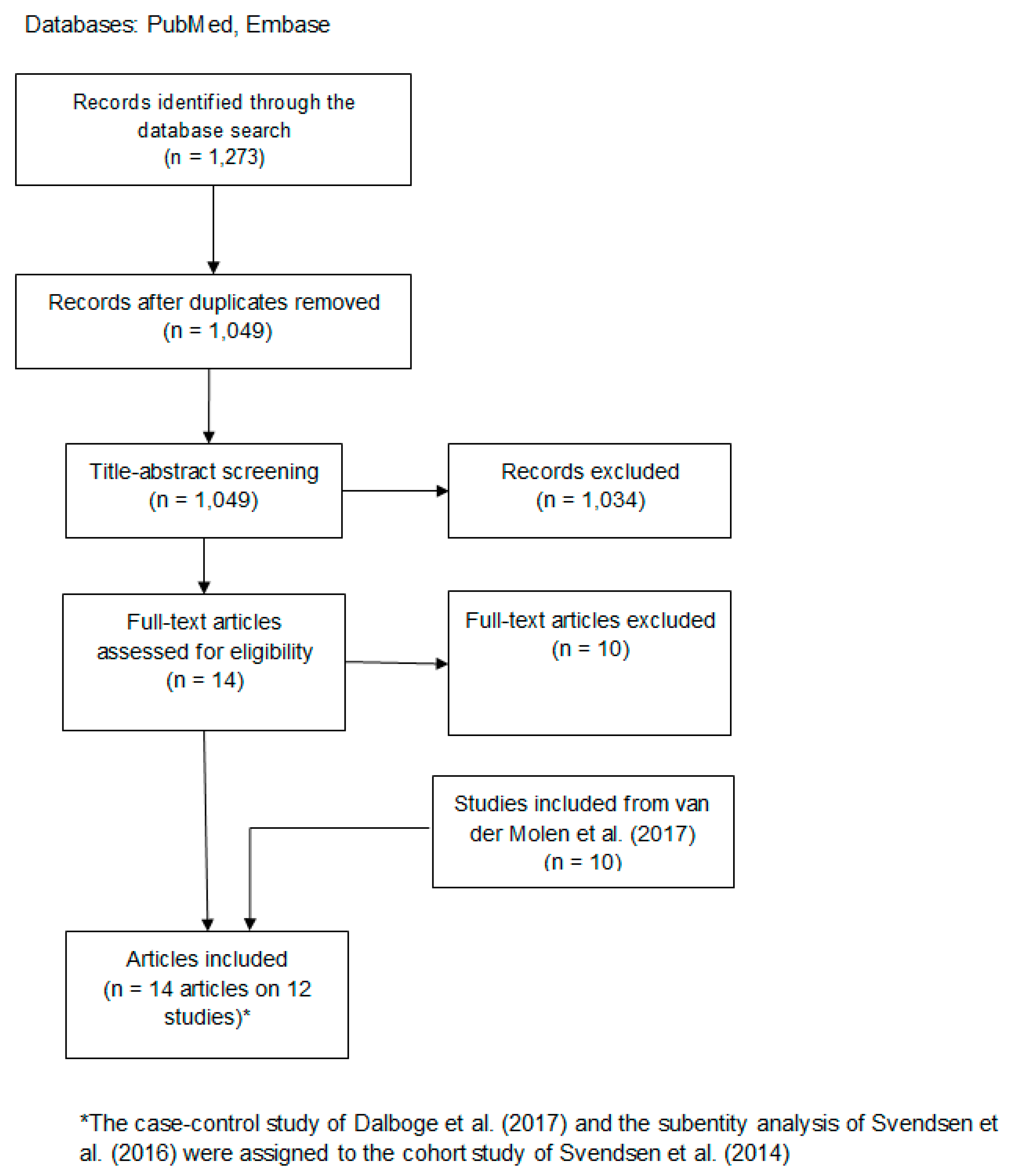
2.1. Criteria for Study Inclusion and Electronic Search
2.2. Title-Abstract and Full-Text Screening
2.3. Data Extraction and Quality Assessment
2.4. Synthesis of Evidence and Statistical Analysis
3. Results
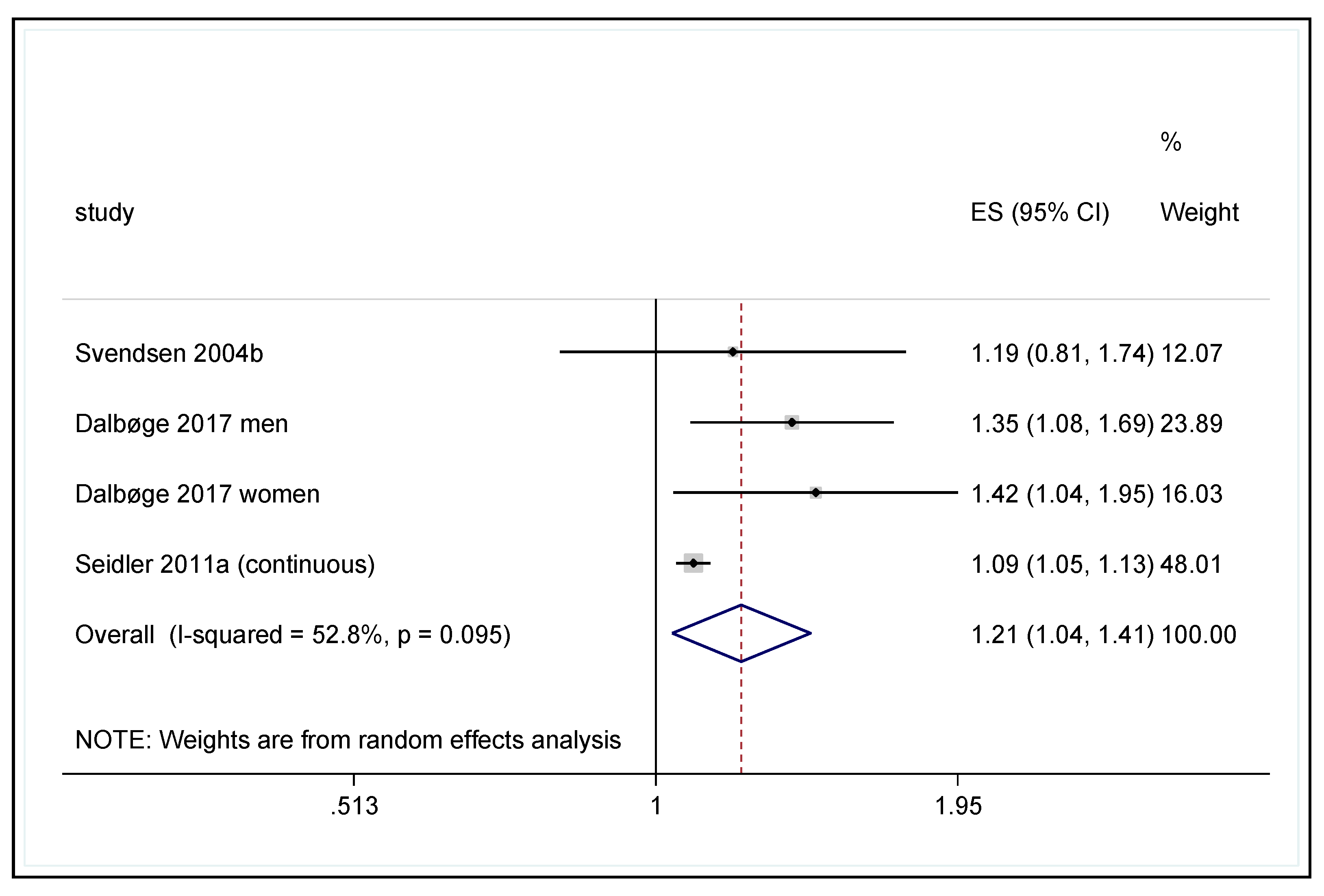
3.1. Working with the Hands at or Above Shoulder Level
3.1.1. Cumulative Exposure Calculation and Risk of Disease
3.1.2. Sex-Specific Differences in Disease Risk
3.1.3. Results of Other Studies
3.2. Working with Repetitive Movement of the Upper Arm at the Shoulder Joint
3.2.1. Cumulative Exposure Calculation and Risk of Disease
3.2.2. Sex-Specific Differences in Disease Risk
3.2.3. Results of Other Studies
3.3. Forceful Shoulder Exertions
3.3.1. Cumulative Exposure Calculation and Risk of Disease
3.3.2. Sex-Specific Differences in Disease Risk
3.3.3. Results of Other Studies
3.4. Working with Vibration of the Hands and Arms
3.4.1. Cumulative Exposure Calculation and Risk of Disease
3.4.2. Sex-Specific Differences in Disease Risk
3.4.3. Results of Other Studies
4. Discussion
4.1. Strengths and Limitations
4.2. Calculation of Cumulative Exposure
4.3. Heterogeneity of the Outcome Definitions
4.4. Assessment of Study Quality
4.5. Biological Plausibility
4.6. Comparison of the Dose-Response Association in Men and Women
4.7. Course of the Dose-Response Association between the Cumulative Load and Specific Shoulder Diseases
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Frost, P.; Andersen, J.H. Shoulder impingement syndrome in relation to shoulder intensive work. Occup. Environ. Med. 1999, 56, 494–498. [Google Scholar] [CrossRef] [PubMed]
- Frost, P.; Bonde, J.P.E.; Mikkelsen, S.; Andersen, J.H.; Fallentin, N.; Kaergaard, A.; Thomsen, J.F. Risk of shoulder tendinitis in relation to shoulder loads in monotonous repetitive work. Am. J. Ind. Med. 2002, 41, 11–18. [Google Scholar] [CrossRef] [PubMed]
- Seidler, A.; Bolm-Audorff, U.; Petereit-Haack, G.; Ball, E.; Klupp, M.; Krauss, N.; Elsner, G. Work-related lesions of the supraspinatus tendon: A case–control study. Int. Arch. Occup. Environ. Health 2011, 84, 425–433. [Google Scholar] [CrossRef] [PubMed]
- Svendsen, S.W.; Bonde, J.P.; Mathiassen, S.E.; Stengaard-Pedersen, K.; Frich, L. Work related shoulder disorders: Quantitative exposure-response relations with reference to arm posture. Occup. Environ. Med. 2004, 61, 844–853. [Google Scholar] [CrossRef]
- Svendsen, S.W.; Dalbøge, A.; Andersen, J.H.; Thomsen, J.F.; Frost, P. Risk of surgery for subacromial impingement syndrome in relation to neck-shoulder complaints and occupational biomechanical exposures: A longitudinal study. Scand. J. Work Environ. Health 2013, 39, 568–577. [Google Scholar] [CrossRef]
- Svendsen, S.W.; Gelineck, J.; Mathiassen, S.E.; Bonde, J.P.; Frich, L.H.; Stengaard-Pedersen, K.; Egund, N. Work above shoulder level and degenerative alterations of the rotator cuff tendons: A magnetic resonance imaging study. Arthritis Rheum. Off. J. Am. Coll. Rheumatol. 2004, 50, 3314–3322. [Google Scholar] [CrossRef]
- Dalbøge, A.; Frost, P.; Andersen, J.H.; Svendsen, S.W. Cumulative occupational shoulder exposures and surgery for subacromial impingement syndrome: A nationwide danish cohort study. Occup. Environ. Med. 2014, 71, 750–756. [Google Scholar] [CrossRef][Green Version]
- Van der Molen, H.F.; Foresti, C.; Daams, J.G.; Frings-Dresen, M.H.; Kuijer, P.P.F. Work-related risk factors for specific shoulder disorders: A systematic review and meta-analysis. Occup. Environ. Med. 2017, 74, 745–755. [Google Scholar] [CrossRef]
- Seidler, A.; Euler, U.; Bolm-Audorff, U.; Ellegast, R.; Grifka, J.; Haerting, J.; Jäger, M.; Michaelis, M.; Kuss, O. Physical workload and accelerated occurrence of lumbar spine diseases: Risk and rate advancement periods in a german multicenter case-control study. Scand. J. Work Environ. Health 2011, 37, 30–36. [Google Scholar] [CrossRef]
- Bodin, J.; Ha, C.; Le Manac’h, A.P.; Sérazin, C.; Descatha, A.; Leclerc, A.; Goldberg, M.; Roquelaure, Y. Risk factors for incidence of rotator cuff syndrome in a large working population. Scand. J. Work Environ. Health 2012, 38, 436–446. [Google Scholar] [CrossRef]
- Herin, F.; Vézina, M.; Thaon, I.; Soulat, J.-M.; Paris, C. Predictors of chronic shoulder pain after 5 years in a working population. PAIN® 2012, 153, 2253–2259. [Google Scholar] [CrossRef] [PubMed]
- Miranda, H.; Viikari-Juntura, E.; Heistaro, S.; Heliövaara, M.; Riihimäki, H. A population study on differences in the determinants of a specific shoulder disorder versus nonspecific shoulder pain without clinical findings. Am. J. Epidemiol. 2005, 161, 847–855. [Google Scholar] [CrossRef] [PubMed]
- Silverstein, B.A.; Bao, S.S.; Fan, Z.J.; Howard, N.; Smith, C.; Spielholz, P.; Bonauto, D.; Viikari-Juntura, E. Rotator cuff syndrome: Personal, work-related psychosocial and physical load factors. J. Occup. Environ. Med. 2008, 50, 1062–1076. [Google Scholar] [CrossRef]
- Sutinen, P.; Toppila, E.; Starck, J.; Brammer, A.; Zou, J.; Pyykkö, I. Hand-arm vibration syndrome with use of anti-vibration chain saws: 19-year follow-up study of forestry workers. Int. Arch. Occup. Environ. Health 2006, 79, 665–671. [Google Scholar] [CrossRef]
- Dalbøge, A.; Frost, P.; Andersen, J.H.; Svendsen, S.W. Surgery for subacromial impingement syndrome in relation to intensities of occupational mechanical exposures across 10-year exposure time windows. Occup. Environ. Med. 2018, 75, 176–182. [Google Scholar] [CrossRef]
- Dalbøge, A.; Frost, P.; Andersen, J.H.; Svendsen, S.W. Surgery for subacromial impingement syndrome in relation to occupational exposures, lifestyle factors and diabetes mellitus: A nationwide nested case–control study. Occup. Environ. Med. 2017, 74, 728–736. [Google Scholar] [CrossRef]
- Møller, S.P.; Brauer, C.; Mikkelsen, S.; Alkjær, T.; Koblauch, H.; Pedersen, E.B.; Simonsen, E.B.; Thygesen, L.C. Risk of subacromial shoulder disorder in airport baggage handlers: Combining duration and intensity of musculoskeletal shoulder loads. Ergonomics 2018, 61, 576–587. [Google Scholar] [CrossRef]
- Thygesen, L.C.; Mikkelsen, S.; Pedersen, E.B.; Møller, K.L.; Alkjær, T.; Koblauch, H.; Simonsen, E.B.; Møller, S.P.; Brauer, C. Subacromial shoulder disorders among baggage handlers: An observational cohort study. Int. Arch. Occup. Environ. Health 2016, 89, 867–876. [Google Scholar] [CrossRef]
- Ijaz, S.; Verbeek, J.; Seidler, A.; Lindbohm, M.-L.; Ojajärvi, A.; Orsini, N.; Costa, G.; Neuvonen, K. Night-shift work and breast cancer—A systematic review and meta-analysis. Scand. J. Work Environ. Health 2013, 39, 431–447. [Google Scholar] [CrossRef]
- Orsini, N.; Bellocco, R.; Greenland, S. Generalized least squares for trend estimation of summarized dose–response data. Stata J. 2006, 6, 40–57. [Google Scholar] [CrossRef]
- Aune, D.; Sen, A.; Prasad, M.; Norat, T.; Janszky, I.; Tonstad, S.; Romundstad, P.; Vatten, L.J. Bmi and all cause mortality: Systematic review and non-linear dose-response meta-analysis of 230 cohort studies with 3.74 million deaths among 30.3 million participants. BMJ 2016, 353, i2156. [Google Scholar] [CrossRef] [PubMed]
- Guyatt, G.; Oxman, A.D.; Akl, E.A.; Kunz, R.; Vist, G.; Brozek, J.; Norris, S.; Falck-Ytter, Y.; Glasziou, P.; deBeer, H.; et al. Grade guidelines: 1. Introduction—Grade evidence profiles and summary of findings tables. J. Clin. Epidemiol. 2011, 64, 383–394. [Google Scholar] [CrossRef] [PubMed]
- Svendsen, S.W. Personal communication, Email dated. 14 July 2017.
- Dalbøge, A.; Frost, P.; Andersen, J.H.; Svendsen, S.W. Exposure–response relationships between cumulative occupational shoulder exposures and different diagnoses related to surgery for subacromial impingement syndrome. Int. Arch. Occup. Environ. Health 2019. [Epub ahead of print]. [Google Scholar]
- Dalbøge, A.; Svendsen, S.W.; Frost, P.; Andersen, J.H. Association between Occupational Mechanical Exposures and Subacromial Impingement Syndrome: A Reference Document. 2019. Available online: https://www.google.com/url?sa=t&rct=j&q=&esrc=s&source=web&cd=7&ved=2ahUKEwjRp6W0iM_nAhWNFMAKHSCsDL4QFjAGegQIBxAB&url=https%3A%2F%2Fwww.aes.dk%2F-%2Fmedia%2F3EA35B61FFE3472EA738F8F4B909BCA7.ashx&usg=AOvVaw1w-un--_wZMqK7aHpHJMeF (accessed on 13 February 2020).
- Hagberg, M. Electromyographic signs of shoulder muscular fatigue in two elevated arm positions. Am. J. Phys. Med. 1981, 60, 111–121. [Google Scholar] [PubMed]
- Herberts, P.; Kadefors, R. A study of painful shoulder in welders. Acta Orthop. Scand. 1976, 47, 381–387. [Google Scholar] [CrossRef]
- Kadefors, R.; Petersen, I.; Herberts, P. Muscular reaction to welding work: An electromyographic investigation. Ergonomics 1976, 19, 543–558. [Google Scholar] [CrossRef]
- Järvholm, U.; Palmerud, G.; Styf, J.; Herberts, P.; Kadefors, R. Intramuscular pressure in the supraspinatus muscle. J. Orthop. Res. 1988, 6, 230–238. [Google Scholar] [CrossRef]
- Järvholm, U.; Styf, J.; Suurkula, M.; Herberts, P. Intramuscular pressure and muscle blood flow in supraspinatus. Eur. J. Appl. Physiol. Occup. Physiol. 1988, 58, 219–224. [Google Scholar] [CrossRef]
- Järvholm, U.; Palmerud, G.; Herberts, P.; Högfors, C.; Kadefors, R. Intramuscular pressure and electromyography in the supraspinatus muscle at shoulder abduction. Clin. Orthop. Relat. Res. 1989, 245, 102–109. [Google Scholar]
- Järvholm, U.; Palmerud, G.; Karlsson, D.; Herberts, P.; Kadefors, R. Intramuscular pressure and electromyography in four shoulder muscles. J. Orthop. Res. 1991, 9, 609–619. [Google Scholar] [CrossRef]
- Palmerud, G.; Forsman, M.; Sporrong, H.; Herberts, P.; Kadefors, R. Intramuscular pressure of the infra-and supraspinatus muscles in relation to hand load and arm posture. Eur. J. Appl. Physiol. 2000, 83, 223–230. [Google Scholar] [CrossRef] [PubMed]
- Burns, W.C.; Whipple, T. Anatomic relationships in the shoulder impingement syndrome. Clin. Orthop. Relat. Res. 1993, 294, 96–102. [Google Scholar] [CrossRef]
- Perry, S.M.; McIlhenny, S.E.; Hoffman, M.C.; Soslowsky, L.J. Inflammatory and angiogenic mrna levels are altered in a supraspinatus tendon overuse animal model. J. Shoulder Elb. Surg. 2005, 14, S79–S83. [Google Scholar] [CrossRef] [PubMed]
- Soslowsky, L.; Thomopoulos, S.; Tun, S.; Flanagan, C.; Keefer, C.; Mastaw, J.; Carpenter, J. Neer award 1999: Overuse activity injures the supraspinatus tendon in an animal model: A histologic and biomechanical study. J. Shoulder Elb. Surg. 2000, 9, 79–84. [Google Scholar] [CrossRef]
- Soslowsky, L.J.; Thomopoulos, S.; Esmail, A.; Flanagan, C.L.; Iannotti, J.P.; Williamson, J.D.; Carpenter, J.E. Rotator cuff tendinosis in an animal model: Role of extrinsic and overuse factors. Ann. Biomed. Eng. 2002, 30, 1057–1063. [Google Scholar] [CrossRef]
- Backman, C.; Boquist, L.; Fridén, J.; Lorentzon, R.; Toolanen, G. Chronic achilles paratenonitis with tendinosis: An experimental model in the rabbit. J. Orthop. Res. 1990, 8, 541–547. [Google Scholar] [CrossRef]
- Barbe, M.F.; Barr, A.E.; Gorzelany, I.; Amin, M.; Gaughan, J.P.; Safadi, F.F. Chronic repetitive reaching and grasping results in decreased motor performance and widespread tissue responses in a rat model of msd. J. Orthop. Res. 2003, 21, 167–176. [Google Scholar] [CrossRef]
- Barbe, M.F.; Elliott, M.B.; Abdelmagid, S.M.; Amin, M.; Popoff, S.N.; Safadi, F.F.; Barr, A.E. Serum and tissue cytokines and chemokines increase with repetitive upper extremity tasks. J. Orthop. Res. 2008, 26, 1320–1326. [Google Scholar] [CrossRef]
- Nakama, L.H.; King, K.B.; Abrahamsson, S.; Rempel, D.M. Effect of repetition rate on the formation of microtears in tendon in an in vivo cyclical loading model. J. Orthop. Res. 2007, 25, 1176–1184. [Google Scholar] [CrossRef]
- Nakama, L.H.; King, K.B.; Abrahamsson, S.; Rempel, D.M. Evidence of tendon microtears due to cyclical loading in an in vivo tendinopathy model. J. Orthop. Res. 2005, 23, 1199–1205. [Google Scholar] [CrossRef]
- Fedorczyk, J.M.; Barr, A.E.; Rani, S.; Gao, H.G.; Amin, M.; Amin, S.; Litvin, J.; Barbe, M.F. Exposure-dependent increases in il-1β, substance p, ctgf, and tendinosis in flexor digitorum tendons with upper extremity repetitive strain injury. J. Orthop. Res. 2010, 28, 298–307. [Google Scholar] [CrossRef] [PubMed]
- Sirén, M.; Viikari-Juntura, E.; Arokoski, J.; Solovieva, S. Physical and psychosocial work exposures as risk factors for disability retirement due to a shoulder lesion. Occup. Environ. Med. 2019, 76, 793–800. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Author, Study Design 1 | Outcome (Prevalence; Incidence) | Exposure | ||
|---|---|---|---|---|
| Definition | Assessment | Definition | Assessment | |
| Dalbøge et al. 2018 [15] cohort; Svendsen 2017 [23] | As in Dalbøge et al. 2014 [7]: Subacromial impingement syndrome first-time surgery 2003–08 ICD-10: M19 or M75.1–M75.9); Svendsen 2017 [23]: only rotator cuff tear or rupture (M75.1) | Medical registry | Job exposure matrix assessments (10-yr time window with a 1-yr lag time) of years of arm elevation (>90°), repetitiveness, force and acceleration (HAV), shoulder load by five specialists in occupational medicine | Registries (years till 1993), expert assessment, job exposure matrix |
| Dalbøge et al. 2017 [16]. nested CC (2 age- and sex matched controls per case), in cohort described by Dalbøge et al. 2014 [7] | As in Dalbøge et al. 2014 [7]: Subacromial impingement syndrome first-time surgery 2003-08 ICD-10: M19 or M75.1–M75.9) | Medical registry | Updated job exposure matrix (JEM) assessments (10-yr time window with a 1-yr lag time) of years of arm elevation (>90°), repetitiveness, force and acceleration (HAV), shoulder load by five specialists in occupational medicine; job exposure matrix assessments up to the index year (yr. of the surgery of the case) | Measurement-based JEM (related to self-reported job titles, up to 6 in a 10-year period) |
| Møller et al. 2018 [17]. Cohort study (Copenhagen Airport Cohort, see Thygesen et al. 2016 [18]) | Diagnosis or surgical treatment of subacromial shoulder disorders (ICD 75.1–75.5, 75.8, 75.9) | National patient register | Accumulated abduction moment, compression force or supraspinatus force and seniority as baggage handler | Capture motion system, ground reaction force, biomechanical modelling and company records |
| Thygesen et al. [18].Cohort study (Copenhagen Airport Cohort) based on unskilled men at Copenhagen Airport & in the Greater Copenhagen area | Diagnosis or surgical treatment of subacromial shoulder disorders (ICD 75.1–75.5, 75.8, 75.9) | National patient register | Seniority as baggage handler | Company and union records |
| Authors/Quality Item | 1 (Study Groups De-fined) | 2 (par-tici-pa-tion ≥70%) | 3 (Num-ber Case ≥50) | 4 (Expo-sure Measure-ment) | 5 (Dose-Re-sponse) | 6 (Blind for Out-come Sta-tus) | 7 (Out-come Defini-tion) | 8 (Assess-ment Method) | 9 (Blind for Expo-sure Status) | 10 (longitu-dinal Study Design) | 11 (Inclu-sion and Exclu-sion Criteria) | 12 (Fol-low-up Period ≥1 year) | 13 (Info complet-ers Versus With-drawal) | 14 (Data Presentation) | 15 (Considera-tion of Confounders) | 16 (Control for Confound-ing) | Sum |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Thygesen et al. 2016 [18] | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + § | 16 |
| Møller et al. 2018 [17] | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + § | 16 |
| Dalbøge et al. 2018 [15] | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + §§ | 16 |
| Dalbøge et al. 2017 [16] | + | − | + | + | + | + | + | + | + | + | + | + | − * | + | + | + §§§ | 14 |
| Study; Outcome | Exposure Parameter | Calculation of Lifetime Hours | Cumulative Exposure (Lifetime Hours) | OR Adjusted for Non-Occupational Factors (95% CI) |
|---|---|---|---|---|
| Dalbøge et al. 2014 [7] * | Arm-Elevation-Years (1 Arm-Elevation-Year = Working with Elevated Arm(s) >90° for 0.5 h/day for 1 Year) | |||
| Outcome: subacromial impingement syndrome first-time surgery 2003-08 ICD-10: M19 or M75.1–M75.9. Men and women (n = 2,374,403 participants, of those 14,118 cases) | 0 | 0 h | 0 h | 1.0 - |
| >0–2 | 3 × 1 × 0.5 h/day × 220 days | 330 h | 1.4 (1.4–1.5) | |
| >2–5 | 3 × 3.5 × 0.5 h/day × 220 days | 1155 h | 1.5 (1.5–1.6) | |
| >5–10 | 3 × 7.5 × 0.5 h/day × 220 days | 2475 h | 1.8 (1.7–1.9) | |
| >10–56 | 3 × 15 × 0.5 h/day × 220 days | 4950 h | 2.1 (2.0–2.2) | |
| Svendsen 2017 [23] (Personal Communication; Same Results Given in Dalbøge et al. 2019a [24]) | ||||
| Outcome: rotator cuff lesion ICD10: M75.1. Men and women | 0 | 0 h | 0 h | 1.0 - |
| >0–2 | 3 × 1 × 0.5 h/day × 220 days | 330 h | 1.5 (1.3–1.7) | |
| >2–5 | 3 × 3.5 × 0.5 h/day × 220 days | 1155 h | 1.6 (1.4–1.9) | |
| >5–10 | 3 × 7.5 × 0.5 h/day × 220 days | 2475 h | 1.9 (1.7–2.2) | |
| >10–56 | 3 × 15 × 0.5 h/day × 220 days | 4950 h | 2.4 (2.1–2.8) | |
| Dalbøge et al. 2017 [16] ** | Arm-Elevation-Years (Calibrated into ‘Predicted Measured Job Exposures’, 1 Arm-Elevation-Year Adds 4.8 min to the Background Duration of 2.3 min per Day with the Arm Elevated >90°) | |||
| Outcome: subacromial impingement syndrome first-time surgery 2003-08 ICD-10: M19 or M75.1–M75.9. Men (n = 701 cases, 974 control subjects) | 0 | >0 h (background duration) | 0 h | 1.0 - |
| >0–10 (mean 3.7) | 3.6 × (3.7 × 7.1 min./day × 220 days)/60 min./h | 347 h | 2.0 (1.6–2.5) | |
| >10–60 (mean 23.5) | 3.6 × (23.5 × 7.1 min./day × 220 days)/60 min./h | 2202 h | 2.3 (1.8–3.0) | |
| Women (n = 863 cases, 1260 control subjects) | 0 | >0 h (background duration | 0 h | 1.0 - |
| >0–10 (mean 4.1) | 3.4 × (4.1 × 7.1 min./day × 220 days)/60 min./h | 363 h | 1.6 (1.3–1.9) | |
| >10–60 (mean 22.2) | 3.4 × (22.2 × 7.1 min./day × 220 days)/60 min./h | 1965 h | 1.9 (1.4–2.6) | |
| Seidler et al. 2011a [3] | Cumulative Work Above Shoulder Level [Hrs.] | |||
| Outcome: supraspinatus lesion. Men(n = 483 cases, n = 300 control subjects) | No work above shoulder level | 0 h | 1.0 | |
| >0–<610 h (median 272 h)$ | 272 h | 1.7 (1.0–2.8) | ||
| 610–<3195 h (median 1529 h)$ | 1529 h | 2.6 (1.6–4.2) | ||
| 3195–64,057 h (median 9965 h) $ | 9965 h | 4.1 (2.6–6.4) | ||
| Per 1000 h. work above shoulder level (based on continuous variable) | 1.09 (1.05–1.13) $ | |||
| Svendsen et al. 2004b [6] | Cumulative Duration (Month) of Upper Arm Elevation > 90° | |||
| Outcome: supraspinatus tendonitis. Men (n = 52 cases) | <10 | 5 × 20 days × 8 h | 800 h | 1.00 |
| 10–<20 | 15 × 20 days × 8 h | 2400 h | 0.95 (0.41–2.20) | |
| ≥20 | 30 × 20 days × 8 h | 4800 h | 2.33 (0.93–5.84) | |
| Study; Outcome | Exposure Parameter | Calculation of Lifetime Hours | Cumulative Exposure (Lifetime Hours of Highly Repetitive Work) † | OR Adjusted for Non-Occupational Factors (95% CI) |
|---|---|---|---|---|
| Dalbøge et al. 2014 [7] * | Repetition Years (1 Repetition Year = Performing Moderately Repetitive Work for 4 h/day for 1 year or Highly Repetitive Work for 1 h/day for 1 Year) | |||
| Outcome: subacromial impingement syndrome first-time surgery 2003-08 ICD-10: M19 orM75.1–M75.9. Men and women (n = 2,374,403 participants, of those 14,118 cases) | 0 | 0 h | 0 h | 1.0 |
| >0–1 | 3 × 0.5 × 1 h/day × 220 days | 330 h | 1.2 (1.1–1.3) | |
| >1–2 | 3 × 1.5 × 1 h/day × 220 days | 990 h | 1.5 (1.5–1.6) | |
| >2–10 | 3 × 6 × 1 h/day × 220 days | 3960 h | 1.6 (1.5–1.6) | |
| >10–68 | 3 × 18 × 1 h/day × 220 days | 11,880 h | 1.9 (1.8–2.0) | |
| Dalbøge et al. 2017 [16] **.N = 1564 Cases, 2234 Control Subjects | Repetition–Years (Calibrated into ‘Predicted Measured Job Exposures’, 1 Repetition Year Adds 25°/s to the Background Median Angular Velocity of Upper Arm Movements of 27°/s per day) | |||
| Outcome: subacromial impingement syndrome first-time surgery 2003-08 ICD-10: M19 or M75.1–M75.9. Men (n = 701 cases, 974 control subjects) | 0 | 1.0 - | ||
| >0–10 (mean 4.8) | 1.7 (1.4–2.1) | |||
| >10–17.5 (mean 12.7) | 2.6 (1.5–4.6) | |||
| Women (n = 863 cases, 1260 control subjects) | 0 | 1.0 - | ||
| >0–10 (mean 5.5) | 1.5 (1.2–1.9) | |||
| >10–17.5 (mean 11.8) | 2.0 (1.0–4.4) | |||
| Study; Outcome | Exposure Parameter | Calculation of Lifetime Duration | Cumulative Exposure (Lifetime Hours Resp. Years) | OR Adjusted for Non-Occupational Factors (95% CI) |
|---|---|---|---|---|
| Dalbøge et al. 2014 [7] * | Force-years (1 Force-Year = Working with a Force Score of 2 (Five-Point Rating of Intensity Of Exertion, Moore, J.S.; Garg, A. The Strain Index: a Proposed Method to Analyze Jobs for Risk Of Distal Upper Extremity Disorders. Am. Ind. Hyg. Assoc. J. 1995, 56:, 443–58) for 1 year) | |||
| Outcome: subacromial impingement syndrome first-time surgery 2003-08 ICD-10: M19 or M75.1–M75.9. Men and women (n = 2,374,403 participants, of those 14,118 cases) | <5 | 0 yrs. | 0 yrs. | 1.0 - |
| 5 | 3 × 2.5 yrs. | 7.5 yrs. | 0.7 (0.6–0.7) | |
| >5–7.5 | 3 × 6.25 yrs. | 18.8 yrs. | 1.2 (1.1–1.2) | |
| >7.5–10 | 3 × 8.75 yrs. | 26.3 yrs. | 1.5 (1.4–1.6) | |
| >10–20 | 3 × 12.5 yrs. | 37.5 yrs. | 1.7 (1.6–1.8) | |
| Dalbøge et al. 2017 [16] ** | Force-Years (1 Force-Year = Working with a Force Score of 2 (Five-Point Rating of Intensity of Exertion, Moore, J.S.; Garg, A. The strain index: a proposed method to analyze jobs for risk of distal upper extremity disorders. Am. Ind. Hyg. Assoc. J. 1995, 56, 443–458) for 1 Year) | |||
| Outcome: subacromial impingement syndrome first-time surgery 2003-08 ICD-10: M19 or M75.1–M75.9. Men (n = 701 cases, 974 control subjects) | 0 | 0 yrs. | 0 yrs. | 1.0 - |
| >0–10 (mean 5.7) | 3.6 × 5.7 yrs. | 20.5 yrs. | 2.0 (1.6–2.5) | |
| >10–30 (mean 16.6) | 3.6 × 16.6 yrs. | 59.8 yrs. | 2.6 (2.0–3.4) | |
| Women (n = 863 cases, 1260 control subjects) | 0 | 0 yrs. | 0 yrs. | 1.0 - |
| >0–10 (mean 6.4) | 3.4 × 6.4 yrs. | 21.8 yrs. | 1.7 (1.4–2.1) | |
| >10–30 (mean 17.7) | 3.4 × 17.7 yrs. | 60.2 yrs. | 2.3 (1.6–3.3) | |
| Seidler et al. 2011a [3] | Cumulative Lifting and Carrying of Loads ≥ 20 kg [hours] | |||
| Outcome: supraspinatus lesion. Men (n = 483 cases, n = 300 control subjects) | No lifting and carrying of loads ≥ 20 kg [h] | 0 h | 1.0 | |
| >0–<9.6 h (median 3.2 h) $ | 3.2 h | 1.4 (0.8–2.4) | ||
| 9.6–<77 h (median 28 h) $ | 28 h | 2.0 (1.2–3.3) | ||
| 77–9038 h (median 385 h) $ | 385 h | 3.3 (2.1–5.2) | ||
| Study; Outcome | Exposure Parameter | Calculation of Lifetime Hours | Cumulative Exposure (Lifetime Hours of Moderate Acceleration) | OR Adjusted for Non-Occupational Factors (95% CI) |
|---|---|---|---|---|
| Dalbøge et al. 2014 [7] * | HAV-Years (1 HAV-Year = Working with a Hand-Held Vibrating Tool with Low Acceleration for 1 h/day for 1 year, or Working with a Hand-Held Vibrating Tool with Moderate Acceleration for 0.5 h/day for 1 year; Low, Moderate and High Acceleration was Defined as <3, ≥3–10 and >10 m/s2, Duration was Rated in Half-Hour Intervals) | |||
| Outcome: subacromial impingement syndrome first-time surgery 2003-08 ICD-10: ML19 or M75.1–M75.9. Men and women (n = 2,374,403 participants, of those 14,118 cases) | 0 | 0 h | 0 h | 1.0 - |
| <0–5 | 3 × 2.5 × 0.5 h/day × 220 days | 825 h | 1.3 (1.2–1.3) | |
| >5–58 | 3 × 10 × 0.5 h/day × 220 days | 3300 h | 1.5 (1.5–1.6) | |
| Dalbøge et al. 2017 [16] ** | HAV-Years (1 HAV-Year = Working with a Hand-Held Vibrating Tool with Low Acceleration for 1 h/day for 1 year, or Working with a Hand-Held Vibrating Tool with Moderate Acceleration for 0.5 h/day for 1 year; Low, Moderate and High Acceleration was Defined As <3, ≥3–10 and >10 m/s2, Duration was Rated in Half-Hour Intervals) | |||
| Outcome: subacromial impingement syndrome first-time surgery 2003-08 ICD-10: M19 or M75.1–M75.9. Men (n = 701 cases, 974 control subjects) | 0 | 0 h | 0 h | 1.0 - |
| >0–58 (mean 14.5) | 3.6 × 14.5 × 0.5 h/day × 220 days | 5742 h | 1.9 (1.5–2.4) | |
| Women (n = 863 cases, 1260 control subjects) | 0 | 0 h | 0 h | 1.0 - |
| >0–20 (mean 10.6) | 3.4 × 10.6 × 0.5 h/day × 220 days | 3964 h | 1.8 (1.3–2.6) | |
| Sutinen et al. 2006 [14] | Lifelong vibration energy [modified from Bovenzi M, Franzinelli A, Mancini R, Cannava MG, Maiorano M, Ceccarelli F (1995) Dose–response relation for vascular disorders induced by vibration in the fingers of forestry workers. Occup Environ Med 52:722–730] | |||
| Outcome: rotator cuff syndrome. Men (n = 52 participants at 11 surveys, of those n = 10 cases) | Per 1 unit of lifelong vibration energy? | 1.04 (1.00–1.07) p = 0.032 | ||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Seidler, A.; Romero Starke, K.; Freiberg, A.; Hegewald, J.; Nienhaus, A.; Bolm-Audorff, U. Dose–Response Relationship between Physical Workload and Specific Shoulder Diseases—A Systematic Review with Meta-Analysis. Int. J. Environ. Res. Public Health 2020, 17, 1243. https://doi.org/10.3390/ijerph17041243
Seidler A, Romero Starke K, Freiberg A, Hegewald J, Nienhaus A, Bolm-Audorff U. Dose–Response Relationship between Physical Workload and Specific Shoulder Diseases—A Systematic Review with Meta-Analysis. International Journal of Environmental Research and Public Health. 2020; 17(4):1243. https://doi.org/10.3390/ijerph17041243
Chicago/Turabian StyleSeidler, Andreas, Karla Romero Starke, Alice Freiberg, Janice Hegewald, Albert Nienhaus, and Ulrich Bolm-Audorff. 2020. "Dose–Response Relationship between Physical Workload and Specific Shoulder Diseases—A Systematic Review with Meta-Analysis" International Journal of Environmental Research and Public Health 17, no. 4: 1243. https://doi.org/10.3390/ijerph17041243
APA StyleSeidler, A., Romero Starke, K., Freiberg, A., Hegewald, J., Nienhaus, A., & Bolm-Audorff, U. (2020). Dose–Response Relationship between Physical Workload and Specific Shoulder Diseases—A Systematic Review with Meta-Analysis. International Journal of Environmental Research and Public Health, 17(4), 1243. https://doi.org/10.3390/ijerph17041243