Diabetes Detection and Communication among Patients Admitted through the Emergency Department of a Public Hospital




Abstract
1. Introduction
2. Materials and Methods
2.1. Study Setting and Population
2.2. Ethics
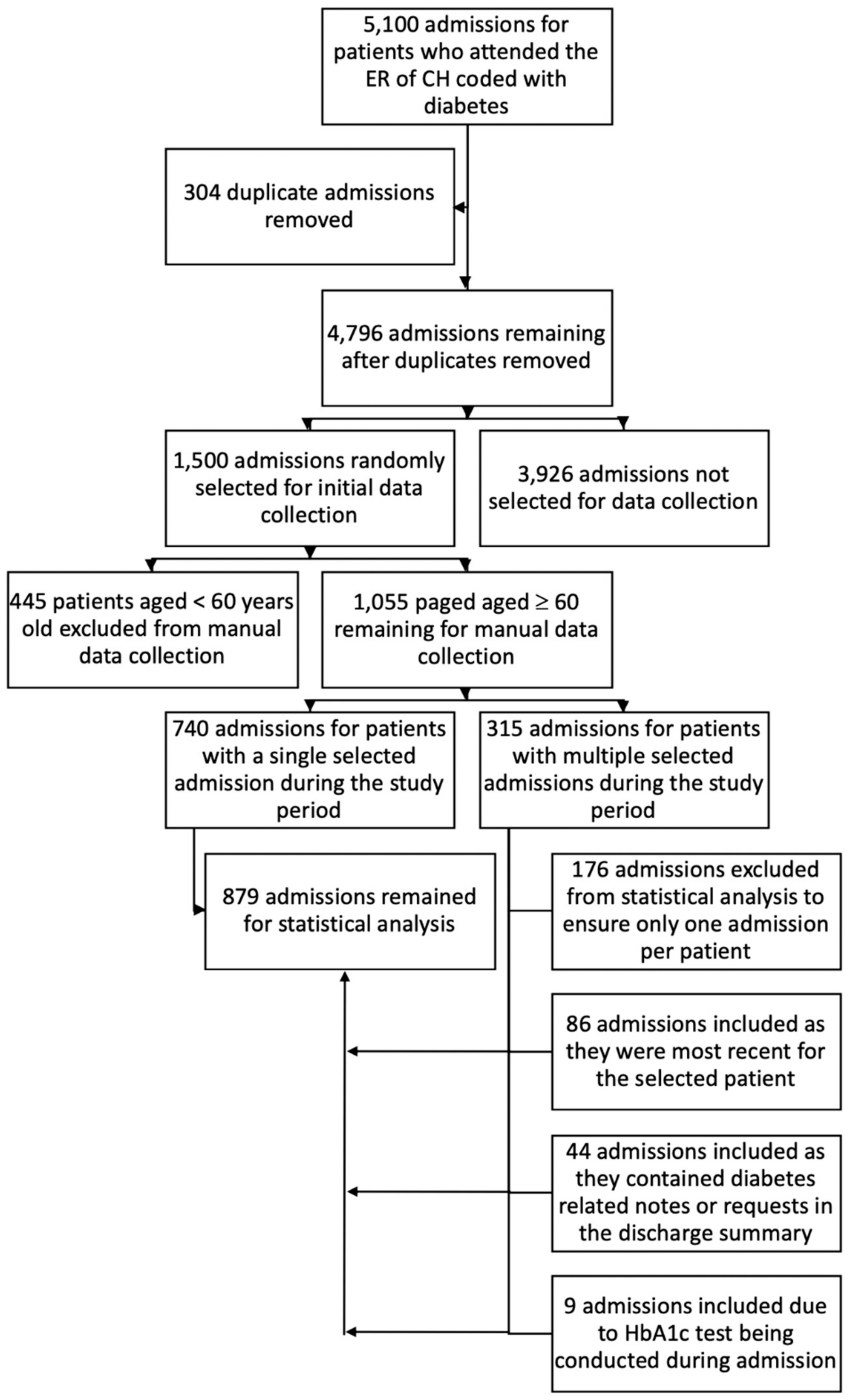
2.3. Selection Protocol
2.4. ED Outcome Variables
2.5. Statistical Analysis
3. Results
3.1. Characteristics of the Patients
3.2. Glycaemic Monitoring of People with Diabetes
3.3. Discharge Summaries
3.4. Factors Associated with Elevated HbA1c
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Wild, S.; Roglic, G.; Green, A.; Sicree, R.; King, H. Global prevalence of diabetes: Estimates for the year 2000 and projections for 2030. Diabetes Care 2004, 27, 1047–1053. [Google Scholar] [CrossRef]
- The Burden of Diabetes in Australia: Its Time for More Action. Baulkham Hills, NSW: Novo Nordisk Pharmaceuticals. 2018. Available online: http://www.novonordisk.com.au/content/dam/australia/affiliate/www-novonordisk-au/Home/Documents/180712_Burden%20of%20Diabetes_Its%20Time%20for%20More%20Action%20Report_Digital_%20FINAL....pdf (accessed on 23 November 2019).
- Diabetes in South Western Sydney [Internet]. Campbelltown, NSW: PHN South Western Sydney: The Australian Initiative. 2016. Available online: http://www.swsphn.com.au/diabetesinsws (accessed on 14 June 2019).
- Shaw, J.; Tanamas, S. Diabetes: The Silent Pandemic and Its Impact on Australia. Baulkham Hills, NSW: Baker IDI, Heart and Diabetes Institute. 2012. Available online: https://static.diabetesaustralia.com.au/s/fileassets/diabetes-australia/e7282521-472b-4313-b18e-be84c3d5d907.pdf (accessed on 18 August 2019).
- Simmons, D.; Wenzel, H. Diabetes inpatients: A case of lose, lose, lose. Is it time to use a ‘diabetes-attributable hospitalization cost’ to assess the impact of diabetes? Diabetic Med. 2011, 28, 1123–1230. [Google Scholar] [CrossRef]
- Dunstan, D.W.; Zimmet, P.Z.; Welborn, T.A.; De Courten, M.P.; Cameron, A.J.; Sicree, R.A.; Dwyer, T.; Colagiuri, S.; Jolley, D.; Knuiman, M.; et al. The rising prevalence of diabetes and impaired glucose tolerance: The Australian Diabetes, Obesity and Lifestyle Study. Diabetes Care 2002, 25, 829–834. [Google Scholar] [CrossRef]
- Cameron, A.J.; Zimmet, P.Z.; Dunstan, D.W.; Dalton, M.; Shaw, J.E.; Welborn, T.A.; Owen, N.; Salmon, J.; Damien, J. Overweight and obesity in Australia: The 1999–2000 Australian Diabetes, Obesity and Lifestyle Study (AusDiab). Med. J. Aust. 2003, 178, 427–432. [Google Scholar] [CrossRef]
- Osuagwu, U.L.; Flack, J.; Wong, J.; Piya, M.; Simmons, D. Prevalence of Diabetes Mellitus and Risk Factors in South Western Sydney-Where are we now? Campbelltown, NSW: Western Sydney University. 2019. Available online: https://www.westernsydney.edu.au/__data/assets/pdf_file/0011/1556390/Diabetes_Monograph.pdf (accessed on 12 November 2019).
- California Healthcare Foundation/American Geriatrics Society Panel on Improving Care for Elders with Diabetes; Brown, A.F.; Mangione, C.M.; Saliba, D.; Sarkisian, C.A. Guidelines for improving the care of the older person with diabetes mellitus. J. Am. Geriatr. Soc. 2003, 51, 265–280. [Google Scholar]
- Kirkman, M.S.; Briscoe, V.J.; Clark, N.; Florez, H.; Haas, L.B.; Halter, J.B.; Huang, E.S.; Korytkowski, M.T.; Munshi, M.N.; Odegard, P.S.; et al. Diabetes in Older Adults. Diabetes Care 2012, 35, 2650. [Google Scholar] [CrossRef]
- Beagley, J.; Guariguata, L.; Weil, C.; Motala, A.A. Global estimates of undiagnosed diabetes in adults. Diabetes Res. Clin. Pract. 2014, 103, 150–160. [Google Scholar] [CrossRef] [PubMed]
- Hng, T.-M.; Hor, A.; Ravi, S.; Feng, X.; Lin, J.; Astell-Burt, T.; Chipps, D.; McLean, M.; Maberly, G. Diabetes case finding in the emergency department, using HbA1c: An opportunity to improve diabetes detection, prevention, and care. BMJ Open Diabetes Res. Care 2016, 4, 1–4. [Google Scholar] [CrossRef]
- American Diabetes Association. (2) Classification and diagnosis of diabetes. Diabetes Care 2015, 38 (Suppl. 1), S8–S16. [Google Scholar] [CrossRef] [PubMed]
- Irvin, C.B.; Wyer, P.C.; Gerson, L.W.; Society for Academic Emergency Medicine Public Health; Education Task Force Preventive Services Work Group. Preventive care in the emergency department, part II: Clinical preventive services—An emergency medicine evidence-based review. Acad. Emerg. Med. 2000, 7, 1042–1054. [Google Scholar] [CrossRef] [PubMed]
- World Health Organisation Consultation. Use of glycated haemoglobin (HbA1c) in the diagnosis of diabetes mellitus. Diab. Res. Cin. Pract. 2011, 93, 299–309. [Google Scholar] [CrossRef]
- Simmons, D.; Zgibor, J.C. Should we screen for type 2 diabetes among asymptomatic individuals? Yes. Diabetologia 2017, 60, 2148–2152. [Google Scholar] [CrossRef] [PubMed]
- ABS. Census of Population and Housing: Nature and Content. Canberra: Australian Bureau of Statistics, 2016 cat no. 2916.0. Available online: http://www.abs.gov.au/websitedbs/D3310114.nsf/Home/2016%20search%20by%20geography (accessed on 17 September 2018).
- Bar-Dayan, Y.; Zilberman, I.; Boaz, M.; Landau, Z.; Glandt, M.; Jakubowicz, D.; Wainstein, J. Prevalence of undiagnosed hyperglycaemia in patients presenting to the Department of Emergency Medicine with no known history of diabetes. Int. J. Clin. Pract. 2016, 70, 771–774. [Google Scholar] [CrossRef] [PubMed]
- Gomez-Peralta, F.; Abreu, C.; Andreu-Urioste, L.; Antoli, A.C.; Rico-Fontsare, C.; Martin-Fernandez, D.; Resina-Rufes, R.; Pérez-García, J.J.; Negrete-Muñoz, Á.; Muñoz-Álvarez, D.; et al. Point-of-care capillary HbA1c measurement in the emergency department: A useful tool to detect unrecognized and uncontrolled diabetes. Int. J. Emerg. Med. 2016, 9, 7. [Google Scholar] [CrossRef] [PubMed]
- Manley, S.E.; O’Brien, K.T.; Quinlan, D.; Round, R.A.; Nightingale, P.G.; Ali, F.; Durrani, B.K.; Liew, A.; Luzio, S.D.; Stratton, I.M.; et al. Can HbA1c detect undiagnosed diabetes in acute medical hospital admissions? Diabetes Res. Clin. Pract. 2016, 115, 106–114. [Google Scholar] [CrossRef]
- Dall, T.M.; Narayan, K.V.; Gillespie, K.B.; Gallo, P.D.; Blanchard, T.D.; Solcan, M.; O’Grady, M.; Quick, W.W. Detecting type 2 diabetes and prediabetes among asymptomatic adults in the United States: Modeling American Diabetes Association versus US Preventive Services Task Force diabetes screening guidelines. Popul. Health Metr. 2014, 12, 12. [Google Scholar] [CrossRef]
- Simmons, D.; Laughton, S. Diabetes detection on the surgical wards in an area with a high prevalence of diabetes. N. Z. Med. J. 1993, 106, 156–157. [Google Scholar]
- AIHW. Diabetes Snapshot, Type 2 Diabetes Canberra: Australian Institute of Health and Welfare. 2018. Available online: https://www.aihw.gov.au/reports/diabetes/diabetes-snapshot/contents/how-many-australians-have-diabetes/type-2-diabetes (accessed on 8 March 2019).
- d’Emden, M.C.; Shaw, J.E.; Colman, P.G.; Colagiuri, S.; Twigg, S.M.; Jones, G.R.; Goodall, I.; Schneider, H.G.; Cheung, N.W. The role of HbA. Med. J. Aust. 2012, 197, 220–221. [Google Scholar]
- NDSS. Available online: https://map.ndss.com.au/#/ (accessed on 24 November 2019).
- Nathan, D.M.; Davidson, M.B.; DeFronzo, R.A.; Heine, R.J.; Henry, R.R.; Pratley, R.; Zinman, B. Impaired fasting glucose and impaired glucose tolerance: Implications for care. Diabetes Care 2007, 30, 753–759. [Google Scholar] [CrossRef]
- Dunbar, J.A.; Colagiuri, S.; Reddy, P.; Vita, P.; Timoshanko, A.; Audehm, R.; Milat, A. Scaling up type 2 diabetes prevention programs: National and state interventions in Australia. In Diabetes Prevention in Practice; Schwarz , P., Reddy, P., Greaves, C., Dunbar, J., Schwarz, J., Eds.; Tumaini Institute for Prevention Management: Dresden, Germany, 2010; Available online: https://pdfs.semanticscholar.org/00b1/c3763be6ee2f8882ebbf076f53e8e4801eea.pdf. (accessed on 3 March 2019).
- NSW Government. NSW Action for Diabetes Prevention: What Health Professionals and Health Services Can Do; NSW Ministry of Health: Sydney, Australia, 2016; pp. 1–59.
- Ginde, A.A.; Savaser, D.J.; Camargo, C.A., Jr. Limited communication and management of emergency department hyperglycemia in hospitalized patients. J. Hosp. Med. 2009, 4, 45–49. [Google Scholar] [CrossRef]
- van Veggel, K.M.; Kruithof, M.K.; Roelandse-Koop, E.; Eekhoff, E.M.; Nanayakkara, P.W. Follow-up of patients with hyperglycemia in the emergency department without a history of diabetes mellitus. Eur. J. Intern. Med. 2014, 25, 909–913. [Google Scholar] [CrossRef]
- Tsopra, R.; Wyatt, J.C.; Beirne, P.; Rodger, K.; Callister, M.; Ghosh, D.; Clifton, I.J.; Whitaker, P.; Peckham, D. Level of accuracy of diagnoses recorded in discharge summaries: A cohort study in three respiratory wards. J. Eval. Clin. Pract. 2019, 25, 36–43. [Google Scholar] [CrossRef] [PubMed]
- International Expert Committee report on the role of the A1C assay in the diagnosis of diabetes. Diabetes Care 2009, 32, 1327–1334. [CrossRef] [PubMed]
- Manley, S. Haemoglobin A1c–a marker for complications of type 2 diabetes: The experience from the UK Prospective Diabetes Study (UKPDS). Clin. Chem. Lab. Med. 2003, 41, 1182–1190. [Google Scholar] [CrossRef] [PubMed]
- Klompas, M.; Eggleston, E.; McVetta, J.; Lazarus, R.; Li, L.; Platt, R. Automated Detection and Classification of Type 1 Versus Type 2 Diabetes Using Electronic Health Record Data. Diabetes Care 2013, 36, 914. [Google Scholar] [CrossRef]
- Lee, M.H.; Liprino, L.; Brooks, J.; Cayzer, B.; Weedon, F.; Bermingham, K.; Jenkins, A.J.; Rowley, K.; O’Neal, D.N. Factors associated with duration of inpatient hospital stay for patients with diabetes mellitus admitted to a medical unit in a community public hospital. Aust. J. Prim. Health 2017, 23, 23–30. [Google Scholar] [CrossRef]
- Baker, S.T.; Chiang, C.Y.; Zajac, J.D.; Bach, L.A.; Jerums, G.; MacIsaac, R.J. Outcomes for general medical inpatients with diabetes mellitus and new hyperglycaemia. Med. J. Aust. 2008, 188, 340–343. [Google Scholar] [CrossRef]
- Mata-Cases, M.; Casajuana, M.; Franch-Nadal, J.; Casellas, A.; Castell, C.; Vinagre, I.; Mauricio, D.; Bolíbar, B. Direct medical costs attributable to type 2 diabetes mellitus: A population-based study in Catalonia, Spain. Eur. J. Health Econ. 2016, 17, 1001–1010. [Google Scholar] [CrossRef]
- Simmons, D.; Yu, D.; Wenzel, H. Changes in hospital admissions and inpatient tariff associated with a Diabetes Integrated Care Initiative: Preliminary findings. J. Diabetes 2014, 6, 81–89. [Google Scholar] [CrossRef]
- Karahalios, A.; Somarajah, G.; Hamblin, P.S.; Karunajeewa, H.; Janus, E.D. Quantifying the hidden healthcare cost of diabetes mellitus in Australian hospital patients. Internal Med. J. 2018, 48, 286–292. [Google Scholar] [CrossRef]
- Astell-Burt, T.; Feng, X.; Kolt, G.S.; McLean, M.; Maberly, G. Understanding geographical inequities in diabetes: Multilevel evidence from 114,755 adults in Sydney, Australia. Diabetes Res. Clin. Pract. 2014, 106, e68–e73. [Google Scholar] [CrossRef]
- George, P.; Valabhji, J.; Dawood, M.; Henry, J. Screening for type 2 diabetes in the accident and emergency department. Diabetic Med. 2005, 22, 1766–1769. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Frequency/Values |
|---|---|
| Age at admission, (mean ± Standard deviation SD) years | 74.6 ± 8.9 |
| Gender, (n, %) | |
| Male | 449 (51.1) |
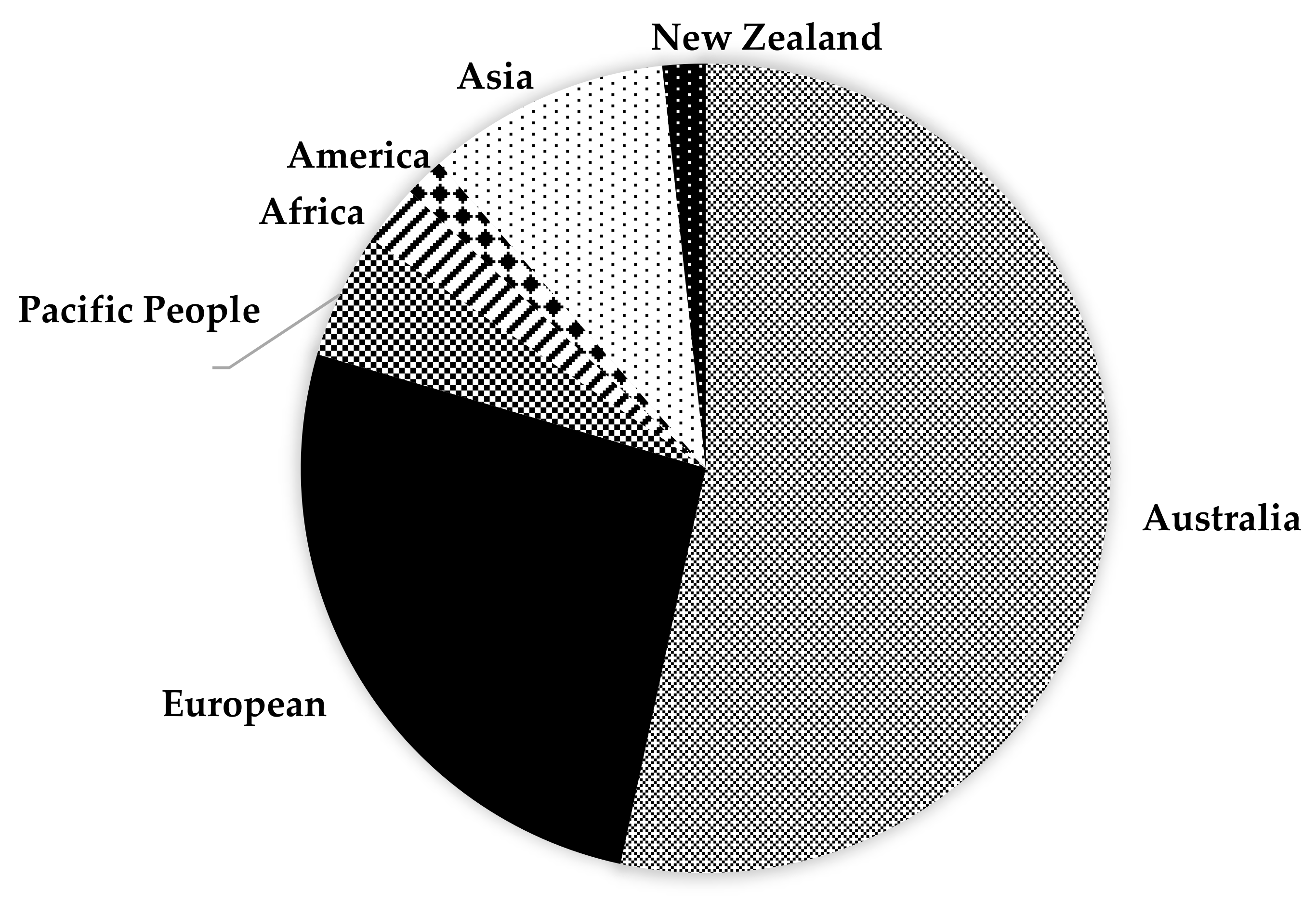
| Country of birth, n (%) | |
| Australia | 467 (53.1) |
| Overseas | 408 (46.4) |
| Diabetes type, n (%) | |
| Type 1 diabetes | 12 (1.4) |
| Type 2 diabetes | 863 (98.2) |
| Other types | 4 (0.4) |
| Body mass index (mean ± SD), kg/m2 | 30.5 ± 7.0 |
| Obesity (≥30 kg/m2) | 238 (47.7) |
| Weight (mean ± SD), kg (n = 522) | 83.8 (20.1) |
| Blood glucose testing | |
| HbA1c done, n (%) | 137 (15.6) |
| Mean ± SD %, mmol/mol | 8.0 ± 1.9, 63.5 ± 20.8 |
| HbA1c > 7%, n (%) α | 85 (62.0) |
| Random Blood Glucose (RBG) done, n (%) (Laboratory RBG/finger prick RBG) | 824 (93.7)/633(70.0) |
| Mean ±SD lab RBG/finger prick RBG, in mmol/L | 9.8 ± 5.2/10.1 ± 4.7 |
| Laboratory, finger prick RBG > 11 mmol/L, n (%) | 193 (23.4), 158 (25.0) |
| Blood pressure (mean ± SD), mmHg | |
| Systolic | 140 (26) |
| Diastolic | 76 (13) |
| BP >130/80, n (%) | 576 (65.5) |
| Length of stay, (mean ± SD) days | 6.7 ± 25.4, range 0–370 |
| >1 day | 556 (63.3%) |
| Arrival by emergency medical service (ambulance) | 558 (63.5%) |
| From nursing home or long-term care facility, % | 94 (10.7) |
| Transfer to critical care unit | 150 (17.1%) |
| Diabetes management, n (%) ƛ | |
| Monotherapy (one treatment) | 300 (34.1) |
| Combination therapy (>one treatment) | 391 (44.5) |
| No medication | 188 (21.4) |
| Medication type | |
| Insulin alone | 241 (27.4) |
| Metformin alone | 489 (55.6) |
| Insulin and metformin | 103 (11.7) |
| Other oral hypoglycaemic agents | 349 (39.7) |
| Sulfonylureas | 201 (22.9) |
| DPP4 inhibitors | 182 (20.7) |
| SGLT2 inhibitors | 64 (7.3) |
| Source of referral to ED | |
| Self/family/friends | 608 (69.2) |
| Medical practitioner (General Practitioner GP/Dentist) | 127 (14.4) |
| Other facilities | 144 (16.4) |
| Mode of transport to ED | |
| Ambulance | 564 (64.2) |
| Private car/others | 261 (29.7) |
| No transport | 54 (6.1) |
| Parameter | Frequency (%) |
|---|---|
| Any diabetes-related note | 171 (20.4) |
| Changes to diabetic medications during admission noted | 109 (13.0) |
| Abnormal blood glucose result noted | 104 (12.4) |
| Request for GP and/or patient to monitor blood sugar level | 68 (8.1) |
| Request for GP to refer patient for HbA1c test | 6 (0.7) |
| Request for GP to follow-up HbA1c result | 1 (0.1) |
| Request for GP to review patient’s diabetes medications | 38 (4.5) |
| Consultation by diabetes educator during admission noted | 21 (2.5) |
| Current HbA1c test result noted | 20 (2.4) |
| Previous HbA1c test result noted | 8 (1.0) |
| Changes to management of diabetes during admission noted | 7 (0.8) |
| Ketosis during admission noted | 3 (0.4) |
| Request for patient to follow-up with endocrinologist noted | 53 (6.3) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Levi, O.U.; Webb, F.; Simmons, D. Diabetes Detection and Communication among Patients Admitted through the Emergency Department of a Public Hospital. Int. J. Environ. Res. Public Health 2020, 17, 980. https://doi.org/10.3390/ijerph17030980
Levi OU, Webb F, Simmons D. Diabetes Detection and Communication among Patients Admitted through the Emergency Department of a Public Hospital. International Journal of Environmental Research and Public Health. 2020; 17(3):980. https://doi.org/10.3390/ijerph17030980
Chicago/Turabian StyleLevi, Osuagwu Uchechukwu, Frederick Webb, and David Simmons. 2020. "Diabetes Detection and Communication among Patients Admitted through the Emergency Department of a Public Hospital" International Journal of Environmental Research and Public Health 17, no. 3: 980. https://doi.org/10.3390/ijerph17030980
APA StyleLevi, O. U., Webb, F., & Simmons, D. (2020). Diabetes Detection and Communication among Patients Admitted through the Emergency Department of a Public Hospital. International Journal of Environmental Research and Public Health, 17(3), 980. https://doi.org/10.3390/ijerph17030980