Improving Screening Uptake among Breast Cancer Survivors and Their First-Degree Relatives at Elevated Risk to Breast Cancer: Results and Implications of a Randomized Study in the State of Georgia


 ,
,
Abstract
1. Introduction
2. Materials and Methods
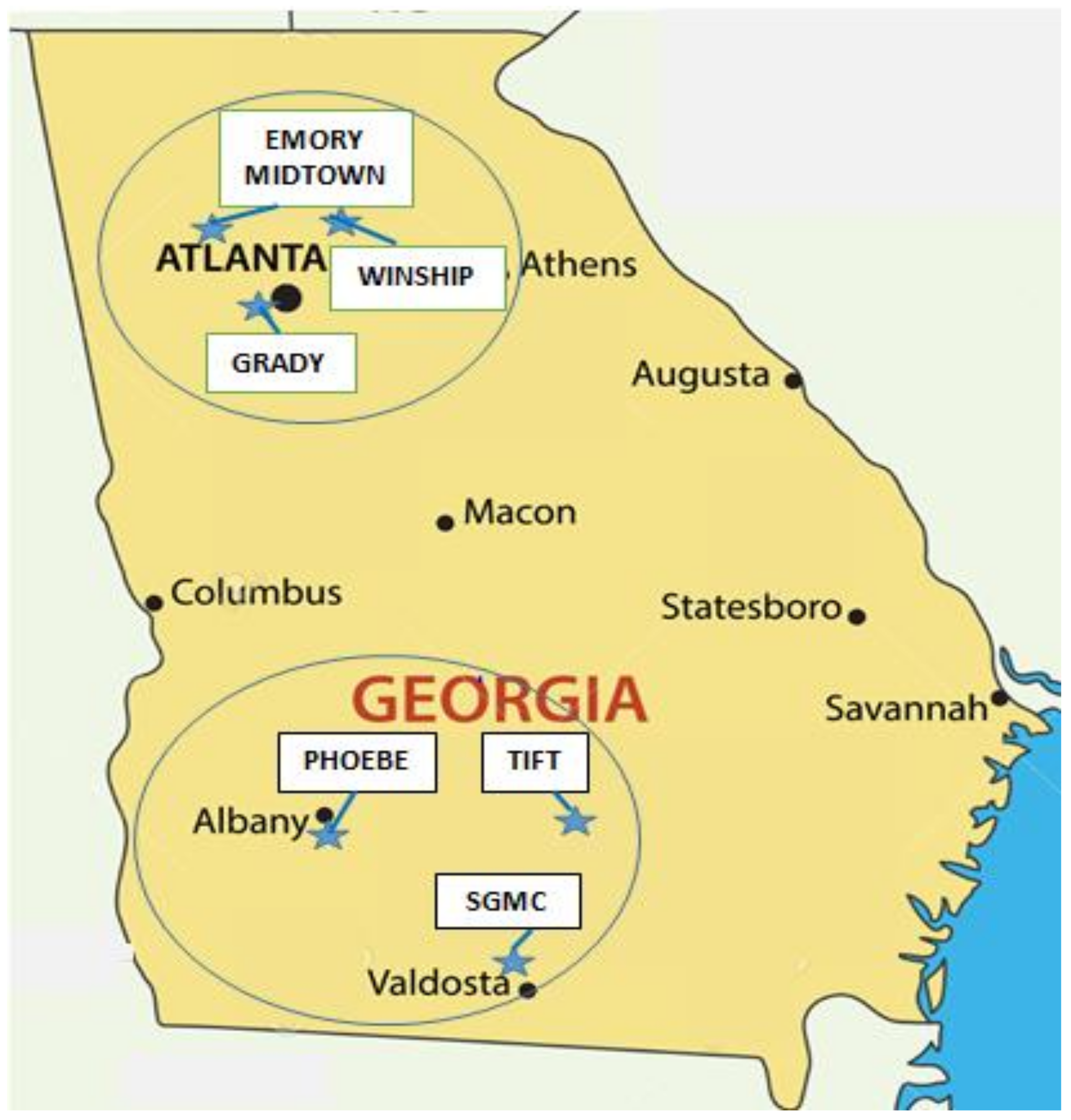
2.1. Study Participants
2.2. Interventions
- The educational brochure was sent to each study participant by mail, typically within a week of randomization.
- A half-hour tailored telephone counseling session was conducted by a member of the study outreach team, in which the importance of breast cancer screening was emphasized, the woman’s “readiness for change” to engage in appropriate screening was evaluated [21], financial and physical barriers to screening were assessed, and recommendations for positive actions were developed and communicated. Additionally, each breast cancer survivor was urged to encourage her female FDRs to “talk with your doctor about… having regular breast screening tests…”. A written version of the telephone counseling script was subsequently mailed to the survivor, along with a separate note encouraging breast cancer screening.
- For study participants able and willing to identify a primary care provider, that PCP was mailed a packet containing the following: (1) a cover letter describing the study and notifying the PCP that a named study participant (who currently was not adherent to breast cancer screening recommendations) was a member of his/her practice; (2) a letter of support―signed by the presidents of the Georgia Chapter of the American College of Physicians, the Georgia Academy of Family Physicians, and the Georgia Chapter of the American College of Obstetrics and Gynecology, as well as by the medical director of the Cancer Coalition of South Georgia―that encouraged the PCP to note their patient’s elevated risk status in her medical record and engage in appropriate screening and follow-up; and (3) a “pink reminder form” with the study participant’s name and screening status for inclusion in her medical record.
2.3. Statistical Analyses
3. Results
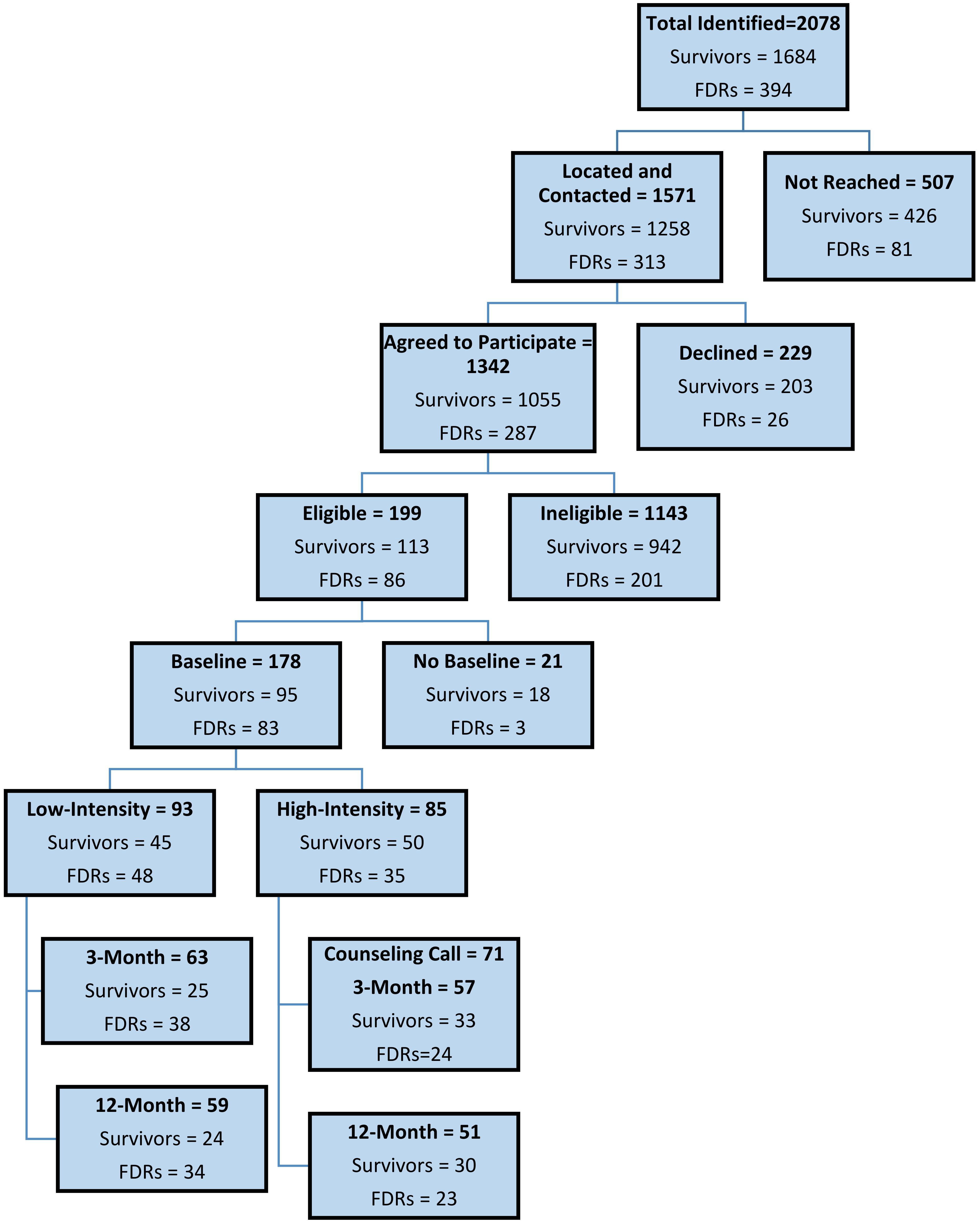
3.1. Study Enrollment and Retention
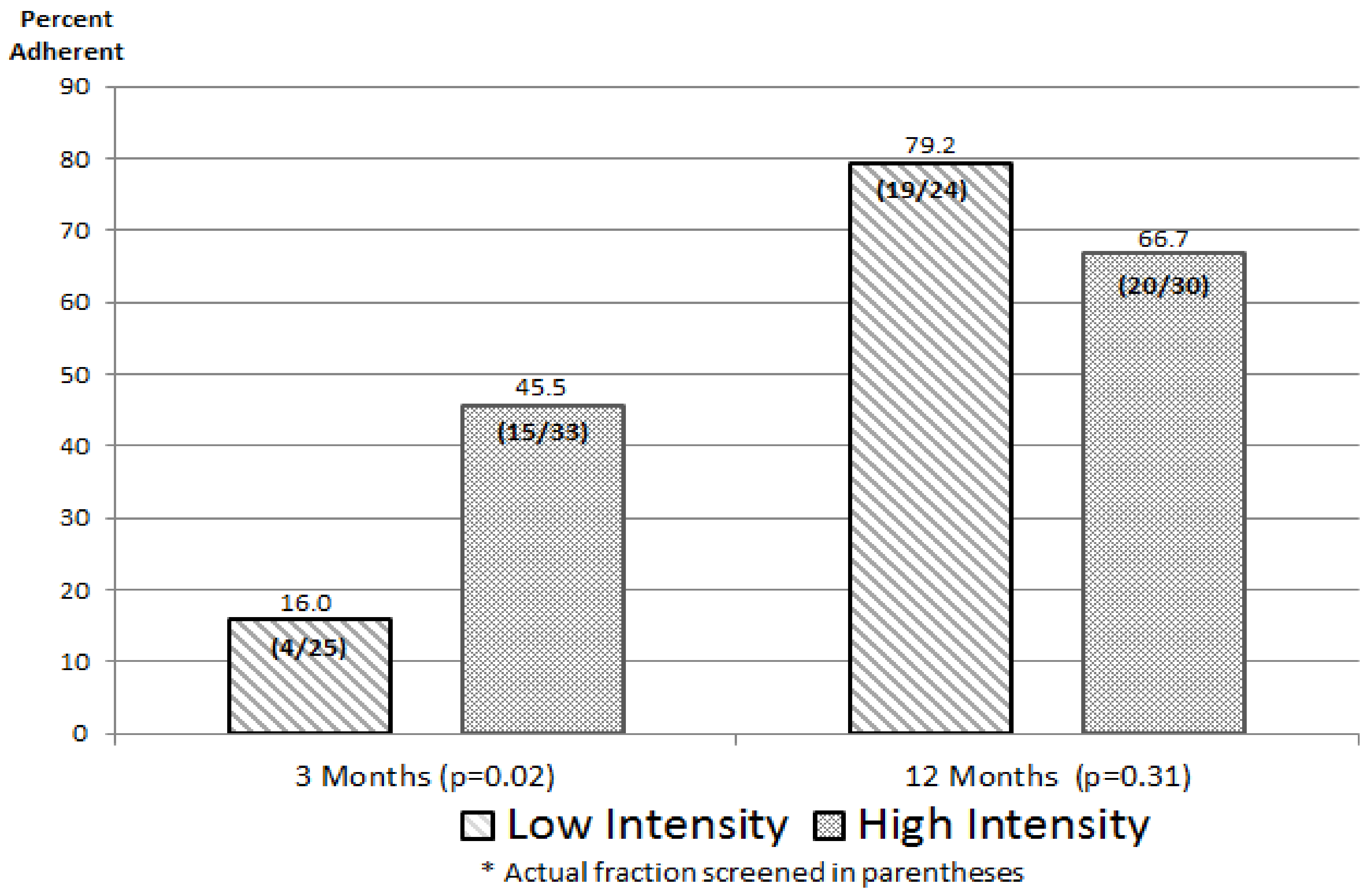
3.2. Intervention Impact
4. Discussion
4.1. Appraisal of Findings
4.2. Study Limitations
5. Implications for Improving Adherence to Breast Cancer Screening
Recommendations
6. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Note
References
- American Cancer Society. Breast Cancer Facts & Figures 2015–2016; American Cancer Society: Atlanta, GA, USA, 2015. [Google Scholar]
- Silverman, B.G.; Lipshitz, I.; Keinan-Boker, L. Second Primary Cancers After Primary Breast Cancer Diagnosis in Israeli Women, 1992 to 2006. J. Glob. Oncol. 2017, 3, 135–142. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.-D.; Chen, S.-C.; Chan, C.H.; Lu, C.-H.; Chen, C.-C.; Lin, J.-T.; Chen, M.-F.; Huang, S.-H.; Yeh, C.-M.; Chen, M.-C. Increased Risk for Second Primary Malignancies in Women with Breast Cancer Diagnosed at Young Age: A Population-Based Study in Taiwan. Cancer Epidemiol. Biomark. Prev. 2008, 17, 2647–2655. [Google Scholar] [CrossRef] [PubMed][Green Version]
- De Bock, G.H.; van der Hage, J.A.; Putter, H.; Bonnema, J.; Bartelink, H.; van de Velde, C.J. Isolated loco-regional recurrence of breast cancer is more common in young patients and following breast conserving surgery. Long-term results of European Organisation for Research and Treatment of Cancer studies. Eur. J. Cancer 2006, 42, 351–356. [Google Scholar] [CrossRef] [PubMed]
- Jobsen, J.J.; Van Der Palen, J.; Ong, F.; Meerwaldt, J.H. Synchronous, bilateral breast cancer: Prognostic value and incidence. Breast 2003, 12, 83–88. [Google Scholar] [CrossRef]
- U.S. Centers for Disease Control and Prevention. Breast Cancer in Young Women. Available online: https://www.cdc.gov/cancer/breast/young_women/bringyourbrave/pdf/BreastCancerYoungWomenFactSheet.pdf (accessed on 18 December 2019).
- Singletary, S.E. Rating the Risk Factors for Breast Cancer. Ann. Surg. 2003, 237, 474–482. [Google Scholar] [CrossRef]
- Bastani, R.; Maxwell, A.E.; Bradford, C.; Das, I.P.; Yan, K.X. Tailored Risk Notification for Women with a Family History of Breast Cancer. Prev. Med. 1999, 29, 355–364. [Google Scholar] [CrossRef]
- Katapodi, M.C.; Duquette, D.; Yang, J.J.; Mendelsohn-Victor, K.; Anderson, B.; Nikolaidis, C.; Mancewicz, E.; Northouse, L.L.; Duffy, S.; Ronis, D.; et al. Recruiting families at risk for hereditary breast and ovarian cancer from a statewide cancer registry: A methodological study. Cancer Causes Control 2017, 28, 191–201. [Google Scholar] [CrossRef]
- Glanz, K.; Steffen, A.D.; Taglialatela, L.A. Effects of Colon Cancer Risk Counseling for First-Degree Relatives. Cancer Epidemiol. Biomark. Prev. 2007, 16, 1485–1491. [Google Scholar] [CrossRef]
- Hewitt, M.; Greenfield, S.; Stovall, E. From Cancer Patient to Cancer Survivor: Lost in Transition; National Academy Press: Washington, DC, USA, 2006. [Google Scholar]
- Mayer, D.K.; Nekhlyudov, L.; Snyder, C.F.; Merrill, J.K.; Wollins, D.S.; Shulman, L.N. American Society of Clinical Oncology Clinical Expert Statement on Cancer Survivorship Care Planning. J. Oncol. Pr. 2014, 10, 345–351. [Google Scholar] [CrossRef]
- Journey Forward. About Journey Forward. Available online: http://www.journeyforward.org/about-journey-forward (accessed on 15 November 2019).
- LIVESTRONG. Your Survivorship Care Plan. Available online: https://www.livestrong.org/we-can-help/healthy-living-after-treatment/your-survivorship-care-plan?gclid = EAIaIQobChMIu7zbl8Dw5QIVj5OzCh15ewI6EAAYASAAEgKiV_D_BwE (accessed on 14 November 2019).
- Commission on Cancer of the American College of Surgeons. Optimal Resources for Cancer Care: 2020 Standards. Available online: https://www.facs.org/quality-programs/cancer/coc/2020-standards (accessed on 18 December 2019).
- American Society of Clinical Oncology. Survivorship Care Planning Tools, ASCO’s Survivorship Care Plan Template (Breast Cancer). Available online: https://www.asco.org/practice-guidelines/cancer-care-initiatives/prevention-survivorship/survivorship-compendium (accessed on 15 November 2019).
- Journey Forward. Cancer Survivorship Care Plan for Breast Cancer. Available online: https://www.journeyforward.org/sites/journeyforward/files/sample-care-plan_breast-cancer.pdf (accessed on 16 November 2019).
- OncoLife Survivorship Care Plan (Penn Medicine). OncoLife Care Plan (Breast Cancer). Available online: https://oncolife.oncolink.org/report/oncolife_report/?ck=d6d4058bb6 (accessed on 13 November 2019).
- National Comprehensive Cancer Network (NCCN). Breast Cancer Screening and Diagnosis, Version 1.2019 (Screening or Symptom Category: Increased Risk). Available online: https://www2.tri-kobe.org/nccn/guideline/breast/english/breast-screening.pdf (accessed on 18 December 2019).
- U.S. Centers for Disease Control and Prevention; National Center for Chronic Disease Prevention and Health Promotion; Division of Cancer Prevention and Control. Breast Cancer: What You Need to Know. Available online: https://www.cdc.gov/cancer/breast/pdf/breastcancerfactsheet.pdf (accessed on 14 November 2019).
- Prochaska, J.O.; Velicer, W.F. The transtheoretical model of health behavior change. Am. J. Heal. Promot. 1997, 12, 38–48. [Google Scholar] [CrossRef]
- Harrell, F.E., Jr. Regression Modeling Strategies, with Applications to Linear Models, Logistic Regression, and Survival Analysis; Springer Series in Statistics; Springer-Verlag: New York, NY, USA, 2001. [Google Scholar]
- Smith, R.A. Risk-based screening for breast cancer: Is there a practical strategy? Semin. Breast Dis. 1999, 2, 280–291. [Google Scholar]
- Carpentier, M.Y.; Tiro, J.A.; Savas, L.S.; Bartholomew, L.K.; Melhado, T.V.; Coan, S.P.; Argenbright, K.E.; Vernon, S.W. Are cancer registries a viable tool for cancer survivor outreach? Feasibility Stud. J. Cancer Surviv. 2013, 7, 155–163. [Google Scholar] [CrossRef] [PubMed]
- Lowery, J.T.; Axell, L.; Vu, K.; Rycroft, R. A novel approach to increase awareness about hereditary colon cancer using a state cancer registry. Genet. Med. 2010, 12, 721–725. [Google Scholar] [CrossRef] [PubMed]
- Jepson, R.G.; Harris, F.M.; Platt, S.; Tannahill, C. The effectiveness of interventions to change six health behaviors: A review of reviews. BMC Public Health 2010, 10, 538. [Google Scholar] [CrossRef] [PubMed]
- Clarke, T.C.; Soler-Vila, H.; Fleming, L.E.; Christ, S.L.; Lee, D.J.; Arheart, K.L. Trends in adherence to recommended cancer screening; The U.S. population and working cancer survivors. Front. Oncol. 2012, 2, 1–13. [Google Scholar] [CrossRef] [PubMed]
- American Cancer Society. Cancer Prevention & Early Detection Facts & Figures 2017–2018; American Cancer Society: Atlanta, GA, USA, 2017. [Google Scholar]
- Yabroff, K.R.; Mandelblatt, J.S. Interventions targeted toward patients to increase mammography use. Cancer Epidemiol. Biomark. Prev. 1999, 8, 749–757. [Google Scholar]
- Mandelblatt, J.S.; Yabroff, K.R. Effectiveness of interventions designed to increase mammography use: A meta-analysis of provider-targeted strategies. Cancer Epidemiol. Biomark. Prev. 1999, 8, 759–767. [Google Scholar]
- Howard, M.; Agarwal, G.; Lytwyn, A. Accuracy of self-reports of Pap and mammography screening compared with medical record: A meta-analysis. Cancer Causes Control 2009, 20, 1–13. [Google Scholar] [CrossRef]
- Rauscher, G.H.; Johnson, T.P.; Cho, Y.I.; Walk, J.A. Accuracy of Self-Reported Cancer-Screening Histories: A Meta-analysis. Cancer Epidemiol. Biomark. Prev. 2008, 17, 748–757. [Google Scholar] [CrossRef]
- Cronin, K.A.; Miglioretti, D.L.; Krapcho, M.; Yu, B.; Geller, B.M.; Carney, P.A.; Onega, T.; Feuer, E.J.; Breen, N.; Ballard-Barbash, R. Bias associated with self-report of prior screening mammography. Cancer Epidemiol. Biomark. Prev. 2009, 18, 1699–1705. [Google Scholar] [CrossRef]
- Tiro, J.A.; Sanders, J.M.; Shay, L.A.; Murphy, C.C.; Hamann, H.A.; Bartholomew, L.K.; Savas, L.S.; Vernon, S.W. Validation of self-reported post-treatment mammography surveillance among breast cancer survivors by electronic medical record extraction method. Breast Cancer Res. Treat. 2015, 151, 427–434. [Google Scholar] [CrossRef] [PubMed]
- Mayer, D.K.; Deal, A.M.; Crane, J.M.; Chen, R.C.; Asher, G.N.; Hanson, L.C.; Wheeler, S.B.; Gerstel, A.; Green, M.A.; Birken, S.A.; et al. Using Survivorship Care Plans to Enhance Communication and Cancer Care Coordination: Results of a Pilot Study. Oncol. Nurs. Forum 2016, 43, 636–645. [Google Scholar] [CrossRef] [PubMed]
- Ezendam, N.P.M.; Nicolaije, K.A.H.; Kruitwagen, R.F.P.M.; Pijnenborg, J.M.A.; Vos, M.C.; Boll, D.; Van Bommel, M.; Van De Poll-Franse, L.V. Survivorship Care Plans to inform the primary care physician: Results from the ROGY care pragmatic cluster randomized controlled trial. J. Cancer Surviv. 2014, 8, 595–602. [Google Scholar] [CrossRef] [PubMed]
- Whelan, S.L. International Association of Cancer Registries (IACR) Newsletter. Cancer Causes Control 1997, 8, 111–121. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Level | Intervention Group | |||
|---|---|---|---|---|---|
| Sample Totals a | Low-Intensity a N = 45 | High-Intensity a N = 50 | p-Value * | ||
| Age | ≤45 years | 19 (20.0) | 10 (22.2) | 9 (18.0) | 0.673 |
| 46−55 years | 51 (53.7) | 22 (48.9) | 29 (58.0) | ||
| ≥56 years | 25 (26.7) | 13 (28.9) | 12 (24.0) | ||
| Race/ethnicity | White | 33 (35.1) | 16 (35.6) | 17 (34.7) | 0.022 |
| Black | 49 (52.1) | 19 (42.2) | 30 (61.2) | ||
| Other | 12 (12.8) | 10 (22.2) | 2 (4.1) | ||
| Marital status | Married/partnership | 49 (52.1) | 22 (48.9) | 27 (55.1) | 0.547 |
| Other | 45 (47.9) | 23 (51.1) | 22 (44.9) | ||
| Education level (highest grade completed) | College or post-grad | 45 (48.4) | 23 (52.3) | 22 (44.9) | 0.477 |
| Other | 48 (51.6) | 21 (47.7) | 27 (55.1) | ||
| Employment status | Working (FT/PT) | 55 (59.1) | 29 (65.9) | 26 (53.1) | 0.208 |
| Other | 38 (40.9) | 15 (34.1) | 23 (46.9) | ||
| Annual family income | <$50,000 | 43 (45.7) | 18 (40.0) | 25 (51.0) | 0.110 |
| ≥$50,000 | 36 (38.3) | 22 (48.9) | 14 (28.6) | ||
| Refused/DK | 15 (16.0) | 5 (11.1) | 10 (20.4) | ||
| Health insurance status b | Private | 54 (59.3) | 28 (65.1) | 26 (54.2) | 0.537 |
| Public | 16 (17.6) | 7 (16.3) | 9 (18.8) | ||
| Uninsured | 21 (23.1) | 8 (18.6) | 13 (27.0) | ||
| SEER Summary Stage c | In Situ | 22 (23.1) | 11 (24.4) | 11 (22.0) | 0.874 |
| Localized | 47 (49.5) | 21 (46.7) | 26 (52.0) | ||
| Regional | 26 (27.4) | 13 (28.9) | 13 (26.0) | ||
| Year of Diagnosis | 2000−2002 | 28 (29.5) | 11 (24.4) | 17 (34.0) | 0.486 |
| 2003−2006 | 38 (40.0) | 18 (40.0) | 20 (40.0) | ||
| 2007−2009 | 29 (30.5) | 16 (35.6) | 13 (26.0) | ||
| Intervention Group | |||||
|---|---|---|---|---|---|
| Characteristics | Level | Sample Totals a | Low-Intensity a N = 48 | High-Intensity a N = 35 | p-Value * |
| Age | ≤45 years | 52 (62.7) | 31 (64.6) | 21 (60.0) | 0.646 |
| 46−55 years | 13 (15.6) | 6 (12.5) | 7 (20.0) | ||
| ≥56 years | 18 (21.7) | 11 (22.9) | 7 (20.0) | ||
| Race/ethnicity | White | 39 (47.5) | 22 (45.8) | 17 (50.0) | 0.330 |
| Black | 40 (48.8) | 23 (47.9) | 17 (50.0) | ||
| Other | 3 (3.7) | 3 (6.3) | 0 (0.0) | ||
| Marital status | Married/partnership | 32 (39.5) | 20 (41.7) | 12 (36.4) | 0.631 |
| Other | 49 (60.5) | 28 (58.3) | 21 (63.6) | ||
| Education level (highest grade completed) | College or post-grad | 41 (50.0) | 23 (47.9) | 18 (47.1) | 0.939 |
| Other | 41 (50.0) | 25 (52.1) | 16 (52.9) | ||
| Employment status | Working (FT/PT) | 53 (66.3) | 29 (61.7) | 24 (72.7) | 0.305 |
| Other | 27 (33.7) | 18 (38.3) | 9 (27.3) | ||
| Annual family income | <$50,000 | 36 (43.9) | 21 (43.8) | 15 (44.1) | 0.289 |
| ≥$50,000 | 39 (47.6) | 21 (43.8) | 18 (53.0) | ||
| Refused/DK | 7 (8.5) | 6 (12.4) | 1 (2.9) | ||
| Health insurance status b | Private | 47 (57.3) | 27 (57.4) | 20 (57.1) | 0.614 |
| Public | 15 (18.3) | 10 (21.3) | 5 (14.3) | ||
| Uninsured | 20 (24.4) | 10 (21.3) | 10 (28.6) | ||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lipscomb, J.; Escoffery, C.; Gillespie, T.W.; Henley, S.J.; Smith, R.A.; Chociemski, T.; Almon, L.; Jiang, R.; Sheng, X.; Goodman, M.; et al. Improving Screening Uptake among Breast Cancer Survivors and Their First-Degree Relatives at Elevated Risk to Breast Cancer: Results and Implications of a Randomized Study in the State of Georgia. Int. J. Environ. Res. Public Health 2020, 17, 977. https://doi.org/10.3390/ijerph17030977
Lipscomb J, Escoffery C, Gillespie TW, Henley SJ, Smith RA, Chociemski T, Almon L, Jiang R, Sheng X, Goodman M, et al. Improving Screening Uptake among Breast Cancer Survivors and Their First-Degree Relatives at Elevated Risk to Breast Cancer: Results and Implications of a Randomized Study in the State of Georgia. International Journal of Environmental Research and Public Health. 2020; 17(3):977. https://doi.org/10.3390/ijerph17030977
Chicago/Turabian StyleLipscomb, Joseph, Cam Escoffery, Theresa W. Gillespie, S. Jane Henley, Robert A. Smith, Toni Chociemski, Lyn Almon, Renjian Jiang, Xi Sheng, Michael Goodman, and et al. 2020. "Improving Screening Uptake among Breast Cancer Survivors and Their First-Degree Relatives at Elevated Risk to Breast Cancer: Results and Implications of a Randomized Study in the State of Georgia" International Journal of Environmental Research and Public Health 17, no. 3: 977. https://doi.org/10.3390/ijerph17030977
APA StyleLipscomb, J., Escoffery, C., Gillespie, T. W., Henley, S. J., Smith, R. A., Chociemski, T., Almon, L., Jiang, R., Sheng, X., Goodman, M., & Ward, K. C. (2020). Improving Screening Uptake among Breast Cancer Survivors and Their First-Degree Relatives at Elevated Risk to Breast Cancer: Results and Implications of a Randomized Study in the State of Georgia. International Journal of Environmental Research and Public Health, 17(3), 977. https://doi.org/10.3390/ijerph17030977