Active Commuting and Depression Symptoms in Adults: A Systematic Review

 ,
,  ,
,  ,
, 
 and
and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Inclusion Criteria
2.2. Search Strategy
2.3. Data Extraction and Harmonisation
2.4. Study Quality and Risk of Bias
2.5. Synthesis of Results
3. Results
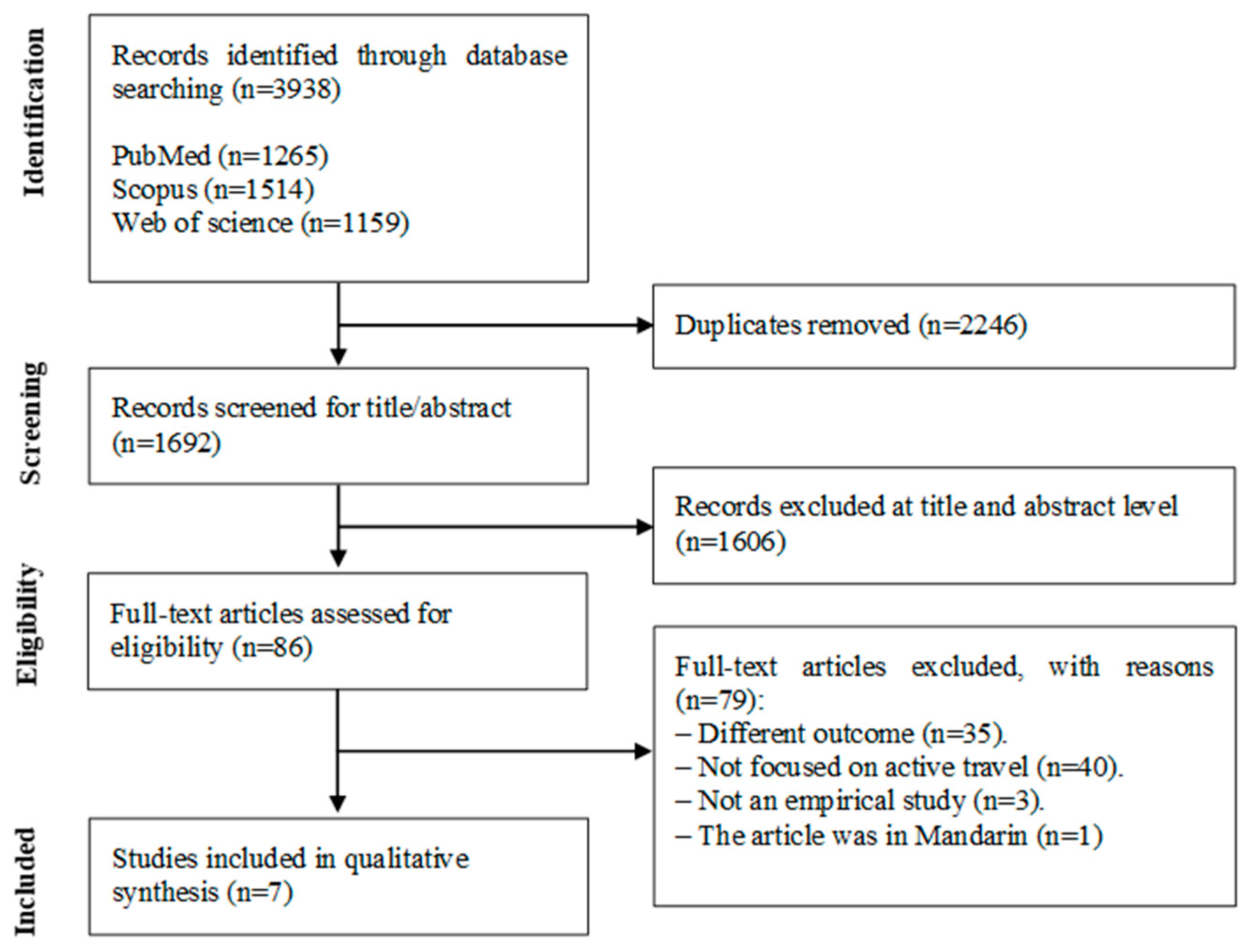
3.1. Search Results
3.2. Study Characteristics
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- WHO. Depression and Other Common Mental Disorders. Global Health Estimates; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- Chapman, D.P.; Perry, G.S. Depression as a major component of public health for older adults. Prev. Chronic Dis. 2008, 5, A22. [Google Scholar] [PubMed]
- Vancampfort, D.; Correll, C.U.; Galling, B.; Probst, M.; De Hert, M.; Ward, P.B.; Rosenbaum, S.; Gaughran, F.; Lally, J.; Stubbs, B. Diabetes mellitus in people with schizophrenia, bipolar disorder and major depressive disorder: A systematic review and large scale meta-analysis. World Psychiatry 2016, 15, 166–174. [Google Scholar] [CrossRef] [PubMed]
- Ferrari, A.J.; Charlson, F.J.; Norman, R.E.; Patten, S.B.; Freedman, G.; Murray, C.J.; Vos, T.; Whiteford, H.A. Burden of depressive disorders by country, sex, age, and year: Findings from the global burden of disease study 2010. PLoS Med. 2013, 10, e1001547. [Google Scholar] [CrossRef] [PubMed]
- Walker, E.R.; McGee, R.E.; Druss, B.G. Mortality in mental disorders and global disease burden implications: A systematic review and meta-analysis. JAMA Psychiatry 2015, 72, 334–341. [Google Scholar] [CrossRef] [PubMed]
- Karyotaki, E.; Smit, Y.; Holdt Henningsen, K.; Huibers, M.J.; Robays, J.; de Beurs, D.; Cuijpers, P. Combining pharmacotherapy and psychotherapy or monotherapy for major depression? A meta-analysis on the long-term effects. J. Affect. Disord. 2016, 194, 144–152. [Google Scholar] [CrossRef] [PubMed]
- Khan, A.; Faucett, J.; Lichtenberg, P.; Kirsch, I.; Brown, W.A. A systematic review of comparative efficacy of treatments and controls for depression. PLoS ONE 2012, 7, e41778. [Google Scholar] [CrossRef]
- Olfson, M.; Amos, T.B.; Benson, C.; McRae, J.; Marcus, S.C. Prospective service use and health care costs of Medicaid beneficiaries with treatment-resistant depression. J. Manag. Care Spec. Pharm. 2018, 24, 226–236. [Google Scholar] [CrossRef]
- Schuch, F.B.; Vancampfort, D.; Firth, J.; Rosenbaum, S.; Ward, P.B.; Silva, E.S.; Hallgren, M.; Ponce De Leon, A.; Dunn, A.L.; Deslandes, A.C.; et al. Physical activity and incident depression: A meta-analysis of prospective cohort studies. Am. J. Psychiatry 2018, 175, 631–648. [Google Scholar] [CrossRef]
- Rebar, A.L.; Stanton, R.; Geard, D.; Short, C.; Duncan, M.J.; Vandelanotte, C. A meta-meta-analysis of the effect of physical activity on depression and anxiety in non-clinical adult populations. Health Psychol. Rev. 2015, 9, 366–378. [Google Scholar] [CrossRef]
- Tasci, G.; Baykara, S.; Gurok, M.G.; Atmaca, M. Effect of exercise on therapeutic response in depression treatment. Psychiatry Clin. Psychopharmacol. 2019, 29, 137–143. [Google Scholar] [CrossRef]
- Sahlqvist, S.; Song, Y.; Ogilvie, D. Is active travel associated with greater physical activity? The contribution of commuting and non-commuting active travel to total physical activity in adults. Prev. Med. 2012, 55, 206–211. [Google Scholar] [CrossRef] [PubMed]
- Yang, L.; Panter, J.; Griffin, S.J.; Ogilvie, D. Associations between active commuting and physical activity in working adults: Cross-sectional results from the Commuting and Health in Cambridge study. Prev. Med. 2012, 55, 453–457. [Google Scholar] [CrossRef] [PubMed]
- Hillsdon, M.; Thorogood, M. A systematic review of physical activity promotion strategies. Br. J. Sports Med. 1996, 30, 84–89. [Google Scholar] [CrossRef] [PubMed]
- Berglund, E.; Lytsy, P.; Westerling, R. Active traveling and its associations with self-rated health, BMI and physical activity: A comparative study in the adult Swedish population. Int. J. Environ. Res. Public Health 2016, 13, 455. [Google Scholar] [CrossRef] [PubMed]
- Humphreys, D.K.; Goodman, A.; Ogilvie, D. Associations between active commuting and physical and mental wellbeing. Prev. Med. 2013, 57, 135–139. [Google Scholar] [CrossRef]
- Chapman, R.; Keall, M.; Howden-Chapman, P.; Grams, M.; Witten, K.; Randal, E.; Woodward, A. A cost benefit analysis of an active travel intervention with health and carbon emission reduction benefits. Int. J. Environ. Res. Public Health 2018, 15. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, P. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Ann. Intern. Med. 2009, 151, 264–269. [Google Scholar] [CrossRef]
- National Collaborating Centre for Methods and Tools. Quality Assessment Tool for Quantitative Studies Method. Available online: http://www.nccmt.ca/resources/search/14 (accessed on 1 July 2016).
- Smith, T.L.; Masaki, K.H.; Fong, K.; Abbott, R.D.; Ross, G.W.; Petrovitch, H.; Blanchette, P.L.; White, L.R. Effect of walking distance on 8-year incident depressive symptoms in elderly men with and without chronic disease: The Honolulu-Asia Aging Study. J. Am. Geriatr. Soc. 2010, 58, 1447–1452. [Google Scholar] [CrossRef]
- Kai, Y.; Nagamatsu, T.; Yamaguchi, Y.; Tokushima, S. Effect of leisure-time physical activity and commuting by walking on depressive symptoms among Japanese workers. Bull. Phys. Fit. Res. Inst. 2011, 109, 1–8. [Google Scholar]
- Julien, D.; Gauvin, L.; Richard, L.; Kestens, Y.; Payette, H. Longitudinal associations between walking frequency and depressive symptoms in older adults: Results from the VoisiNuAge study. J. Am. Geriatr. Soc. 2013, 61, 2072–2078. [Google Scholar] [CrossRef]
- Torres, E.R.; Sampselle, C.M.; Neighbors, H.W.; Ronis, D.L.; Gretebeck, K.A. Depressive Symptoms and Walking in African-Americans. Public Health Nurs. 2015, 32, 381–387. [Google Scholar] [CrossRef] [PubMed]
- Kuwahara, K.; Honda, T.; Nakagawa, T.; Yamamoto, S.; Akter, S.; Hayashi, T.; Mizoue, T. Associations of leisure-time, occupational, and commuting physical activity with risk of depressive symptoms among Japanese workers: A cohort study. Int. J. Behav. Nutr. Phys. Act. 2015, 12, 119. [Google Scholar] [CrossRef] [PubMed]
- Knott, C.S.; Panter, J.; Foley, L.; Ogilvie, D. Changes in the mode of travel to work and the severity of depressive symptoms: A longitudinal analysis of UK Biobank. Prev. Med. 2018, 112, 61–69. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Rodriguez, D.A.; Sarmiento, O.L.; Guaje, O. Commute patterns and depression: Evidence from eleven Latin American cities. J. Transp. health 2019, 14. [Google Scholar] [CrossRef]
- Marques, A.; Peralta, M.; Martins, J.; de Matos, M.G.; Brownson, R.C. Cross-sectional and prospective relationship between physical activity and chronic diseases in European older adults. Int. J. Public Health 2017, 62, 495–502. [Google Scholar] [CrossRef]
- Lampinen, P.; Heikkinen, R.L.; Ruoppila, I. Changes in intensity of physical exercise as predictors of depressive symptoms among older adults: An eight-year follow-up. Prev. Med. 2000, 30, 371–380. [Google Scholar] [CrossRef]
- Siefken, K.; Junge, A.; Laemmle, L. How does sport affect mental health? An investigation into the relationship of leisure-time physical activity with depression and anxiety. Hum. Mov. 2019, 20, 62–74. [Google Scholar] [CrossRef]
- Joshi, S.; Mooney, S.J.; Kennedy, G.J.; Benjamin, E.O.; Ompad, D.; Rundle, A.G.; Beard, J.R.; Cerda, M. Beyond METs: Types of physical activity and depression among older adults. Age Ageing 2016, 45, 103–109. [Google Scholar] [CrossRef]
- Dishman, R.K.; Sui, X.; Church, T.S.; Hand, G.A.; Trivedi, M.H.; Blair, S.N. Decline in cardiorespiratory fitness and odds of incident depression. Am. J. Prev. Med. 2012, 43, 361–368. [Google Scholar] [CrossRef]
- McKercher, C.M.; Schmidt, M.D.; Sanderson, K.A.; Patton, G.C.; Dwyer, T.; Venn, A.J. Physical activity and depression in young adults. Am. J. Prev. Med. 2009, 36, 161–164. [Google Scholar] [CrossRef]
- Kull, M.; Ainsaar, M.; Kiive, E.; Raudsepp, L. Relationship between low depressiveness and domain specific physical activity in women. Health Care Women Int. 2012, 33, 457–472. [Google Scholar] [CrossRef]
- Mytton, O.T.; Panter, J.; Ogilvie, D. Longitudinal associations of active commuting with wellbeing and sickness absence. Prev. Med. 2016, 84, 19–26. [Google Scholar] [CrossRef]
- Costa, S.; Ogilvie, D.; Dalton, A.; Westgate, K.; Brage, S.; Panter, J. Quantifying the physical activity energy expenditure of commuters using a combination of global positioning system and combined heart rate and movement sensors. Prev. Med. 2015, 81, 339–344. [Google Scholar] [CrossRef] [PubMed]
- Sampson, L.; Martins, S.S.; Yu, S.; Chiavegatto Filho, A.D.P.; Andrade, L.H.; Viana, M.C.; Medina-Mora, M.E.; Benjet, C.; Torres, Y.; Piazza, M.; et al. The relationship between neighborhood-level socioeconomic characteristics and individual mental disorders in five cities in Latin America: Multilevel models from the World Mental Health Surveys. Soc. Psychiatry Psychiatr. Epidemiol. 2019, 54, 157–170. [Google Scholar] [CrossRef] [PubMed]
- Lucas, K. Transport and social exclusion: Where are we now? Transp. Policy 2012, 20, 105–113. [Google Scholar] [CrossRef]


{kind=link}
| Author, Year | Study Design | Sample and Country | Depression Measure | Active Commuting Measure | Observations | Main Results | Methodological Quality |
|---|---|---|---|---|---|---|---|
| Smith et al., 2010 | Prospective cohort. | n = 3196 Japanese-American men who were involved in the Honolulu Heart Program aged 71–93 years; mean age 77 years. United States. | Center for Epidemiologic Studies Depression Scale (CES-D 11) | Participants reported how many city blocks they walked each day. Blocks were converted into miles using 12 blocks per mile as a conversion factor. This assessment was developed from the Harvard Alumni Survey. | Walking distance included leisure-time and active commuting. | Those who walked more had significantly lower rates of prevalent depressive symptoms in cross-sectional analyses. Elderly men, without chronic diseases, who walked longer distances per day were less likely to develop new depressive symptoms over eight years of follow-up. | Moderate |
| Kai et al., 2011 | Prospective (1-year follow-up). | n = 634: 536 men, 98 women aged 20–60 years; 36.7 ± 9.2 years. Japan. | Center for Epidemiologic Studies Depression Scale (CES-D) | The duration of leisure-time physical activity and commuting by walking were measured using a self-report questionnaire. | Walking distance included leisure-time physical activity and commuting to work. | The adjusted odds ratio (OR) of depressive symptoms in the highest tertile of leisure-time physical activity was 50% lower (OR = 0.50, 95% CI: 0.26–0.97) than those in the lowest tertile. In contrast, no significant association was found between the risk of depressive symptoms and duration of commuting by walking. | Moderate |
| Julien et al., 2013 | Prospective (5-years follow-up). VoisiNuAge Study. | n = 498: 236 men, 262 women aged 68–84 years (74.86 ± 4.18 men and 74.90 ± 3.97 women). Canada. | Geriatric Depression Scale (GDS) | Physical Activity Scale for the Elderly (PASE). | Walking distance included leisure-time and active commuting. | Depressive symptoms predicted walking frequency (higher depressive symptoms were related to fewer walking days), but walking frequency did not predict depressive symptoms at subsequent time points. | Moderate |
| Torres at el., 2015 | Cross-sectional. National Survey of American Life (NSAL). | n = 2978: 1903 men, 1075 women aged ≥18 years. United states. | Center for Epidemiologic Studies Depression Scale (CES-D) | Walking was measured with responses to one question from the Americans’ Changing Lives questionnaire. | Walking distance included leisure-time and active commuting. | Women who reported often walking had lower odds for depressive symptoms than women who reported never walking (OR = 0.56, 95% CI: 0.38–0.82). Walking frequency was not related to depressive symptoms in men. | Moderate |
| Kuwahara et al., 2015 | Prospective (5-year follow-up). Japan Epidemiology Collaboration on Occupational Health (J-ECOH) Study. | n = 29,082 workers: 24,676 men, 4406 women aged 20–64 years; mean age 42.7 years. Japan. | Epidemiologic Studies Depression Scale (CES-D), Self-Rating Depression Scale (SDS) | Participants were asked whether they regularly engaged in any physical activity during leisure. Duration of walking to and from work was self-reported and categorised as <20minutes, 20–40 min, and ≥ 40 min. | It assessed leisure-time physical activity, physical activity at work, and active commuting. | Leisure exercise showed a U-shaped association with the risk of depressive symptoms. Walking to and from work was not associated with depressive symptoms. | Moderate |
| Knott et al., 2018 | Population-based prospective cohort. UK Biobank. | n = 5474, aged 37–73 years. United Kingdom. | Patient Health Questionnaire (PHQ-2) | Participants reported the frequency of trips from home to work (trips/week); the distance travelled (miles); and the mode of transport used (“car or motor vehicle” (hereafter ”car” for simplicity), ”public transport”, and ”walk” and/or ”cycle”). | Paper was focused on modes of travel to work. | Participants who were asymptomatic at baseline and switched to more active modes of commuting tended to report a lower severity of symptoms at follow-up than those who continued to travel inactively (β = −0.10, 95% CI: −0.20–0.00). Among commuters who were symptomatic at baseline, longer journeys were associated with worse symptoms at follow-up (β = 0.64, 95% CI: 0.13–1.16). Shifting from exclusive car use towards more active commuting may help prevent and attenuate depressive symptoms in working adults. | Moderate |
| Wang et al., 2019 | Cross-sectional. La Encuesta CAF 2016. | n = 5438. Argentina, Bolivia, Brazil, Colombia, Ecuador, México, Panamá, Peru, Uruguay, and Venezuela. | Center for Epidemiologic Studies Depression Scale (CES-D) | Participants reported commuting time during a “normal day”, uncongested commuting time, and travel mode commonly used for the commute. | Different modes of travel were assessed. | Every 10 more minutes of commuting time is associated with a 0.5% (p = 0.011) higher probability of screening positively for depression. There were not found any significant associations between non-motorised modes of travel and depression. | Moderate |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marques, A.; Peralta, M.; Henriques-Neto, D.; Frasquilho, D.; Rubio Gouveira, É.; Gomez-Baya, D. Active Commuting and Depression Symptoms in Adults: A Systematic Review. Int. J. Environ. Res. Public Health 2020, 17, 1041. https://doi.org/10.3390/ijerph17031041
Marques A, Peralta M, Henriques-Neto D, Frasquilho D, Rubio Gouveira É, Gomez-Baya D. Active Commuting and Depression Symptoms in Adults: A Systematic Review. International Journal of Environmental Research and Public Health. 2020; 17(3):1041. https://doi.org/10.3390/ijerph17031041
Chicago/Turabian StyleMarques, Adilson, Miguel Peralta, Duarte Henriques-Neto, Diana Frasquilho, Élvio Rubio Gouveira, and Diego Gomez-Baya. 2020. "Active Commuting and Depression Symptoms in Adults: A Systematic Review" International Journal of Environmental Research and Public Health 17, no. 3: 1041. https://doi.org/10.3390/ijerph17031041
APA StyleMarques, A., Peralta, M., Henriques-Neto, D., Frasquilho, D., Rubio Gouveira, É., & Gomez-Baya, D. (2020). Active Commuting and Depression Symptoms in Adults: A Systematic Review. International Journal of Environmental Research and Public Health, 17(3), 1041. https://doi.org/10.3390/ijerph17031041