The Effects of an Artificial Garden on Heart Rate Variability among Healthy Young Japanese Adults


Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Design and Procedure
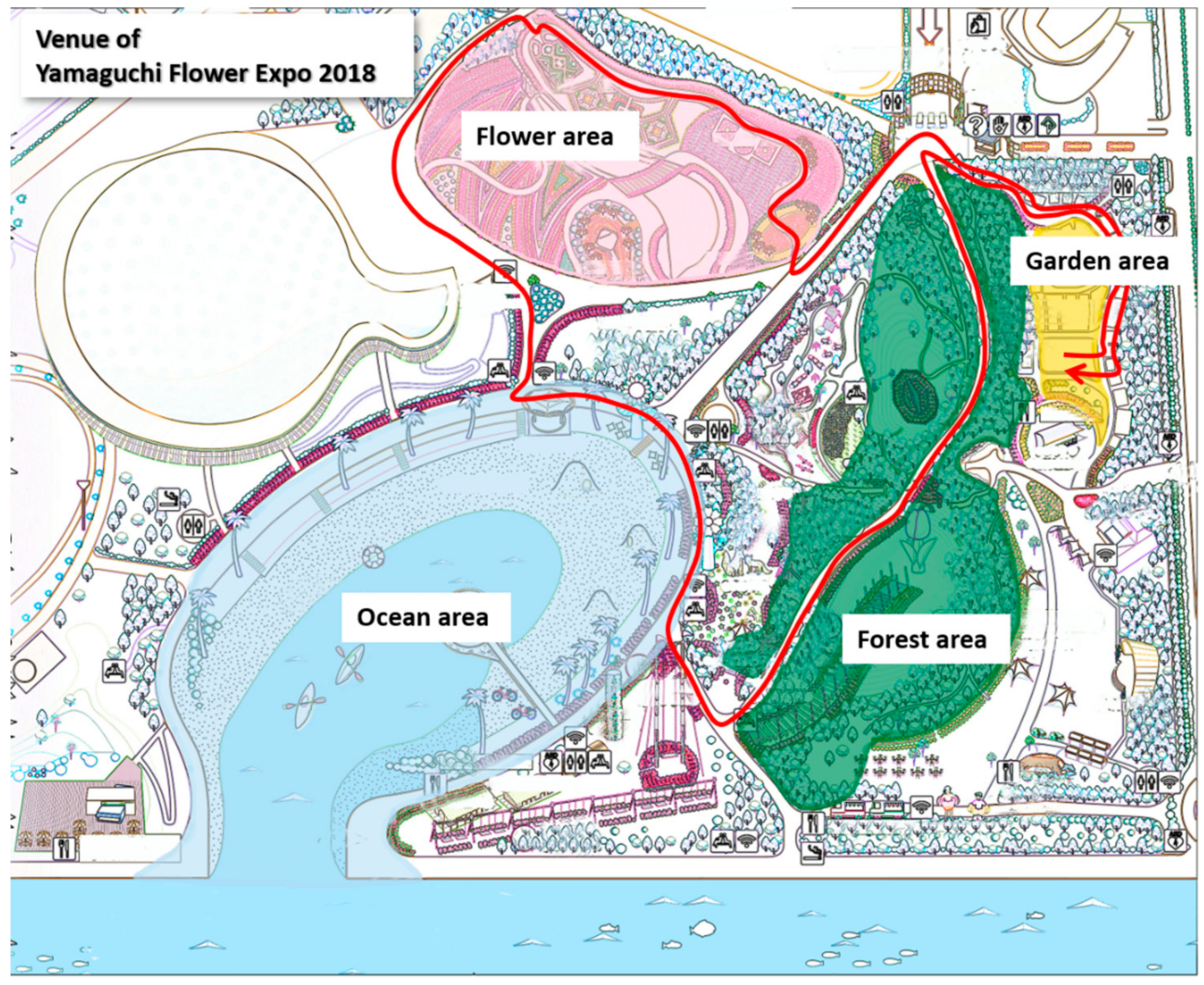
2.2.1. Study Site
2.2.2. Preliminary Survey
2.2.3. Experimental Procedure
2.3. Data Management and Statistical Analysis
3. Results
3.1. Baseline HRV
3.2. HRV Change after the Walk
3.3. HRV Changes in Four Areas (Forest, Flower, Ocean, and Garden of Health)
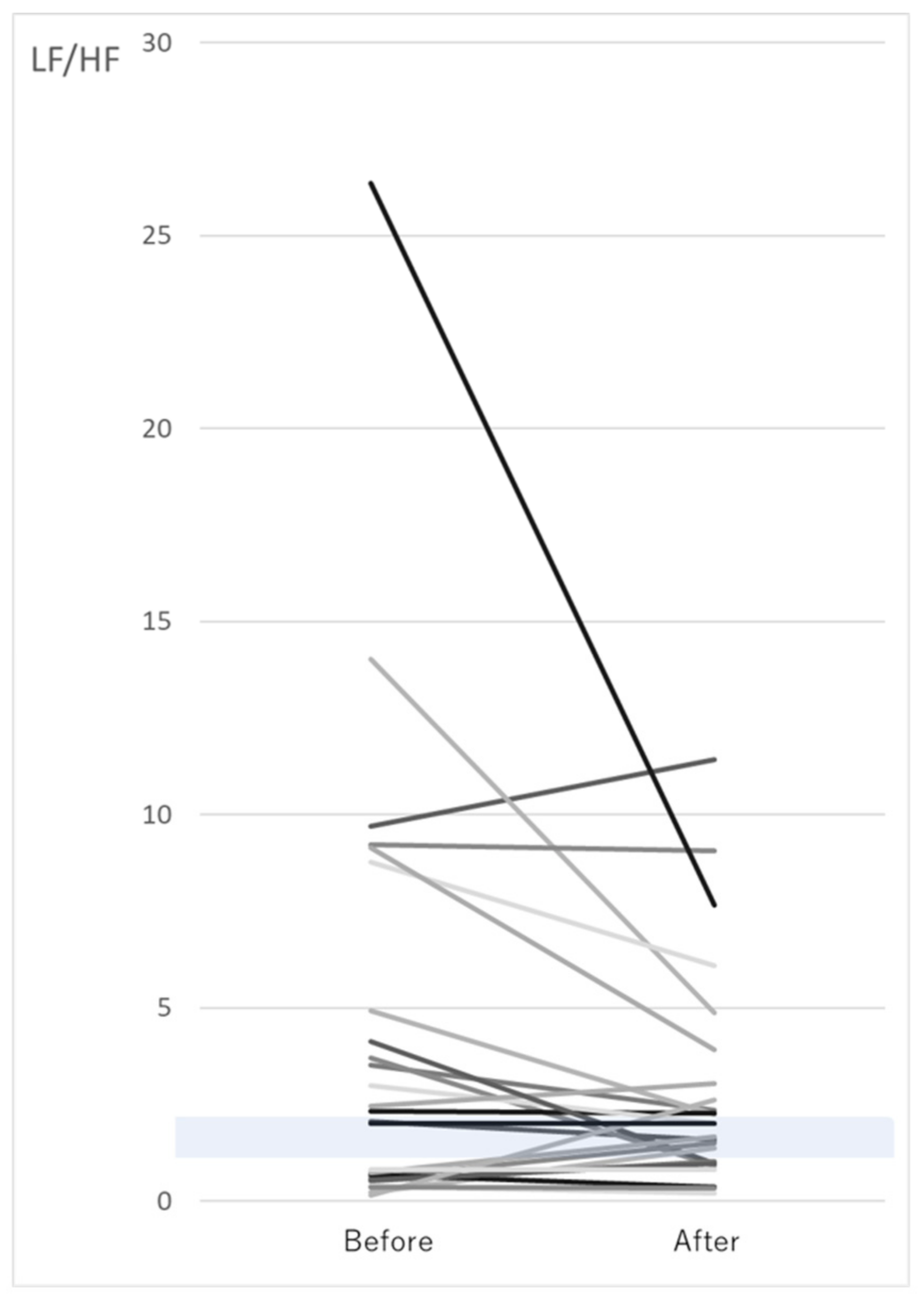
3.4. Changes in LF/HF after the Walk
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- The WHO World Mental Health Survey Consortium. Prevalence, Severity, and Unmet Need for Treatment of Mental Disorders in the World Health Organization World Mental Health Surveys. JAMA 2004, 291, 2581–2590. [Google Scholar] [CrossRef] [PubMed]
- Dye, C. Health and Urban Living. Science 2008, 319, 766–769. [Google Scholar] [CrossRef] [PubMed]
- Wagner, K.H.; Brath, H. A global view on the development of non communicable diseases. Prev. Med. 2012, 54, S38–S41. [Google Scholar] [CrossRef] [PubMed]
- Tsuko Tanaka, A.; Takano, T.; Nakam Ura, K.; Takeuchi, S. Health levels infuenced by urban residential conditions in a Megacity Tokyo. Urban Stud. 1996, 33, 879–894. [Google Scholar] [CrossRef]
- Peen, J.; Schoevers, R.A.; Beekman, A.T.; Dekker, J. The current status of urban-rural differences in psychiatric disorders. Acta Psychiatr. Scand. 2010, 121, 84–93. [Google Scholar] [CrossRef] [PubMed]
- Lederbogen, F.; Kirsch, P.; Haddad, L.; Streit, F.; Tost, H.; Schuch, P.; Wüst, S.; Pruessner, J.C.; Rietschel, M.; Deuschle, M.; et al. City living and urban upbringing affect neural social stress processing in humans. Nature 2011, 474, 498–501. [Google Scholar] [CrossRef]
- McKenzie, K.; Murray, A.; Booth, T. The impact of urban-rural environments on mental health Do urban environments increase the risk of anxiety, depression and psychosis? An epidemiological study. Karen McKenzie, Department of Clinical Psychology, University of Edinburgh. Aja Murray an. J. Affect. Disord. 2013, 150, 1019–1024. [Google Scholar] [CrossRef]
- Hartig, T.; Mitchell, R.; De Vries, S.; Frumkin, H. Nature and Health. Annu. Rev. Public Health 2014, 35, 207–228. [Google Scholar] [CrossRef]
- Ulrich, R.S. Visual landscapes and psychological well-being. Landsc. Res. 1979, 4, 17–23. [Google Scholar] [CrossRef]
- Maas, J.; Verheij, R.A.; Groenewegen, P.P.; De Vries, S.; Spreeuwenberg, P. Green space, urbanity, and health: How strong is the relation? J. Epidemiol. Community Health 2006, 60, 587–592. [Google Scholar] [CrossRef]
- Im, S.G.; Choi, H.; Jeon, Y.H.; Song, M.K.; Kim, W.; Woo, J.M. Comparison of Effect of Two-Hour Exposure to Forest and Urban Environments on Cytokine, Anti-Oxidant, and Stress Levels in Young Adults. Int. J. Environ. Res. Public Health 2016, 13, 625. [Google Scholar] [CrossRef] [PubMed]
- Park, B.J.; Tsunetsugu, Y.; Kasetani, T.; Hirano, H.; Kagawa, T.; Sato, M.; Miyazaki, Y. Physiological Effects of Shinrin-yoku (Taking in the Atmosphere of the Forest)—Using Salivary Cortisol and Cerebral Activity as Indicators-. J. Physiol. Anthr. 2007, 26, 123–128. [Google Scholar] [CrossRef]
- Han, J.W.; Choi, H.; Jeon, Y.H.; Yoon, C.H.; Woo, J.M.; Kim, W. The Effects of Forest Therapy on Coping with Chronic Widespread Pain: Physiological and Psychological Differences between Participants in a Forest Therapy Program and a Control Group. Int. J. Environ. Res. Public Health 2016, 13, 255. [Google Scholar] [CrossRef] [PubMed]
- Joung, D.; Kim, G.; Choi, Y.; Lim, H.; Park, S.; Woo, J.M.; Park, B.J. The Prefrontal Cortex Activity and Psychological Effects of Viewing Forest Landscapes in Autumn Season. Int. J. Environ. Res. Public Health 2015, 12, 7235. [Google Scholar] [CrossRef] [PubMed]
- Horiuchi, M.; Endo, J.; Takayama, N.; Murase, K.; Nishiyama, N.; Saito, H.; Fujiwara, A. Impact of Viewing vs. Not Viewing a Real Forest on Physiological and Psychological Responses in the Same Setting. Int. J. Environ. Res. Public Health 2014, 11, 10883–10901. [Google Scholar] [CrossRef] [PubMed]
- Tsutsumi, M.; Nogaki, H.; Shimizu, Y.; Stone, T.E.; Kobayashi, T. Individual reactions to viewing preferred video representations of the natural environment: A comparison of mental and physical reactions. Jpn. J. Nurs. Sci. 2017, 14, 3–12. [Google Scholar] [CrossRef]
- Triguero-Mas, M.; Dadvand, P.; Cirach, M.; Martínez, D.; Medina, A.; Mompart, A.; Basagaña, X.; Gražulevičienė, R.; Nieuwenhuijsen, M.J. Natural outdoor environments and mental and physical health: Relationships and mechanisms. Environ. Int. 2015, 77, 35–41. [Google Scholar] [CrossRef]
- Ikei, H.; Komatsu, M.; Song, C.; Himoro, E.; Miyazaki, Y. The physiological and psychological relaxing effects of viewing rose flowers in office workers. J. Physiol. Anthr. 2014, 33, 1–5. [Google Scholar] [CrossRef]
- Li, Q.; Kobayashi, M.; Wakayama, Y.; Inagaki, H.; Katsumata, M.; Hirata, Y.; Hirata, K.; Shimizu, T.; Kawada, T.; Ohira, J.T.; et al. Effect of Phytoncide from Trees on Human Natural Killer Cell Function. Int. J. Immunopathol. Pharmacol. 2009, 22, 951–959. [Google Scholar] [CrossRef]
- Song, C.; Ikei, H.; Miyazaki, Y. Physiological Effects of Visual Stimulation with Forest Imagery. Int. J. Environ. Res. Public Health 2018, 15, 213. [Google Scholar] [CrossRef]
- Song, C.; Ikei, H.; Kagawa, T.; Miyazaki, Y. Physiological and Psychological Effects of Viewing Forests on Young Women. Forests 2019, 10, 635. [Google Scholar] [CrossRef]
- Roe, J.; Barnes, L.; Napoli, N.; Thibodeaux, J. The Restorative Health Benefits of a Tactical Urban Intervention: An Urban Waterfront Study. Front. Built Environ. 2019, 5, 1–10. [Google Scholar] [CrossRef]
- Vert, C.; Gascon, M.; Ranzani, O.; Márquez, S.; Triguero-Mas, M.; Carrasco-Turigas, G.; Arjona, L.; Koch, S.; Llopis, M.; Donaire-Gonzalez, D.; et al. Physical and mental health effects of repeated short walks in a blue space environment: A randomised crossover study. Environ. Res. 2020, 188, 109812. [Google Scholar] [CrossRef] [PubMed]
- Gascon, M.; Zijlema, W.; Vert, C.; White, M.P.; Nieuwenhuijsen, M.J. Outdoor blue spaces, human health and well-being: A systematic review of quantitative studies. Int. J. Hyg. Environ. Health 2017, 220, 1207–1221. [Google Scholar] [CrossRef]
- Lahart, I.; Darcy, P.; Gidlow, C.; Calogiuri, G. The effects of green exercise on physical and mental wellbeing: A systematic review. Int. J. Environ. Res. Public Health 2019, 16, 1352. [Google Scholar] [CrossRef]
- Song, C.; Ikei, H.; Kagawa, T.; Miyazaki, Y. Effects of Walking in a Forest on Young Women. Int. J. Environ. Res. Public Health 2019, 16, 229. [Google Scholar] [CrossRef]
- De Brito, J.N.; Pope, Z.; Mitchell, N.; Schneider, I.E.; Larson, J.M.; Horton, T.H.; Pereira, M.A. The effect of green walking on heart rate variability: A pilot crossover study. Environ. Res. 2020, 185. Available online: https://www.sciencedirect.com/science/article/pii/S0013935120303017 (accessed on 18 March 2020). [CrossRef]
- Massaro, S.; Pecchia, L. Heart Rate Variability (HRV) Analysis: A Methodology for Organizational Neuroscience. Organ. Res. Methods 2019, 22, 354–393. [Google Scholar] [CrossRef]
- Lal, D.; Corey, J.P. Vasomotor rhinitis update. Curr. Opin. Otolaryngol. Head Neck Surg. 2004, 12, 243–247. [Google Scholar] [CrossRef]
- Vayisoglu, Y.; Ozcan, C.; Pekdemir, H.; Gorur, K.; Pata, Y.S.; Çamsarı, A. Autonomic Nervous System Evaluation Using Heart Rate Variability Parameters in Vasomotor Rhinitis Patients. Int. J. Otolaryngol. 2006, 35, 338–342. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variable | Males (n = 13) | Females (n = 25) | All (n = 38) |
|---|---|---|---|
| Mean (SD) | Mean (SD) | Mean (SD) | |
| Age (years) | 21.9 (1.0) | 21.2 (1.2) | |
| Height (cm) | 170.2 (6.8) | 158.2 (5.3) | |
| Weight (kg) | 62.0 (8.0) | 49.8 (6.0) | |
| BMI (kg/m2) | 21.2 (1.9) | 19.9 (2.2) | |
| Males (n = 13) | Females (n = 25) | All (n = 38) | |
| Physical symptom | n (%) | n (%) | n (%) |
| allergic rhinitis | 3 (23) | 12 (48) | 15 (39) |
| sleep disorder | 2 (15) | 3 (12) | 5 (13) |
| fitness habits | 3 (23) | 8 (32) | 11 (29) |
| Variable | Allergic Rhinitis | Sleep Disorder | Fitness Habits | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| All (n = 38) | Presence (n = 15) | Absence (n = 23) | p-Value | Presence (n = 5) | Absence (n = 33) | p-Value | Presence (n = 10) | Absence (n = 28) | p-Value | |
| Mean (SD) | Mean (SD) | Mean (SD) | Mean (SD) | Mean (SD) | Mean (SD) | Mean (SD) | ||||
| HF (ms2) | 721 (695) | 937 (897) | 585 (462) | 0.13 | 508 (298) | 752 (720) | 0.48 | 1089 (803) | 576 (572) | <0.05 |
| LF/HF | 1.7 (2.0) | 1.2 (1.0) | 1.9 (2.4) | 0.26 | 3.6 (3.5) | 1.4 (1.5) | <0.05 | 0.7 (0.6) | 2.0 (2.3) | 0.08 |
| HR (bpm) | 75.1 (11.8) | 72.1 (3.0) | 77.3 (2.5) | 0.19 | 79.8 (5.3) | 74.5 (2.1) | 0.36 | 69.1 (3.4) | 77.7 (2.2) | <0.05 |
| ccvTP | 4.1 (1.4) | 4.4 (1.3) | 3.9 (1.4) | 0.27 | 4.0 (1.3) | 4.2 (2.0) | 0.31 | 4.4 (1.0) | 3.9 (1.5) | 0.34 |
| Variable | Pretest | Post-Test | p-Value |
|---|---|---|---|
| Mean (SD) | Mean (SD) | ||
| HF (ms2) | 557 (619) | 451 (619) | 0.20 |
| LF/HF | 3.4 (4.9) | 3.3 (3.4) | 0.08 |
| HR (bpm) | 75.7 (10.1) | 76.1 (9.2) | 0.84 |
| ccvTP | 4.2 (1.5) | 3.8 (1.5) | 0.58 |
| Variable | Garden for Health | Ccean | Flowers | Forest | ANOVA | |
|---|---|---|---|---|---|---|
| Mean (SD) | Mean (SD) | Mean (SD) | Mean (SD) | F-Value | p-Value | |
| HF (ms2) | 145 (130) | 125 (109) | 125 (109) | 123 (104) | 0.31 | 0.81 |
| LF/HF | 6.7 (3.7) | 6.6 (3.5) | 6.9 (3.5) | 6.2 (3.0) | 0.25 | 0.86 |
| HR (bpm) | 89.4 (12.3) | 93.4 (9.7) | 91.4 (10.3) | 93.1 (12.5) | 0.91 | 0.44 |
| CVRR | 5.0 (1.5) | 5.0 (1.1) | 5.0 (1.3) | 4.8 (1.4) | 0.32 | 0.81 |
| log in time (min) | 3–35 | 2–14 | 7–28 | 8–60 | ||
| Variable | Allergic Rhinitis | Sleep Disoder | Fitness Habits | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Presence (n = 15) | Absence (n = 23) | p-Value | Presence (n = 5) | Absence (n = 33) | p-Value | Presence (n = 10) | Absence (n = 28) | p-Value | ||
| HF (ms2) | pretest | 896 (835) | 510 (898) | 0.18 | 309 (396) | 710 (152) | 0.35 | 1184 (1210) | 452 (633) | <0.05 |
| post-test | 770 (895) | 293 (309) | <0.05 | 445 (395) | 481 (672) | 0.91 | 1099 (983) | 232 (186) | <0.0001 | |
| LF/HF | pretest | 2.2 (3.1) | 4.1 (5.7) | 0.24 | 9.5 (10.3) | 2.5 (3.0) | <0.01 | 2.1 (1.5) | 3.8 (0.9) | 0.34 |
| post-test | 2.5 (3.2) | 3.6 (3.6) | 0.33 | 5.0 (3.2) | 3.0 (3.4) | 0.21 | 2.4 (3.4) | 3.5 (3.5) | 0.39 | |
| HR (bpm) | pretest | 71.9 (8.0) | 78.1 (10.7) | 0.06 | 84.8 (6.1) | 74.4 (9.9) | <0.05 | 69.5 (8.3) | 78.1 (9.8) | <0.05 |
| post-test | 72.7 (7.8) | 78.3 (9.6) | 0.07 | 80.9 (7.0) | 75.4 (9.4) | 0.22 | 68.8 (7.3) | 79.0 (8.4) | <0.001 | |
| ccvTP | pretest | 4.7 (0.5) | 4.1 (0.4) | 0.35 | 4.7 (0.9) | 4.3 (0.3) | 0.66 | 5.3 (2.4) | 4.0 (1.5) | <0.05 |
| post-test | 4.2 (1.7) | 3.7 (1.4) | 0.29 | 5.0 (1.8) | 3.7 (1.5) | 0.08 | 5.1 (1.5) | 3.4 (1.3) | <0.01 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Suenaga, H.; Murakami, K.; Murata, N.; Nishikawa, S.; Tsutsumi, M.; Nogaki, H. The Effects of an Artificial Garden on Heart Rate Variability among Healthy Young Japanese Adults. Int. J. Environ. Res. Public Health 2020, 17, 9465. https://doi.org/10.3390/ijerph17249465
Suenaga H, Murakami K, Murata N, Nishikawa S, Tsutsumi M, Nogaki H. The Effects of an Artificial Garden on Heart Rate Variability among Healthy Young Japanese Adults. International Journal of Environmental Research and Public Health. 2020; 17(24):9465. https://doi.org/10.3390/ijerph17249465
Chicago/Turabian StyleSuenaga, Hiromi, Kanako Murakami, Nozomi Murata, Syoriki Nishikawa, Masae Tsutsumi, and Hiroshi Nogaki. 2020. "The Effects of an Artificial Garden on Heart Rate Variability among Healthy Young Japanese Adults" International Journal of Environmental Research and Public Health 17, no. 24: 9465. https://doi.org/10.3390/ijerph17249465
APA StyleSuenaga, H., Murakami, K., Murata, N., Nishikawa, S., Tsutsumi, M., & Nogaki, H. (2020). The Effects of an Artificial Garden on Heart Rate Variability among Healthy Young Japanese Adults. International Journal of Environmental Research and Public Health, 17(24), 9465. https://doi.org/10.3390/ijerph17249465