Psychological Health and Physical Activity Levels during the COVID-19 Pandemic: A Systematic Review

 ,
,  ,
,  ,
,  , ,
, ,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Design
2.2. Databases and Search Strategy
2.3. Inclusion/Exclusion Criteria Selection of Studies
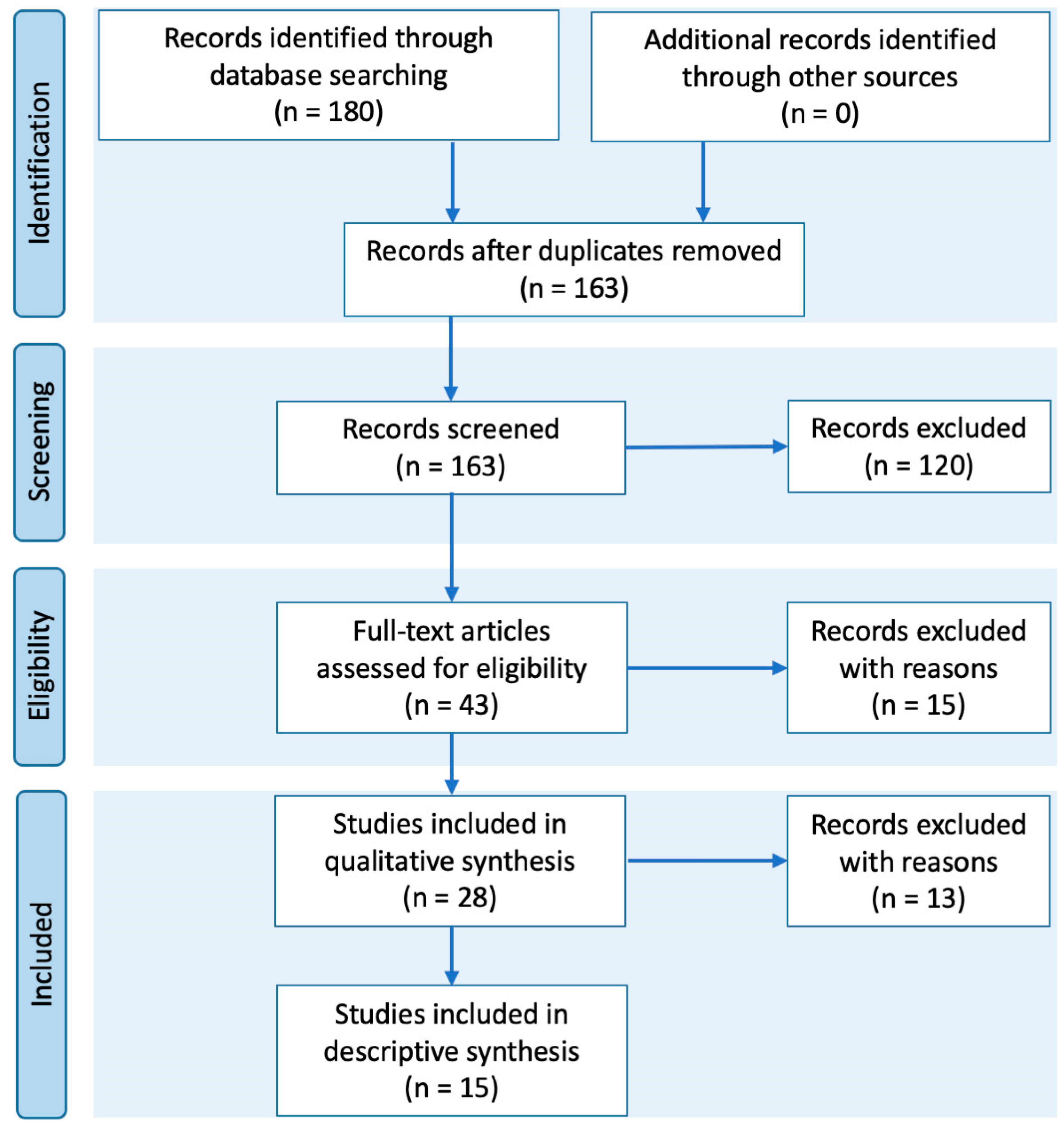
3. Results
- (a)
- From the 120 initially excluded articles: 1. The study could not be retrieved (0); 2. The study is within the theoretical frameworks of medicine (1); 3. The study population is: 3.1. pregnant women, people with physical disabilities, and/or prisoners (2); 3.2. individuals who are not yet adults (12); 3.3. participants who suffer from a particular illness or patients with COVID-19 or history of the disease (38); 4. The type of publication was report (14), opinion study, political commentary, social media events, and protocols (15), essays (11), case studies (6), reviews, systematic reviews, or meta-analysis (5), no original research (16);
- (b)
- From the second round, 15 articles were excluded because they were associated with mental health (7) or PA (8) only but not both;
- (c)
- From the third round, 13 articles were excluded after reading the full text because they were reports (7); report reviews (3); commentaries (1); or protocol research (2).
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Lai, C.C.; Shih, T.P.; Ko, W.C.; Tang, H.J.; Hsueh, P.R. Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) and coronavirus disease-2019 (COVID-19): The epidemic and the challenges. Int. J. Antimicrob. Agents 2020, 55, 105924. [Google Scholar] [CrossRef] [PubMed]
- Tobaiqy, M.; Qashqary, M.; Al-Dahery, S.; Mujallad, A.; Hershan, A.; Kamal, M.; Helmi, N. Therapeutic management of patients with COVID-19: A systematic review. Infect. Prev. Pr. 2020, 2, 100061. [Google Scholar] [CrossRef]
- World Health Organization. Considerations in Adjusting Public Health and Social Measures in the Context of COVID-19: Interim Guidance. Available online: https://www.who.int/publications/i/item/considerations-in-adjusting-public-health-and-social-measures-in-the-context-of-covid-19-interim-guidance (accessed on 20 August 2020).
- World Health Organization. Síndrome Inflamatorio Multisistémico En Niños y Adolescentes Con COVID-19; World Health Organization: Geneva, Switzerlands, 2020; pp. 1–3. [Google Scholar]
- Scarmozzino, F.; Visioli, F. Covid-19 and the Subsequent Lockdown Modified Dietary Habits of Almost Half the Population in an Italian Sample. Foods 2020, 9, 675. [Google Scholar] [CrossRef] [PubMed]
- Zachary, Z.; Forbes, B.; Lopez, B.; Pedersen, G.; Welty, J.; Deyo, A.; Kerekes, M. Since January 2020 Elsevier Has Created a COVID-19 Resource Centre with Free Information in English and Mandarin on the Novel Coronavirus COVID-19. Obes Res. Clin. Pract. 2020, 14, 210–216. [Google Scholar] [CrossRef] [PubMed]
- Ammar, A.; Brach, M.; Trabelsi, K.; Chtourou, H.; Boukhris, O.; Masmoudi, L.; Bouaziz, B.; Bentlage, E.; How, D.; Ahmed, M.; et al. Effects of COVID-19 Home Confinement on Eating Behaviour and Physical Activity: Results of the ECLB-COVID19 International Online Survey. Nutrients 2020, 12, 1583. [Google Scholar] [CrossRef] [PubMed]
- Neill, E.; Meyer, D.; Toh, W.L.; Van Rheenen, T.E.; Phillipou, A.; Tan, E.J.; Rossell, S.L. Alcohol use in Australia during the early days of the COVID-19 pandemic: Initial results from the COLLATE project. Psychiatry Clin. Neurosci. 2020, 74, 542–549. [Google Scholar] [CrossRef] [PubMed]
- Smith, L.; Jacob, L.; Yakkundi, A.; McDermott, D.; Armstrong, N.C.; Barnett, Y.; López-Sánchez, G.F.; Martin, S.; Butler, L.; Tully, M. Correlates of symptoms of anxiety and depression and mental wellbeing associated with COVID-19: A cross-sectional study of UK-based respondents. Psychiatry Res. 2020, 291, 113138. [Google Scholar] [CrossRef]
- Gómez-Salgado, J.; Andrés-Villas, M.; Domínguez-Salas, S.; Díaz-Milanés, D.; Ruiz-Frutos, C. Related Health Factors of Psychological Distress During the COVID-19 Pandemic in Spain. Int. J. Environ. Res. Public Health 2020, 17, 3947. [Google Scholar] [CrossRef] [PubMed]
- Troyer, E.A.; Kohn, J.N.; Hong, S. Are we facing a crashing wave of neuropsychiatric sequelae of COVID-19? Neuropsychiatric symptoms and potential immunologic mechanisms. Brain Behav. Immun. 2020, 87, 34–39. [Google Scholar] [CrossRef] [PubMed]
- Rogers, J.P.; Chesney, E.; Oliver, D.; Pollak, T.A.; McGuire, P.; Fusar-Poli, P.; Zandi, M.S.; Lewis, G.; David, A.S. Psychiatric and neuropsychiatric presentations associated with severe coronavirus infections: A systematic review and meta-analysis with comparison to the COVID-19 pandemic. Lancet Psychiatry 2020, 7, 611–627. [Google Scholar] [CrossRef]
- Lei, L.; Huang, X.; Zhang, S.; Yang, J.; Yang, L.; Xu, M. Comparison of Prevalence and Associated Factors of Anxiety and Depression Among People Affected by versus People Unaffected by Quarantine During the COVID-19 Epidemic in Southwestern China. Med Sci. Monit. 2020, 26, e924609-1. [Google Scholar] [CrossRef] [PubMed]
- Mukhtar, S. Psychological health during the coronavirus disease 2019 pandemic outbreak. Int. J. Soc. Psychiatry 2020, 66, 512–516. [Google Scholar] [CrossRef] [PubMed]
- Chekroud, S.R.; Gueorguieva, R.; Zheutlin, A.B.; Paulus, M.; Krumholz, H.M.; Krystal, J.H.; Chekroud, A.M. Association between physical exercise and mental health in 1·2 million individuals in the USA between 2011 and 2015: A cross-sectional study. Lancet Psychiatry 2018, 5, 739–746. [Google Scholar] [CrossRef]
- Constandt, B.; Thibaut, E.; De Bosscher, V.; Scheerder, J.; Ricour, M.; Willem, A. Exercising in Times of Lockdown: An Analysis of the Impact of COVID-19 on Levels and Patterns of Exercise among Adults in Belgium. Int. J. Environ. Res. Public Health 2020, 17, 4144. [Google Scholar] [CrossRef] [PubMed]
- Gallé, F.; Sabella, E.A.; Da Molin, G.; De Giglio, O.; Caggiano, G.; Di Onofrio, V.; Ferracuti, S.; Montagna, M.T.; Liguori, G.; Orsi, G.B.; et al. Understanding Knowledge and Behaviors Related to Covid–19 Epidemic in Italian Undergraduate Students: The Epico Study. Int. J. Environ. Res. Public Health 2020, 17, 3481. [Google Scholar] [CrossRef]
- López-Bueno, R.; Calatayud, J.; Casaña, J.; Casajús, J.A.; Smith, L.; Tully, M.A.; Andersen, L.L.; López-Sánchez, G.F. COVID-19 Confinement and Health Risk Behaviors in Spain. Front. Psychol. 2020, 11, 1426. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Altman, D.; Antes, G.; Atkins, D.; Barbour, V.; Barrowman, N.; Berlin, J.A.; et al. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6. [Google Scholar] [CrossRef]
- Arana, J.; Lapresa, D.; Anguera, M.T.; Garzón, B. Ad hoc procedure for optimising agreement between observational records. Anales de Psicología 2016, 32, 589. [Google Scholar] [CrossRef]
- Arnau Gras, J.; Anguera, M.T.; Homez Benito, J. Metodología de La Investigación En Ciencias Del Comportamiento; Murcia Universidad: Murcia, Spain, 1990. [Google Scholar]
- Huckins, J.F.; DaSilva, A.W.; Wang, W.; Hedlund, E.; Rogers, C.; Nepal, S.K.; Wu, J.; Obuchi, M.; Murphy, E.I.; Meyer, M.L.; et al. Mental Health and Behavior During the Early Phases of the COVID-19 Pandemic: A Longitudinal Mobile Smartphone and Ecological Momentary Assessment Study in College Students (Preprint). J. Med. Internet Res. 2020, 22, e20185. [Google Scholar] [CrossRef]
- Becerra-García, J.; Giménez Ballesta, G.; Sánchez-Gutiérrez, T.; Barbeito Resa, S.; Calvo Calvo, A. Síntomas Psicopatológicos Durante La Cuarentena Por Covid-19 En Población General Española: Un Análisis Preliminar En Función de Variables Sociodemográficas y Ambientales-Ocupacionales. Rev. Esp. Salud Publica 2020, 94, e1–e11. [Google Scholar]
- Shanahan, L.; Steinhoff, A.; Bechtiger, L.; Murray, A.L.; Nivette, A.; Hepp, U.; Ribeaud, D.; Eisner, M. Emotional distress in young adults during the COVID-19 pandemic: Evidence of risk and resilience from a longitudinal cohort study. Psychol. Med. 2020, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, F.; El Morr, C.; Ritvo, P.; Othman, N.; Moineddin, R.; Team, M.; Kaipainen, K.; Buntrock, C.; Parsons, C. An Eight-Week, Web-Based Mindfulness Virtual Community Intervention for Students’ Mental Health: Randomized Controlled Trial. JMIR Ment. Health 2020, 7, e15520. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Zhang, H.; Ma, X.; Di, Q. Mental Health Problems during the COVID-19 Pandemics and the Mitigation Effects of Exercise: A Longitudinal Study of College Students in China. Int. J. Environ. Res. Public Health 2020, 17, 3722. [Google Scholar] [CrossRef] [PubMed]
- Wu, K.; Wei, X. Analysis of Psychological and Sleep Status and Exercise Rehabilitation of Front-Line Clinical Staff in the Fight Against COVID-19 in China. Med Sci. Monit. Basic Res. 2020, 26, e924085. [Google Scholar] [CrossRef] [PubMed]
- Zhang, S.X.; Wang, Y.; Rauch, A.; Wei, F. Unprecedented disruption of lives and work: Health, distress and life satisfaction of working adults in China one month into the COVID-19 outbreak. Psychiatry Res. 2020, 288, 112958. [Google Scholar] [CrossRef] [PubMed]
- Bezerra, A.C.V.; Da Silva, C.E.M.; Soares, F.R.G.; Da Silva, J.A.M. Fatores associados ao comportamento da população durante o isolamento social na pandemia de COVID-19. Ciência Saúde Coletiva 2020, 25, 2411–2421. [Google Scholar] [CrossRef]
- Shechter, A.; Diaz, F.; Moise, N.; Anstey, D.E.; Ye, S.; Agarwal, S.; Birk, J.L.; Brodie, D.; Cannone, D.E.; Chang, B.; et al. Psychological distress, coping behaviors, and preferences for support among New York healthcare workers during the COVID-19 pandemic. Gen. Hosp. Psychiatry 2020, 66, 1–8. [Google Scholar] [CrossRef]
- Antunes, R.; Frontini, R.; Amaro, N.M.; Salvador, R.; Matos, R.; Morouço, P.; Rebelo-Gonçalves, R. Exploring Lifestyle Habits, Physical Activity, Anxiety and Basic Psychological Needs in a Sample of Portuguese Adults during COVID-19. Int. J. Environ. Res. Public Health 2020, 17, 4360. [Google Scholar] [CrossRef]
- Maugeri, G.; Castrogiovanni, P.; Battaglia, G.; Pippi, R.; D’Agata, V.; Palma, A.; Di Rosa, M.; Musumeci, G. The impact of physical activity on psychological health during Covid-19 pandemic in Italy. Heliyon 2020, 6, e04315. [Google Scholar] [CrossRef]
- Stanton, R.; To, Q.G.; Khalesi, S.; Williams, S.L.; Alley, S.; Thwaite, T.L.; Fenning, A.; Vandelanotte, C. Depression, Anxiety and Stress during COVID-19: Associations with Changes in Physical Activity, Sleep, Tobacco and Alcohol Use in Australian Adults. Int. J. Environ. Res. Public Health 2020, 17, 4065. [Google Scholar] [CrossRef]
- Pillay, L.; Van Rensburg, D.C.C.J.; Van Rensburg, A.J.; Ramagole, D.A.; Holtzhausen, L.; Dijkstra, H.P.; Cronje, T. Nowhere to hide: The significant impact of coronavirus disease 2019 (COVID-19) measures on elite and semi-elite South African athletes. J. Sci. Med. Sport 2020, 23, 670–679. [Google Scholar] [CrossRef] [PubMed]
- Lesser, I.A.; Nienhuis, C.P. The Impact of COVID-19 on Physical Activity Behavior and Well-Being of Canadians. Int. J. Environ. Res. Public Health 2020, 17, 3899. [Google Scholar] [CrossRef]
- Li, Z.; Ge, J.; Yang, M.; Feng, J.; Qiao, M.; Jiang, R.; Bi, J.; Zhan, G.; Xu, X.; Wang, L.; et al. Vicarious traumatization in the general public, members, and non-members of medical teams aiding in COVID-19 control. Brain Behav. Immun. 2020, 88, 916–919. [Google Scholar] [CrossRef]
- Xiao, H.; Zhang, Y.; Kong, D.; Li, S.; Yang, N. Social Capital and Sleep Quality in Individuals Who Self-Isolated for 14 Days During the Coronavirus Disease 2019 (COVID-19) Outbreak in January 2020 in China. Med. Sci. Monit. 2020, 26, e923921-1. [Google Scholar] [CrossRef]
- Goethals, L.; Barth, N.; Guyot, J.; Hupin, D.; Celarier, T.; Bongue, B. Impact of Home Quarantine on Physical Activity Among Older Adults Living at Home During the COVID-19 Pandemic: Qualitative Interview Study. JMIR Aging 2020, 3, e19007. [Google Scholar] [CrossRef] [PubMed]
- Galloza, J.; Castillo, B.; Micheo, W. Benefits of Exercise in the Older Population. Phys. Med. Rehabil. Clin. N. Am. 2017, 28, 659–669. [Google Scholar] [CrossRef] [PubMed]
- Stubbs, B.; Vancampfort, D.; Rosenbaum, S.; Firth, J.; Cosco, T.; Veronese, N.; Salum, G.A.; Schuch, F.B. An examination of the anxiolytic effects of exercise for people with anxiety and stress-related disorders: A meta-analysis. Psychiatry Res. 2017, 249, 102–108. [Google Scholar] [CrossRef] [PubMed]
- Mattioli, A.V.; Puviani, M.B. Lifestyle at Time of COVID-19: How Could Quarantine Affect Cardiovascular Risk. Am. J. Lifestyle Med. 2020, 14, 240–242. [Google Scholar] [CrossRef]
- Lara, B.B.; Carnes, A.; Dakterzada, F.; Benitez, I.; Piñol-Ripoll, G. Neuropsychiatric symptoms and quality of life in Spanish patients with Alzheimer’s disease during the COVID-19 lockdown. Eur. J. Neurol. 2020, 27, 1744–1747. [Google Scholar] [CrossRef]
- Lee, I.-M.; Shiroma, E.J.; Lobelo, F.; Puska, P.; Blair, S.N.; Katzmarzyk, P.T. Effect of physical inactivity on major non-communicable diseases worldwide: An analysis of burden of disease and life expectancy. Lancet 2012, 380, 219–229. [Google Scholar] [CrossRef]
- Hamilton, M.T.; Healy, G.N.; Dunstan, D.W.; Zderic, T.W.; Owen, N. Too little exercise and too much sitting: Inactivity physiology and the need for new recommendations on sedentary behavior. Curr. Cardiovasc. Risk Rep. 2008, 2, 292–298. [Google Scholar] [CrossRef] [PubMed]
- Owen, N.; Sparling, P.B.; Healy, G.N.; Dunstan, D.W.; Matthews, C.E. Sedentary Behavior: Emerging Evidence for a New Health Risk. Mayo Clin. Proc. 2010, 85, 1138–1141. [Google Scholar] [CrossRef] [PubMed]
- Moccia, F.; Gerbino, A.; Lionetti, V.; Miragoli, M.; Munaron, L.M.; Pagliaro, P.; Pasqua, T.; Penna, C.; Rocca, C.; Samaja, M.; et al. COVID-19-associated cardiovascular morbidity in older adults: A position paper from the Italian Society of Cardiovascular Researches. GeroScience 2020, 42, 1021–1049. [Google Scholar] [CrossRef] [PubMed]
- Duncan, G.E.; Avery, A.R.; Seto, E.; Tsang, S. Perceived change in physical activity levels and mental health during COVID-19: Findings among adult twin pairs. PLoS ONE 2020, 15, e0237695. [Google Scholar] [CrossRef] [PubMed]
- López-Bueno, R.; Calatayud, J.; Ezzatvar, Y.; Casajús, J.A.; Smith, L.; Andersen, L.L.; López-Sánchez, G.F. Association Between Current Physical Activity and Current Perceived Anxiety and Mood in the Initial Phase of COVID-19 Confinement. Front. Psychiatry 2020, 11, 729. [Google Scholar] [CrossRef] [PubMed]
- Pieh, C.; Budimir, S.; Probst, T. The effect of age, gender, income, work, and physical activity on mental health during coronavirus disease (COVID-19) lockdown in Austria. J. Psychosom. Res. 2020, 136, 110186. [Google Scholar] [CrossRef]
- Prochaska, J.O.; DiClemente, C.C. Stages and processes of self-change of smoking: Toward an integrative model of change. J. Consult. Clin. Psychol. 1983, 51, 390–395. [Google Scholar] [CrossRef]
- Faulkner, J.; O’brien, W.J.; Mcgrane, B.; Wadsworth, D.; Batten, J.; Askew, C.D.; Badenhorst, C.; Byrd, E.; Coulter, M.; Draper, N.; et al. Physical activity, mental health and well-being of adults during early COVID-19 containment strategies: A multi-country cross-sectional analysis. medRxiv 2020. [Google Scholar] [CrossRef]
- Cohen, S. Psychosocial Vulnerabilities to Upper Respiratory Infectious Illness: Implications for Susceptibility to Coronavirus Disease 2019 (COVID-19). Perspect. Psychol. Sci. 2020. [Google Scholar] [CrossRef]
- Callow, D.D.; Arnold-Nedimala, N.A.; Jordan, L.S.; Pena, G.S.; Won, J.; Woodard, J.L.; Smith, J.C. The Mental Health Benefits of Physical Activity in Older Adults Survive the COVID-19 Pandemic. Am. J. Geriatr. Psychiatry 2020, 28, 1046–1057. [Google Scholar] [CrossRef]
- Sansano, O.; Giné-Garriga, M.; Brach, J.S.; Wert, D.M.; Jerez-Roig, J.; Guerra-Balic, M.; Oviedo, G.R.; Fortuño, J.; Gómara-Toldrà, N.; Soto-Bagaria, L.; et al. Exercise-Based Interventions to Enhance Long-Term Sustainability of Physical Activity in Older Adults: A Systematic Review and Meta-Analysis of Randomized Clinical Trials. Int. J. Environ. Res. Public Health 2019, 16, 2527. [Google Scholar] [CrossRef] [PubMed]
- Schuch, F.B.; Bulzing, R.A.; Meyer, J.; Vancampfort, D.; Firth, J.; Stubbs, B.; Grabovac, I.; Willeit, P.; Tavares, V.D.O.; Calegaro, V.C.; et al. Associations of moderate to vigorous physical activity and sedentary behavior with depressive and anxiety symptoms in self-isolating people during the COVID-19 pandemic: A cross-sectional survey in Brazil. Psychiatry Res. 2020, 292, 113339. [Google Scholar] [CrossRef] [PubMed]
- Teychenne, M.; White, R.L.; Richards, J.; Schuch, F.B.; Rosenbaum, S.; Bennie, J.A. Do we need physical activity guidelines for mental health: What does the evidence tell us? Ment. HealthPhys. Act. 2020, 18, 100315. [Google Scholar] [CrossRef]


{kind=link}
| Inclusion Criteria | Exclusion Criteria |
|---|---|
| 1. Empirical research and peer-reviewed articles | 1. The study could not be retrieved. |
| 2. The study is within the theoretical frameworks of biomedicine, genetics, and pharmacy. | |
| 2. Study population: 2.1. Participants are aged 18 or older | 3. Study population: 3.1 Participants are pregnant women, people with physical disabilities, and/or prisoners 3.2. Participants are individuals who are not yet adults (infants, children, teenagers) 3.3. Participants suffer from a particular illness |
| 3. Time period: 3.1. Published from 1 January 2019 to 15 July 2020 | 4. Type of publication contains no original data such as reports, opinion studies, essays or comments, case studies, reviews, and no research. |
| 4. Publication criteria: 4.1. Written in English and/or Spanish 4.2. Any country 4.3. Have an abstract | |
| 5. Type of publication contains: lifestyle habits, anxiety levels, association between psychological distress and changes in health behaviors, preservation of PA during the pandemic, obstacles and facilitators of PA, psychopathological symptoms, impact of the COVID-19 outbreak |
| Databases | Articles |
|---|---|
| MEDLINE | 107 |
| APA PsycInfo | 60 |
| CINAHL Complete | 6 |
| Psychology and Behavioral Sciences Collection | 3 |
| Library, Information Science & Technology Abstracts | 2 |
| APA PsycArticles | 1 |
| GreenFILE | 1 |
| Authors | Setting of Target Population | Study Design | Sample Size | Age Range | Gender/Sex | Population | Recruitment |
|---|---|---|---|---|---|---|---|
| Ahmad, 2020 [25] | Canada | Intervention | n = 113 | --- | M = 28 F = 85 | Undergraduate | Online |
| Antunes, 2020 [31] | Portugal | Cross-sectional design | n = 1404 | 18 and older | F = 977 M = 426 Prefer not to specify = 1 | General population | Social media and newspapers |
| Becerra-García, 2020 [23] | Spain | A cross-sectional pilot study | n = 151 | 18–76 years | --- | General population | Online |
| Huckins, 2020 [22] | United States | Longitudinalmultimodal study | n = 217 | 18 to 22 years | F = 147 M = 70 | University students | Not mentioned |
| Lesser, 2020 [35] | Canada | Cross-sectional design | n = 1098 | 19 and older | F = 871 M = 215 | General population | Twitter, Facebook, and LinkedIn; local newspaper; national news network |
| Maugeri, 2020 [32] | Italy | Cross-sectional design | n = 2524 | 18 and older | F = 1426 M = 1098 | General population | Instagram, LinkedIn, Facebook, WhatsApp, and email |
| Pillay, 2020 [34] | South Africa | Cross-sectional study | n = 692 | 18 and older | F = 225 M = 463 Prefer not to say = 4 | Semi-elite athletes | |
| Shanahan, 2020 [24] | Zurich | Prospective-longitudinal study Type: Longitudinal cohort study | n = 1180 n = 786 | 20–22 years | --- | Young adults | Online survey |
| Shechter, 2020 [30] | United States | Cross-sectional design | n = 657 | 18 or older | F = 509 M = 143 Genderqueer = 1 Prefer not to answer r = 4 | Healthcare workers | |
| Stanton, 2020 [33] | Australia | Descriptive statistics; Non-parametric analysis: Kruskal–Wallis test, Wilcoxon rank-sum, and Spearman’s correlation; Linear regression; Logistic regression; Crude odds ratios | n = 1491 Sample: 1491 adults | 18–45 years | F = 484 M = 999 | General population | Online survey (Qualtrics survey platform) Social media sources and institutional outreach |
| Vasconcelos, 2020 [29] | Brazil | Cross-sectional design | n = 16.440 | 18 or older | F = 11344 M = 5096 | General population | WhatsApp, Instagram, and Facebook |
| Wu, 2020 [27] | China | Experimental design | n = 120 | 25–59 years | F = 89 M = 31 | Front-line clinicalstaff | Not mentioned |
| Zachary, (2020) [6] | United States | Quantitative descriptive/correlational design | n = 173 | 18 or older | F = 96 M = 77 | General population | |
| Zhang, 2020a [26] | Multiple provinces across China | Longitudinal survey design | n = 66 | Average = 20.70 years | F = 41 M = 25 | University students | WeChat moments and WeChat pushes |
| Zhang, 2020b [28] | China | Cross-sectional design | n = 369 | Average = 36.6 years | F = 165 M = 204 | General population | Not mentioned |
| Authors. | Goals | Measurement (Instruments) | Outcomes |
|---|---|---|---|
| Ahmad, 2020 [25] | To study the MVC a intervention and its effects in depression, anxiety, stress, quality of life, life satisfaction, and mindfulness. |
|
|
| Antunes, 2020 [31] | To observe lifestyle habits, anxiety levels and BPN c during the COVID-19 d pandemic. |
|
|
| Becerra-Garcia, 2020 [23] | To analyze psychopathological symptoms during the COVID-19 quarantine based on sociodemographic, occupational, and environmental-contextual variables. |
|
|
| Huckins, 2020 [22] | To study behaviors and mental health during the COVID-19 pandemic. To study the relationship between COVID-19 news and mental health changes. |
|
|
| Lesser, 2020 [35] | To study the impacts of the COVID-19 pandemic and public health constraints. To report changes in PA obstacles, facilitators, engagement, and well-being. To investigate differences in outdoor PA. |
|
|
| Maugeri, 2020 [32] | To study changes in PA levels during the lockdown. To analyze the impacts of PA on mental health. |
|
|
| Pillay, 2020 [34] | To study athletes’ perceptions on returning to their sports. To investigate maintaining PA during the pandemic. To study the athletes’ knowledge of COVID-19, mental health, sleep, health care access, and nutrition. |
|
|
| Shanahan, 2020 [24] | To observe emotional distress in young adults related to COVID-19. |
|
|
| Shechter, 2020 [30] | To describe health care workers’ distress, coping behaviors, and preferences. |
|
|
| Stanton, 2020 [33] | To study the association between psychological distress and changes in health behaviors during the COVID-19 pandemic. |
|
|
| Vasconcelos, 2020 [29] | To describe people’s behavior and how they were affected during COVID-19 quarantine. |
|
|
| Wu, 2020 [27] | To study the changes in psychological factors and sleep status in COVID-19 front-line medical staff. To show evidence of exercise interventions to relieve psychological stress and improve sleep quality. |
|
|
| Zachary, 2020 [6] | To quantify COVID-19 self-quarantine impacts on behaviors associated with weight gain. |
|
|
| Zhang, 2020a [26] | To study the adverse impacts of the COVID-19 outbreak on mental health, understand its underlying mechanisms, and explore coping strategies. |
|
|
| Zhang, 2020b [28] | To assess health and well-being of adults living and working after one month of COVID-19 outbreak. |
|
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Violant-Holz, V.; Gallego-Jiménez, M.G.; González-González, C.S.; Muñoz-Violant, S.; Rodríguez, M.J.; Sansano-Nadal, O.; Guerra-Balic, M. Psychological Health and Physical Activity Levels during the COVID-19 Pandemic: A Systematic Review. Int. J. Environ. Res. Public Health 2020, 17, 9419. https://doi.org/10.3390/ijerph17249419
Violant-Holz V, Gallego-Jiménez MG, González-González CS, Muñoz-Violant S, Rodríguez MJ, Sansano-Nadal O, Guerra-Balic M. Psychological Health and Physical Activity Levels during the COVID-19 Pandemic: A Systematic Review. International Journal of Environmental Research and Public Health. 2020; 17(24):9419. https://doi.org/10.3390/ijerph17249419
Chicago/Turabian StyleViolant-Holz, Verónica, M. Gloria Gallego-Jiménez, Carina S. González-González, Sarah Muñoz-Violant, Manuel José Rodríguez, Oriol Sansano-Nadal, and Myriam Guerra-Balic. 2020. "Psychological Health and Physical Activity Levels during the COVID-19 Pandemic: A Systematic Review" International Journal of Environmental Research and Public Health 17, no. 24: 9419. https://doi.org/10.3390/ijerph17249419
APA StyleViolant-Holz, V., Gallego-Jiménez, M. G., González-González, C. S., Muñoz-Violant, S., Rodríguez, M. J., Sansano-Nadal, O., & Guerra-Balic, M. (2020). Psychological Health and Physical Activity Levels during the COVID-19 Pandemic: A Systematic Review. International Journal of Environmental Research and Public Health, 17(24), 9419. https://doi.org/10.3390/ijerph17249419