How Have Public Safety Personnel Seeking Digital Mental Healthcare Been Affected by the COVID-19 Pandemic? An Exploratory Mixed Methods Study

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Context and Timeline
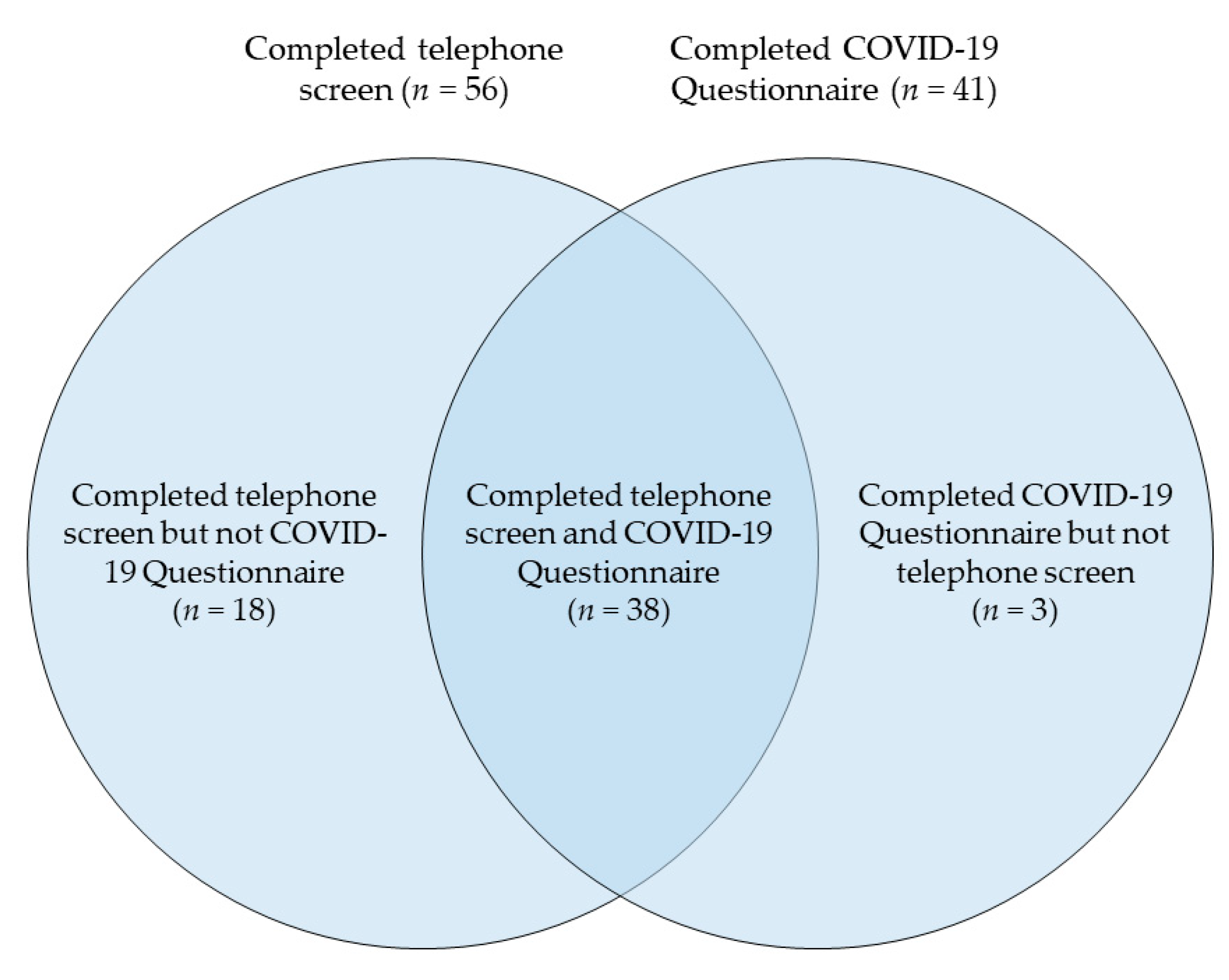
2.2. Procedure and Participants
2.3. Data and Analysis
3. Results
3.1. Participant Characteristics
3.2. Results of COVID-19 Questionnaire
3.3. Results of Qualitative Analyses of Telephone Screens
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Canadian Institute for Public Safety Research and Treatment. Glossary of Terms: A Shared Understanding of the Common Terms Used to Describe Psychological Trauma (Version 2.0). 2019. Available online: https://www.cipsrt-icrtsp.ca/en/resources/glossary-of-terms (accessed on 26 October 2020).
- Carleton, R.N.; Afifi, T.O.; Turner, S.; Taillieu, T.; Duranceau, S.; LeBouthillier, D.M.; Sareen, J.; Ricciardelli, R.; MacPhee, R.S.; Groll, D.; et al. Mental Disorder Symptoms among Public Safety Personnel in Canada. Can. J. Psychiatry 2018, 63, 54–64. [Google Scholar] [CrossRef] [PubMed]
- Carleton, R.N.; Afifi, T.O.; Turner, S.; Taillieu, T.; LeBouthillier, D.M.; Duranceau, S.; Sareen, J.; Ricciardelli, R.; MacPhee, R.S.; Groll, D.; et al. Suicidal ideation, plans, and attempts among public safety personnel in Canada. Can. Psychol./Psychol. Can. 2018, 59, 220–231. [Google Scholar] [CrossRef]
- Statistics Canada. Rates of Selected Mental or Substance Use Disorders, Lifetime and 12 Month, Canada, Household Population 15 and Older; Government of Canada: Ottawa, ON, Canada, 2012. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/advice-for-public (accessed on 26 October 2020).
- Carleton, R.N.; Afifi, T.O.; Taillieu, T.; Turner, S.; Krakauer, R.; Anderson, G.S.; MacPhee, R.S.; Ricciardelli, R.; Cramm, H.A.; Groll, D.; et al. Exposures to potentially traumatic events among public safety personnel in Canada. Can. J. Behav. Sci./Rev. Can. Des Sci. Du Comport. 2019, 51, 37–52. [Google Scholar] [CrossRef]
- Van Ameringen, M.; Mancini, C.; Patterson, B.; Boyle, M.H. Post-Traumatic Stress Disorder in Canada. Cns Neurosci. Ther. 2008, 14, 171–181. [Google Scholar] [CrossRef]
- American Psychiatric Association (Ed.) Diagnostic and Statistical Manual of Mental Disorders: DSM-5, 5th ed.; American Psychiatric Association: Washington, DC, USA, 2013; ISBN 978-0-89042-554-1. [Google Scholar]
- Carleton, R.N.; Afifi, T.O.; Taillieu, T.; Turner, S.; Mason, J.E.; Ricciardelli, R.; McCreary, D.R.; Vaughan, A.D.; Anderson, G.S.; Krakauer, R.L.; et al. Assessing the Relative Impact of Diverse Stressors among Public Safety Personnel. Intern. J. Environ. Res. Public Health 2020, 17, 1234. [Google Scholar] [CrossRef]
- Carleton, R.N.; Afifi, T.O.; Turner, S.; Taillieu, T.; Vaughan, A.D.; Anderson, G.S.; Ricciardelli, R.; MacPhee, R.S.; Cramm, H.A.; Czarnuch, S.; et al. Mental health training, attitudes toward support, and screening positive for mental disorders. Cogn. Behav. Ther. 2020, 49, 55–73. [Google Scholar] [CrossRef]
- Ricciardelli, R.; Czarnuch, S.; Carleton, R.N.; Gacek, J.; Shewmake, J. Canadian Public Safety Personnel and Occupational Stressors: How PSP Interpret Stressors on Duty. Int. J. Environ. Res. Public Health 2020, 17, 4736. [Google Scholar] [CrossRef]
- World Health Organization. Coronavirus Disease (COVID-19) Advice for the Public 2020. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/advice-for-public (accessed on 26 October 2020).
- Paluszek, M.M.; Landry, C.A.; Taylor, S.; Asmundson, G.J.G. The psychological sequelae of the COVID-19 pandemic: Psychological processes, current reearch ventures, and preparing for a postpandemic world. Behav. Ther. 2020, 43, 158–163. Available online: https://www.researchgate.net/profile/Michelle_Paluszek/publication/342258521_The_Psychological_Sequelae_of_the_COVID-19_Pandemic_Psychological_Processes_Current_Research_Ventures_and_Preparing_for_a_Postpandemic_World/links/5efe0bd8a6fdcc4ca444ed94/The-Psychological-Sequelae-of-the-COVID-19-Pandemic-Psychological-Processes-Current-Research-Ventures-and-Preparing-for-a-Postpandemic-World.pdf (accessed on 26 October 2020).
- Shultz, J.M.; Espinel, Z.; Flynn, B.W.; Hoffman, Y.; Cohen, R.E. DEEP PREP: All-Hazards Disaster Behavioural Health Training; Disaster Life Support Publishing: Tampa, FL, USA, 2007. [Google Scholar]
- Taylor, S. The Psychology of Pandemics: Preparing for the Next Global Outbreak of Infectious Disease; Cambridge Scholars Publishing: Newcastle Upon Tyne, UK, 2019; ISBN 978-1-5275-4118-4. [Google Scholar]
- Cao, W.; Fang, Z.; Hou, G.; Han, M.; Xu, X.; Dong, J.; Zheng, J. The psychological impact of the COVID-19 epidemic on college students in China. Psychiatry Res. 2020, 287, 112934. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Pan, R.; Wan, X.; Tan, Y.; Xu, L.; Ho, C.S.; Ho, R.C. Immediate Psychological Responses and Associated Factors during the Initial Stage of the 2019 Coronavirus Disease (COVID-19) Epidemic among the General Population in China. Int. J. Environ. Res. Public Health 2020, 17, 1729. [Google Scholar] [CrossRef]
- Taylor, S.; Landry, C.A.; Paluszek, M.M.; Fergus, T.A.; McKay, D.; Asmundson, G.J.G. Development and initial validation of the COVID Stress Scales. J. Anxiety Disord. 2020, 72, 102232. [Google Scholar] [CrossRef] [PubMed]
- Titov, N.; Staples, L.; Kayrouz, R.; Cross, S.; Karin, E.; Ryan, K.; Dear, B.; Nielssen, O. Rapid report: Early demand, profiles and concerns of mental health users during the coronavirus (COVID-19) pandemic. Internet Interv. 2020, 21, 100327. [Google Scholar] [CrossRef] [PubMed]
- Qiu, J.; Shen, B.; Zhao, M.; Wang, Z.; Xie, B.; Xu, Y. A nationwide survey of psychological distress among Chinese people in the COVID-19 epidemic: Implications and policy recommendations. Gen. Psychiatry 2020, 33, e100213. [Google Scholar] [CrossRef] [PubMed]
- Taylor, S.; Landry, C.A.; Paluszek, M.M.; Fergus, T.A.; McKay, D.; Asmundson, G.J.G. COVID stress syndrome: Concept, structure, and correlates. Depress. Anxiety 2020, 37, 706–714. [Google Scholar] [CrossRef]
- Stogner, J.; Miller, B.L.; McLean, K. Police Stress, Mental Health, and Resiliency during the COVID-19 Pandemic. Am. J. Crim. Justice 2020, 45, 718–730. [Google Scholar] [CrossRef]
- Heber, A.; Testa, V.; Smith-MacDonald, L.; Brémault-Phillips, S.; Carleton, R.N. Rapid response to COVID-19: Addressing challenges and increasing the mental readiness of public safety personnel. Health Promot. Chronic Dis. Prev. Can. Res. Policy Pract. 2020, 40, 350–355. [Google Scholar] [CrossRef]
- McCall, H.C.; Hadjistavropoulos, H.D.; Burnett, J.L.; Beahm, J.D.; Carleton, R.N.; Fournier, A.K. Stakeholder perspectives on internet-delivered cognitive behavioural therapy for public safety personnel: A qualitative analysis. Can. J. Behav. Sci. 2020, in press. [Google Scholar] [CrossRef]
- Ricciardelli, R.; Carleton, R.N.; Mooney, T.; Cramm, H. “Playing the system”: Structural factors potentiating mental health stigma, challenging awareness, and creating barriers to care for Canadian public safety personnel. Health (Lond.) 2020, 24, 259–278. [Google Scholar] [CrossRef]
- Andersson, G. Internet-Delivered Psychological Treatments. Annu. Rev. Clin. Psychol. 2016, 12, 157–179. [Google Scholar] [CrossRef]
- Donker, T.; Blankers, M.; Hedman, E.; Ljótsson, B.; Petrie, K.; Christensen, H. Economic evaluations of Internet interventions for mental health: A systematic review. Psychol. Med. 2015, 45, 3357–3376. [Google Scholar] [CrossRef]
- McCall, H.C.; Sison, A.P.; Burnett, J.L.; Beahm, J.D.; Hadjistavropoulos, H.D. Exploring Perceptions of Internet-Delivered Cognitive Behaviour Therapy among Public Safety Personnel: Informing Dissemination Efforts. Int. J. Environ. Res. Public Health 2020, 17, 6026. [Google Scholar] [CrossRef] [PubMed]
- Government of Canada. Coronavirus Disease (COVID-19): Outbreak Update—Canada.ca. 2020. Available online: https://web.archive.org/web/20200623024826/https://www.canada.ca/en/public-health/services/diseases/2019-novel-coronavirus-infection.html?topic=tilelink (accessed on 24 October 2020).
- Giles, D. Saskatchewan Confirms First Presumptive Case of Novel Coronavirus. Global News. 2020. Available online: https://globalnews.ca/news/6666466/coronavirus-saskatchewan-covid-19-coronavirus-saskatoon/ (accessed on 24 October 2020).
- Giles, D. Saskatchewan Declares State of Emergency as Coronavirus Concerns Grow|Globalnews.ca. 2020. Available online: https://web.archive.org/web/20200318221045/https://globalnews.ca/news/6698018/saskatchewan-state-of-emergency-covid-19-coronavirus/ (accessed on 24 October 2020).
- COVID-19. Government of Saskatchewan. Available online: https://www.saskatchewan.ca/government/health-care-administration-and-provider-resources/treatment-procedures-and-guidelines/emerging-public-health-issues/2019-novel-coronavirus (accessed on 24 November 2020).
- Foss, C.; Ellefsen, B. The value of combining qualitative and quantitative approaches in nursing research by means of method triangulation. J. Adv. Nurs. 2002, 40, 242–248. [Google Scholar] [CrossRef] [PubMed]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B.W. The PHQ-9: Validity of a brief depression severity measure. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef] [PubMed]
- Spitzer, R.L.; Kroenke, K.; Williams, J.B.W.; Löwe, B. A Brief Measure for Assessing Generalized Anxiety Disorder: The GAD-7. Arch. Intern. Med. 2006, 166, 1092. [Google Scholar] [CrossRef] [PubMed]
- Blevins, C.A.; Weathers, F.W.; Davis, M.T.; Witte, T.K.; Domino, J.L. The Posttraumatic Stress Disorder Checklist for DSM-5 (PCL-5): Development and Initial Psychometric Evaluation: Posttraumatic Stress Disorder Checklist for DSM-5. J. Trauma. Stress 2015, 28, 489–498. [Google Scholar] [CrossRef] [PubMed]
- Ehrenreich-May, J. Fear of Illness and Virus Evaluation Scales. 2020. Available online: https://adaa.org/sites/default/files/UofMiamiFear%20of%20Illness%20and%20Virus%20Evaluation%20(FIVE)%20scales%20for%20Child-%2C%20Parent-%20and%20Adult-Report.pdf (accessed on 24 October 2020).
- Kroenke, K.; Spitzer, R.L.; Williams, J.B.W.; Löwe, B. The Patient Health Questionnaire Somatic, Anxiety, and Depressive Symptom Scales: A systematic review. Gen. Hosp. Psychiatry 2010, 32, 345–359. [Google Scholar] [CrossRef] [PubMed]
- Bovin, M.J.; Marx, B.P.; Weathers, F.W.; Gallagher, M.W.; Rodriguez, P.; Schnurr, P.P.; Keane, T.M. Psychometric properties of the PTSD Checklist for Diagnostic and Statistical Manual of Mental Disorders–Fifth Edition (PCL-5) in veterans. Psychol. Assess. 2016, 28, 1379–1391. [Google Scholar] [CrossRef] [PubMed]
- Manea, L.; Gilbody, S.; McMillan, D. Optimal cut-off score for diagnosing depression with the Patient Health Questionnaire (PHQ-9): A meta-analysis. Can. Med. Assoc. J. 2012, 184, E191–E196. [Google Scholar] [CrossRef]
- Levis, B.; Benedetti, A.; Ioannidis, J.P.A.; Sun, Y.; Negeri, Z.; He, C.; Wu, Y.; Krishnan, A.; Bhandari, P.M.; Neupane, D.; et al. Patient Health Questionnaire-9 scores do not accurately estimate depression prevalence: Individual participant data meta-analysis. J. Clin. Epidemiol. 2020, 122, 115–128.e1. [Google Scholar] [CrossRef]
- Wortmann, J.H.; Jordan, A.H.; Weathers, F.W.; Resick, P.A.; Dondanville, K.A.; Hall-Clark, B.; Foa, E.B.; Young-McCaughan, S.; Yarvis, J.S.; Hembree, E.A.; et al. Psychometric analysis of the PTSD Checklist-5 (PCL-5) among treatment-seeking military service members. Psychol. Assess. 2016, 28, 1392–1403. [Google Scholar] [CrossRef]
- QSR International. NVivo 12 Qualitative Data Analysis Software. 2018. Available online: https://www.qsrinternational.com/nvivo-qualitative-data-analysis-software/home (accessed on 26 October 2020).
- Hsieh, H.-F.; Shannon, S.E. Three Approaches to Qualitative Content Analysis. Qual. Health Res. 2005, 15, 1277–1288. [Google Scholar] [CrossRef] [PubMed]
- Lu, W.; Wang, H.; Lin, Y.; Li, L. Psychological status of medical workforce during the COVID-19 pandemic: A cross-sectional study. Psychiatry Res. 2020, 288, 112936. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristic | Participants Who Completed COVID-19 Questionnaire (n = 41) | Participants Who Completed Telephone Screen (n = 56) | All Participants (N = 59) | |
|---|---|---|---|---|
| Age, M (SD) | 40.13 (10.80) | 39.73 (10.20) | 39.73 (10.20) | |
| Gender, n (%) | ||||
| Woman | 24 (59) | 32 (57) | 34 (58) | |
| Man | 16 (39) | 24 (43) | 24 (41) | |
| Other | 1 (2) | 0 | 1 (2) | |
| Ethnicity, n (%) | ||||
| White | 32 (78) | 45 (80) | 46 (78) | |
| First Nations, Inuit, or Metis | 7 (17) | 7 (13) | 9 (15) | |
| Other | 2 (5) | 4 (7) | 4 (7) | |
| Married or common law, n (%) | ||||
| Yes | 21 (51) | 31 (55) | 32 (54) | |
| No | 20 (49) | 25 (45) | 27 (46) | |
| Children, n (%) | ||||
| Yes | 19 (46) | 27 (48) | 27 (46) | |
| No | 22 (54) | 29 (52) | 32 (54) | |
| Community size, n (%) | ||||
| Population of 100,000 or greater | 15 (37) | 30 (54) | 27 (46) | |
| Population under 100,000 | 26 (63) | 26 (46) | 32 (54) | |
| PSP Sector, n (%) | ||||
| Police | 14 (34) | 21 (38) | 21 (36) | |
| Corrections | 8 (20) | 9 (16) | 10 (17) | |
| Emergency Medical Service | 8 (20) | 11 (20) | 12 (20) | |
| Fire | 4 (10) | 4 (7) | 4 (7) | |
| Dispatch/Communications | 3 (7) | 5 (9) | 5 (8) | |
| Other | 4 (10) | 6 (11) | 7 (12) | |
| Clinical characteristics, M (SD) | ||||
| PHQ-9 score | 12.76 (6.30) | 12.11 (6.16) | 12.17 (6.28) | |
| GAD-7 score | 11.51 (5.92) | 10.79 (5.74) | 10.63 (5.77) | |
| PCL-5 score | 31.95 (19.68) | 30.93 (20.11) | 30.76 (19.61) | |
| Item | Frequency of Responses, n (%) | Mean Response, SD | |||
|---|---|---|---|---|---|
| I Am Not Afraid of This at All (0) | I Am Afraid of This Some of the Time (1) | I Am Afraid of This Most of the Time (2) | I Am Afraid of This All of the Time (3) | ||
| 1. I am afraid I may get COVID-19. | 16 (39) | 22 (54) | 2 (5) | 1 (2) | 0.71 (0.68) |
| 2. I am afraid I will get very, very sick if I catch COVID-19. | 19 (46) | 18 (44) | 1 (2) | 3 (7) | 0.71 (0.84) |
| 3. I am afraid I will have to go to the hospital because of COVID-19. | 26 (63) | 14 (34) | 0 | 1 (2) | 0.41 (0.63) |
| 4. I am afraid I might die if I get COVID-19. | 27 (66) | 12 (29) | 1 (2) | 1 (2) | 0.41 (0.67) |
| 5. I am afraid my pet might get COVID-19. | 33 (80) | 6 (15) | 2 (5) | 0 | 0.24 (0.54) |
| 6. I am afraid a family member might get sick or die because of COVID-19. | 5 (12) | 21 (51) | 9 (22) | 6 (15) | 1.39 (0.89) |
| 7. I am afraid I may do something that would cause someone else to get COVID-19. | 12 (29) | 20 (49) | 4 (10) | 5 (12) | 1.05 (0.95) |
| 8. I am afraid a friend might get sick or die because of COVID-19. | 18 (44) | 18 (44) | 5 (12) | 0 | 0.68 (0.69) |
| 9. I am afraid people in the world might get sick or die because of COVID-19. | 25 (61) | 12 (29) | 4 (10) | 0 | 0.49 (0.68) |
| Impact | Participants (n = 41) | |
|---|---|---|
| COVID-19 status, n (%) | ||
| Recovered | 1 (2) | |
| Never infected | 40 (98) | |
| Someone close to participant has had COVID-19, n (%) | ||
| Yes | 5 (12) | |
| No | 36 (88) | |
| Childcare issues related to COVID-19, n (%) | ||
| Yes | 6 (15) | |
| No | 13 (32) | |
| No children | 22 (54) | |
| Lost job or income due to COVID-19, n (%) | ||
| Yes | 4 (10) | |
| No | 37 (90) | |
| Impact of COVID-19 on ability to meet financial obligations, n (%) | ||
| Too soon to tell | 1 (2) | |
| No impact | 4 (10) | |
| Minor impact | 4 (10) | |
| Moderate impact | 29 (71) | |
| Major impact | 3 (7) | |
| Concern about ability to maintain physical distance at work, n (%) | ||
| Yes | 23 (56) | |
| No | 18 (44) | |
| Difficulties with feeling socially isolated due to COVID-19, n (%) | ||
| Yes | 15 (37) | |
| No | 26 (63) | |
| Being afraid of COVID-19 has gotten in the way of enjoying life, n (%) | ||
| Not true for participant at all | 24 (59) | |
| Somewhat true | 16 (39) | |
| Mostly true | 1 (2) | |
| Definitely true | 0 | |
| Being afraid of COVID-19 has caused strong emotions, n (%) | ||
| Not true for participant at all | 18 (44) | |
| Somewhat true | 17 (41) | |
| Mostly true | 4 (10) | |
| Definitely true | 2 (5) | |
| Domain/Theme | Definition | Participants (n = 56) | |
|---|---|---|---|
| Negative emotions, n (%) | 22 (39) | ||
| Fear of others contracting COVID-19 | Fears about loved ones or co-workers contracting the virus, getting sick, or dying. | 12 (21) | |
| Fear of contracting COVID-19 | Fears about themselves contracting the virus, getting sick, or dying. | 8 (14) | |
| Isolation | Negative emotions resulting from physical distancing measures leading to isolation. | 5 (9) | |
| Boredom | Boredom due to closures. | 3 (5) | |
| General stress | Increased overall stress levels. | 5 (9) | |
| Logistical impacts, n (%) | 17 (30) | ||
| Impact on work | Concerns included increased call volumes, the inability of the healthcare system to manage the impact of COVID-19, and concerns about management not taking the pandemic seriously. | 6 (11) | |
| Financial concerns | Financial concerns included reduced business in secondary businesses, partners losing job/income, or reduced shifts/hours. | 6 (11) | |
| Reduced access to support | Closures affecting access to support for participants themselves or their family members. | 5 (9) | |
| Impact on home life | Concerns were related to not having access to childcare and having to navigate a new routine. | 4 (7) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
McCall, H.; Beahm, J.; Landry, C.; Huang, Z.; Carleton, R.N.; Hadjistavropoulos, H. How Have Public Safety Personnel Seeking Digital Mental Healthcare Been Affected by the COVID-19 Pandemic? An Exploratory Mixed Methods Study. Int. J. Environ. Res. Public Health 2020, 17, 9319. https://doi.org/10.3390/ijerph17249319
McCall H, Beahm J, Landry C, Huang Z, Carleton RN, Hadjistavropoulos H. How Have Public Safety Personnel Seeking Digital Mental Healthcare Been Affected by the COVID-19 Pandemic? An Exploratory Mixed Methods Study. International Journal of Environmental Research and Public Health. 2020; 17(24):9319. https://doi.org/10.3390/ijerph17249319
Chicago/Turabian StyleMcCall, Hugh, Janine Beahm, Caeleigh Landry, Ziyin Huang, R. Nicholas Carleton, and Heather Hadjistavropoulos. 2020. "How Have Public Safety Personnel Seeking Digital Mental Healthcare Been Affected by the COVID-19 Pandemic? An Exploratory Mixed Methods Study" International Journal of Environmental Research and Public Health 17, no. 24: 9319. https://doi.org/10.3390/ijerph17249319
APA StyleMcCall, H., Beahm, J., Landry, C., Huang, Z., Carleton, R. N., & Hadjistavropoulos, H. (2020). How Have Public Safety Personnel Seeking Digital Mental Healthcare Been Affected by the COVID-19 Pandemic? An Exploratory Mixed Methods Study. International Journal of Environmental Research and Public Health, 17(24), 9319. https://doi.org/10.3390/ijerph17249319