Relationships of Fat and Muscle Mass with Chronic Kidney Disease in Older Adults: A Cross-Sectional Pilot Study

 ,
,  ,
, 
Abstract
1. Introduction
2. Materials and Methods
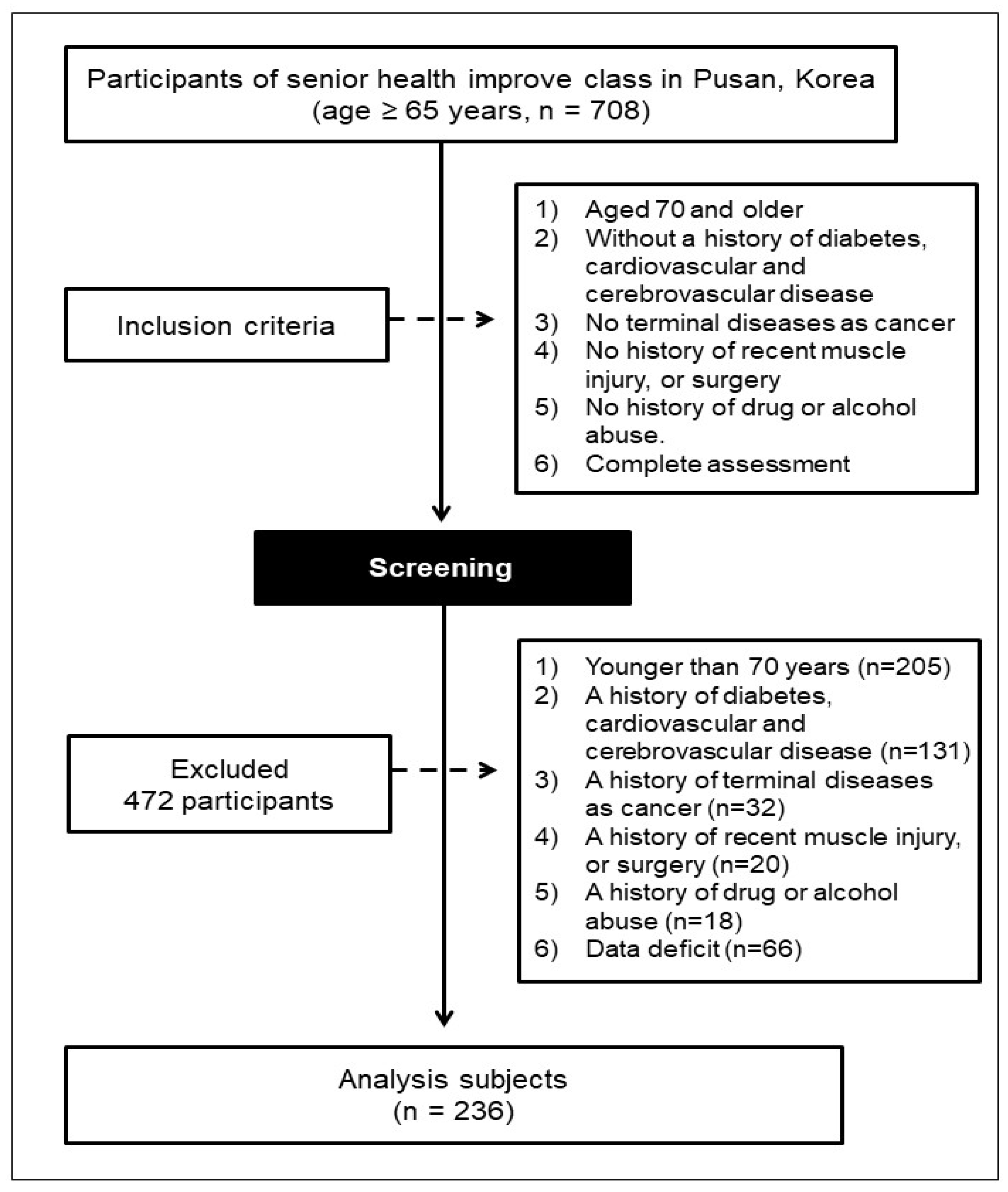
2.1. Participants
2.2. Anthropometry and Body Composition
2.3. Estimated Glomerular Filtration rate (eGFR) and Biochemical Measurements
2.4. Statistical Analysis
3. Results
3.1. Characteristics of the Study Participants and the Differences between Men and Women
3.2. Anthropometric Parameters
3.3. Body Composition Parameters
3.4. Biochemical Parameters
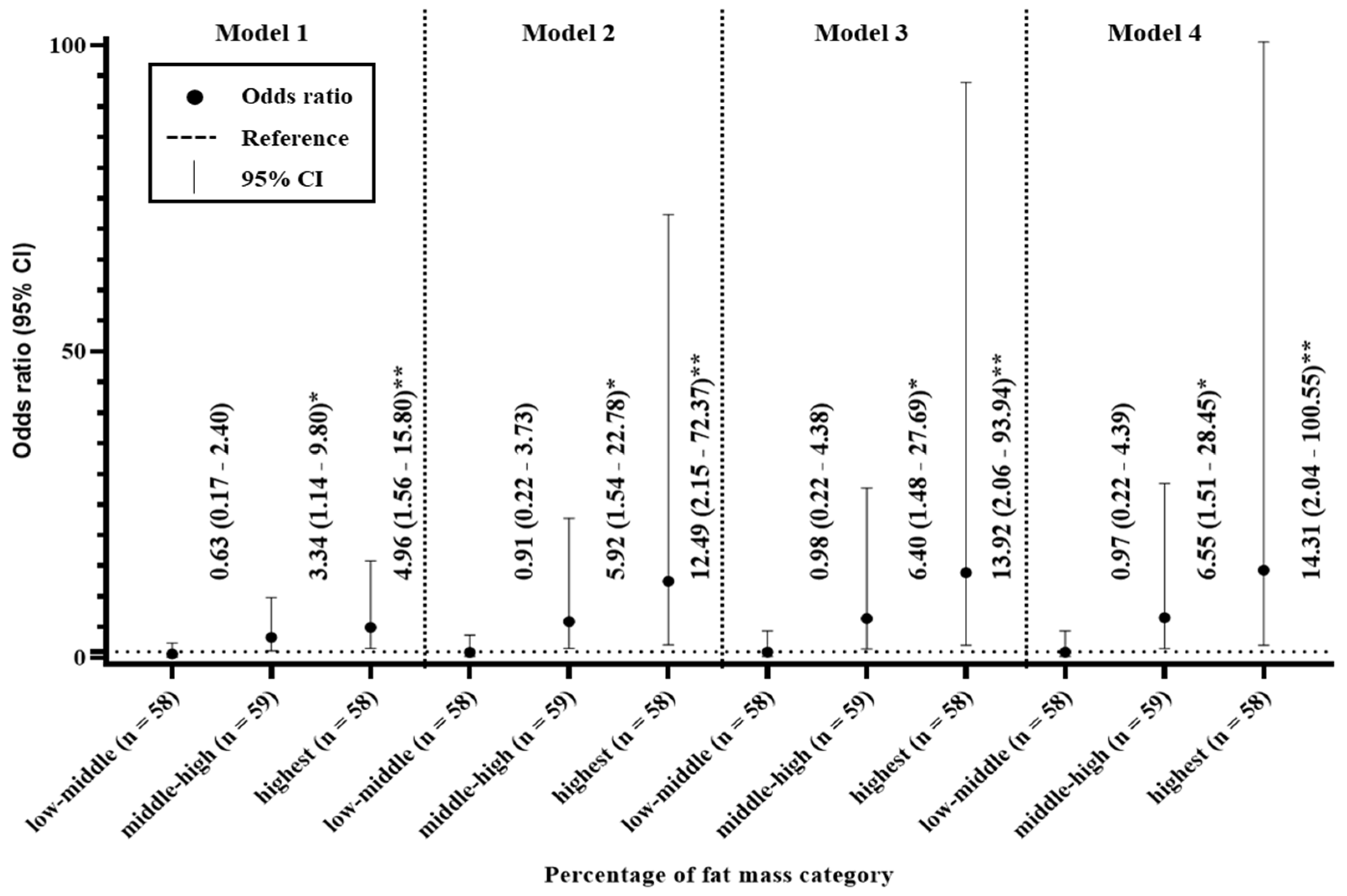
3.5. Odds Ratios for the Percentage of Fat Mass
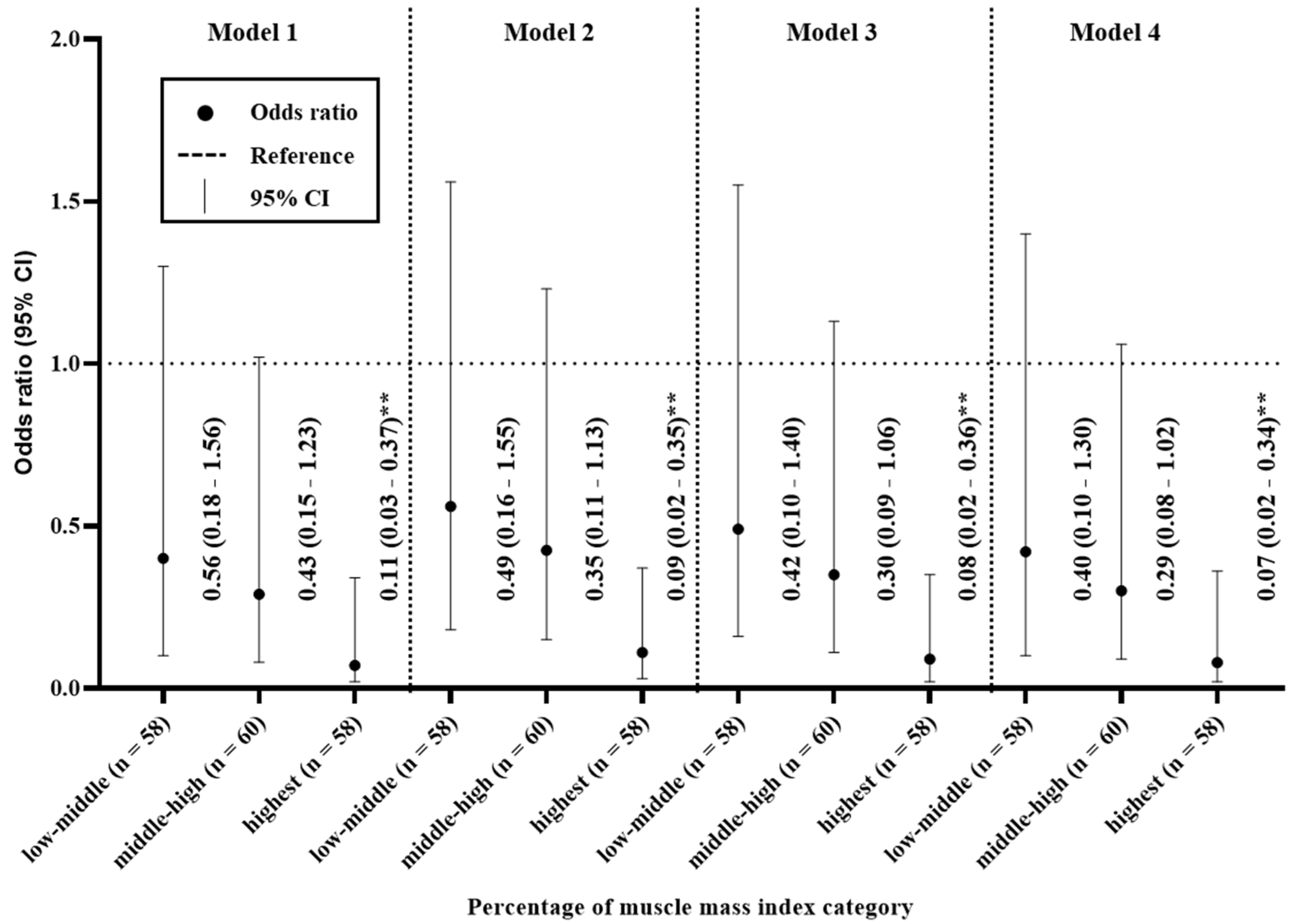
3.6. Odds Ratios for the Percentage of Muscle Mass Index
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Tsujimoto, T.; Sairenchi, T.; Iso, H.; Irie, F.; Yamagishi, K.; Watanabe, H.; Tanaka, K.; Muto, T.; Ota, H. The dose-response relationship between body mass index and the risk of incident stage ≥3 chronic kidney disease in a general Japanese population: The Ibaraki prefectural health study (IPHS). J. Epidemiol. 2014, 24, 444–451. [Google Scholar] [CrossRef]
- Zhang, L.; Wang, F.; Wang, L.; Wang, W.; Liu, B.; Liu, J.; Chen, M.; He, Q.; Liao, Y.; Yu, X.; et al. Prevalence of chronic kidney disease in China: A cross-sectional survey. Lancet 2012, 379, 815–822. [Google Scholar] [CrossRef]
- Imai, E.; Horio, M.; Watanabe, T.; Iseki, K.; Yamagata, K.; Hara, S.; Ura, N.; Kiyohara, Y.; Moriyama, T.; Ando, Y.; et al. Prevalence of chronic kidney disease in the Japanese general population. Clin. Exp. Nephrol. 2009, 13, 621–630. [Google Scholar] [CrossRef]
- Kang, H.T.; Lee, J.; Linton, J.A.; Park, B.J.; Lee, Y.J. Trends in the prevalence of chronic kidney disease in Korean adults: The Korean National Health and Nutrition Examination Survey from 1998 to 2009. Nephrol. Dial. Transplant. 2013, 28, 927–936. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Coresh, J.; Selvin, E.; Stevens, L.A.; Manzi, J.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Levey, A.S. Prevalence of chronic kidney disease in the United States. JAMA 2007, 298, 2038–2047. [Google Scholar] [CrossRef] [PubMed]
- Ejerblad, E.; Fored, C.M.; Lindblad, P.; Fryzek, J.; McLaughlin, J.K.; Nyren, O. Obesity and risk for chronic renal failure. J. Am. Soc. Nephrol. 2006, 17, 1695–1702. [Google Scholar] [CrossRef] [PubMed]
- Chadban, S.J.; Briganti, E.M.; Kerr, P.G.; Dunstan, D.W.; Welborn, T.A.; Zimmet, P.Z.; Atkins, R.C. Prevalence of kidney damage in Australian adults: The AusDiab kidney study. J. Am. Soc. Nephrol. 2003, 14, 131–138. [Google Scholar] [CrossRef]
- Rothman, K.J. BMI-related errors in the measurement of obesity. Int. J. Obes. 2008, 32, 56–59. [Google Scholar] [CrossRef]
- Burkhauser, R.V.; Cawley, J. Beyond BMI: The value of more accurate measures of fatness and obesity in social science research. J. Health Econ. 2008, 27, 519–529. [Google Scholar] [CrossRef]
- Evans, W.J. Skeletal muscle loss: Cachexia, sarcopenia, and inactivity. Am. J. Clin. Nutr. 2010, 91, 1123S–1127S. [Google Scholar] [CrossRef]
- Hamdy, O.; Porramatikul, S.; Al-Ozairi, E. Metabolic obesity: The paradox between visceral and subcutaneous fat. Curr. Diabetes Rev. 2006, 2, 367–373. [Google Scholar] [PubMed]
- Sharma, D.; Hawkins, M.; Abramowitz, M.K. Association of sarcopenia with eGFR and misclassification of obesity in adults with CKD in the United States. Clin. J. Am. Soc. Nephrol. 2014, 9, 2079–2088. [Google Scholar] [CrossRef] [PubMed]
- Kim, B.; Tsujimoto, T.; So, R.; Zhao, X.; Oh, S.; Tanaka, K. Changes in muscle strength after diet-induced weight reduction in adult men with obesity: A prospective study. Diabetes Metab. Syndr. Obes. 2017, 10, 187–194. [Google Scholar] [CrossRef] [PubMed]
- Kim, B.; Tsujimoto, T.; So, R.; Zhao, X.; Oh, S.; Tanaka, K. Weight reduction does not induce an undesirable decrease in muscle mass, muscle strength, or physical performance in men with obesity: A pilot study. J. Exerc. Nutr. Biochem. 2017, 21, 37–44. [Google Scholar] [CrossRef]
- Matsuo, S.; Imai, E.; Horio, M.; Yasuda, Y.; Tomita, K.; Nitta, K.; Yamagata, K.; Tomino, Y.; Yokoyama, H.; Hishida, A. Revised equations for estimated GFR from serum creatinine in Japan. Am. J. Kidney Dis. 2009, 53, 982–992. [Google Scholar] [CrossRef]
- Lee, S.; Shimada, H.; Park, H.; Makizako, H.; Lee, S.; Doi, T.; Yoshida, D.; Tsutsumimoto, K.; Anan, Y.; Suzuki, T. The association between kidney function and cognitive decline in community-dwelling, elderly Japanese people. J. Am. Med. Dir. Assoc. 2015, 16, 349.e1–394.e5. [Google Scholar] [CrossRef]
- Hsu, C.Y.; McCulloch, C.E.; Iribarren, C.; Darbinian, J.; Go, A.S. Body mass index and risk for end-stage renal disease. Ann. Intern. Med. 2006, 144, 21–28. [Google Scholar] [CrossRef]
- Iseki, K.; Ikemiya, Y.; Kinjo, K.; Inoue, T.; Iseki, C.; Takishita, S. Body mass index and the risk of development of end-stage renal disease in a screened cohort. Kidney Int. 2004, 65, 1870–1876. [Google Scholar] [CrossRef]
- Kim, J.K.; Song, Y.R.; Kwon, Y.J.; Kim, H.J.; Kim, S.G.; Ju, Y.S. Increased body fat rather than body weight has harmful effects on 4-year changes of renal function in the general elderly population with a normal or mildly impaired renal function. Clin. Interv. Aging 2014, 9, 1277–1286. [Google Scholar] [CrossRef]
- Chen, Y.Y.; Fang, W.H.; Wang, C.C.; Kao, T.W.; Chang, Y.W.; Yang, H.F.; Wu, C.J.; Sun, Y.S.; Chen, W.L. Changes of percent body fat as a useful surrogate for risk of declined renal function. Sci. Rep. 2018, 8, 17289. [Google Scholar] [CrossRef]
- Henegar, J.R.; Bigler, S.A.; Henegar, L.K.; Tyagi, S.C.; Hall, J.E. Functional and structural changes in the kidney in the early stages of obesity. J. Am. Soc. Nephrol. 2001, 12, 1211–1217. [Google Scholar] [PubMed]
- Li, F.Y.; Cheng, K.K.; Lam, K.S.; Vanhoutte, P.M.; Xu, A. Cross-talk between adipose tissue and vasculature: Role of adiponectin. Acta Physiol. 2011, 203, 167–180. [Google Scholar] [CrossRef]
- Gu, P.; Xu, A. Interplay between adipose tissue and blood vessels in obesity and vascular dysfunction. Rev. Endocr. Metab. Disord. 2013, 14, 49–58. [Google Scholar] [CrossRef] [PubMed]
- Xu, A.; Vanhoutte, P.M. Adiponectin and adipocyte fatty acid binding protein in the pathogenesis of cardiovascular disease. Am. J. Physiol. Heart Circ. Physiol. 2012, 302, 1231–1240. [Google Scholar] [CrossRef] [PubMed]
- Malmstrom, T.K.; Miller, D.K.; Herning, M.M.; Morley, J.E. Low appendicular skeletal muscle mass (ASM) with limited mobility and poor health outcomes in middle-aged African Americans. J. Cachexia Sarcopenia Muscle 2013, 4, 179–186. [Google Scholar] [CrossRef] [PubMed]
- Zamboni, M.; Mazzali, G.; Fantin, F.; Rossi, A.; Di Francesco, V. Sarcopenic obesity: A new category of obesity in the elderly. Nutr. Metab. Cardiovasc Dis. 2008, 18, 388–395. [Google Scholar] [CrossRef] [PubMed]
- Workeneh, B.T.; Mitch, W.E. Review of muscle wasting associated with chronic kidney disease. Am. J. Clin. Nutr. 2010, 91, 1128–1132. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Total (n = 236) | Men (n = 47) | Women (n = 189) | p Value | |
|---|---|---|---|---|
| Age, year | 76.8 ± 3.7 | 77.3 ± 3.7 | 76.7 ± 3.7 | =0.25 |
| Height, cm | 155.7 ± 6.8 | 155.5 ± 6.0 | 155.7 ± 7.0 | =0.83 |
| Body weight, kg | 60.0 ± 8.7 | 58.2 ± 8.4 | 60.4 ± 8.7 | =0.11 |
| BMI, kg/m2 | 24.8 ± 3.2 | 24.1 ± 3.2 | 24.9 ± 3.1 | =0.09 |
| LM, kg | 37.2 ± 5.7 | 36.1 ± 5.3 | 37.5 ± 5.8 | =0.13 |
| ASM, kg | 15.4 ± 3.2 | 15.2 ± 3.7 | 15.5 ± 3.0 | =0.55 |
| MMI, kg/m2 | 6.3 ± 1.0 | 6.3 ± 1.5 | 6.3 ± 0.8 | =0.65 |
| %MMI, % | 25.8 ± 4.5 | 26.3 ± 7.0 | 25.6 ± 3.6 | =0.37 |
| %FM, % | 37.5 ± 7.7 | 37.5 ± 7.6 | 37.5 ± 7.7 | =0.96 |
| SBP, mm Hg | 139.1 ± 18.3 | 145.0 ± 17.8 | 137.7 ± 18.2 | <0.05 |
| DBP, mm Hg | 74.3 ± 11.3 | 78.3 ± 12.4 | 73.3 ± 10.8 | <0.05 |
| CRE, mg/dL | 0.8 ± 0.2 | 1.0 ± 0.2 | 0.8 ± 0.2 | <0.01 |
| eGFR, mg/dL | 57.7 ± 12.4 | 58.9 ± 11.8 | 57.4 ± 12.6 | =0.44 |
| TC, mg/dL | 184.3 ± 36.3 | 176.5 ± 34.2 | 186.3 ± 36.6 | =0.10 |
| HDLC, mg/dL | 53.7 ± 13.7 | 50.3 ± 13.0 | 54.5 ± 13.8 | =0.06 |
| TG, mg/dL | 131.2 ± 61.5 | 125.8 ± 53.1 | 132.5 ± 63.5 | =0.51 |
| FPG, mg/dL | 99.6 ± 23.2 | 102.7 ± 19.8 | 98.8 ± 23.9 | =0.31 |
| Insulin, IU | 8.8 ± 7.7 | 8.5 ± 7.2 | 8.9 ± 7.8 | =0.77 |
| Smoking (yes) | 5.1 % (12) | 4.3 % (2) | 5.3 % (10) | =0.77 |
| Alcohol (yes) | 25.0 % (59) | 19.1 % (9) | 26.5 % (50) | =0.30 |
| eGFR Category (mL/min/1.73 m2) | Post Hoc | b SS | p for b Trend | |||
|---|---|---|---|---|---|---|
| (A) eGFR ≥ 60 | (B) eGFR 45–59.9 | (C) eGFR < 45 | ||||
| (n = 102) | (n = 98) | (n = 36) | ||||
| # Age, year | 76.1 (75.4, 76.8) | 77.2 (76.5, 77.9) | 77.6 (76.3, 78.3) | NS | 2.54 | <0.05 |
| a Height, cm | 159.0 (157.8, 160.2) | 153.7 (152.4,154.9) | 151.5 (149.5, 153.6) | A > B, C | −6.40 | <0.01 |
| Body weight, kg | 61.6 (59.9, 63.3) | 59.2 (57.5, 60.9) | 57.6 (54.7, 60.4) | A > C | −2.48 | <0.05 |
| BMI, kg/m2 | 24.5 (23.7, 25.0) | 25.0 (24.4, 25.6) | 25.1 (24.1, 26.1) | NS | 1.53 | =0.13 |
| eGFR Category (mL/min/1.73 m2) | Post Hoc | b SS | p for b Trend | |||
|---|---|---|---|---|---|---|
| (A) eGFR ≥ 60 | (B) eGFR 45–59.9 | (C) eGFR < 45 | ||||
| (n = 102) | (n = 98) | (n = 36) | ||||
| LM, kg | 39.8 (38.8, 40.9) | 35.4 (34.4, 36.4) | 34.6 (32.9, 36.3) | A > B, C | −5.51 | <0.01 |
| ASM, kg | 16.8 (16.2, 17.3) | 14.6 (14.0, 15.2) | 13.8 (12.8, 14.7) | A > B, C | −5.60 | <0.01 |
| MMI, kg/m2 | 6.6 (6.4, 6.8) | 6.2 (6.0, 6.4) | 6.0 (5.7, 6.3) | A > B, C | −3.95 | <0.01 |
| %MMI, % | 27.2 (26.3, 28.0) | 24.9 (24.0, 25.8) | 24.0 (22.6, 25.5) | A > B, C | −5.47 | <0.01 |
| %FM, % | 35.0 (33.6, 36.5) | 39.5 (38.0, 41.0) | 39.3 (36.8, 41.7) | A < B, C | 4.27 | <0.01 |
| eGFR Category (mL/min/1.73 m2) | Post Hoc | b SS | p for b Trend | |||
|---|---|---|---|---|---|---|
| (A) eGFR ≥ 60 | (B) eGFR 45-59.9 | (C) eGFR < 45 | ||||
| (n = 102) | (n = 98) | (n = 36) | ||||
| SBP, mm Hg | 138.0 (134.4, 141.5) | 141.7 (138.1, 145.3) | 135.5 (129.5, 141.4) | NS | 0.48 | =0.63 |
| DBP, mm Hg | 73.3 (71.4, 75.8) | 76.3 (74.1, 78.5) | 70.9 (67.2, 74.5) | B > C | −0.61 | =0.54 |
| CRE, mg/dL | 0.7 (0.65, 0.69) | 0.8 (0.8, 0.9) | 1.1 (1.1, 1.2) | A < B < C | 12.66 | <0.01 |
| eGFR, mg/dL | 68.8 (67.7, 70.0) | 53.2 (52.1, 54.3) | 38.3 (36.4, 40.1) | A > B > C | −15.45 | <0.01 |
| TC, mg/dL | 189.3 (182.3, 196.2) | 183.8 (176.7, 190.9) | 171.6 (159.9, 183.4) | A > C | −2.58 | <0.05 |
| HDLC, mg/dL | 56.0 (53.3, 58.6) | 53.3 (50.7, 56.0) | 48.3 (43.8, 52.7) | A > C | −2.64 | <0.01 |
| TG, mg/dL | 120.7 (108.7, 132.7) | 135.2 (123.0, 147.4) | 150.0 (129.9, 170.1) | A < C | 3.15 | <0.01 |
| FPG, mg/dL | 97.3 (92.9, 101.8) | 97.1 (92.6, 101.6) | 112.7 (105.2, 120.1) | A, B < C | 1.96 | =0.05 |
| Insulin, IU | 7.8 (6.2, 9.3) | 9.7 (8.2, 11.2) | 9.6 (7.0, 12.1) | NS | 2.43 | <0.05 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, B.; Park, H.; Kim, G.; Isobe, T.; Sakae, T.; Oh, S. Relationships of Fat and Muscle Mass with Chronic Kidney Disease in Older Adults: A Cross-Sectional Pilot Study. Int. J. Environ. Res. Public Health 2020, 17, 9124. https://doi.org/10.3390/ijerph17239124
Kim B, Park H, Kim G, Isobe T, Sakae T, Oh S. Relationships of Fat and Muscle Mass with Chronic Kidney Disease in Older Adults: A Cross-Sectional Pilot Study. International Journal of Environmental Research and Public Health. 2020; 17(23):9124. https://doi.org/10.3390/ijerph17239124
Chicago/Turabian StyleKim, Bokun, Hyuntae Park, Gwonmin Kim, Tomonori Isobe, Takeji Sakae, and Sechang Oh. 2020. "Relationships of Fat and Muscle Mass with Chronic Kidney Disease in Older Adults: A Cross-Sectional Pilot Study" International Journal of Environmental Research and Public Health 17, no. 23: 9124. https://doi.org/10.3390/ijerph17239124
APA StyleKim, B., Park, H., Kim, G., Isobe, T., Sakae, T., & Oh, S. (2020). Relationships of Fat and Muscle Mass with Chronic Kidney Disease in Older Adults: A Cross-Sectional Pilot Study. International Journal of Environmental Research and Public Health, 17(23), 9124. https://doi.org/10.3390/ijerph17239124