High Variability in Implementation of Selective-Prevention Services for Cardiometabolic Diseases in Five European Primary Care Settings


 , ,
, ,  ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Design and Settings
2.2. Participants
2.3. Procedures and Outcomes
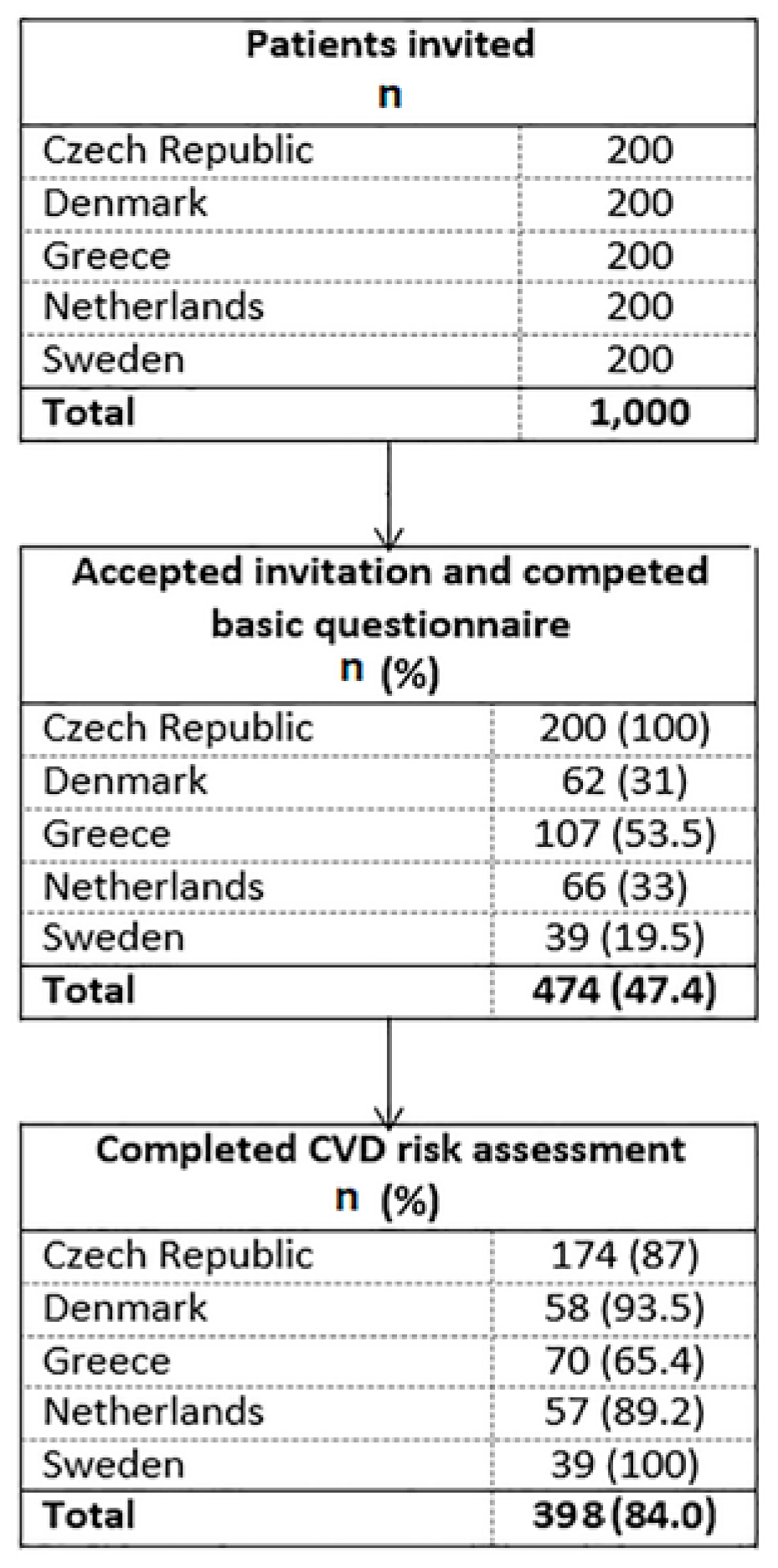
- Identification and invitation of 200 participants: Eligible participants were identified via primary care practice patient lists. They were invited to the study either personally by the staff of the practice (the Czech Republic, Greece, the Netherlands and Sweden), or—in the case of Denmark—via patients’ digital mailbox (a digital mail-system provided by the government for secure and direct communication between individuals, public authorities and other trusted organizations). The recruitment period ran from April through October 2018 at all sites.
- Initial assessment of participant CMD-risk profile: An online questionnaire, developed and based on the European Social Survey (http://www.europeansocialsurvey.org), was used. The questionnaire was either administered to participants by practice personnel or research assistants during a face-to-face consultation (the Czech Republic, Greece, the Netherlands and Sweden) or completed by participants online (Denmark). The questionnaire recorded demographic characteristics (age, gender, education, work status, insurance and income) and lifestyle-related CMD-risk factors (smoking, alcohol consumption, physical activity and nutrition).
- Comprehensive CVD-risk assessment: Each country selected a tool for CVD-risk measurement, based on the ESC or national guidelines [6]. Locally validated tools used in clinical practice in each country were selected to facilitate the local adaptation of the planned implementation. In the Czech Republic and Greece, country-adjusted versions of the European Heart SCORE were used [12]. In Sweden, Svenska Score (or SCORE Sweden) was selected [13]. In Denmark and the Netherlands, the modified Heartscore BMI score [14] and the Dutch Prevention Consultation Cardiometabolic Risk (PC CMR) [15] were used, respectively. Upon assessment, participants were verbally informed about their CVD-risk, and where relevant, provided with practical advice on how to reduce it.
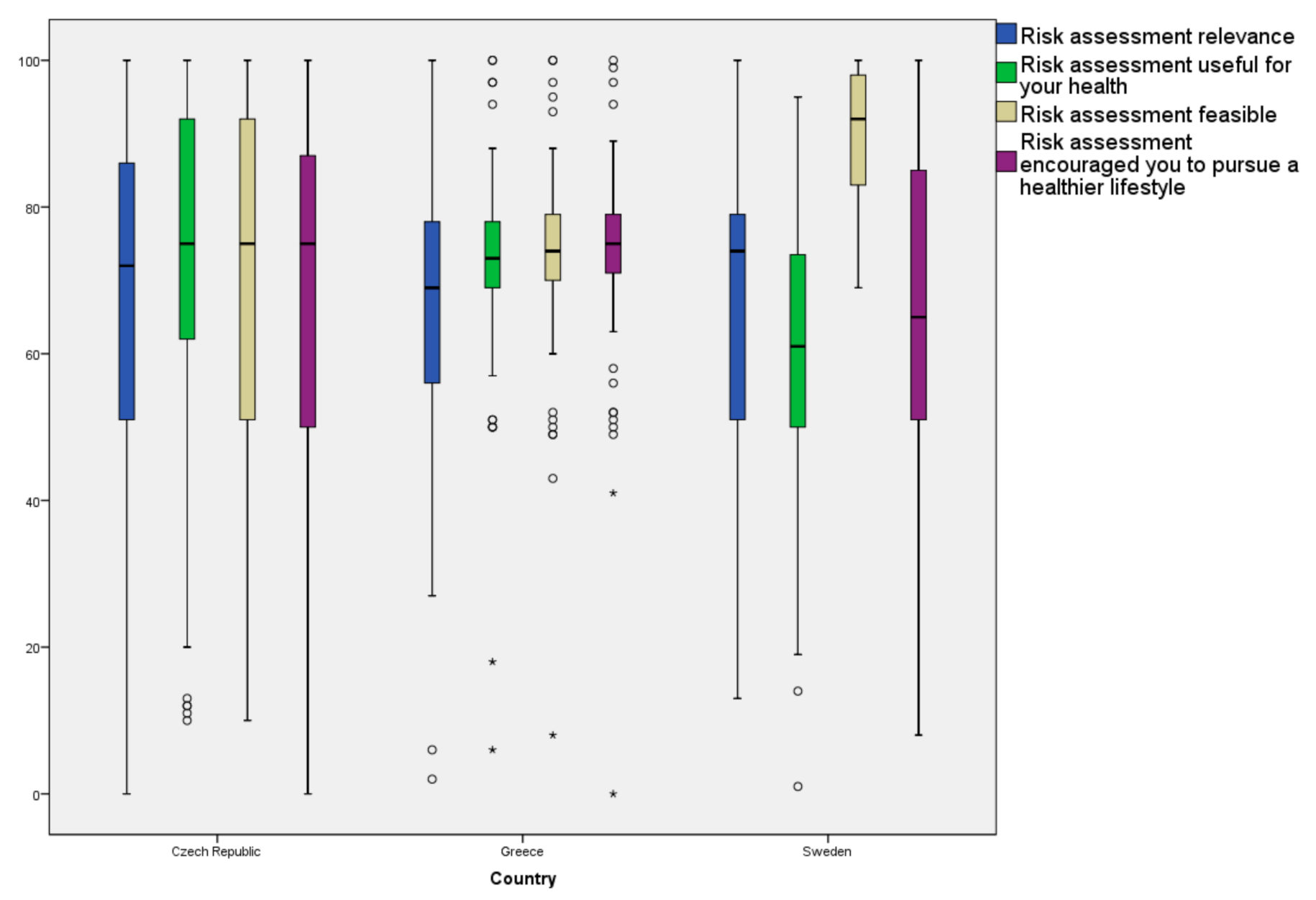
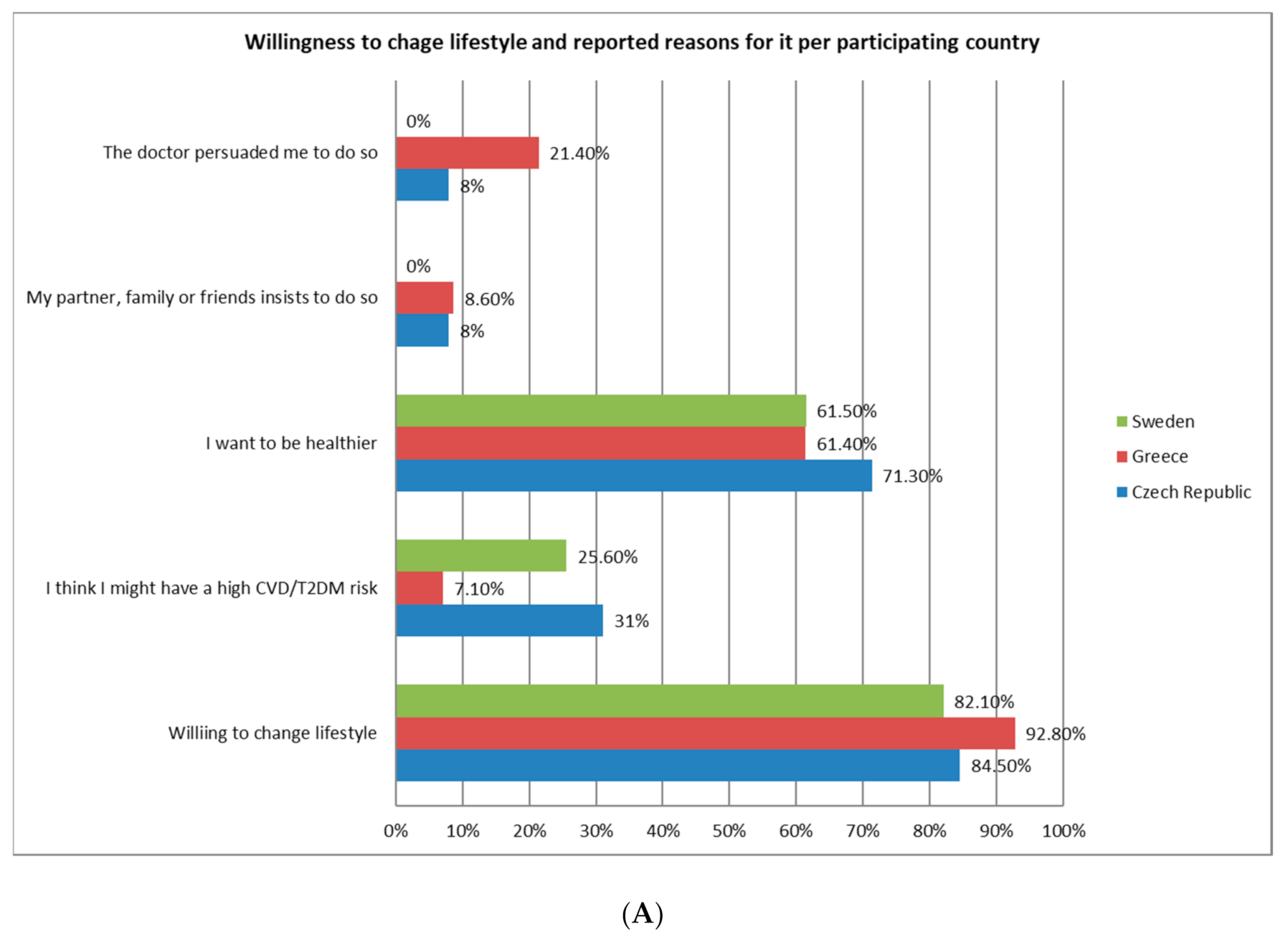
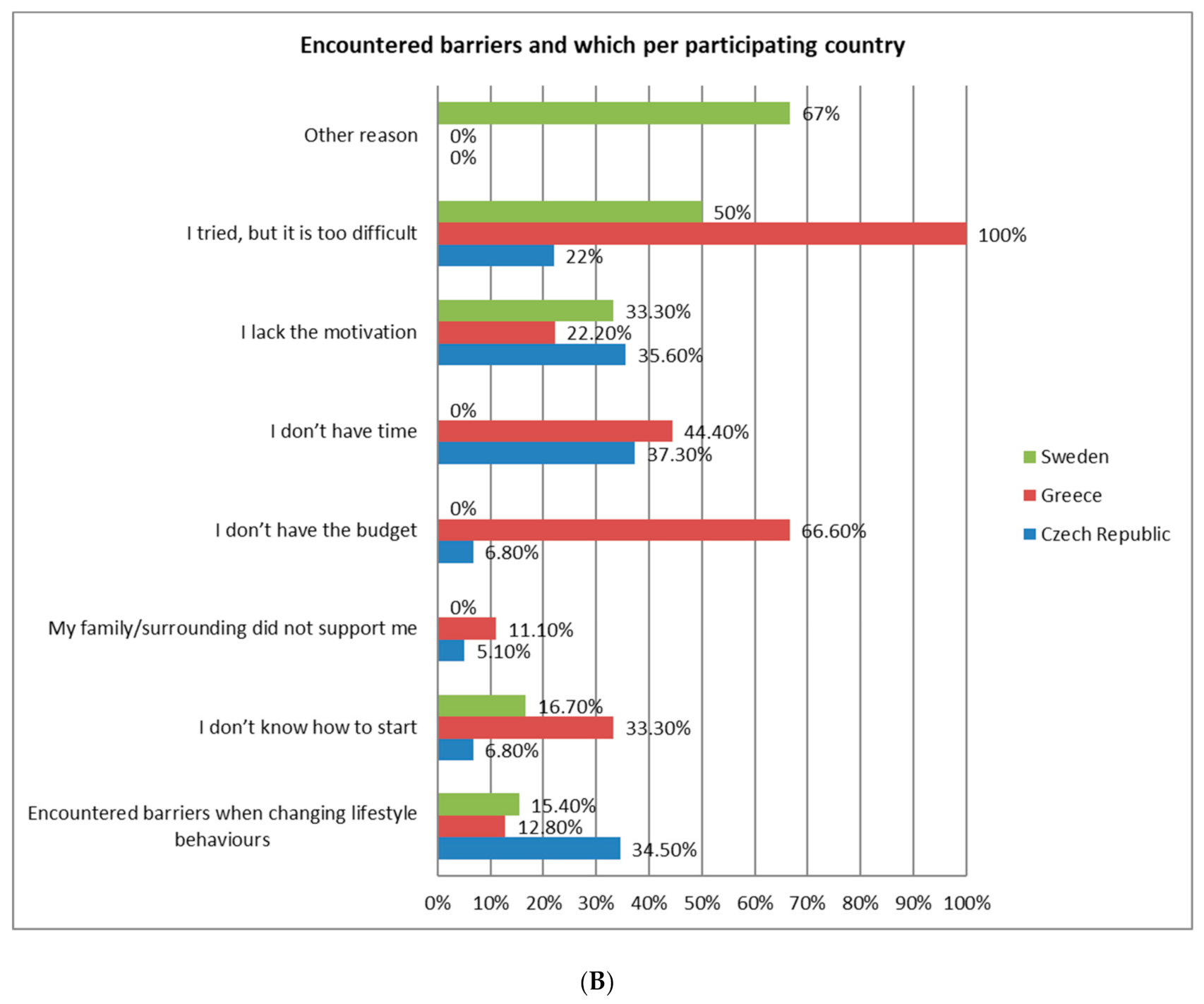
- Participant evaluation of the implementation selective-preventive services: On a ten-point Likert scale, participants were asked to assess the relevance, usefulness and feasibility of the selective-prevention services, as well as the extent to which it encouraged a healthier lifestyle. Participants’ willingness to change risk behavior, as well as any encountered barriers to lifestyle modification, were also assessed.
- Numbers and proportions of patients who accepted the invitation and completed their CMD-risk profiling (feasibility)
- Numbers and proportions of participants who completed the comprehensive CVD-risk assessment (feasibility)
- Participant-reported intervention relevance, usefulness, feasibility and impact in pursuing a healthier lifestyle, along with respective barriers (evaluation)
2.4. Statistical Analysis
2.5. Ethics
3. Results
3.1. Recruitment
3.2. Participants
3.3. CMD-Risk Profiling
3.4. CVD-Risk Assessment
3.5. Participant Evaluation of the Intervention
3.6. Perception and Barriers Towards Lifestyle Modification
4. Discussion
4.1. Summary of Findings and Comparison with Literature
4.2. Strengths and Limitations
4.3. Study Implications
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Townsend, N.; Wilson, L.; Bhatnagar, P.; Wickramasinghe, K.; Rayner, M.; Nichols, M. Cardiovascular disease in Europe: Epidemiological update 2016. Eur. Heart J. 2016, 37, 3232–3245. [Google Scholar] [CrossRef] [PubMed]
- WHO. Global Action Plan for the Prevention and Control of NCDs WHO Library Cataloguing-In-Publication Data. Global Action Plan for the Prevention and Control of Noncommunicable Diseases 2013–2020; WHO Press, World Health Organization: Geneva, Switzerland, 2019; ISBN 978 92 4 150623 6. [Google Scholar]
- James, W.P. The epidemiology of obesity: The size of the problem. J. Intern. Med. 2008, 263, 336–352. [Google Scholar] [CrossRef] [PubMed]
- Yusuf, S.; Reddy, S.; Ounpuu, S.; Anand, S. Global burden of cardiovascular diseases: Part II: Variations in cardiovascular disease by specific ethnic groups and geographic regions and prevention strategies. Circulation 2001, 104, 2855–2864. [Google Scholar] [CrossRef] [PubMed]
- Deaton, C.; Froelicher, E.S.; Wu, L.H.; Ho, C.; Shishani, K.; Jaarsma, T. The global burden of cardiovascular disease. J. Cardiovasc. Nurs. 2011, 26 (Suppl. 4), S5–S14. [Google Scholar] [CrossRef]
- Piepoli, M.F.; Hoes, A.W.; Agewall, S.; Albus, C.; Brotons, C.; Catapano, A.L.; Cooney, M.-T.; Corrà, U.; Cosyns, B.; Deaton, C.; et al. 2016 European guidelines on cardiovascular disease prevention in clinical practice. The Sixth Joint Task Force of the European Society of Cardiology and Other Societies on Cardiovascular Disease Prevention in Clinical Practice (constituted by representatives of 10 societies and by invited experts. Developed with the special contribution of the European Association for Cardiovascular Prevention & Rehabilitation). Eur. Heart J. 2016, 37, 2315–2381. [Google Scholar]
- Mrazek, P.J.; Haggerty, R.J. (Eds.) Reducing Risks for Mental Disorders: Frontiers for Preventive Intervention Research; National Academies Press (US): Washington, DC, USA, 1994; PMID: 25144015. [Google Scholar]
- Unal, B.; Critchley, J.A.; Capewell, S. Modelling the decline in coronary heart disease deaths in England and Wales, 1981–2000: Comparing contributions from primary prevention and secondary prevention. Br. Med. J. 2005, 331, 614. [Google Scholar] [CrossRef]
- Si, S.; Moss, J.R.; Sullivan, T.R.; Newton, S.S.; Stocks, N.P. Effectiveness of general practice-based health checks: A systematic review and meta-analysis. Br. J. Gen. Pract. 2014, 64, e47–e53. [Google Scholar] [CrossRef]
- De Waard, A.-K.M.; Hollander, M.; Korevaar, J.C.; Nielen, M.M.J.; Carlsson, A.C.; Lionis, C.; Seifert, B.; Thilsing, T.; De Wit, N.J.; Schellevis, F.G.; et al. Selective prevention of cardiometabolic diseases: Activities and attitudes of general practitioners across Europe. Eur. J. Public Health 2019, 29, 88–93. [Google Scholar] [CrossRef]
- Král, N.; de Waard, A.M.; Schellevis, F.G.; Korevaar, J.; Lionis, C.; Carlsson, A.C.; Sønderlund, A.L.; Søndergaard, J.; Larsen, L.B.; Hollander, M.; et al. What should selective cardiometabolic prevention programmes in European primary care look like? A consensus-based design by the SPIM-EU group. Eur. J. Gen. Pract. 2019, 25, 101–108. [Google Scholar] [CrossRef]
- Conroy, R.M.; Pyorala, K.; Fitzgerald, A.P.; Sans, S.; Menotti, A.; De Backer, G.; De Bacquer, D.; Ducimetière, P.; Jousilahti, P.; Keil, U.; et al. SCORE project group: Estimation of ten-year risk of fatal cardiovascular disease in Europe: The SCORE project. Eur. Heart J. 2003, 24, 987–1003. [Google Scholar] [CrossRef]
- Karjalainen, T.; Adiels, M.; Björck, L.; Cooney, M.T.; Graham, I.; Perk, J.; Rosengren, A.; Söderberg, S.; Eliasson, M. An evaluation of the performance of SCORE Sweden 2015 in estimating cardiovascular risk: The Northern Sweden MONICA Study 1999–2014. Eur. J. Prev. Cardiol. 2017, 24, 103–110. [Google Scholar] [CrossRef] [PubMed]
- Larsen, L.B.; Sonderlund, A.L.; Sondergaard, J.; Thomsen, J.L.; Halling, A.; Hvidt, N.C.; Hvidt, E.A.; Mønsted, T.; Pedersen, L.B.; Roos, E.M.; et al. Targeted prevention in primary care aimed at lifestyle-related diseases: A study protocol for a non-randomised pilot study. BMC Fam. Pract. 2018, 19, 124. [Google Scholar] [CrossRef] [PubMed]
- Dekker, J.M.; Alssema, M.; Janssen, P.G.H.; van der Paardt, M.; Festen, C.S.S.; van Oosterhout, M.J.W. NHG-standard Prevention Consultation cardiometabolic risk from the Dutch College of General Practitioners. Huisarts Wet 2011, 54, 138–155. [Google Scholar]
- OECD Statistics. Available online: https://www.oecd-ilibrary.org/docserver/9789264283404en.pdf?expires=1572474646&id=id&accname=guest&checksum=A2A41FB427AA628DB7F20BF18547D101 (accessed on 20 May 2019).
- Available online: https://www.folkhalsomyndigheten.se/folkhalsorapportering-statistik/tolkad-rapportering/folkhalsans-utveckling/levnadsvanor/tobaksrokning-daglig/ (accessed on 20 May 2019).
- Brotons, C.; Björkelund, C.; Bulc, M.; Ciurana, R.; Godycki-Cwirko, M.; Jurgova, E.; Kloppe, P.; Lionis, C.; Mierzecki, A.; Piñeiro, R.; et al. Prevention and health promotion in clinical practice: The views of general practitioners in Europe. Prev. Med. 2005, 40, 595–601. [Google Scholar] [CrossRef] [PubMed]
- van der Meer, V.; Nielen, M.M.; Drenthen, A.J.; van Vliet, M.; Assendelft, W.J.; Schellevis, F.G. Cardiometabolic prevention consultation in the Netherlands: Screening uptake and detection of cardiometabolic risk factors and diseases-a pilot study. BMC Fam. Pract. 2013, 14, 29. [Google Scholar] [CrossRef]
- de Waard, A.M.; Wandell, P.E.; Holzmann, M.J.; Korevaar, J.C.; Hollanderm, M.; Gornitzki, C.; De Wit, N.J.; Schellevis, F.G.; Lionis, C.; Søndergaard, J.; et al. Barriers and facilitators to participation in a health check for cardiometabolic diseases in primary care: A systematic review. Eur. J. Prev. Cardiol. 2018, 25, 1326–1340. [Google Scholar] [CrossRef]
- Wändell, P.; de Waard, A.-K.; Holzmann, M.; Gornitzki, C.; Lionis, C.; de Wit, N.; Søndergaard, J.; Sønderlund, A.L.; Král, N.; Seifert, B.; et al. Barriers and facilitators among health professionals in primary care to prevention of cardiometabolic diseases. A systematic review. Fam. Pract. 2018, 35, 383–398. [Google Scholar] [CrossRef]
- Lionis, C.; Petelos, E.; Papadakis, S.; Tsiligianni, I.; Anastasaki, M.; Angelaki, A.; Bertsias, A.; Mechili1, E.A.; Papadakaki1, M.; Sifaki-Pistolla, D.; et al. Towards evidence-informed integration of public health and primary health care: Experiences from Crete. WHO Public Health Panor. 2018, 4, 699–714. [Google Scholar]
- World Health Organization. Greek Health Reform: Opening of New Primary Health Care Units; WHO Press, World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- Available online: https://www.vzp.cz/pojistenci/prevence/preventivni-prohlidky (accessed on 11 March 2019). (In Czech).
- Dekker, J.M.; Alssema, M.; Janssen, P.G.; Goudswaard, L.N.; Werkgroup NHG. Summary of the practice guideline ‘The Prevention Visit’ from the Dutch College of General Practitioners. Ned. Tijdschr. Voor Geneeskd. 2011, 155, A3428. [Google Scholar]
- Norberg, M.; Wall, S.; Boman, K.; Weinehall, L. The Vasterbotten Intervention Programme: Background, design and implications. Glob. Health Action 2010, 3, 4643. [Google Scholar] [CrossRef]
- Sonderlund, A.L.; Thilsing, T.; Korevaar, J.; Hollander, M.; Lionis, C.; Schellevis, F.; Wändell, P.; Axel, C.; Carlsson, A.C.; de Waard, A.-K.; et al. An evidence-based toolboxfor thedesignand implementation of selective-prevention primary-care initiatives targeting cardiometabolic disease. Prev. Med. Rep. 2019, 16, 100979. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Czech Republic (N = 200) | Denmark (N = 62) | Greece (N = 107) | Netherlands (N = 66) | Sweden (N = 39) |
|---|---|---|---|---|---|
| Gender,n (%) | |||||
| Female | 121 (60.5) | 29 (46.8) | 34 (59.8) | 36 (54.5) | 27(69.2) |
| Male | 79 (39.5) | 33 (53.2) | 43 (40.2) | 30 (45.5) | 12 (30.8) |
| Age (years),mean (SD) | 50.0 (8.8) | 55.5 (6.3) | 52.7 (8.5) | 54.0 (10.3) | 51.1 (6.3) |
| Education,n (%) | |||||
| None | 0 (0) | 0 (0) | 5 (4.7) | 0 (0) | 0 (0) |
| Primary | 1 (0.5) | 1 (1.9) | 19 (17.8) | 1 (1.5) | 0 (0) |
| Secondary | 34 (17.2) | 8 (14.8) | 52 (48.6) | 12 (18.2) | 0 (0) |
| College/University | 163 (82.3) | 45 (83.4) | 31 (29) | 53 (80.3) | 39 (100) |
| Work status,n (%) | |||||
| Full-time | 131 (65.5) | 37 (59.7) | 62 (57.9) | 32 (48.5) | 36 (92.3) |
| Part-time | 30 (15) | 11 (17.7) | 22 (20.6) | 17 (25.8) | 2 (5.1) |
| Pensioner | 11 (5.5) | 8 (12.9) | 9 (8.4) | 12 (18.2) | 1 (2.6) |
| Unemployed | 4 (2) | 4 (6.5) | 14 (13.1) | 3 (4.5) | 0 (0) |
| Disabled | 24 (12) | 2 (3.2) | 0 (0) | 2 (3) | 0 (0) |
| Health insurance,n (%) | |||||
| Yes | 192 (96) | 26 (41.9) | 84 (79.2) | 66 (100) | 27 (69.2) |
| No | 3 (1.5) | 4 (6.5) | 21 (19.8) | 0 (0) | 7 (17.9) |
| Not applicable | 5 (2.5) | 32 (51.6) | 1 (0.9) | 0 (0) | 5 (12.8) |
| Income compared to country’s average,n (%) | |||||
| Lower | 44 (22) | 21 (34.4) | 67 (62.6) | 5 (7.7) | 3 (7.7) |
| Corresponding | 61 (30.7) | 22 (36.1) | 23 (21.5) | 35 (53.8) | 8 (20.5) |
| Higher | 84 (42.2) | 17 (27.9) | 0 (0) | 24 (36.9) | 24 (61.5) |
| Don’t know | 10 (5) | 1 (1.6) | 17 (15.9) | 1 (1.5) | 4 (10.3) |
| Variable | Czech Republic (n = 200) | Denmark (n = 62) | Greece (n = 107) | Netherlands (n = 66) | Sweden (n = 39) |
|---|---|---|---|---|---|
| Smoking,n (%) | |||||
| Never | 122 (61) | 24 (40) | 35 (32.7) | 36 (56.3) | 28 (71.8) |
| Quit over 6 monthsago | 34 (17) | 20 (33.3) | 16 (15) | 22 (34.4) | 8 (20.5) |
| Quit less than 6 monthsago | 3 (1.5) | 1 (1.7) | 1 (0.9) | 1 (1.6) | 1 (2.6%) |
| Occasionally | 13 (6.5) | 5 (8.3) | 9 (8.4) | 3 (4.7) | 0 (0) |
| Everyday | 28 (14) | 10 (16.7) | 46 (43) | 2 (3.1) | 2 (5.1) |
| Drinks/week,median (min, max; IQR) | 2 (0, 40; 6) | 4 (0, 60; 8) | 7 (0, 46; 9) | 2 (0, 70; 7) | 3 (0, 30; 5) |
| Consumption of ≥4 (female) or 5 (male) drinks on a single occasion,n (%) | |||||
| Everyday | 4 (2) | 4 (6.5) | 3 (2.8) | 2 (3.1) | 0 (0) |
| Once a week | 29 (14.5) | 8 (12.9%) | 12 (11.3) | 8 (12.5) | 4 (10.3) |
| Once a month | 48 (24) | 18 (29) | 11 (10.4) | 8 (12.5) | 8 (20.5) |
| Rarely | 86 (43) | 29 (46.8) | 31 (29.2) | 25 (39.1) | 24 (61.5) |
| Never | 33 (16) | 3 (4.8) | 49 (46.2) | 21 (32.8) | 3 (7.7) |
| Physical activity,n (%) | |||||
| Sedentary (rarely/never) | 29 (14.7) | 5 (8.1) | 21 (19.6) | 8 (12.1) | 4 (10.3) |
| Underactive (light/moderate, not weekly) | 62 (31.6) | 12 (25) | 51 (48.1) | 13 (20) | 10 (25.6) |
| Regular-light (light, weekly) | 146 (74.1) | 38 (67.9) | 75 (70.1) | 39 (60.9) | 33 (84.6) |
| Regular-moderate (moderate, weekly, ≤30 min/day) | 91 (46.4) | 29 (52.7) | 36 (33.6) | 29 (44.6) | 22 (56.4) |
| Regular-vigorous (vigorous, weekly, ≤20 min/day) | 59 (30.1) | 12 (23.5) | 10 (9.3) | 16 (24.2) | 16 (41) |
| Active-moderate (30 min moderate for ≥5 days/week) | 58 (29.4) | 26 (47.3) | 13 (12.1) | 28 (42.4) | 15 (38.5) |
| Active-vigorous (20 min vigorous for ≥3 days/week) | 33 (16.8) | 11 (20) | 10 (9.3) | 11 (17.5) | 11 (28.2) |
| Vegetable consumption,n (%) | |||||
| ≤once/week | 22 (11.1) | 2 (3.2) | 32 (29.9) | 0 (0) | 2 (5.1) |
| A few times/week | 89 (44.7) | 22 (35.5) | 62 (57.9) | 13 (20) | 5 (12.8) |
| Once/day | 71 (35.7) | 25 (40.3) | 12 (11.2) | 46 (70.8) | 24 (61.5) |
| ≥twice/day | 17 (8.5) | 13 (21) | 1 (0.9) | 6 (9.2) | 8 (20.5) |
| Fruit consumption,n (%) | |||||
| ≤once/week | 21 (10.5) | 9 (14.5) | 27 (25.2) | 2 (3.1) | 5 (12.8) |
| A few times/week | 71 (35.5) | 24 (38.7) | 57 (53.3) | 17 (26.2) | 12 (30.8) |
| Once/day | 83 (41.5) | 22 (35.5) | 19 (17.8) | 30 (46.2) | 15 (38.5) |
| ≥twice/day | 25 (12.5) | 7 (11.3) | 4 (3.7) | 16 (24.6) | 7 (17.9) |
| Fish consumption,n (%) | |||||
| A few times/month | 123 (62.1) | 31 (50) | 72 (67.3) | 17 (26.2) | 6 (15.4) |
| Once/week | 56 (28.3) | 19 (30.6) | 26 (24.3) | 33 (50.8) | 14 (35.9) |
| Twice/week | 13 (6.6) | 9 (14.5) | 9 (8.4) | 12 (18.5) | 13 (33.3) |
| ≥three times/week | 6 (3) | 3 (4.8) | 0 (0) | 3 (4.6) | 6 (15.4) |
| Pastry consumption,n (%) | |||||
| ≤once/week | 28 (14) | 16 (25.8) | 21 (20.2) | 18 (27.7) | 19 (48.7) |
| A few times/week | 59 (29.5) | 25 (40.3) | 32 (30.8) | 27 (40.9) | 15 (38.5) |
| Nearly every day | 41 (20.5) | 15 (24.2) | 20 (19.2) | 9 (13.8) | 5 (12.8) |
| Everyday | 72 (36) | 6 (9.7) | 31 (29.8) | 11 (16.9) | 0 (0) |
| Score | Czech Republic (n = 174) | Denmark (n = 58) | Greece (n = 70) | Netherlands (n = 57) | Sweden (n = 39) |
|---|---|---|---|---|---|
| Heart SCORE,median (25–75%) | 1 (0–2) | 1 (0–3) | |||
| Heart SCORE ≥ 5%,n (%) | 12 (6.9) | 8 (11.4) | |||
| Heart SCORE ≥ 10%,n (%) | 4 (2.3) | 3 (4.3) | |||
| Svenska Score,median (25–75%) | 0 (0–1) | ||||
| SvenskaScore ≥ 5%,n (%) | 0 (0) | ||||
| Svenska Score ≥ 10%,n (%) | 0 (0) | ||||
| Modified Heartscore BMI score,median (25–75%) | 2 (1–3) | ||||
| Modified Heartscore BMI score ≥ 5%,n(%) | 5 (8.6) | ||||
| PC CMR,median (25–75%) | 22 (13.5–39.5) | ||||
| PC CMR ≥ 23%(men) or PC CMR ≥ 19%(women),n (%) | 21 (36.8) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lionis, C.; Anastasaki, M.; Bertsias, A.; Angelaki, A.; Carlsson, A.C.; Gudjonsdottir, H.; Wändell, P.; Larrabee Sonderlund, A.; Thilsing, T.; Søndergaard, J.; et al. High Variability in Implementation of Selective-Prevention Services for Cardiometabolic Diseases in Five European Primary Care Settings. Int. J. Environ. Res. Public Health 2020, 17, 9080. https://doi.org/10.3390/ijerph17239080
Lionis C, Anastasaki M, Bertsias A, Angelaki A, Carlsson AC, Gudjonsdottir H, Wändell P, Larrabee Sonderlund A, Thilsing T, Søndergaard J, et al. High Variability in Implementation of Selective-Prevention Services for Cardiometabolic Diseases in Five European Primary Care Settings. International Journal of Environmental Research and Public Health. 2020; 17(23):9080. https://doi.org/10.3390/ijerph17239080
Chicago/Turabian StyleLionis, Christos, Marilena Anastasaki, Antonios Bertsias, Agapi Angelaki, Axel C. Carlsson, Hrafnhildur Gudjonsdottir, Per Wändell, Anders Larrabee Sonderlund, Trine Thilsing, Jens Søndergaard, and et al. 2020. "High Variability in Implementation of Selective-Prevention Services for Cardiometabolic Diseases in Five European Primary Care Settings" International Journal of Environmental Research and Public Health 17, no. 23: 9080. https://doi.org/10.3390/ijerph17239080
APA StyleLionis, C., Anastasaki, M., Bertsias, A., Angelaki, A., Carlsson, A. C., Gudjonsdottir, H., Wändell, P., Larrabee Sonderlund, A., Thilsing, T., Søndergaard, J., Seifert, B., Kral, N., De Wit, N. J., Hollander, M., Korevaar, J., & Schellevis, F. (2020). High Variability in Implementation of Selective-Prevention Services for Cardiometabolic Diseases in Five European Primary Care Settings. International Journal of Environmental Research and Public Health, 17(23), 9080. https://doi.org/10.3390/ijerph17239080