Effects of Smoking Cannabis on Visual Function and Driving Performance. A Driving-Simulator Based Study

 , ,
, ,  , and
, and
Abstract
1. Introduction
2. Materials and Methods
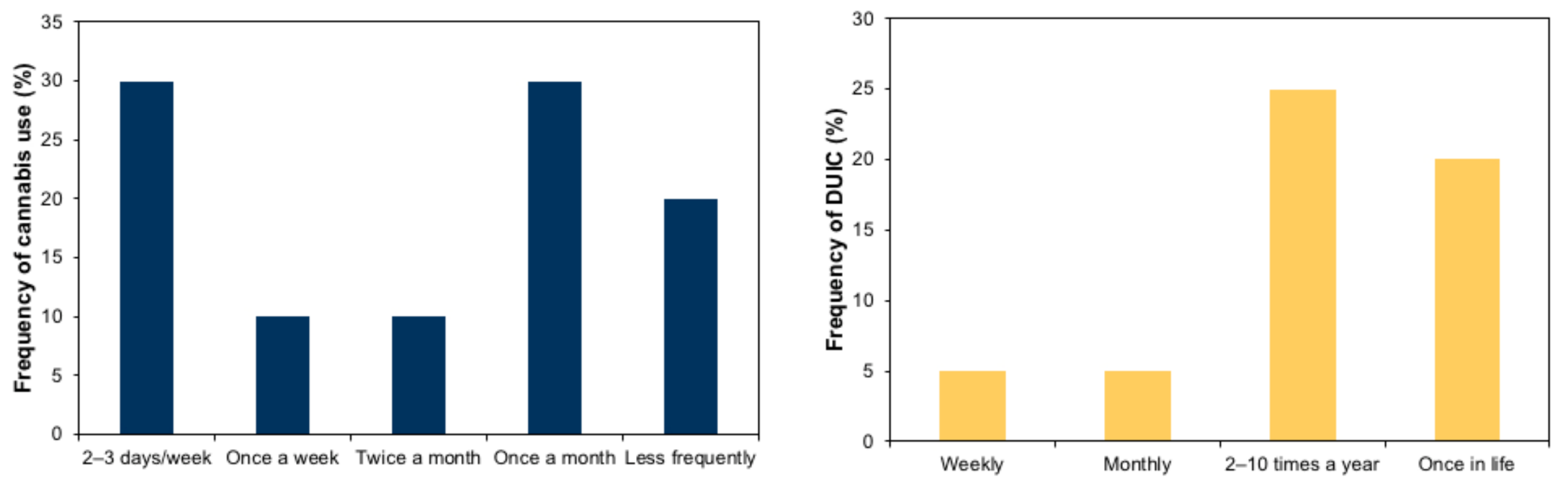
2.1. Participants
2.2. Visual Assessment
2.3. Driving Assessment
2.4. Procedure
2.5. Statistical Analysis
3. Results
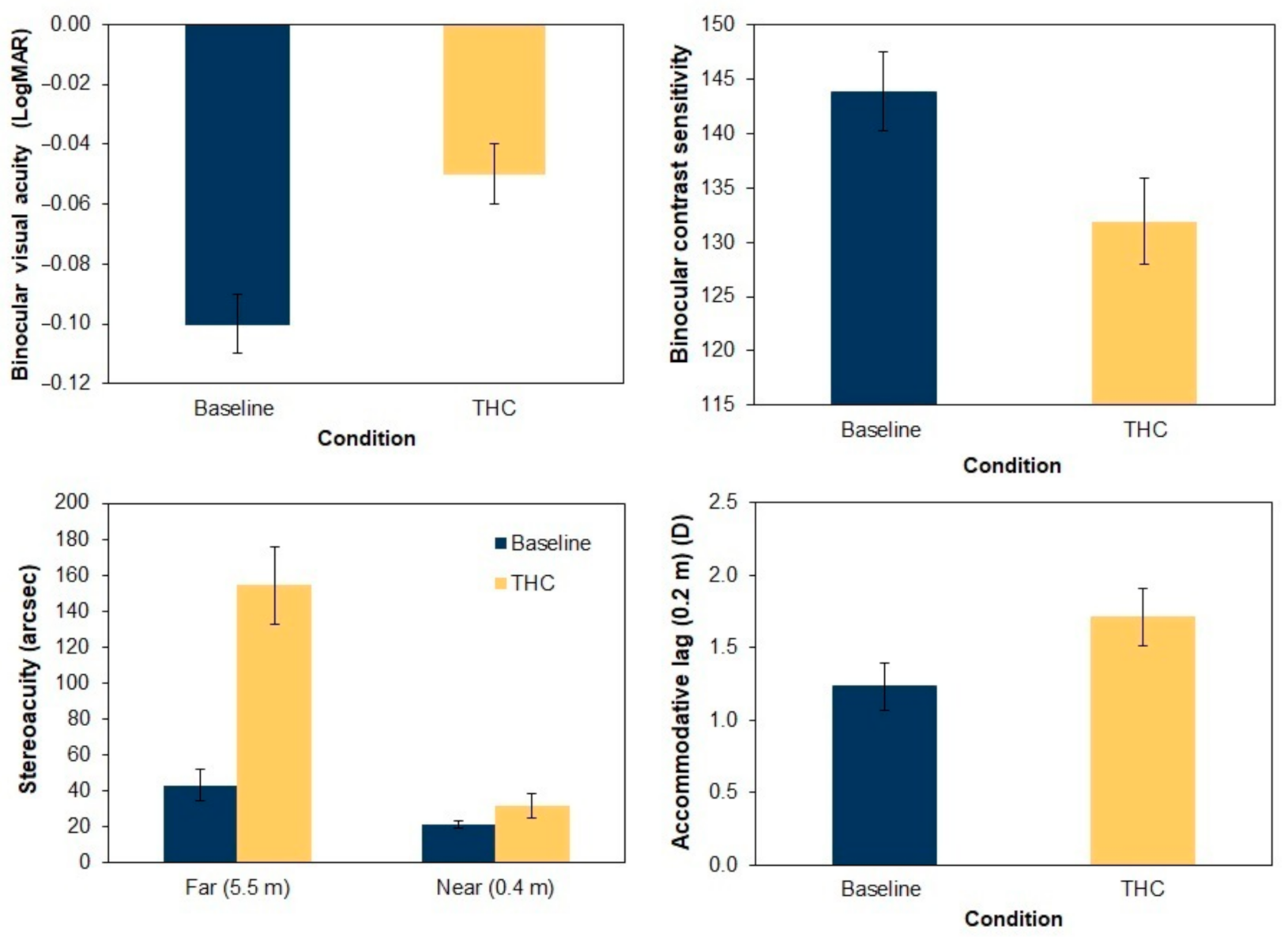
3.1. Visual Assessment
3.2. Driving Assessment
3.3. Relationship between Visual Parameters and Driving Performance
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Kelley-Baker, T.; Berning, A.; Ramirez, A.; Lacey, J.; Carr, K.; Waehrer, G.; Compton, R. 2013–2014 National Roadside Study of Alcohol and Drug Use by Drivers: Drug Results (Report No. DOT HS 812 411); National Highway Traffic Safety Administration, Department of Transportation: Washington, DC, USA, 2017. [Google Scholar]
- Gómez-Talegón, T.; Fierro, I.; González-Luque, J.C.; Colás, M.; López-Rivadulla, M.; Javier Álvarez, F. Prevalence of psychoactive substances, alcohol, illicit drugs, and medicines, in Spanish drivers: A roadside study. Forensic Sci. Int. 2012, 223, 106–113. [Google Scholar] [CrossRef] [PubMed]
- Domingo-Salvany, A.; Herrero, M.J.; Fernandez, B.; Perez, J.; del Real, P.; González-Luque, J.C.; de la Torre, R. Prevalence of psychoactive substances, alcohol and illicit drugs, in Spanish drivers: A roadside study in 2015. Forensic Sci. Int. 2017, 278, 253–259. [Google Scholar] [CrossRef] [PubMed]
- Berning, A.; Compton, R.; Wochinger, K. Results of the 2013–2014 National Roadside Survey of Alcohol and Drug Use by Drivers (Report No. DOT HS 812 118); National Highway Traffic Safety Administration, Department of Transportation: Washington, DC, USA, 2015. [Google Scholar]
- Robertson, R.D.; Mainegra Hing, M.; Pashley, C.R.; Brown, S.W.; Vanlaar, W.G.M. Prevalence and trends of drugged driving in Canada. Accid. Anal. Prev. 2017, 99, 236–241. [Google Scholar] [CrossRef] [PubMed]
- Gjerde, H.; Strand, M.C.; Mørland, J. Driving Under the Influence of Non-Alcohol Drugs--An Update Part I: Epidemiological Studies. Forensic Sci. Rev. 2015, 27, 89–113. [Google Scholar] [PubMed]
- Asbridge, M.; Hayden, J.A.; Cartwright, J.L. Acute cannabis consumption and motor vehicle collision risk: Systematic review of observational studies and meta-analysis. BMJ 2012, 344, e536. [Google Scholar] [CrossRef]
- Micallef, J.; Dupouey, J.; Jouve, E.; Truillet, R.; Lacarelle, B.; Taillard, J.; Daurat, A.; Authié, C.; Blin, O.; Rascol, O.; et al. Cannabis smoking impairs driving performance on the simulator and real driving: A randomized, double-blind, placebo-controlled, crossover trial. Fundam. Clin. Pharmacol. 2018, 32, 558–570. [Google Scholar] [CrossRef]
- Hartman, R.L.; Brown, T.L.; Milavetz, G.; Spurgin, A.; Pierce, R.S.; Gorelick, D.A.; Gaffney, G.; Huestis, M.A. Cannabis Effects on Driving Lateral Control With and Without Alcohol. Drug Alcohol Depend. 2015, 154, 25–37. [Google Scholar] [CrossRef]
- Hartman, R.L.; Brown, T.L.; Milavetz, G.; Spurgin, A.; Pierce, R.S.; Gorelick, D.A.; Gaffney, G.; Huestis, M.A. Cannabis effects on driving longitudinal control with and without alcohol. J. Appl. Toxicol. 2016, 36, 1418–1429. [Google Scholar] [CrossRef]
- Adams, A.J.; Flom, M.C.; Jones, R.T. Evidence for acute effects of alcohol and marijuana on color discrimination. Percept. Psychophys. 1976, 20, 119–124. [Google Scholar] [CrossRef]
- Semple, D.M.; Ramsden, F.; McIntosh, A.M. Reduced binocular depth inversion in regular cannabis users. Farmacol. Biochem. Behav. 2003, 75, 789–793. [Google Scholar] [CrossRef]
- Schwitzer, T.; Schwan, R.; Albuisson, E.; Giersch, A.; Lalanne, L.; Angioi-Duprez, K.; Laprevote, V. Association Between Regular Cannabis Use and Ganglion Cell Dysfunction. JAMA Ophthalmol. 2017, 135, 54. [Google Scholar] [CrossRef] [PubMed]
- Emrich, H.M.; Weber, M.M.; Wendl, A.; Zihl, J.; Von Meyer, L.; Hanisch, W. Reduced binocular depth inversion as an indicator of cannabis-induced censorship impairment. Pharmacol. Biochem. Behav. 1991, 40, 689–690. [Google Scholar] [CrossRef]
- Dawson, W.W.; Jiménez-Antillon, C.F.; Perez, J.M.; Zeskind, J.A. Marijuana and vision-after ten years’ use in Costa Rica. Investig. Ophthalmol. Vis. Sci. 1977, 16, 689–699. [Google Scholar]
- Brown, B.; Adams, A.; Haegerstrom-Portnoy, G.; Jones, R.; Flom, M. Effects of alcohol and marijuana on dynamic visual acuity: I. Threshold measurements. Percept. Psychophys. 1975, 18, 441–446. [Google Scholar] [CrossRef]
- Huestegge, L.; Kunert, H.-J.; Radach, R. Long-term effects of cannabis on eye movement control in reading. Psychopharmacology 2010, 209, 77–84. [Google Scholar] [CrossRef]
- Mikulskaya, E.; Martin, F.H. Contrast sensitivity and motion discrimination in cannabis users. Psychopharmacology 2018, 235, 2459–2469. [Google Scholar] [CrossRef]
- Lalanne, L.; Ferrand-Devouge, E.; Kirchherr, S.; Rauch, L.; Koning, E.; Speeg, C.; Laprevote, V.; Giersch, A. Impaired contrast sensitivity at low spatial frequency in cannabis users with early onset. Eur. Neuropsychopharmacol. 2017, 27, 1289–1297. [Google Scholar] [CrossRef]
- Owsley, C.; Stalvey, B.T.; Wells, J.; Sloane, M.E.; McGwin, G. Visual Risk Factors for Crash Involvement in Older Drivers with Cataract. Arch. Ophthalmol. 2001, 119, 881. [Google Scholar] [CrossRef]
- Adamson, S.J.; Kay-Lambkin, F.J.; Baker, A.L.; Lewin, T.J.; Thornton, L.; Kelly, B.J.; Sellman, J.D. An improved brief measure of cannabis misuse: The Cannabis Use Disorders Identification Test-Revised (CUDIT-R). Drug Alcohol Depend. 2010, 110, 137–143. [Google Scholar] [CrossRef]
- Babor, T.F.; Higgins-Biddle, J.C.; Saunders, J.B.; Monteiro, M.G. The Alcohol Use Disorders Identification Test Guidelines for Use in Primary Care, 2nd ed.; World Health Organization, Department of Mental Health and Substance Dependence: Geneva, Switzerland, 2001; pp. 1–40. [Google Scholar]
- Glasser, A. Accommodation. In Adler’s Physiology of the Eye; Levin, L., Nilsson, S., Ver Hoeve, J., Wu, S., Alm, A., Kaufman, P., Eds.; Saunders: London, UK, 2011; pp. 40–70. [Google Scholar]
- Sheppard, A.L.; Davies, L.N. Clinical evaluation of the Grand Seiko Auto Ref/Keratometer WAM-5500. Ophthalmic Physiol. Opt. 2010, 30, 143–151. [Google Scholar] [CrossRef]
- Poltavski, D.V.; Biberdorf, D.; Petros, T.V. Accommodative response and cortical activity during sustained attention. Vis. Res. 2012, 63, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Ortiz, C.; Ortiz-Peregrina, S.; Castro, J.J.; Casares-López, M.; Salas, C. Driver distraction by smartphone use (WhatsApp) in different age groups. Accid. Anal. Prev. 2018, 117, 239–249. [Google Scholar] [CrossRef] [PubMed]
- Casares-López, M.; Castro-Torres, J.J.; Martino, F.; Ortiz-Peregrina, S.; Ortiz, C.; Anera, R.G. Contrast sensitivity and retinal straylight after alcohol consumption: Effects on driving performance. Sci. Rep. 2020, 10, 13599. [Google Scholar] [CrossRef] [PubMed]
- Ortiz-Peregrina, S.; Ortiz, C.; Salas, C.; Casares-López, M.; Soler, M.; Anera, R.G. Intraocular scattering as a predictor of driving performance in older adults with cataracts. PLoS ONE 2020, 15, e0227892. [Google Scholar] [CrossRef]
- Ortiz-Peregrina, S.; Oviedo-Trespalacios, O.; Ortiz, C.; Casares-López, M.; Salas, C.; Anera, R.G. Factors determining speed management during distracted driving (WhatsApp messaging). Sci. Rep. 2020, 10, 13263. [Google Scholar] [CrossRef]
- Ortiz-Peregrina, S.; Ortiz, C.; Casares-López, M.; Castro-Torres, J.J.; Jiménez Del Barco, L.; Anera, R.G. Impact of Age-Related Vision Changes on Driving. Int. J. Environ. Res. Public Health. 2020, 17, 7416. [Google Scholar] [CrossRef]
- Wood, J.M. Age and visual impairment decrease driving performance as measured on a closed-road circuit. Hum. Factors 2002, 44, 482–494. [Google Scholar] [CrossRef]
- Grotenhermen, F. Pharmacokinetics and Pharmacodynamics of Cannabinoids. Clin. Pharmacokinet. 2003, 42, 327–360. [Google Scholar] [CrossRef]
- Desrosiers, N.A.; Milman, G.; Mendu, D.R.; Lee, D.; Barnes, A.J.; Gorelick, D.A.; Huestis, M.A. Cannabinoids in Oral Fluid by on-site immunoassay and by GC- MS using two different oral fluid collection devices. Anal. Bioanal. Chem. 2014, 406, 4117–4128. [Google Scholar] [CrossRef]
- Ramaekers, J.G.; Robbe, H.W.J.; O’Hanlon, J.F. Marijuana, alcohol and actual driving performance. Hum. Psychopharmacol. 2000, 15, 551–558. [Google Scholar] [CrossRef]
- Downey, L.A.; King, R.; Papafotiou, K.; Swann, P.; Ogden, E.; Boorman, M.; Stough, C. The effects of cannabis and alcohol on simulated driving: Influences of dose and experience. Accid. Anal. Prev. 2013, 50, 879–886. [Google Scholar] [CrossRef] [PubMed]
- Li, M.-C.; Brady, J.E.; DiMaggio, C.J.; Lusardi, A.R.; Tzong, K.Y.; Li, G. Marijuana use and motor vehicle crashes. Epidemiol. Rev. 2012, 34, 65–72. [Google Scholar] [CrossRef] [PubMed]
- Hostiuc, S.; Moldoveanu, A.; Negoi, I.; Drima, E. The Association of Unfavorable Traffic Events and Cannabis Usage: A Meta-Analysis. Front. Pharmacol. 2018, 9, 99. [Google Scholar] [CrossRef] [PubMed]
- Adams, A.; Brown, B.; Flom, M.; Jones, R.; Jampolsky, A. Alcohol and marijuana effects on static visual acuity. Am. J. Optom. Physiol. Opt. 1975, 52, 729–735. [Google Scholar] [CrossRef]
- Noyes, R.; Brunk, S.F.; Avery, D.H.; Canter, A. The analgesic properties of delta-9-tetrahydrocannabinol and codeine. Clin. Pharmacol. Ther. 1975, 18, 84–89. [Google Scholar] [CrossRef]
- Owsley, C.; McGwin, G. Vision and driving. Vision Res. 2010, 50, 2348–2361. [Google Scholar] [CrossRef]
- Szlyk, J.P.; Pizzimenti, C.E.; Fishman, G.A.; Kelsch, R.; Wetzel, L.C.; Kagan, S.; Ho, K. A Comparison of Driving in Older Subjects with and Without Age-Related Macular Degeneration. Arch. Ophthalmol. 1995, 113, 1033–1040. [Google Scholar] [CrossRef]
- Yellott, J.I. Binocular depth inversion. Sci. Am. 1981, 245, 148–159. [Google Scholar] [CrossRef][Green Version]
- Schwitzer, T.; Schwan, R.; Angioi-Duprez, K.; Ingster-Moati, I.; Lalanne, L.; Giersch, A.; Laprevote, V. The cannabinoid system and visual processing: A review on experimental findings and clinical presumptions. Eur. Neuropsychopharmacol. 2015, 25, 100–112. [Google Scholar] [CrossRef]
- Brown, B.; Adams, A.J.; Haegerstrom-Portnoy, G.; Jones, R.T.; Flom, M.C. Pupil Size After Use of Marijuana and Alcohol. Am. J. Ophthalmol. 1977, 83, 350–354. [Google Scholar] [CrossRef]
- Korczyn, A.D. The ocular effects of cannabinoids. Gen. Pharmacol. Vasc. Syst. 1980, 11, 419–423. [Google Scholar] [CrossRef]
- Bédard, M.; Parkkari, M.; Weaver, B.; Riendeau, J.; Dahlquist, M. Assessment of driving performance using a simulator protocol: Validity and reproducibility. Am. J. Occup. Ther. 2010, 64, 336–340. [Google Scholar] [CrossRef] [PubMed]
- Bondallaz, P.; Favrat, B.; Chtioui, H.; Fornari, E.; Maeder, P.; Giroud, C. Cannabis and its effects on driving skills. Forensic Sci. Int. 2016, 268, 92–102. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Section of the Route | Driving Performance Variables |
|---|---|
| Dual carriageway | Mean speed (kph) Distance travelled onto the shoulder (m) 1 |
| Mountain road | Mean speed (kph) Distance driven invading the opposite lane (m) Distance driven onto the shoulder (m) Total distance driven outside the lane (i.e., the distance travelled onto the shoulder plus the distance travelled invading the opposite lane) (m) 1 Standard deviation of the lateral position (SDLP) (m) 1 Reaction time (s) 1 |
| City | Mean speed (kph) |
| Total circuit | Total time (s) Collisions Overall Driving Performance Score (OPDS) |
| Visual Parameter | Baseline Condition | THC Condition | t/Z | p Value |
|---|---|---|---|---|
| Binocular VA (logMAR) | −0.10 (0.01) | −0.05 (0.01) | −4.516 | <0.001 |
| Binocular CS | 143.85 (3.64) | 131.93 (4.01) | 3.223 | 0.004 |
| Stereoacuity- far (5.5 m) (arcsec) 1 | 43.16 (8.89) | 154.21 (21.73) | −3.623 | <0.001 |
| Stereoacuity-near (0.4 m) (arcsec) 1 | 21.18 (2.11) | 31.68 (6.99) | −2.496 | 0.01 |
| Pupil size (scotopic) (mm) | 6.65 (0.18) | 6.33 (0.15) | 2.94 | 0.008 |
| Pupil size (low mesopic) (mm) | 5.91 (0.19) | 5.93 (0.16) | −0.156 | 0.87 |
| Pupil size (high mesopic) (mm) | 5.39 (0.18) | 5.43 (0.20) | −0.271 | 0.79 |
| Accommodative lag (0.4 m) (D) | 1.07 (0.17) | 1.38 (0.13) | 1.949 | 0.07 |
| Accommodative lag (0.2 m) (D) | 1.23 (0.16) | 1.71 (0.20) | 2.892 | 0.01 |
| Driving Parameter | Baseline Condition | THC Condition | t/Z | p Value |
|---|---|---|---|---|
| Dual Carriageway | ||||
| Mean speed (km/h) | 115.54 (1.59) | 118.47 (2.44) | −1.515 | 0.15 |
| Distance driven onto the shoulder (m) 1 | 71.44 (18.89) | 122.83 (23.54) | −1.61 | 0.11 |
| Mountain Road | ||||
| Mean speed (km/h) | 55.08 (0.35) | 55.86 (0.39) | −1.77 | 0.09 |
| Distance driven invading the opposite lane (m) 1 | 322.09 (49.62) | 458.87 (115.12) | −1.493 | 0.14 |
| Distance driven onto the shoulder (m) 1 | 16.96 (3.56) | 52.14 (15.44) | −3.219 | 0.001 |
| Total distance driven outside the lane (m) 1 | 339.04 (49.86) | 511.01 (112.27) | −1.979 | 0.048 |
| SDLP (m) | 0.52 (0.02) | 0.57 (0.02) | −3.10 | 0.006 |
| Reaction time (s) 1 | 0.84 (0.03) | 0.92 (0.04) | −0.312 | 0.76 |
| City | ||||
| Mean speed (km/h) | 29.34 (1.05) | 29.94 (1.03) | −0.66 | 0.52 |
| Total circuit | ||||
| Total time (s) | 794.38 (12.12) | 784.61 (10.84) | 0.906 | 0.38 |
| Collisions 1 | 0.50 (0.14) | 0.70 (0.26) | −1.068 | 0.29 |
| Overall Driving Performance Score 1 | 0.21 (0.13) | −0.29 (0.12) | −3.114 | 0.002 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ortiz-Peregrina, S.; Ortiz, C.; Castro-Torres, J.J.; Jiménez, J.R.; Anera, R.G. Effects of Smoking Cannabis on Visual Function and Driving Performance. A Driving-Simulator Based Study. Int. J. Environ. Res. Public Health 2020, 17, 9033. https://doi.org/10.3390/ijerph17239033
Ortiz-Peregrina S, Ortiz C, Castro-Torres JJ, Jiménez JR, Anera RG. Effects of Smoking Cannabis on Visual Function and Driving Performance. A Driving-Simulator Based Study. International Journal of Environmental Research and Public Health. 2020; 17(23):9033. https://doi.org/10.3390/ijerph17239033
Chicago/Turabian StyleOrtiz-Peregrina, Sonia, Carolina Ortiz, José J. Castro-Torres, José R. Jiménez, and Rosario G. Anera. 2020. "Effects of Smoking Cannabis on Visual Function and Driving Performance. A Driving-Simulator Based Study" International Journal of Environmental Research and Public Health 17, no. 23: 9033. https://doi.org/10.3390/ijerph17239033
APA StyleOrtiz-Peregrina, S., Ortiz, C., Castro-Torres, J. J., Jiménez, J. R., & Anera, R. G. (2020). Effects of Smoking Cannabis on Visual Function and Driving Performance. A Driving-Simulator Based Study. International Journal of Environmental Research and Public Health, 17(23), 9033. https://doi.org/10.3390/ijerph17239033