A Scoping Review of the Risk Factors Associated with Anaemia among Children Under Five Years in Sub-Saharan African Countries


Abstract
1. Introduction
The Aim of the Scoping Review
2. Materials and Methods
2.1. Protocol and Registration Declaration
2.2. Eligibility Criteria
2.2.1. Population
2.2.2. Interventions
2.2.3. Comparators
2.2.4. Outcomes
2.2.5. Timing or Time Frames
2.2.6. Study Designs
2.3. Information Sources
2.4. Search Strategy
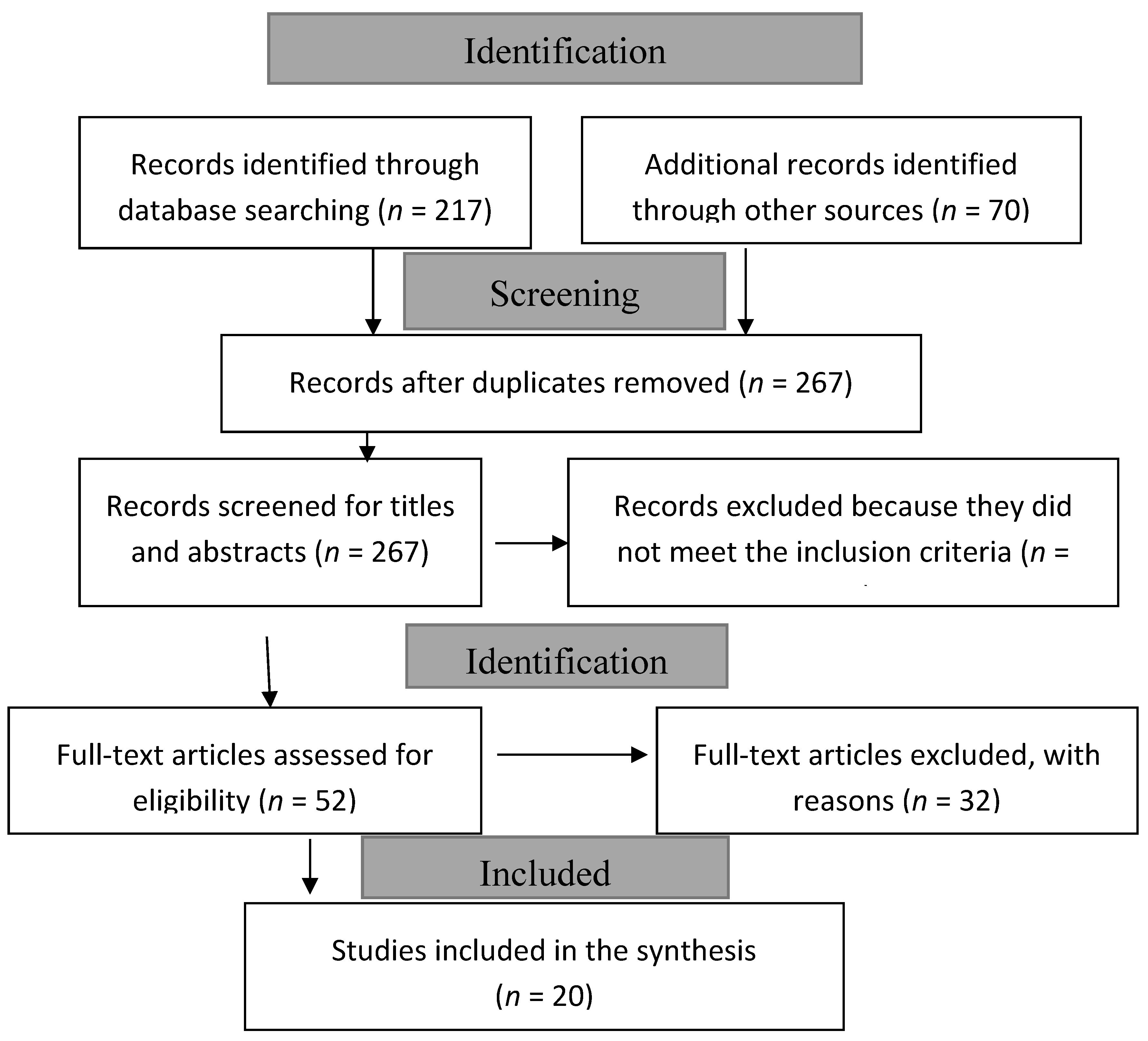
2.5. Selection Process
2.6. Data Charting Management
3. Results
3.1. The Study Profile Counts
- (i)
- Using other analytical methods rather than classical regression analysis.
- (ii)
- Studies did not report separate results for children 0–59 months.
- (iii)
- Studies that considered anaemia outcomes based on the maternal or child’s specifics.
- (iv)
- Studies not from SSA countries.
- (v)
- Papers without the full text available.
3.2. Characteristics of the Included Studies
3.3. The Study Profiles by Countries
3.4. Classification by Survey Types
3.5. Classification by Analytical Methods
3.6. Classification of the Risk Factors
3.6.1. Child-Related Variables
3.6.2. Distributions of Parental/Caregivers-Related Variables
3.6.3. Distributions of Household-Related Variables
- (i)
- Household size, in four (17%) studies.
- (ii)
- The number of children that were under-five years living in the same household (17%).
- (iii)
- Having an improved source of drinking water, reported in eight (33%) studies.
- (iv)
- The child slept under a mosquito net the previous night before the survey (17%).
3.6.4. Distribution of Study Characteristics by Community-Related Variables
4. Discussion
5. Strengths and Limitations
6. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Global Anaemia Prevalence and Number of Individuals Affected. Available online: https://www.who.int/vmnis/anaemia/prevalence/summary/anaemia_data_status_t2/en/ (accessed on 25 November 2020).
- Kawo, K.N.; Asfaw, Z.G.; Yohannes, N. Multilevel Analysis of Determinants of Anemia Prevalence among Children Aged 6–59 Months in Ethiopia: Classical and Bayesian Approaches. Anemia 2018, 2018, 3087354. [Google Scholar] [CrossRef] [PubMed]
- Osungbade, K.O.; Oladunjoye, A.O. Anaemia in Developing Countries: Burden and Prospects of Prevention and Control. In Anaemia; IntechOpen: London, UK, 2012. [Google Scholar]
- Prevalence of Anaemia in Children under 5 Years. Available online: https://www.who.int/data/gho/data/indicators/indicator-details/GHO/prevalence-of-anaemia-in-children-under-5-years-(-) (accessed on 25 November 2020).
- Nigeria Demographic and Health Survey 2018. Available online: https://www.dhsprogram.com/pubs/pdf/FR359/FR359.pdf (accessed on 25 November 2020).
- Tradingeconomics Nigeria—Prevalence of Anemia Among Children (% Of Children Under 5). Available online: https://tradingeconomics.com/nigeria/prevalence-of-anemia-among-children-percent-of-children-under-5-wb-data.html (accessed on 25 November 2020).
- Belachew, A.; Tewabe, T. Under-five anemia and its associated factors with dietary diversity, food security, stunted, and deworming in Ethiopia: Systematic review and meta-analysis. Syst. Rev. 2020, 9, 31. [Google Scholar] [CrossRef] [PubMed]
- De Benoist, B.; Cogswell, M.; Egli, I.; McLean, E. Worldwide Prevalence of Anaemia 1993–2005 of: WHO Global Database of Anaemia; World Health Organization: Geneva, Switzerland, 2008; ISBN 978-92-4-159665-7. [Google Scholar]
- Austin, A.M.; Fawzi, W.; Hill, A.G. Anaemia among Egyptian Children between 2000 and 2005: Trends and predictors. Matern. Child Nutr. 2012, 8, 522–532. [Google Scholar] [CrossRef] [PubMed]
- Kikafunda, J.K.; Lukwago, F.B.; Turyashemererwa, F.; Kikafunda, J.K.; Lukwago, F.B.; Turyashemererwa, F. Anaemia and associated factors among under-fives and their mothers in Bushenyi district, Western Uganda. Public Health Nutr. 2009, 12, 2302–2308. [Google Scholar] [CrossRef]
- Mitchinson, C.; Strobel, N.; McAullay, D.; McAuley, K.; Bailie, R.; Edmond, K.M. Anemia in disadvantaged children aged under five years; quality of care in primary practice. BMC Pediatrics 2019, 19, 178. [Google Scholar] [CrossRef]
- Bamidele, J.O.; Abodunrin, O.L.; Olajide, F.O.; Oke, Y.F. Prevalence and determinants of anemia among primary school pupils of a peri-urban community in Osun State, Nigeria. Int. J. Adolesc. Med. Health 2010, 22, 461–468. [Google Scholar] [CrossRef]
- Demirchyan, A.; Petrosyan, V.; Sargsyan, V.; Hekimian, K. Prevalence and determinants of anaemia among children aged 0–59 months in a rural region of Armenia: A case-control study. Public Health Nutr. 2016, 19, 1260–1269. [Google Scholar] [CrossRef]
- Manda, S.; Haushona, N.; Bergquist, R. A Scoping Review of Spatial Analysis Approaches Using Health Survey Data in Sub-Saharan Africa. Int. J. Environ. Res. Public Health 2020, 17, 70. [Google Scholar] [CrossRef]
- Larissa Shamseer, D.M. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015: Elaboration and explanation. BMJ 2015, 349, g7647. [Google Scholar] [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef]
- Creating a PRISMA Flow Diagram. Available online: https://guides.lib.unc.edu/prisma (accessed on 16 August 2020).
- Dwumoh, D.; Essuman, E.E.; Afagbedzi, S.K. Determinant of factors associated with child health outcomes and service utilization in Ghana: Multiple indicator cluster survey conducted in 2011. Arch. Public Health 2014, 72, 42. [Google Scholar] [CrossRef] [PubMed]
- Hershey, C.L.; Florey, L.S.; Ali, D.; Bennett, A.; Luhanga, M.; Mathanga, D.P.; Salgado, S.R.; Nielsen, C.F.; Troell, P.; Jenda, G.; et al. Malaria Control Interventions Contributed to Declines in Malaria Parasitemia, Severe Anemia, and All-Cause Mortality in Children Less Than 5 Years of Age in Malawi, 2000–2010. Am. J. Trop. Med. Hyg. 2017, 97, 76–88. [Google Scholar] [CrossRef] [PubMed]
- Jones, A.D.; Colecraft, E.K.; Awuah, R.B.; Boatemaa, S.; Lambrecht, N.J.; Adjorlolo, L.K.; Wilson, M.L. Livestock ownership is associated with higher odds of anaemia among preschool-aged children, but not women of reproductive age in Ghana. Matern. Child Nutr. 2018, 14, e12604. [Google Scholar] [CrossRef] [PubMed]
- Machisa, M.; Wichmann, J.; Nyasulu, P.S. Biomass fuel use for household cooking in Swaziland: Is there an association with anaemia and stunting in children aged 6–36 months? Trans. R. Soc. Trop. Med. Hyg. 2013, 107, 535–544. [Google Scholar] [CrossRef] [PubMed]
- Mohammed, S.H.; Habtewold, T.D.; Esmaillzadeh, A. Household, maternal, and child related determinants of hemoglobin levels of Ethiopian children: Hierarchical regression analysis. BMC Pediatrics 2019, 19, 113. [Google Scholar] [CrossRef]
- Moschovis, P.P.; Wiens, M.O.; Arlington, L.; Antsygina, O.; Hayden, D.; Dzik, W.; Kiwanuka, J.P.; Christiani, D.C.; Hibberd, P.L. Individual, maternal and household risk factors for anaemia among young children in sub-Saharan Africa: A cross-sectional study. BMJ Open 2018, 8, e019654. [Google Scholar] [CrossRef]
- Nambiema, A.; Robert, A.; Yaya, I. Prevalence and risk factors of anemia in children aged from 6 to 59 months in Togo: Analysis from Togo demographic and health survey data, 2013–2014. BMC Public Health 2019, 19, 215. [Google Scholar] [CrossRef]
- Ntenda, P.A.M.; Chilumpha, S.; Mwenyenkulu, E.T.; Kazambwe, J.F.; El-Meidany, W. Clinical malaria and the potential risk of anaemia among preschool-aged children: A population-based study of the 2015-2016 Malawi micronutrient survey. Infect. Dis. Poverty 2019, 8, 95. [Google Scholar] [CrossRef]
- Ntenda, P.A.M.; Chuang, K.Y.; Tiruneh, F.N.; Chuang, Y.C. Multilevel Analysis of the Effects of Individual- and Community-Level Factors on Childhood Anemia, Severe Anemia, and Hemoglobin Concentration in Malawi. J. Trop. Pediatr. 2018, 64, 267–278. [Google Scholar] [CrossRef]
- Immurana, M.; Urmi, A. Socio-economic factors and child health status in Ghana. Int. J. Health 2017, 5. [Google Scholar] [CrossRef]
- Candia, D.A. Douglas Andabati Candia Influence of malaria on anemia levels among children less than 60 months of age. Int. J. Adv. Res. Dev. 2017, 2, 5. [Google Scholar]
- Menon, M.P.; Yoon, S.S.; Uganda Malaria Indicator Survey Technical Working, G. Prevalence and Factors Associated with Anemia among Children under 5 Years of Age—Uganda, 2009. Am. J. Trop. Med. Hyg. 2015, 93, 521–526. [Google Scholar] [CrossRef] [PubMed]
- Nikoi, E.; Anthamatten, P. Childhood anaemia in Ghana: An examination of associated socioeconomic and health factors. Afr. Geogr. Rev. 2013, 33, 19–35. [Google Scholar] [CrossRef]
- Ojoniyi, O.O.; Odimegwu, C.O.; Olamijuwon, E.O.; Akinyemi, J.O. Does education offset the effect of maternal disadvantage on childhood anaemia in Tanzania? Evidence from a nationally representative cross-sectional study. BMC Pediatrics 2019, 19, 89. [Google Scholar] [CrossRef] [PubMed]
- Muchie, K.F. Determinants of severity levels of anemia among children aged 6–59 months in Ethiopia: Further analysis of the 2011 Ethiopian demographic and health survey. BMC Nutr. 2016, 2, 51. [Google Scholar] [CrossRef]
- Asresie, M.B.; Fekadu, G.A.; Dagnew, G.W. Determinants of Anemia among Children Aged 6–59 Months in Ethiopia: Further Analysis of the 2016 Ethiopian Demographic Health Survey. Adv. Public Health 2020, 2020, 3634591. [Google Scholar] [CrossRef]
- Semedo, R.M.; Santos, M.M.; Baião, M.R.; Luiz, R.R.; da Veiga, G.V. Prevalence of anaemia and associated factors among children below five years of age in Cape Verde, West Africa. J. Health Popul. Nutr. 2014, 32, 646–657. [Google Scholar]
- Ntenda, P.A.M.; Nkoka, O.; Bass, P.; Senghore, T. Maternal anemia is a potential risk factor for anemia in children aged 6–59 months in Southern Africa: A multilevel analysis. BMC Public Health 2018, 18, 650. [Google Scholar] [CrossRef]
- Ngnie-Teta, I.; Receveur, O.; Kuate-Defo, B. Risk factors for moderate to severe anemia among children in Benin and Mali: Insights from a multilevel analysis. Food Nutr. Bull. 2007, 28, 76–89. [Google Scholar] [CrossRef]
- Mishra, V.; Retherford, R.D. Does biofuel smoke contribute to anaemia and stunting in early childhood? Int. J. Epidemiol. 2007, 36, 117–129. [Google Scholar] [CrossRef]
- Page, C.M.; Patel, A.; Hibberd, P.L. Does smoke from biomass fuel contribute to anemia in pregnant women in Nagpur, India? A cross-sectional study. PLoS ONE 2015, 10, e0127890. [Google Scholar] [CrossRef] [PubMed]
- Sub-Saharan Africa. Available online: https://en.wikipedia.org/wiki/Sub-Saharan_Africa (accessed on 25 November 2020).
- Nguyen, P.H.; Scott, S.; Avula, R.; Tran, L.M.; Menon, P. Trends and drivers of change in the prevalence of anaemia among 1 million women and children in India, 2006 to 2016. BMJ Glob. Health 2018, 3, e001010. [Google Scholar] [CrossRef] [PubMed]
- Harding, K.L.; Aguayo, V.M.; Namirembe, G.; Webb, P. Determinants of anemia among women and children in Nepal and Pakistan: An analysis of recent national survey data. Matern. Child Nutr. 2018, 14, e12478. [Google Scholar] [CrossRef] [PubMed]
- Jackson, R.T.; Hamad, N.A.; AL-Somaie, M.; Guoad, N.A.; Prakash, P. Gender and Age Differences in Anemia Prevalence during the Lifecycle in Kuwait. Ecol. Food Nutr. 2004, 43, 61–75. [Google Scholar] [CrossRef]
- National Malaria Elimination Program (NMEP); National Population Commission (NPopC); National Bureau. ICF International Nigeria Malaria Indicator Survey [MIS8] 2015; NMEP, NPopC, and ICF International: Abuja, Nigeria; Rockville, ML, USA, 2016; p. 190. [Google Scholar]
- National Population Commission (NPC); National Malaria Control Program (NMCP). ICF Macro Nigeria Malaria Indicator Survey [MIS8] 2010. NPC, NMCP, ICF International: Abuja, Nigeria; Rockville, ML, USA, 2012; p. 137. [Google Scholar]
- Navickas, R.; Petric, V.K.; Feigl, A.B.; Seychell, M. Multimorbidity: What do we know? What should we do? J. Comorb. 2016, 6, 4–11. [Google Scholar] [CrossRef]
- Ferro, M.A.; Lipman, E.L.; Van Lieshout, R.J.; Gorter, J.W.; Shanahan, L.; Boyle, M.; Georgiades, K.; Timmons, B. Multimorbidity in Children and Youth Across the Life-course (MY LIFE): Protocol of a Canadian prospective study. BMJ Open 2019, 9, e034544. [Google Scholar] [CrossRef]
- Russell, J.; Grant, C.C.; Morton, S.M.B. Multimorbidity in Early Childhood and Socioeconomic Disadvantage: Findings from a Large New Zealand Child Cohort. Acad. Pediatr. 2020, 20, 619–627. [Google Scholar] [CrossRef]
- Green, B.N.; Johnson, C.D.; Haldeman, S.; Griffith, E.; Clay, M.B.; Kane, E.J.; Castellote, J.M.; Rajasekaran, S.; Smuck, M.; Hurwitz, E.L.; et al. A scoping review of biopsychosocial risk factors and co-morbidities for common spinal disorders. PLoS ONE 2018, 13, e0197987. [Google Scholar] [CrossRef]


{kind=link}
| Author(s) (Year) | Country | Title of Study | Survey Type | Prevalence of Anaemia | Participation | Methods |
|---|---|---|---|---|---|---|
| Dwumoh et al. (2014) [18] | Ghana | Determinant of factors associated with child health outcomes and service utilization in Ghana: Multiple indicator cluster survey conducted in 2011 | MICS | There was no % prevalence reported | 7550 | Binary logistic regression models and multiple linear regression |
| Hershey et al. (2017) [19] | Malawi | Malaria Control Interventions Contributed to Declines in Malaria Parasitaemia, Severe Anaemia, and All-Cause Mortality in Children Less Than 5 Years of Age in Malawi, 2000–2010 | DHS, MICS and MIS | Prevalence of severe anaemia in 2010 was 8.7% | Proportion | Multivariable, random effects logistic regression models |
| Jones et al. (2018) [20] | Ghana | Livestock ownership is associated with higher odds of anaemia among preschool-aged children, but not women of reproductive age in Ghana | DHS | Moderate anaemia was 56.4%, mild anaemia was 40.2% | 2735 | Multiple binary logistic regression models |
| Machisa et al. (2013) [21] | Swaziland | Biomass fuel use for household cooking in Swaziland: is there an association with anaemia and stunting in children aged 6–36 months? | DHS | 51.8% in children 6–36 months | 1150 | Multinomial logistic regression analyses |
| Mohammed et al. (2019) [22] | Ethiopia | Household, maternal, and child-related determinants of haemoglobin levels of Ethiopian children: hierarchical regression analysis | DHS 2016 | 71.92% in the study population (6–23 months) | 2902 | Hierarchical linear regression analysis |
| Moschovis et al. (2018) [23] | 27 SSA countries | Individual, maternal and household risk factors for anaemia among young children in sub-Saharan Africa: a cross-sectional study | DHS 2008–2014 | 59.9% among children 6–59 months | 96,804 | Multiple linear regression or multiple binary logistic regression |
| Nambiema et al. (2019) [24] | Togo | Prevalence and risk factors of anaemia in children aged from 6 to 59 months in Togo: analysis from Togo demographic and health survey data | DHS 2013–2014 | 70.9% among children 6–59 months | 2890 | Logistic regression models |
| Ngnie-Teta et al. (2007)[25] | Benin | Risk factors for moderate to severe anaemia among children in Benin and Mali: insights from a multilevel analysis | DHS 2001 | 82% | 2284 | Multilevel binary logistic model |
| Mali | Risk factors for moderate to severe anaemia among children in Benin and Mali: insights from a multilevel analysis | DHS 2001 | 83% | 2826 | Multilevel binary logistic model | |
| Ntenda et al. (2019) [26] | Malawi | Clinical malaria and the potential risk of anaemia among preschool-aged children: a population-based study of the 2015–2016 Malawi micronutrient survey | 2015–2016 MNS | 29% | 1051 | Multivariate binary logistic regression models |
| Ntenda et al. (2018) [27] | Malawi | Multilevel Analysis of the Effects of Individual- and Community-Level Factors on Childhood Anaemia, Severe Anaemia, and Haemoglobin Concentration in Malawi | 2010 DHS | 63% | 2597 | Multilevel linear regression models |
| Kawo et al. (2018) [2] | Ethiopia | Multilevel Analysis of Determinants of Anaemia Prevalence among Children Aged 6–59 Months in Ethiopia: Classical and Bayesian Approaches | 2010 DHS | 42.8% | 5507 | Multilevel binary logistic regression analysis |
| Immurana and Arabi (2017) [28] | Ghana | Socioeconomic factors and child health status in Ghana | 2014 DHS | 71.11% male and 67.95% female children | 2220 | Binary probit model |
| Candia (2017) [29] | Uganda | Influence of malaria on anaemia levels among children less than 60 months of age | MIS | 53.22% | 4940 | Ordered logistic regression model |
| Menon and Yoon (2015) [30] | Uganda | Prevalence and Factors Associated with Anaemia among Children Under 5 Years of Age—Uganda, 2009 | 2009 MIS | 60% of children under five years | 4065 | Multivariate binary logistic regression model |
| Nikol and Anthamatten (2013) [31] | Ghana | Childhood anaemia in Ghana: an examination of associated socioeconomic and health factors | 2008 DHS | 79.8% | 2055 | Generalized linear mixed regression model |
| Ojoniyi et al. (2019) [32] | Tanzania | Does education offset the effect of maternal disadvantage on childhood anaemia in Tanzania? Evidence from a nationally representative cross-sectional study | 2015–2016 DHS/MIS | 58.6% | 7916 | Proportional odds model |
| Muchie (2016) [33] | Ethiopia | Determinants of severity levels of anaemia among children aged 6–59 months in Ethiopia: further analysis of the 2011 Ethiopian demographic and health survey | 2011 DHS | 28.6% were severely/moderately anaemic and 21.7% were mildly anaemic | 7636 | Proportional odds model of ordinal logistic regression |
| Asresie et al. (2020) [34] | Ethiopia | Determinants of Anaemia among Children Aged 6–59 Months in Ethiopia: Further Analysis of the 2016 Ethiopian Demographic Health Survey | 2016 DHS | 58% of children 6–59 months | 8462 | Binary Logistic regression analyses |
| Semedo et al. (2014) [35] | Cape Verde | Prevalence of anaemia and associated factors among children below five years of age in Cape Verde, West Africa | NHS | 51.8% | 933 | Hierarchical model for multiple analysis |
| Ntenda et al. (2018) [36] | Malawi | Maternal anaemia is a potential risk factor for anaemia in children aged 6–59 months in Southern Africa: a multilevel analysis | 2010 DHS | 63.8% | 2507 | Generalized linear mixed models (GLMMs) |
| Mozambique | Maternal anaemia is a potential risk factor for anaemia in children aged 6–59 months in Southern Africa: a multilevel analysis | 2013 DHS | 70% | 1933 | Generalized linear mixed models (GLMMs) | |
| Namibia | Maternal anaemia is a potential risk factor for anaemia in children aged 6–59 months in Southern Africa: a multilevel analysis | 2013 DHS | 49% | 1116 | Generalized linear mixed models (GLMMs) | |
| Zimbabwe | Maternal anaemia is a potential risk factor for anaemia in children aged 6–59 months in Southern Africa: a multilevel analysis | 2010–2011 DHS | 58.6% | 2578 | Generalized linear mixed models (GLMMs) |
| Country Specific Articles | Number | % | References |
|---|---|---|---|
| Ghana | 4 | 16.8 | [18,20,28,31] |
| Ethiopia | 4 | 16.8 | [2,22,33,34] |
| Mali | 1 | 4.2 | [25] |
| Benin | 1 | 4.2 | [25] |
| Uganda | 2 | 8.4 | [29,30] |
| Tanzania | 1 | 4.2 | [32] |
| Malawi | 4 | 16.8 | [19,26,27,36] |
| Swaziland | 1 | 4.2 | [21] |
| Multi-country | 1 | 4.2 | [23] |
| Togo | 1 | 4.2 | [24] |
| Cape Verde | 1 | 4.2 | [35] |
| Mozambique | 1 | 4.2 | [36] |
| Namibia | 1 | 4.2 | [36] |
| Zimbabwe | 1 | 4.2 | [36] |
| 24 * | 100 |
| Survey Type Specific | N | % |
|---|---|---|
| Demographic and Health Survey (DHS) | 19 | 70 |
| Multiple Indicator Survey (MIS) | 4 | 15 |
| Micronutrient Survey (MNS) | 1 | 4 |
| Multiple Indicator Cluster Survey (MICS) | 2 | 7 |
| National Health Survey (NHS) | 1 | 4 |
| Total | 27 * | 100 |
| Analytical Methods | N | % | References |
|---|---|---|---|
| Multivariate Linear Regression | 2 | 8 | [18,23] |
| Multivariate Logistic Regression | 9 | 36 | [18,19,20,23,24,26,28,30,34] |
| Proportional Ordinal Logistic Regression | 3 | 12 | [29,32,33] |
| Multilevel Regression | 5 | 20 | [2,22,25,27] |
| Generalised Linear Mixed Regression Model | 5 | 20 | [31,36] |
| Multinomial Regression | 1 | 4 | [21] |
| Total | 25 * | 100 |
| Risk Factor: Child-Related Variables | Number of Studies Which Investigated the Risk Factor (%) | References |
|---|---|---|
| Age of the child | 23/24 (96%) | [2,18,19,21,22,23,24,25,27,28,29,30,32,33,34,35,36] |
| Sex of the child | 17/24 (71%) | [2,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,35,36] |
| Has health insurance | 4/24 (17%) | [18,28,31,32] |
| Perceived birth size | 3/24 (12%) | [2,22,33] |
| Ever had vaccination status | 1/24 (4%) | [35] |
| Product of multiple births | 2/24 (8%) | [23,32] |
| Preceding birth interval | 1/24 (4%) | [23] |
| Birth order | 6/24 (25%) | [23,25,26,28,33] |
| Iron supplement | 4/24 (17%) | [2,20,21] |
| Duration of breastfeeding | 4/24 (17%) | [20,21,22,35] |
| Breastfeeding | 2/24 (8%) | [22,23] |
| Had diarrhoea in last 2 weeks | 12/24 (50%) | [20,21,23,25,26,34,35,36] |
| Had fever in last 2 weeks | 11/24 46%) | [20,21,23,26,31,35,36] |
| Vitamin A consumption | 4/24 (16.6%) | [20,21,22,27] |
| Min Dietary Diversity (MDD) | 1/24 (4%) | [22] |
| Min Meal Frequency (MMF) | 1/24 (4%) | [22] |
| Treatment for intestinal worms in the last 6 months | 3/24 (12%) | [20,23,36] |
| Nutrition status | 1/24 (4%) | [24] |
| Stunting | 9/24 (37%) | [2,23,25,27,36] |
| Wasting | 3/24 (12%) | [2,27] |
| Underweight | 5/24 (20%) | [36] |
| Overweight | 1/24 (4%) | [32] |
| Malaria status (blood smear) | 3/24 (12%) | [19,24,26] |
| Malaria status (rapid test) | 1/24 (4%) | [30] |
| Parental/Caregiver-Related Variables | Number of Studies That Investigated the Risk Factors | References |
|---|---|---|
| Mother’s age in years (grouped) | 13/24 (54%) | [18,22,23,25,26,27,28,32,33,34,36] |
| Mother’s age at child’s birth | 1/24 (4%) | [21] |
| Mother working Status | 6/24 (25%) | [2,24,28,32,33,34] |
| Mother’s educational status | 20/24 (83%) | [2,18,20,21,22,24,25,27,28,29,30,31,32,33,34,36] |
| Father’s educational status | 4/24 (17%) | [25,28,33] |
| Father is alive at the date of the survey | 1/24 (4%) | [24] |
| Mother’s marital status | 3/24 (12%) | [2,28,32] |
| Mother’s body mass index (kg/m2) | 4/24 (17%) | [21,22,23,31] |
| Mother’s anaemia status | 12/24 (50%) | [21,22,23,24,26,27,31,33,34,36] |
| ANC attendance | 1/24 (4%) | [22] |
| Religion status | 2/24 (8%) | [28,33] |
| Mother’s iron supplementation during pregnancy | ¼ (4%) | [21] |
| Household-Related Variables | Number of Studies Which Investigated the Risk Factor | References |
|---|---|---|
| Wealth status | 21/24 (87%) | [2,18,19,20,21,22,23,24,25,27,28,29,30,31,32,34,36] |
| Place of residence | 18/24 (75%) | [2,18,20,22,23,24,25,26,27,29,30,36] |
| Household had bed net | 2/24 (8%) | [20,30] |
| Age of household head | 1/24 (4%) | [28] |
| Recent anti-malaria indoor residual spraying of household | 1/24 (4%) | [20] |
| Household size | 4/24 (17%) | [21,23,25,34] |
| Number of children under 5 in the household | 3/24 (12%) | [2,32,33,34] |
| Water source outside the premises | 1/24 (4%) | [23] |
| Improved source of drinking water | 8/24 (33%) | [2,20,22,23,25,29,33] |
| Improved type of toilet facilities | 2/24 (8%) | [20,23] |
| Unsafe stool disposal | 1/24 (4%) | [23] |
| Improved floor material type | 1/24 (4%) | [23] |
| Sex of household head | 2/24 (8%) | [20] |
| Shared toilet facilities with other household members | 1/24 (4%) | [23] |
| Use biomass for cooking | 3/24 (12%) | [23,36] |
| Under-fives slept under mosquito nets last night | 4/24 (17%) | [19,21,25] |
| Household ownership of livestock | 1/24 (4%) | [20] |
| Community Variables | Number of Studies Which Investigated the Risk Factor | References |
|---|---|---|
| Community wealth | 4/24 (17%) | [20,36] |
| Community female education | 4/24 (17%) | [27,36] |
| Community distance to health facility | 3/24 (12%) | [36] |
| Community safe water access | 3/24 (12%) | [36] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Obasohan, P.E.; Walters, S.J.; Jacques, R.; Khatab, K. A Scoping Review of the Risk Factors Associated with Anaemia among Children Under Five Years in Sub-Saharan African Countries. Int. J. Environ. Res. Public Health 2020, 17, 8829. https://doi.org/10.3390/ijerph17238829
Obasohan PE, Walters SJ, Jacques R, Khatab K. A Scoping Review of the Risk Factors Associated with Anaemia among Children Under Five Years in Sub-Saharan African Countries. International Journal of Environmental Research and Public Health. 2020; 17(23):8829. https://doi.org/10.3390/ijerph17238829
Chicago/Turabian StyleObasohan, Phillips Edomwonyi, Stephen J. Walters, Richard Jacques, and Khaled Khatab. 2020. "A Scoping Review of the Risk Factors Associated with Anaemia among Children Under Five Years in Sub-Saharan African Countries" International Journal of Environmental Research and Public Health 17, no. 23: 8829. https://doi.org/10.3390/ijerph17238829
APA StyleObasohan, P. E., Walters, S. J., Jacques, R., & Khatab, K. (2020). A Scoping Review of the Risk Factors Associated with Anaemia among Children Under Five Years in Sub-Saharan African Countries. International Journal of Environmental Research and Public Health, 17(23), 8829. https://doi.org/10.3390/ijerph17238829