Towards a New System for the Assessment of the Quality in Care Pathways: An Overview of Systematic Reviews

 ,
,  , , ,
, , ,
Abstract
1. Introduction
2. Methods
2.1. Research Question
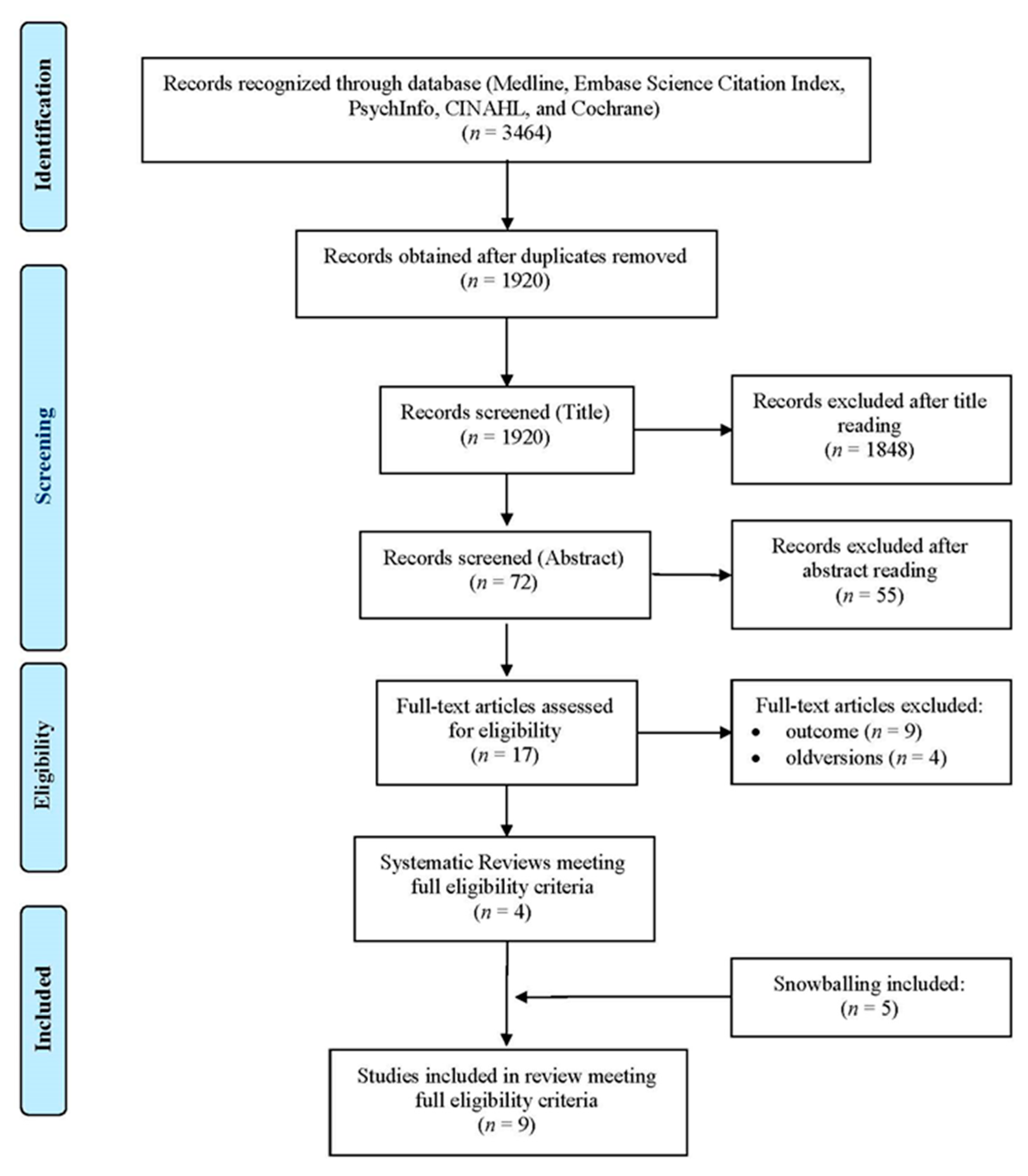
2.2. Search Strategy
2.3. Definition of Measurement Instruments
2.4. Eligibility Criteria
2.5. Data Extraction
2.6. Quality Appraisal of Reviews
2.7. Statistical Analysis
3. Results
3.1. Terminology and Definitions of CP
3.2. Synthesis of Reviews Included
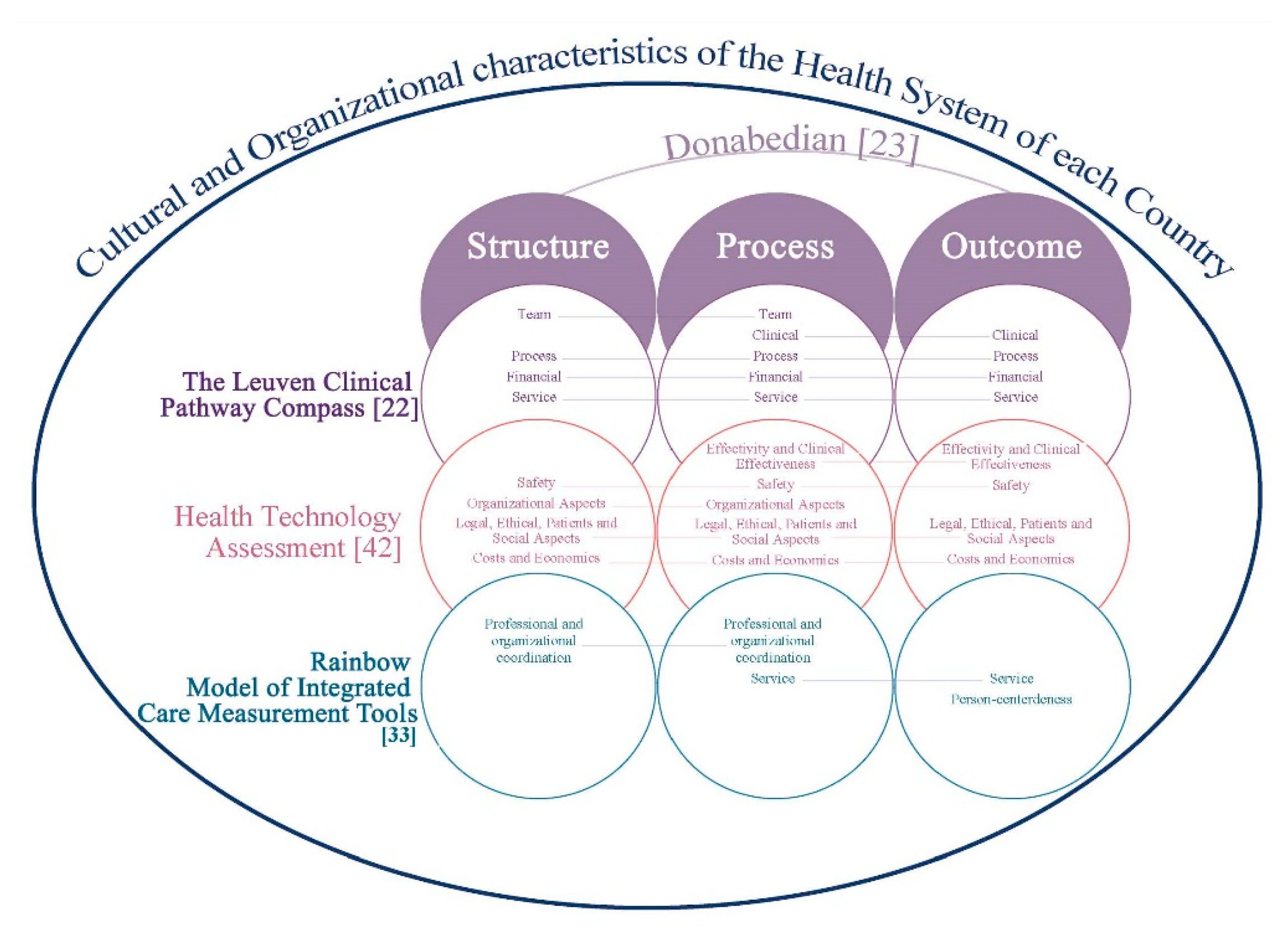
3.3. Prevalent Domains and Categorization of Indicators with Donabedian’s Model
3.4. Instruments/Tools
3.5. Quality Appraisal of Reviews
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- European Pathway Association. Care Pathways. Available online: http://e-p-a.org/care-pathways/ (accessed on 2 July 2020).
- Vanhaecht, K.; Bollmann, M.; Bower, K.; Gallagher, C.; Gardini, A.; Guezo, J.; Jansen, U.; Massoud, T.; Moody, K.; Sermeus, W.; et al. Prevalence and use of clinical pathways in 23 countries—An international survey by the European Pathway Association. J. Integr. Care Pathw. 2006, 10, 28–34. [Google Scholar]
- Kreindler, S.A.; Larson, B.K.; Wu, F.M.; Carluzzo, K.L.; Gbemudu, J.N.; Struthers, A.; Van Citters, A.D.; Shortell, S.M.; Nelson, E.C.; Fisher, E.S. Interpretations of integration in early accountable care organizations. Milbank Q. 2012, 90, 457–483. [Google Scholar] [CrossRef] [PubMed]
- Jiwani, I.; Fleury, M.J. Divergent modes of integration: The Canadian way. Int. J. Integr. Care. 2011, 11, e018. [Google Scholar] [CrossRef] [PubMed]
- El Baz, N.; Middel, B.; van Dijk, J.P.; Oosterhof, A.; Boonstra, P.W.; Reijneveld, S.A. Are the outcomes of clinical pathways evidence-based? A critical appraisal of clinical pathway evaluation research. J. Eval. Clin. Pract. 2007, 13, 920–992. [Google Scholar] [CrossRef] [PubMed]
- Vanhaecht, K.; Panella, M.; van Zelm, R.; Sermeus, W. An overview on the history and concept of care pathways as complex interventions. Int. J. Care Pathw. 2010, 14, 117–123. [Google Scholar] [CrossRef]
- Panella, M.; Marchisio, S.; Di Stanislao, F. Reducing clinical variations with clinical pathways: Do pathways work? Int. J. Qual. Health Care 2003, 15, 509–521. [Google Scholar] [CrossRef] [PubMed]
- Wensing, M.; Elwyn, G. Methods for incorporating patients’ views in health care. BMJ 2003, 326, 877–879. [Google Scholar] [CrossRef]
- Campbell, M.; Fitzpatrick, R.; Haines, A.; Kinmonth, A.L.; Sandercock, P.; Spiegelhalter, D.; Tyrer, P. Framework for design and evaluation of complex interventions to improve health. BMJ 2000, 321, 694–696. [Google Scholar] [CrossRef]
- Ruggeri, M.; Manca, A.; Coretti, S.; Codella, P.; Iacopino, V.; Romano, F.; Mascia, D.; Orlando, V.; Cicchetti, A. Investigating the Generalizability of Economic Evaluations Conducted in Italy: A Critical Review. Value Health 2015, 18, 709–720. [Google Scholar] [CrossRef]
- Verbeek, J.; Hiligsmann, M.; Cicchetti, A.; Marchetti, M. Sharing and collecting hospital-based health technology assessment reports internationally: Is an extensive participation of stakeholders realistic? Int. J. Technol. Assess. Health Care 2018, 34, 527–534. [Google Scholar] [CrossRef]
- Vanhaecht, K.; De Witte, K.; Panella, M.; Sermeus, W. Do pathways lead to better organized care processes? J. Eval. Clin. Pract. 2009, 15, 782–788. [Google Scholar] [CrossRef] [PubMed]
- Whittle, C.L.; McDonald, P.; Dunn, L. Developing the Integrated Care Pathway appraisal tool (ICPAT): A pilot study. J. Integr. Care Pathw. 2004, 8, 77–81. [Google Scholar] [CrossRef]
- Kinsman, L.; Rotter, T.; James, E.; Snow, P.; Willis, J. What is a clinical pathway? Development of a definition to inform the debate. BMC Med. 2010, 8, 31. [Google Scholar] [CrossRef] [PubMed]
- Vanhaecht, K.; Panella, M.; van Zelm, R.; Sermeus, W. Is there a future for pathways? Five pieces of the puzzle. Int. J. Care Pathw. 2009, 13, 82–86. [Google Scholar] [CrossRef]
- Noto, G.; Raschetti, R.; Maggini, M. Gestione Integrata e Percorsi Assistenziali; Il Pensiero Scientifico Editore: Rome, Italy, 2011; pp. 48–63. [Google Scholar]
- Toy, J.M.; Drechsler, A.; Waters, R.C. Clinical pathways for primary care: Current use, interest and perceived usability. J. Am. Med. Inform. Assoc. 2018, 25, 901–906. [Google Scholar] [CrossRef] [PubMed]
- Song, X.P.; Tian, J.H.; Cui, Q.; Zhang, T.T.; Yang, K.H.; Ding, G.W. Could clinical pathways improve the quality of care in patients with gastrointestinal cancer? A meta-analysis. Asian Pac. J. Cancer Prev. 2014, 15, 8361–8366. [Google Scholar] [CrossRef] [PubMed]
- Barbieri, A.; Vanhaecht, K.; Van Herck, P.; Sermeus, W.; Faggiano, F.; Marchisio, S.; Panella, M. Effects of clinical pathways in the joint replacement: A meta-analysis. BMC Med. 2009, 7, 32. [Google Scholar] [CrossRef]
- Sloan, D.M.; Guinane, C.S. Analysing Clinical Care Pathways: 3-Dimensional Tools for Quality Outcomes Measurement and Improvement; McGraw-Hill: Washington, DC, USA, 1999; pp. 18–35. [Google Scholar]
- Donabedian, A. Evaluating the Quality of Medical Care. Milbank Meml. Fund Q. 2005, 83, 691–729. [Google Scholar] [CrossRef]
- Vanhaecht, K.; Sermeus, W. The Leuven Clinical Pathway Compass. J. Integr. Care Pathw. 2003, 7, 2–7. [Google Scholar] [CrossRef]
- Donabedian, A. Twenty Years of Research on the Quality of Medical Care: 1964–1984. Eval. Health Prof. 1985, 8, 243. [Google Scholar] [CrossRef]
- Shea, B.J.; Reeves, B.C.; Wells, G.; Thuku, M.; Hamel, C.; Moran, J.; Moher, D.; Tugwell, P.; Welch, V.; Kristjansson, E.; et al. AMSTAR 2: A critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ 2017, 358, j4008. [Google Scholar] [CrossRef] [PubMed]
- Vanhaecht, K.; De Witte, K.; Depreitere, R.; Sermeus, W. Clinical pathway audit tools: A systematic review. J. Nurs. Manag. 2006, 14, 529–537. [Google Scholar] [CrossRef] [PubMed]
- Lemmens, L.; van Zelm, R.; Vanhaecht, K.; Kerkkamp, H. Systematic review: Indicators to evaluate effectiveness of clinical pathways for gastrointestinal surgery. J. Eval. Clin. Pract. 2008, 14, 880–887. [Google Scholar] [CrossRef] [PubMed]
- Van Zelm, R.; Janssen, I.; Vanhaecht, K.; van Overstraeten, A.d.B.; Panella, M.; Sermeus, W.; Coeckelberghs, E. Development of a model care pathway for adults undergoing colorectal cancer surgery: Evidence-based key interventions and indicators. J. Eval. Clin. Pract. 2018, 24, 232–239. [Google Scholar] [CrossRef] [PubMed]
- Strandberg-Larsen, M.; Krasnik, A. Measurement of integrated healthcare delivery: A systematic review of methods and future research directions. Int. J. Integr. Care 2009, 9, e01. [Google Scholar] [CrossRef] [PubMed]
- Lyngsø, A.M.; Godtfredsen, N.S.; Høst, D.; Frølich, A. Instruments to assess integrated care: A systematic review. Int. J. Integr. Care 2014, 14, e027. [Google Scholar] [CrossRef]
- Uijen, A.A.; Heinst, C.W.; Schellevis, F.G.; van den Bosch, W.J.H.M.; van de Laar, F.A.; Terwee, C.B.; Schers, H.J. Measurement Properties of Questionnaires Measuring Continuity of Care: A Systematic Review. PLoS ONE 2012, 7, e42256. [Google Scholar] [CrossRef]
- Bautista, M.A.; Nurjono, M.; Lim, Y.W.; Dessers, E.; Vrijhoef, H.J. Instruments Measuring Integrated Care: A Systematic Review of Measurement Properties. Milbank Q. 2016, 94, 862–917. [Google Scholar] [CrossRef]
- Suter, E.; Oelke, N.D.; Lima, M.d.S.; Stiphout, M.; Janke, R.; Witt, R.R.; Van Vliet-Brown, C.; Schill, K.; Rostami, M.; Hepp, S.; et al. Indicators and Measurement Tools for Health Systems Integration: A Knowledge Synthesis. Int. J. Integr. Care 2017, 17, 4. [Google Scholar] [CrossRef]
- Valentijn, P.P.; Pereira, F.; Sterner, C.W.; Vrijhoef, H.; Ruwaard, D.; Hegbrant, J.; Strippoli, G. Validation of the Rainbow Model of Integrated Care Measurement Tools (RMIC-MTs) in renal care for patient and care providers. PLoS ONE 2019, 14, e0222593. [Google Scholar] [CrossRef]
- Schuur, J.D.; Baugh, C.W.; Hess, E.P.; Hilton, J.A.; Pines, J.M.; Asplin, B.R. Critical pathways for post-emergency outpatient diagnosis and treatment: Tools to improve the value of emergency care. Acad. Emerg. Med. 2011, 18, e52–e63. [Google Scholar] [CrossRef] [PubMed]
- De Luc, K.; Kitchiner, D.; Layton, A.; Morris, E.; Murray, Y.; Overill, S. Developing Care Pathways: The Handbook; Routledge: London, UK, 2001; pp. 1–79. [Google Scholar]
- De Bleser, L.; Depreitere, R.; De Waele, K.; Vanhaecht, K.; Vlayen, J.; Sermeus, W. Defining pathways. J. Nurs. Manag. 2006, 14, 553–563. [Google Scholar] [CrossRef] [PubMed]
- Lawal, A.K.; Rotter, T.; Kinsman, L.; Machotta, A.; Ronellenfitsch, U.; Scott, S.D.; Goodridge, D.; Plishka, C.; Groot, G. What is a clinical pathway? Refinement of an operational definition to identify clinical pathway studies for a Cochrane systematic review. BMC Med. 2016, 14, 35. [Google Scholar] [CrossRef] [PubMed]
- Schrijvers, G.; van Hoorn, A.; Huiskes, N. The Care Pathway Concept: Concepts and theories: An introduction. Int. J. Integr. Care 2012, 12, e192. [Google Scholar] [CrossRef] [PubMed]
- Hébert, R.; Veil, A. Monitoring the degree of implementation of an integrated delivery system. Int. J. Integr. Care 2004, 4, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Zander, K. Integrated Care Pathways: Eleven international trends. J. Integr. Care Pathw. 2002, 6, 101–107. [Google Scholar] [CrossRef]
- Versi, E. ‘Gold standard’ is an appropriate term. BMJ 1992, 305, 187. [Google Scholar] [CrossRef]
- Ruggeri, M.; Cadeddu, C.; Roazzi, P.; Mandolini, D.; Grigioni, M.; Marchetti, M. Multi-Criteria-Decision-Analysis (MCDA) for the Horizon Scanning of Health Innovations an Application to COVID 19 Emergency. Int. J. Environ. Res. Public Health 2020, 17, 7823. [Google Scholar] [CrossRef]
- Moore, G.F.; Audrey, S.; Barker, M.; Bond, L.; Bonell, C.; Hardeman, W.; Moore, L.; O’Cathain, A.; Tinati, T.; Wight, D.; et al. Process evaluation of complex interventions: Medical Research Council guidance. BMJ 2015, 350, h1258. [Google Scholar] [CrossRef]
- Munro, A.; Bloor, M. Process evaluation: The new miracle ingredient in public health research? Qual. Res. 2010, 10, 699–713. [Google Scholar] [CrossRef]
- Di Muzio, M.; Giannetta, N.; Calagna, O.; Liquori, G.; Gazzelloni, A.; Di Simone, E.; Sollazzo, F.; Moriconi, A.; Latina, R.; Dionisi, S.; et al. Pain management in ERAS® approach for abdominal surgery: A narrative review. BPA Appl. Psychol. Bull. 2019, 67, 2–12. [Google Scholar]
- Italian Minister of Health: Il Nuovo Sistema di Garanzia (NSG). Available online: http://www.salute.gov.it/portale/lea/dettaglioContenutiLea.jsp?lingua=italiano&id=5238&area=Lea&menu=monitoraggioLea (accessed on 1 September 2020).
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. Cochrane Handbook for Systematic Reviews of Interventions Version 6.0; Cochrane: London, UK, 2019; Available online: www.training.cochrane.org/handbook (accessed on 1 September 2020).
- Iannone, P.; Coclite, D.; Napoletano, A.; Fauci, A.; Graziano, G.; Iacorossi, L.; D’Angelo, D. The new National Guidelines System in Italy: A first evaluation. G. Ital. Nefrol. 2019. Available online: https://giornaleitalianodinefrologia.it/wp-content/uploads/sites/3/2019/06/36-3-2019-1.pdf (accessed on 20 November 2020).
- Schrijvers, G. Disease management: A proposal for a new definition. Int. J. Integr. Care 2009, 9, e06. [Google Scholar] [CrossRef] [PubMed]
- Castro, E.M.; Van Regenmortel, T.; Vanhaecht, K.; Sermeus, W.; Van Hecke, A. Patient empowerment, patient participation and patient-centeredness in hospital care: A concept analysis based on a literature review. Patient Educ. Couns. 2016, 99, 1923–1939. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| n. | Authors (Year) | Title | Focus |
|---|---|---|---|
| 1 | Vanhaecht et al., (2006) [25] | Clinical pathway audit tools: a systematic review | Clinical Pathways |
| 2 | Lemmens et al., (2008) [26] | Systematic review: indicators to evaluate effectiveness of clinical pathways for gastrointestinal surgery | Clinical Pathways |
| 3 | van Zelm et al., (2018) [27] | Development of a model care pathway for adults undergoing colorectal cancer surgery: evidence-based key interventions and indicators | Clinical Pathways |
| 4 | Strandberg-Larsen et al., (2009) [28] | Measurement of integrated healthcare delivery: a systematic review of methods and future research directions | Integrated Care |
| 5 | Lyngsø et al., (2014) [29] | Instruments to assess integrated care: a systematic review | Integrated Care |
| 6 | Uijen et al., (2012) [30] | Measurement properties of questionnaires measuring continuity of care: a systematic review | Integrated Health Care |
| 7 | Bautista et al., (2016) [31] | Instruments measuring integrated care: a systematic review of measurement properties | Integrated Care |
| 8 | Suter et al., (2017) [32] | Indicators and measurement tools for health systems integration: a knowledge synthesis | Integrated Care |
| 9 | Valentijn et al., (2019) [33] | Validation of the Rainbow Model of Integrated Care Measurement Tools (RMIC-MTs) in renal care for patient and care providers | Integrated Care |
| The Leuven Clinical Pathway Compass (2003) [22] | 1. Vanhaecht et al., (2006) [25] | 2. Lemmens et al., (2008) [26] | 3. van Zelm et al., (2016) [27] | 4. Strandberg-Larsen et al., (2009) [28] | 5. Uijen et al., (2012) [30] | 6. Bautista et al., (2016) [31] | 7. Suter et al., (2017) [32] | Total |
|---|---|---|---|---|---|---|---|---|
| DOMAINS and Indicators | n | n | n | n | n | n | n | n (%) |
| (1) Team | 0 | |||||||
| Influence on team satisfaction | 1 | 1 | ||||||
| Multidisciplinary involvement/team effectiveness | 7 | 10 | 12 | 29 | ||||
| Physician integration within care teams/professional Integration/nursing care integration | 5 | 11 | 6 | 22 | ||||
| Supporting services (i.e., education and social services) | 14 | 6 | 20 | |||||
| Total Team | 72 (9.8) | |||||||
| (2) Clinical | ||||||||
| Complication rate | 14 | 14 | ||||||
| Compliance to protocol | 1 | 1 | ||||||
| Discharge destination | 15 | 15 | ||||||
| Mortality | 10 | 6 | 16 | |||||
| Number of admissions or length of stay on HDU/ICU * | 4 | 4 | ||||||
| Number of complications/post-operative morbidity | 16 | 16 | ||||||
| Number of re-admissions | 3 | 3 | ||||||
| Number of re-operations | 2 | 2 | ||||||
| Pain scores/post-operative pain | 2 | 3 | 5 | |||||
| Post-operative treatment with fluids | 2 | 2 | ||||||
| Readmission rate (<30 days) | 0 | |||||||
| Removal of bladder catheter | 2 | 3 | 5 | |||||
| Reoperation/intervention | 2 | 2 | ||||||
| Time taken to mobilize | 11 | 11 | ||||||
| Use of intravenous catheter | 1 | 1 | ||||||
| Stress Index | 1 | 1 | ||||||
| Total Clinical | 98 (13.2) | |||||||
| (3) Process | 0 | |||||||
| Accountability | 4 | 4 | ||||||
| Appropriate use of antibiotics/others | 1 | 1 | ||||||
| Completeness and quality of documentation/data tracked and shared with stakeholders/informatic integration | 3 | 1 | 3 | 1 | 8 | |||
| Clinical outcomes being measured | 2 | 2 | ||||||
| Care continuity/clinical integration | 8 | 17 | 172 | 197 | ||||
| EBM/guideline | 5 | 5 | ||||||
| Implementation of pathway | 3 | 3 | ||||||
| Maintenance of pathway | 5 | 5 | ||||||
| Number of clinical examinations (labs, radiology) | 3 | 3 | ||||||
| Organizational goals and objectives aligned across sectors | 1 | 1 | ||||||
| Outcome management | 7 | 7 | ||||||
| Performance measurement domains and tools in place | 2 | 2 | ||||||
| Primary care network structures | 8 | 8 | 16 | |||||
| Safety (risk management) | 7 | 7 | ||||||
| Transitional (transferring care from one area to another) | 17 | 17 | ||||||
| Use of shared clinical pathways across the continuum of healthcare (e.g., diabetes, asthma care) Organizational integration or coordination and specialty/or combination | 4 | 40 | 7 | 51 | ||||
| Total Process | 329 (44.4) | |||||||
| (4) Financial | ||||||||
| Attainment of goals and objectives are supported by funding and human resource allocation | 1 | 1 | ||||||
| Influence on length of stay | 20 | 15 | 35 | |||||
| Influence on length of stay HDU/ICU | 1 | 1 | ||||||
| Influence on medical costs | 5 | 5 | ||||||
| Total Financial | 42 (5.3) | |||||||
| (5) Service | ||||||||
| Influence on patient satisfaction | 6 | 1 | 7 | |||||
| Individualization of care pathways for patients with co-morbidities | 7 | 7 | ||||||
| Patient centered care/family involvement in care planning | 3 | 148 | 34 | 185 | ||||
| Quality of life (SF-36) | 1 | 1 | 2 | |||||
| Total Service | 201 (27.3) |
| n. | Authors | Items of AMSTAR 2 | Overall Rating Quality | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 * | 3 | 4 * | 5 | 6 | 7 | 8 | 9 * | 10 | 11 * | 12 | 13 * | 14 ** | 15 * | 16 | |||
| 1 | Vanhaecht et al., (2006) [25] | NA | PY | Y | PY | Y | Y | Y | Y | NA | N | NA | NA | NA | Y | Y | N | Low |
| 2 | Lemmens et al., (2008) [26] | NA | PY | Y | PY | Y | Y | Y | Y | NA | Y | NA | NA | NA | Y | Y | PY | Moderate |
| 3 | van Zelm et al., (2018) [27] | NA | PY | Y | Y | Y | Y | Y | Y | NA | Y | NA | NA | NA | Y | Y | N | High |
| 4 | Strandberg-Larsen et al., (2009) [28] | NA | PY | Y | Y | Y | Y | Y | Y | NA | Y | NA | NA | NA | Y | N | N | Low |
| 5 | Lyngsø et al., (2014) [29] | NA | PY | Y | PY | N | N | PY | PY | NA | N | NA | NA | NA | Y | Y | N | Critically Low |
| 6 | Uijen et al., (2012) [30] | NA | PY | Y | PY | Y | Y | Y | Y | NA | Y | NA | NA | NA | Y | Y | Y | Moderate |
| 7 | Bautista et al., (2016) [31] | NA | PY | Y | Y | Y | Y | Y | Y | NA | Y | NA | NA | NA | Y | Y | Y | High |
| 8 | Suter et al., (2017) [32] | NA | PY | Y | PY | Y | Y | Y | Y | NA | Y | NA | NA | NA | Y | Y | Y | Moderate |
| 9 | Valentijn et al., (2019) [33] | NA | PY | Y | Y | Y | Y | PY | Y | NA | Y | NA | NA | NA | Y | Y | Y | High |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Latina, R.; Salomone, K.; D’Angelo, D.; Coclite, D.; Castellini, G.; Gianola, S.; Fauci, A.; Napoletano, A.; Iacorossi, L.; Iannone, P. Towards a New System for the Assessment of the Quality in Care Pathways: An Overview of Systematic Reviews. Int. J. Environ. Res. Public Health 2020, 17, 8634. https://doi.org/10.3390/ijerph17228634
Latina R, Salomone K, D’Angelo D, Coclite D, Castellini G, Gianola S, Fauci A, Napoletano A, Iacorossi L, Iannone P. Towards a New System for the Assessment of the Quality in Care Pathways: An Overview of Systematic Reviews. International Journal of Environmental Research and Public Health. 2020; 17(22):8634. https://doi.org/10.3390/ijerph17228634
Chicago/Turabian StyleLatina, Roberto, Katia Salomone, Daniela D’Angelo, Daniela Coclite, Greta Castellini, Silvia Gianola, Alice Fauci, Antonello Napoletano, Laura Iacorossi, and Primiano Iannone. 2020. "Towards a New System for the Assessment of the Quality in Care Pathways: An Overview of Systematic Reviews" International Journal of Environmental Research and Public Health 17, no. 22: 8634. https://doi.org/10.3390/ijerph17228634
APA StyleLatina, R., Salomone, K., D’Angelo, D., Coclite, D., Castellini, G., Gianola, S., Fauci, A., Napoletano, A., Iacorossi, L., & Iannone, P. (2020). Towards a New System for the Assessment of the Quality in Care Pathways: An Overview of Systematic Reviews. International Journal of Environmental Research and Public Health, 17(22), 8634. https://doi.org/10.3390/ijerph17228634