Time Course and Determinants of Individual Motivation among Women Enrolled in a Diet and Physical Activity Primary Prevention Trial

 ,
,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. The DAMA (Diet, Physical Activity and Mammography) Study
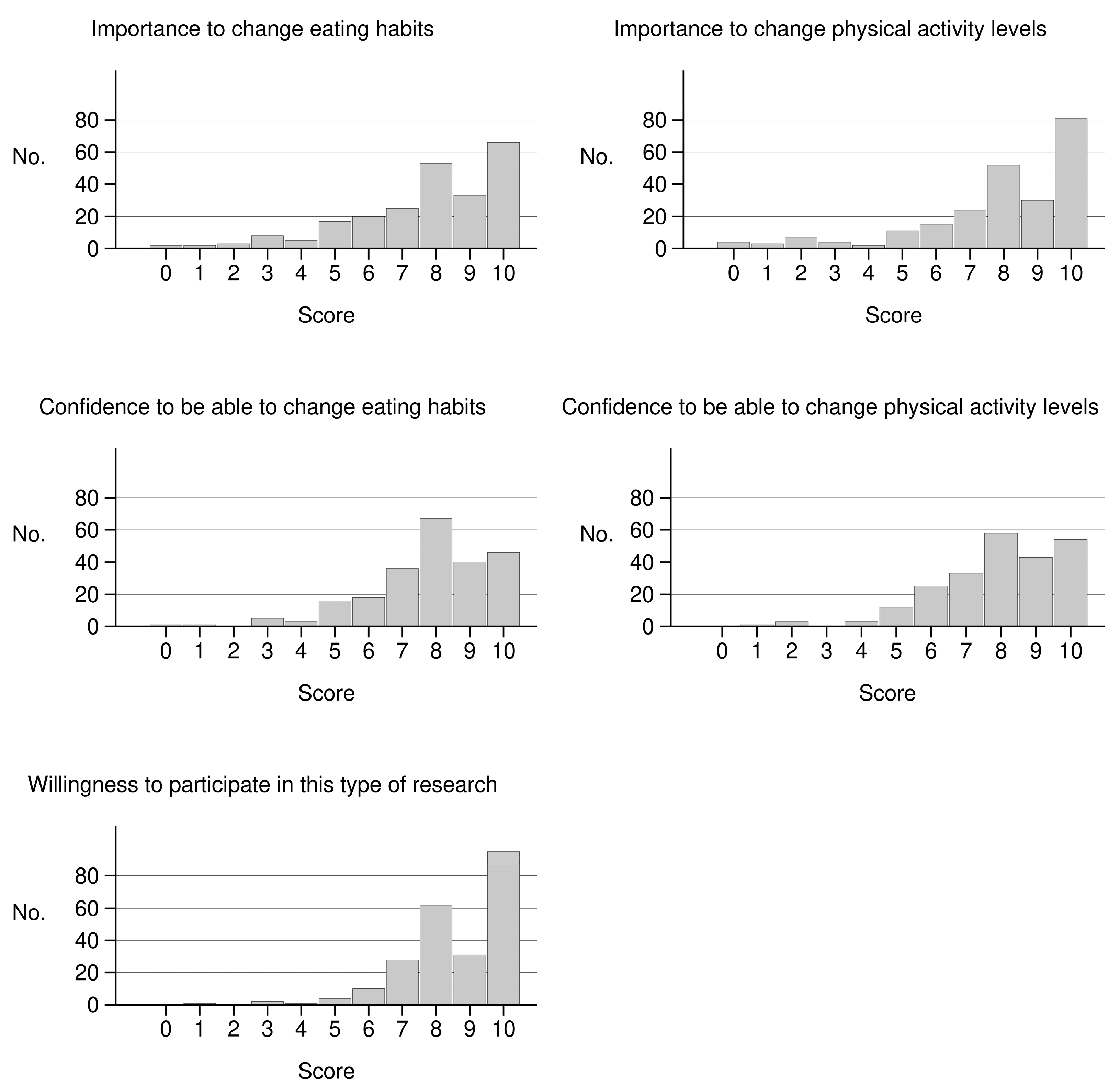
2.2. The Motivation Questionnaire
- How much do you think it is important to change your eating habits?
- How much do you think it is important to change your physical activity levels?
- How confident do you feel of being able to change your eating habits?
- How confident do you feel of being able to change your physical activity levels?
- How willing do you feel to participate in this type of research?
2.3. Statistical Analysis
2.4. Ethics
3. Results
3.1. Lifestyle Factors Associated with Motivation at Study Baseline
3.2. Changes in Motivation during the Study and Associated Factors
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- World Health Organization. Preventing Chronic Diseases: A Vital Investment: WHO Global Report. Available online: https://www.who.int/chp/chronic_disease_report/en/ (accessed on 12 June 2020).
- Delormier, T.; Frohlich, K.L.; Potvin, L. Food and eating as social practice--understanding eating patterns as social phenomena and implications for public health. Sociol. Health Illn. 2009, 31, 215–228. [Google Scholar] [CrossRef] [PubMed]
- Robinson, E.; Blissett, J.; Higgs, S. Social influences on eating: Implications for nutritional interventions. Nutr. Res. Rev. 2013, 26, 166–176. [Google Scholar] [CrossRef] [PubMed]
- Korhonen, M.; Kastarinen, M.; Uusitupa, M.; Pusk, P.; Nissinen, A. The effect of intensified diet counseling on the diet of hypertensive subjects in primary health care: A 2-year open randomized controlled trial of lifestyle intervention against hypertension in eastern Finland. Prev. Med. 2003, 36, 8–16. [Google Scholar] [CrossRef] [PubMed]
- Toft, U.; Kristoffersen, L.; Ladelund, S.; Ovesen, L.; Lau, C.; Pisinger, C.; von Huth Smith, L.; Borch-Johnsen, K.; Jørgensen, T. The effect of adding group-based counselling to individual lifestyle counselling on changes in dietary intake. The Inter99 study—A randomized controlled trial. Int. J. Behav. Nutr. Phys. Act. 2008, 5, 59. [Google Scholar] [CrossRef] [PubMed]
- Lin, J.S.; O’Connor, E.; Evans, C.V.; Senger, C.A.; Rowland, M.G.; Groom, H.C. Behavioral Counseling to Promote a Healthy Lifestyle in Persons with Cardiovascular Risk Factors: A Systematic Review for the U.S. Preventive Services Task Force. Ann. Intern. Med. 2014, 161, 568–578. [Google Scholar] [CrossRef] [PubMed]
- Dacey, M.L.; Kennedy, M.A.; Polak, R.; Phillips, E.M. Physical activity counseling in medical school education: A systematic review. Med. Educ. Online 2014, 19, 24325. [Google Scholar] [CrossRef] [PubMed]
- Lindberg, N.M.; Stevens, V.J.; Smith, K.S.; Glasgow, R.E.; Toobert, D.J. A brief intervention designed to increase breast cancer self-screening. Am. J. Health Promot. 2009, 23, 320–323. [Google Scholar] [CrossRef] [PubMed]
- Ismail, K.; Winkley, K.; Rabe-Hesketh, S. Systematic review and meta-analysis of randomised controlled trials of psychological interventions to improve glycaemic control in patients with type 2 diabetes. Lancet 2004, 363, 1589–1597. [Google Scholar] [CrossRef]
- Morrison, Z.; Douglas, A.; Bhopal, R.; Sheikh, A.; Trial Investigators. Understanding experiences of participating in a weight loss lifestyle intervention trial: A qualitative evaluation of South Asians at high risk of diabetes. BMJ Open 2014, 4, e004736. [Google Scholar] [CrossRef]
- Hammarström, A.; Wiklund, A.F.; Lindahl, B.; Larsson, C.; Ahlgren, C. Experiences of barriers and facilitators to weight-loss in a diet intervention-A qualitative study of women in northern Sweden. BMC Womens Health 2014, 14, 59. [Google Scholar] [CrossRef]
- Penn, L.; Dombrowski, S.U.; Sniehotta, F.F.; White, M. Perspectives of UK Pakistani women on their behaviour change to prevent type 2 diabetes: Qualitative study using the theory domain framework. BMJ Open 2014, 4, e004530. [Google Scholar] [CrossRef] [PubMed]
- Masala, G.; Assedi, M.; Caini, S.; Ermini, I.; Occhini, D.; Castaldo, M.; Bendinelli, B.; Zagni, D.; Tanzini, D.; Saieva, C.; et al. The DAMA trial: A diet and physical activity intervention trial to reduce mammographic breast density in postmenopausal women in Tuscany, Italy. Study protocol and baseline characteristics. Tumori 2014, 100, 377–385. [Google Scholar] [CrossRef] [PubMed]
- Masala, G.; Assedi, M.; Sera, F.; Ermini, I.; Occhini, D.; Castaldo, M.; Pierpaoli, E.; Caini, S.; Bendinelli, B.; Ambrogetti, D.; et al. Can Dietary and Physical Activity Modifications Reduce Breast Density in Postmenopausal Women? The DAMA Study, a Randomized Intervention Trial in Italy. Cancer Epidemiol. Biomark. Prev. 2019, 28, 41–50. [Google Scholar] [CrossRef] [PubMed]
- Palli, D.; Berrino, F.; Vineis, P.; Tumino, R.; Panico, S.; Masala, G.; Saieva, C.; Salvini, S.; Ceroti, M.; Pala, V.; et al. A molecular epidemiology project on diet and cancer: The EPIC-Italy Prospective Study. Design and baseline characteristics of participants. Tumori J. 2003, 89, 586–593. [Google Scholar] [CrossRef]
- Ainsworth, B.E.; Haskell, W.L.; Whitt, M.C.; Irwin, M.L.; Swartz, A.M.; Strath, S.J.; O’Brien, W.L.; Bassett, D.R., Jr.; Schmitz, K.H.; Emplaincourt, P.O.; et al. Compendium of physical activities: An update of activity codes and MET intensities. Med. Sci. Sports Exerc. 2000, 32 (Suppl. 9), S498–S504. [Google Scholar] [CrossRef]
- Rollnick, S.; Mason, P.; Butler, C. Cambiare Stili di Vita non Salutari. Strategie di Counseling Motivazionale Breve [In Italian]; Erickson: Trento, Italy, 2003. [Google Scholar]
- Miller, W.R. Motivational interviewing with problem drinkers. Behav. Psychother. 1983, 11, 147–172. [Google Scholar] [CrossRef]
- DiClemente, C.; Prochaska, J. Toward a comprehensive, transtheoretical model of change. In Treating Addictive Behaviours; Miller, W., Heather, N., Eds.; Plenum Press: New York, NY, USA, 1999. [Google Scholar]
- Prochaska, J.O.; DiClemente, C.C. The transtheoretical approach. In Handbook of Psychotherapy Integration, 2nd ed.; Norcross, J.C., Goldfried, M.R., Eds.; Oxford University Press: New York, NY, USA, 2005; pp. 147–171. [Google Scholar]
- Brookhart, M.A.; Patrick, A.R.; Dormuth, C.; Avorn, J.; Shrank, W.; Cadarette, S.M.; Solomon, D.H. Adherence to lipid-lowering therapy and the use of preventive health services: An investigation of the healthy user effect. Am. J. Epidemiol. 2007, 166, 348–354. [Google Scholar] [CrossRef]
- Silverman, S.L.; Gold, D.T. Healthy users, healthy adherers, and healthy behaviors? J. Bone Miner. Res. 2011, 26, 681–682. [Google Scholar] [CrossRef]
- Lagerlund, M.; Sparén, P.; Thurfjell, E.; Ekbom, A.; Lambe, M. Predictors of non-attendance in a population-based mammography screening programme; socio-demographic factors and aspects of health behaviour. Eur. J. Cancer Prev. 2000, 9, 25–33. [Google Scholar] [CrossRef]
- Younge, J.O.; Kouwenhoven-Pasmooij, T.A.; Freak-Poli, R.; Roos-Hesselink, J.W.; Hunink, M.G.M. Randomized study designs for lifestyle interventions: A tutorial. Int. J. Epidemiol. 2015, 44, 2006–2019. [Google Scholar] [CrossRef]
- Artinian, N.T.; Fletcher, G.F.; Mozaffarian, D.; Kris-Etherton, P.; Van Horn, L.; Lihtenstein, A.H.; Kumanyika, S.; Kraus, W.E.; Fleg, J.L.; Redeker, N.S.; et al. American Heart Association Prevention Committee of the Council on Cardiovascular Nursing. Interventions to promote physical activity and dietary lifestyle changes for cardiovascular risk factor reduction in adults: A scientific statement from the American Heart Association. Circulation 2010, 122, 406–441. [Google Scholar] [PubMed]
- Dalle Grave, R.; Calugi, S.; Centis, E.; El Ghoch, M.; Marchesini, G. Cognitive-behavioral strategies to increase the adherence to exercise in the management of obesity. J. Obes. 2011, 2011, 348293. [Google Scholar] [CrossRef] [PubMed]
- Prochaska, J.J.; Prochaska, J.O. A Review of Multiple Health Behavior Change Interventions for Primary Prevention. Am. J. Lifestyle Med. 2011, 5, 10. [Google Scholar] [CrossRef] [PubMed]
- Barnett, A.G.; van der Pols, J.C.; Dobson, A.J. Regression to the mean: What it is and how to deal with it. Int. J. Epidemiol. 2005, 34, 215–220. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| OR (a) | Lower 95% CI | Upper 95% CI | p(b) | ||
|---|---|---|---|---|---|
| How much do you think it is important to change your eating habits? | |||||
| Red and processed meat | 3rd vs. 1st tertile | 0.33 | 0.15 | 0.72 | 0.005 |
| Sweets, biscuits and cakes | 3rd vs. 1st tertile | 2.02 | 0.94 | 4.32 | 0.085 |
| Olive oil | 3rd vs. 1st tertile | 3.71 | 1.74 | 7.90 | 0.001 |
| Household physical activity | 3rd vs. 1st tertile | 2.01 | 0.96 | 4.23 | 0.064 |
| How confident do you feel of being able to change your eating habits? | |||||
| Drinks wine | current vs. never | 0.40 | 0.15 | 1.08 | 0.071 |
| Fruit | 3rd vs. 1st tertile | 2.13 | 0.99 | 4.57 | 0.055 |
| Rice and pasta | 3rd vs. 1st tertile | 0.44 | 0.21 | 0.92 | 0.031 |
| Coffee | 3rd vs. 1st tertile | 0.33 | 0.15 | 0.72 | 0.005 |
| Household physical activity | 3rd vs. 1st tertile | 2.04 | 0.97 | 4.30 | 0.058 |
| How much do you think it is important to change your physical activity levels? | |||||
| Red and processed meat | 3rd vs. 1st tertile | 0.46 | 0.22 | 0.99 | 0.049 |
| Olive oil | 3rd vs. 1st tertile | 2.85 | 1.31 | 6.19 | 0.009 |
| Recreational physical activity | 3rd vs. 1st tertile | 0.33 | 0.15 | 0.72 | 0.005 |
| How confident do you feel of being able to change your physical activity levels? | |||||
| Vegetables | 3rd vs. 1st tertile | 0.31 | 0.10 | 0.93 | 0.044 |
| Fruit | 3rd vs. 1st tertile | 2.49 | 1.12 | 5.54 | 0.028 |
| Red and processed meat | 3rd vs. 1st tertile | 0.47 | 0.22 | 1.02 | 0.056 |
| Olive oil | 3rd vs. 1st tertile | 4.34 | 1.44 | 13.07 | 0.015 |
| How willing do you feel to participate in this type of research? | |||||
| Drinks wine | current vs. never | 0.45 | 0.19 | 1.05 | 0.063 |
| Rice and pasta | 3rd vs. 1st tertile | 0.36 | 0.18 | 0.74 | 0.006 |
| Olive oil | 3rd vs. 1st tertile | 3.80 | 1.84 | 7.87 | <0.001 |
| Coffee | 3rd vs. 1st tertile | 0.49 | 0.24 | 0.98 | 0.043 |
| β (a) | Lower 95% CI | Upper 95% CI | p(b) | ||
|---|---|---|---|---|---|
| How much do you think it is important to change your eating habits? | |||||
| Study arm | Diet | 0.81 | 0.21 | 1.40 | 0.008 |
| Study arm | Physical activity | 0.55 | −0.05 | 1.15 | 0.072 |
| Study arm | Diet + physical activity | 0.60 | −0.01 | 1.20 | 0.053 |
| Smoking | Former vs. never | 0.45 | 0.01 | 0.89 | 0.044 |
| How confident do you feel of being able to change your eating habits? | |||||
| Study arm | Diet | 0.66 | 0.04 | 1.28 | 0.038 |
| Study arm | Physical activity | 0.49 | −0.14 | 1.12 | 0.129 |
| Study arm | Diet + physical activity | 0.67 | 0.02 | 1.31 | 0.043 |
| Red and processed meat | 3rd vs. 1st tertile | −1.00 | −1.55 | −0.45 | <0.001 |
| Fish | 3rd vs. 1st tertile | 0.52 | −0.06 | 1.10 | 0.075 |
| Wine | 3rd vs. 1st tertile | −0.69 | −1.35 | −0.03 | 0.038 |
| Dairy | 3rd vs. 1st tertile | 0.74 | 0.19 | 1.28 | 0.008 |
| Walking | 3rd vs. 1st tertile | 0.58 | −0.01 | 1.16 | 0.053 |
| How much do you think it is important to change your physical activity levels? | |||||
| Study arm | Diet | 0.71 | 0.16 | 1.26 | 0.012 |
| Study arm | Physical activity | 0.84 | 0.28 | 1.39 | 0.003 |
| Study arm | Diet + physical activity | 0.54 | −0.02 | 1.11 | 0.059 |
| Red and processed meat | 3rd vs. 1st tertile | −0.48 | −0.97 | 0.01 | 0.055 |
| Rice and pasta | 3rd vs. 1st tertile | −0.62 | −1.12 | −0.13 | 0.014 |
| Dairy | 3rd vs. 1st tertile | 0.50 | 0.01 | 1.00 | 0.042 |
| How confident do you feel of being able to change your physical activity levels? | |||||
| Study arm | Diet | 0.73 | 0.08 | 1.38 | 0.028 |
| Study arm | Physical activity | 0.97 | 0.31 | 1.63 | 0.004 |
| Study arm | Diet + physical activity | 0.27 | −0.39 | 0.92 | 0.428 |
| Red and processed meat | 3rd vs. 1st tertile | −0.63 | −1.20 | −0.07 | 0.029 |
| Legumes | 3rd vs. 1st tertile | 0.66 | 0.07 | 1.24 | 0.030 |
| Walking | 3rd vs. 1st tertile | 1.09 | 0.50 | 1.68 | <0.001 |
| How willing do you feel to participate in this type of research? | |||||
| Study arm | Diet | 0.73 | −0.09 | 1.56 | 0.080 |
| Study arm | Physical activity | 0.12 | −0.69 | 0.94 | 0.767 |
| Study arm | Diet + physical activity | 0.17 | −0.68 | 1.01 | 0.699 |
| Red and processed meat | 3rd vs. 1st tertile | −0.85 | −1.58 | −0.11 | 0.022 |
| Rice and pasta | 3rd vs. 1st tertile | −0.67 | −1.39 | 0.06 | 0.073 |
| Wine | 3rd vs. 1st tertile | −1.49 | −2.35 | −0.64 | 0.003 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Caini, S.; Assedi, M.; Grechi, E.; Ermini, I.; Zagni, D.; Occhini, D.; Castaldo, M.; Bendinelli, B.; Palli, D.; Masala, G. Time Course and Determinants of Individual Motivation among Women Enrolled in a Diet and Physical Activity Primary Prevention Trial. Int. J. Environ. Res. Public Health 2020, 17, 8589. https://doi.org/10.3390/ijerph17228589
Caini S, Assedi M, Grechi E, Ermini I, Zagni D, Occhini D, Castaldo M, Bendinelli B, Palli D, Masala G. Time Course and Determinants of Individual Motivation among Women Enrolled in a Diet and Physical Activity Primary Prevention Trial. International Journal of Environmental Research and Public Health. 2020; 17(22):8589. https://doi.org/10.3390/ijerph17228589
Chicago/Turabian StyleCaini, Saverio, Melania Assedi, Elisa Grechi, Ilaria Ermini, Donatella Zagni, Daniela Occhini, Maria Castaldo, Benedetta Bendinelli, Domenico Palli, and Giovanna Masala. 2020. "Time Course and Determinants of Individual Motivation among Women Enrolled in a Diet and Physical Activity Primary Prevention Trial" International Journal of Environmental Research and Public Health 17, no. 22: 8589. https://doi.org/10.3390/ijerph17228589
APA StyleCaini, S., Assedi, M., Grechi, E., Ermini, I., Zagni, D., Occhini, D., Castaldo, M., Bendinelli, B., Palli, D., & Masala, G. (2020). Time Course and Determinants of Individual Motivation among Women Enrolled in a Diet and Physical Activity Primary Prevention Trial. International Journal of Environmental Research and Public Health, 17(22), 8589. https://doi.org/10.3390/ijerph17228589