Classification of Whole-Body Postural Discomfort Using Cluster Analysis


Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
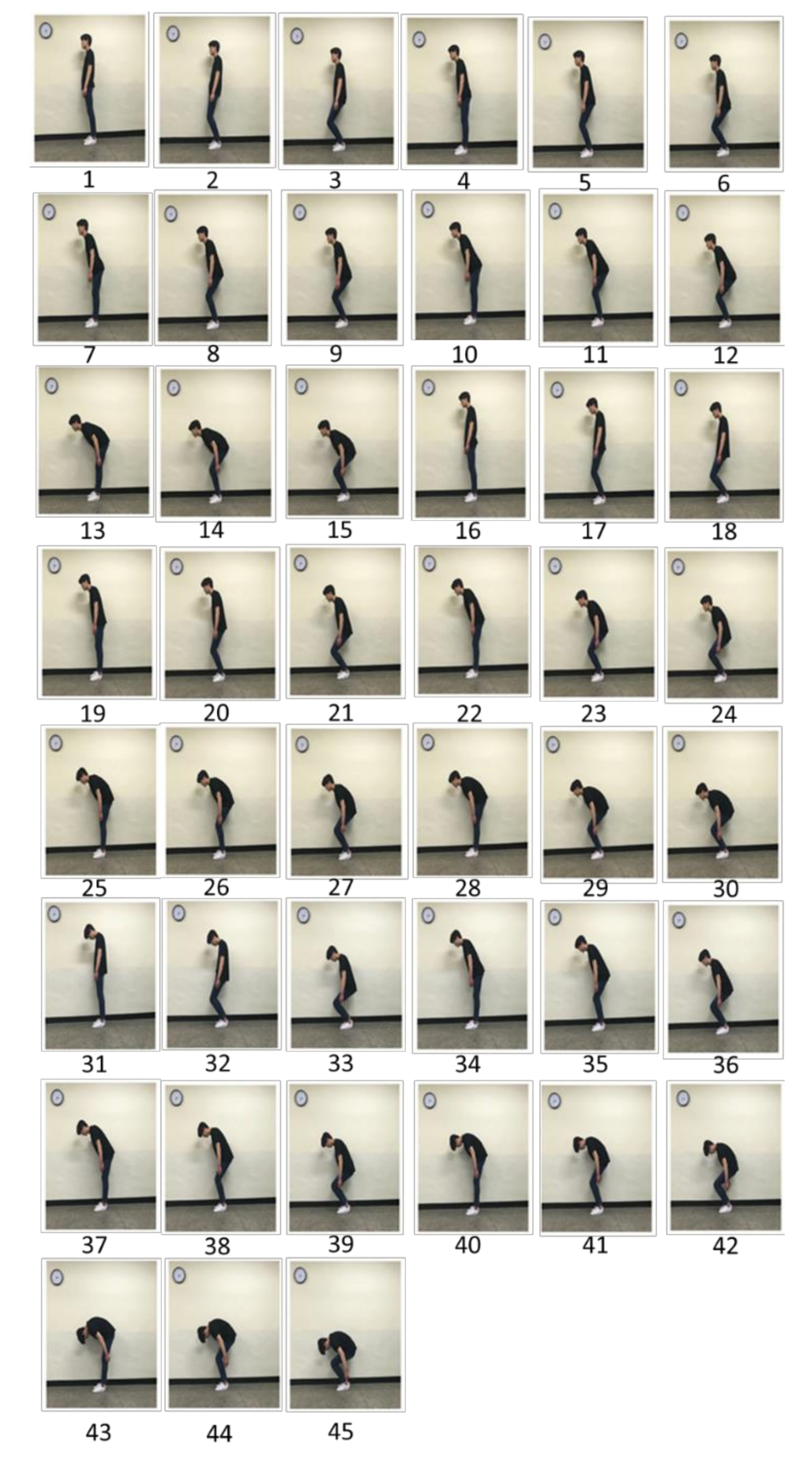
2.2. Experimental Protocol
2.3. Data Analysis
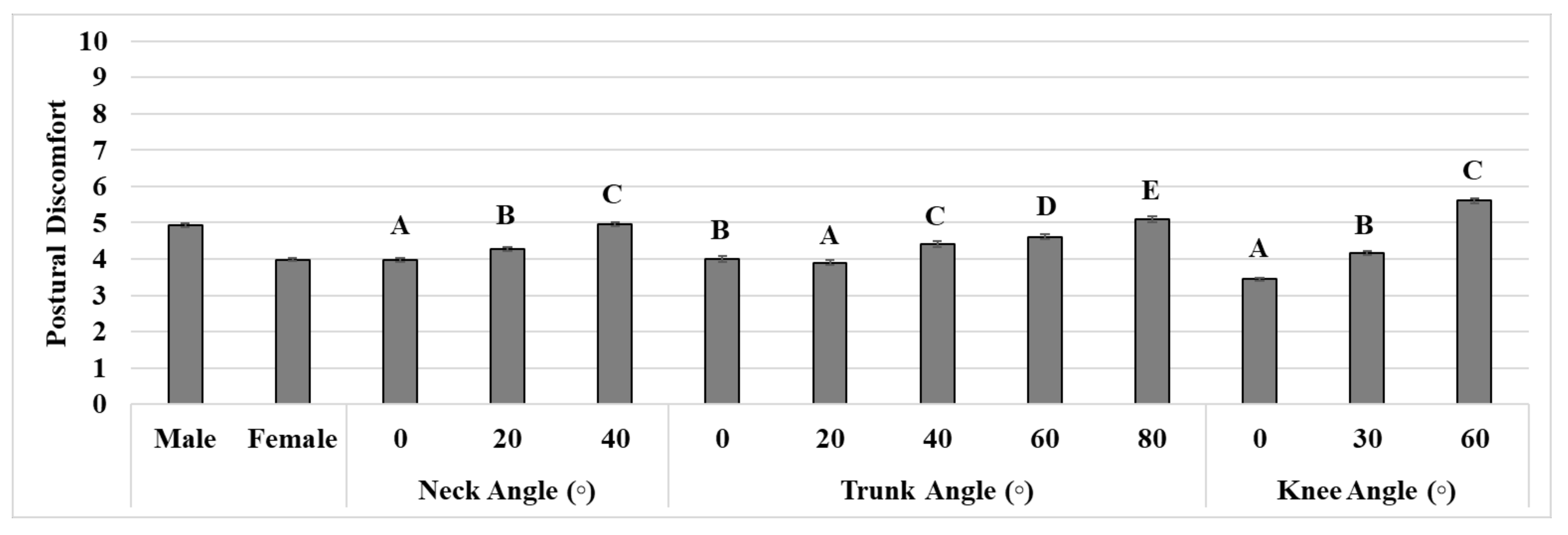
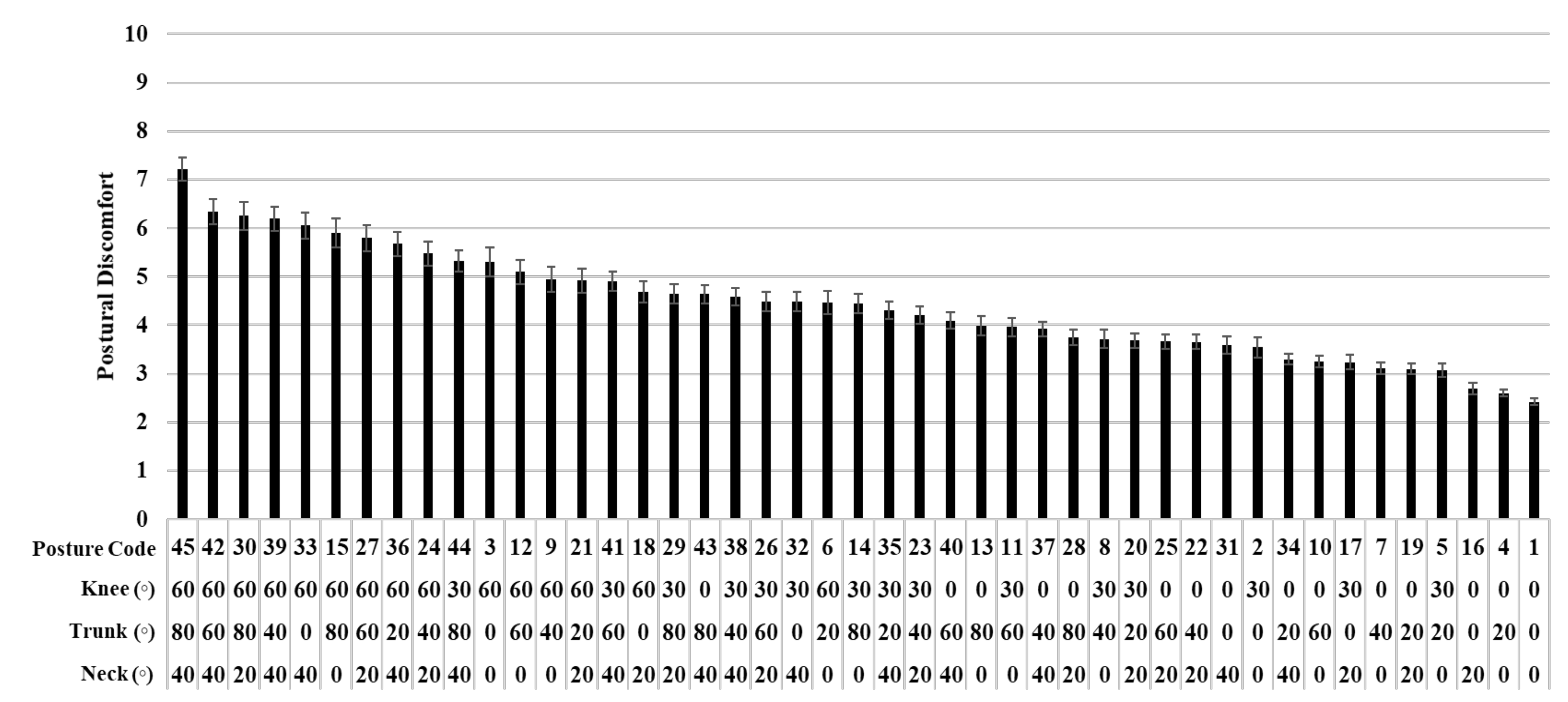
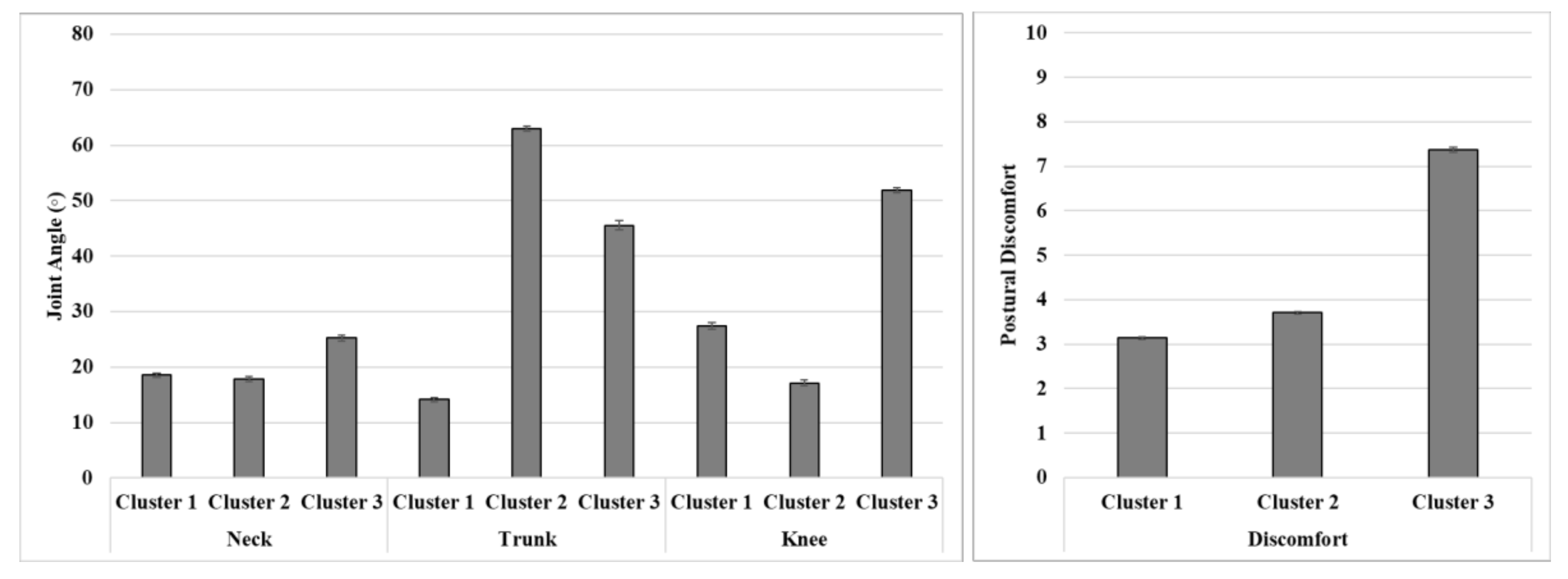
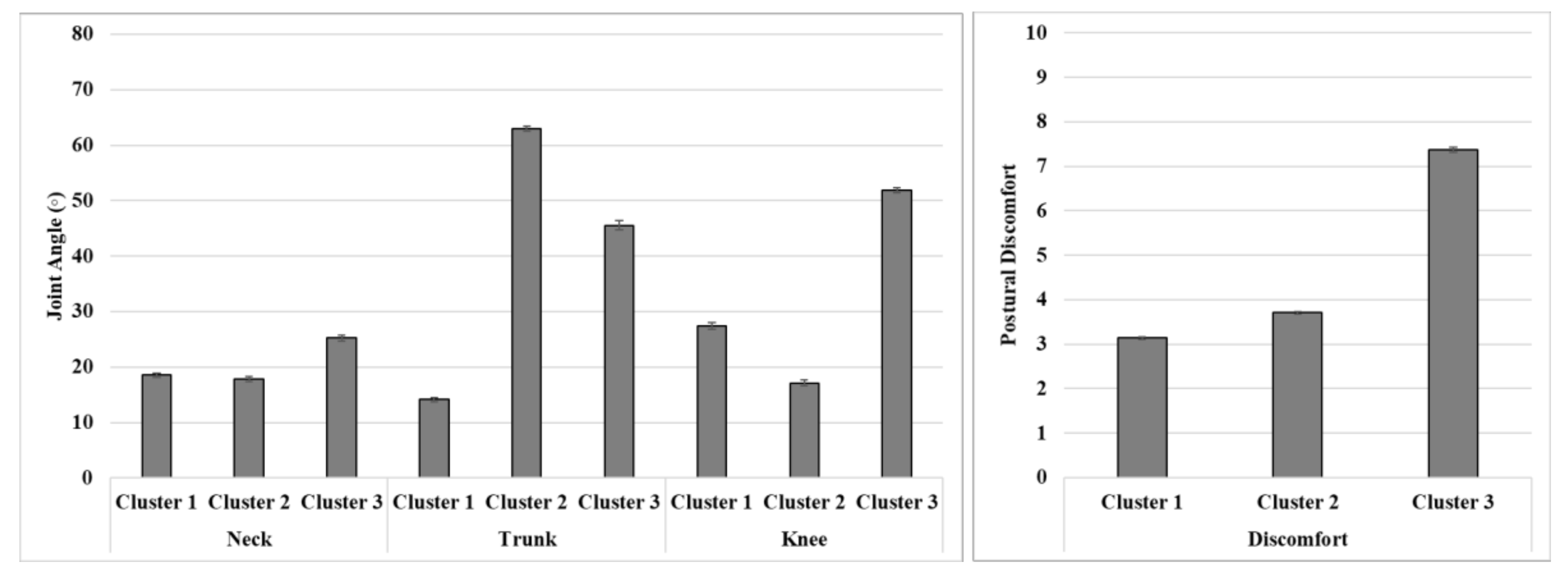
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Chung, M.K.; Lee, I.; Kee, D. Assessment of postural load for lower limb postures based on perceived discomfort. Int. J. Ind. Ergon. 2003, 31, 17–32. [Google Scholar]
- Hwang, J.; Kong, Y.-K.; Jung, M.-C. Posture evaluations of tethering and loose-housing systems in dairy farms. Appl. Ergon. 2010, 42, 1–8. [Google Scholar]
- Lim, C.-M.; Jung, M.-C.; Kong, Y.-K. Evaluation of upper-limb body postures based on the effects of back and shoulder flexion angles on subjective discomfort ratings, heart rates and muscle activities. Ergonomics 2011, 54, 849–857. [Google Scholar]
- Wang, H.; Hwang, J.; Lee, K.-S.; Kwag, J.-S.; Jang, J.-S.; Jung, M.-C. Upper Body and Finger Posture Evaluations at an Electric Iron Assembly Plant. Hum. Factors Ergon. Manuf. 2012, 24, 161–171. [Google Scholar]
- McAtamney, L.; Corlett, E.N. RULA: A survey method for the investigation of work-related upper limb disorders. Appl. Ergon. 1993, 24, 91–99. [Google Scholar]
- Hignett, S.; McAtamney, L. Rapid Entire Body Assessment (REBA). Appl. Ergon. 2000, 31, 201–205. [Google Scholar]
- Scott, G.B.; Lambe, N.R. Working practices in a perchery system, using the OVAKO Working posture Analysing System (OWAS). Appl. Ergon. 1996, 27, 281–284. [Google Scholar]
- Vink, P. Comfort and Design: Principles and Good Practice; CRC press: Boca Raton, FL, USA, 2004. [Google Scholar]
- Zhang, L.; Helander, M.G.; Drury, C.G. Identifying Factors of Comfort and Discomfort in Sitting. Hum. Factors J. Hum. Factors Ergon. Soc. 1996, 38, 377–389. [Google Scholar]
- Reenen, H.H.H.-V.; Van Der Beek, A.J.; Blatter, B.M.; Van Der Grinten, M.P.; Van Mechelen, W.; Bongers, P.M. Does musculoskeletal discomfort at work predict future musculoskeletal pain? Ergonomics 2008, 51, 637–648. [Google Scholar]
- Genaidy, A.; Barkawi, H.; Christensen, D. Ranking of static non-neutral postures around the joints of the upper extremity and the spine. Ergonomics 1995, 38, 1851–1858. [Google Scholar]
- Kee, D. Gender differences in rankings of joint motion stressfulness based on psychophysical scaling. Int. J. Ind. Ergon. 2005, 35, 461–469. [Google Scholar]
- Lin, C.-L.; Wang, M.-J.J.; Drury, C.G.; Chen, Y.-S. Evaluation of perceived discomfort in repetitive arm reaching and holding tasks. Int. J. Ind. Ergon. 2010, 40, 90–96. [Google Scholar]
- Mukhopadhyay, P.; Gallwey, T.J.; O’Sullivan, L.W. Effect of grip force and shoulder abduction angles in repetitive clockwise forearm pronation/supination movements. In Proceedings of the International Annual Occupational Ergonomics and Safety Conference, Toronto, ON, Canada, 3–12 June 2003; pp. 81–88. [Google Scholar]
- Hwang, J.; Shin, H.; Jung, M.-C. Joint motion pattern classification by cluster analysis of kinematic, demographic, and subjective variables. Appl. Ergon. 2013, 44, 636–642. [Google Scholar]
- Kyung, G.; Nussbaum, M.A.; Babski-Reeves, K. Enhancing digital driver models: Identification of distinct postural strategies used by drivers. Ergonomics 2010, 53, 375–384. [Google Scholar]
- Callaghan, J.P.; Coke, S.K.; Beach, T.A. Gender- and time-varying postural and discomfort responses during prolonged driving. Occup. Ergon. 2010, 9, 41–53. [Google Scholar]
- Chung, M.K.; Lee, I.; Kee, D. Quantitative postural load assessment for whole body manual tasks based on perceived discomfort. Ergonomics 2005, 48, 492–505. [Google Scholar]
- Kee, D.; Karwowski, W. LUBA: An assessment technique for postural loading on the upper body based on joint motion discomfort and maximum holding time. Appl. Ergon. 2001, 32, 357–366. [Google Scholar]
- Hwang, J.; Jung, M.-C. Age and sex differences in ranges of motion and motion patterns. Int. J. Occup. Saf. Ergon. 2015, 21, 173–186. [Google Scholar]
- Punnett, L.; Fine, L.J.; Keyserling, W.M.; Herrin, G.D.; Chaffin, D.B. Back disorders and nonneutral trunk postures of automobile assembly workers. Scand. J. Work. Environ. Health 1991, 17, 337–346. [Google Scholar]
- Keyserling, W.M.; Sudarsan, S.P.; Martin, B.J.; Haig, A.J.; Armstrong, T.J. Effects of low back disability status on lower back discomfort during sustained and cyclical trunk flexion. Ergonomics 2005, 48, 219–233. [Google Scholar]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Demographic Variable | Male | Female | Total |
|---|---|---|---|
| Number of participants | 42 | 53 | 95 |
| Age (years) | 24.5 (2.5) | 21.0 (2.9) | 22.5 (2.8) |
| Height (cm) | 176.5 (7.2) | 165.2 (5.9) | 170.8 (6.5) |
| Weight (kg) | 69.2 (8.5) | 55.1 (6.5) | 62.1 (8.1) |
| Posture Code | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 |
| Neck (°) | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Trunk (°) | 0 | 0 | 0 | 20 | 20 | 20 | 40 | 40 | 40 | 60 |
| Knee (°) | 0 | 30 | 60 | 0 | 30 | 60 | 0 | 30 | 60 | 0 |
| Posture Code | 11 | 12 | 13 | 14 | 15 | 16 | 17 | 18 | 19 | 20 |
| Neck (°) | 0 | 0 | 0 | 0 | 0 | 20 | 20 | 20 | 20 | 20 |
| Trunk (°) | 60 | 60 | 80 | 80 | 80 | 0 | 0 | 0 | 20 | 20 |
| Knee (°) | 30 | 60 | 0 | 30 | 60 | 0 | 30 | 60 | 0 | 30 |
| Posture Code | 21 | 22 | 23 | 24 | 25 | 26 | 27 | 28 | 29 | 30 |
| Neck (°) | 20 | 20 | 20 | 20 | 20 | 20 | 20 | 20 | 20 | 20 |
| Trunk (°) | 20 | 40 | 40 | 40 | 60 | 60 | 60 | 80 | 80 | 80 |
| Knee (°) | 60 | 0 | 30 | 60 | 0 | 30 | 60 | 0 | 30 | 60 |
| Posture Code | 31 | 32 | 33 | 34 | 35 | 36 | 37 | 38 | 39 | 40 |
| Neck (°) | 40 | 40 | 40 | 40 | 40 | 40 | 40 | 40 | 40 | 40 |
| Trunk (°) | 0 | 0 | 0 | 20 | 20 | 20 | 40 | 40 | 40 | 60 |
| Knee (°) | 0 | 30 | 60 | 0 | 30 | 60 | 0 | 30 | 60 | 0 |
| Posture Code | 41 | 42 | 43 | 44 | 45 | |||||
| Neck (°) | 40 | 40 | 40 | 40 | 40 | |||||
| Trunk (°) | 60 | 60 | 80 | 80 | 80 | |||||
| Knee (°) | 30 | 60 | 0 | 30 | 60 |
| Parameters | Cluster 1 | Cluster 2 | Cluster 3 |
| Number of observations | 1624 | 1553 | 1057 |
| Average distance from centroid | 1.8 | 1.8 | 1.9 |
| Maximum distance from centroid | 3.0 | 3.3 | 3.3 |
| Distance between Cluster Centroids | Cluster 1 | Cluster 2 | Cluster 3 |
| Cluster 1 | 0 | 1.8 | 2.5 |
| Cluster 2 | 1.8 | 0 | 2.3 |
| Cluster 3 | 2.5 | 2.3 | 0 |
| Gender | Variable | Cluster 1 | Cluster 2 | Cluster 3 | Total |
|---|---|---|---|---|---|
| Male | Number of observations | 545 | 632 | 676 | 1853 |
| Proportion (%) | 29.4 | 34.1 | 36.5 | 100 | |
| Female | Number of observations | 1079 | 921 | 381 | 2381 |
| Proportion (%) | 45.3 | 38.7 | 16.0 | 100 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hwang, J.; Lee, K.-S. Classification of Whole-Body Postural Discomfort Using Cluster Analysis. Int. J. Environ. Res. Public Health 2020, 17, 8314. https://doi.org/10.3390/ijerph17228314
Hwang J, Lee K-S. Classification of Whole-Body Postural Discomfort Using Cluster Analysis. International Journal of Environmental Research and Public Health. 2020; 17(22):8314. https://doi.org/10.3390/ijerph17228314
Chicago/Turabian StyleHwang, Jaejin, and Kyung-Sun Lee. 2020. "Classification of Whole-Body Postural Discomfort Using Cluster Analysis" International Journal of Environmental Research and Public Health 17, no. 22: 8314. https://doi.org/10.3390/ijerph17228314
APA StyleHwang, J., & Lee, K.-S. (2020). Classification of Whole-Body Postural Discomfort Using Cluster Analysis. International Journal of Environmental Research and Public Health, 17(22), 8314. https://doi.org/10.3390/ijerph17228314