Environmental and Psychosocial Interventions in Age-Friendly Communities and Active Ageing: A Systematic Review

 ,
,  ,
,  and
and 
Abstract
1. Introduction: Background and Current Situation
1.1. Active and Healthy Ageing and Age-Friendly Cities
1.2. Summarising Existing Knowledge Regarding Age-Friendly Cities and Communities
1.3. Approaches to Interventions
2. Material and Methods
2.1. Search Strategy: Data Sources and Search Criteria
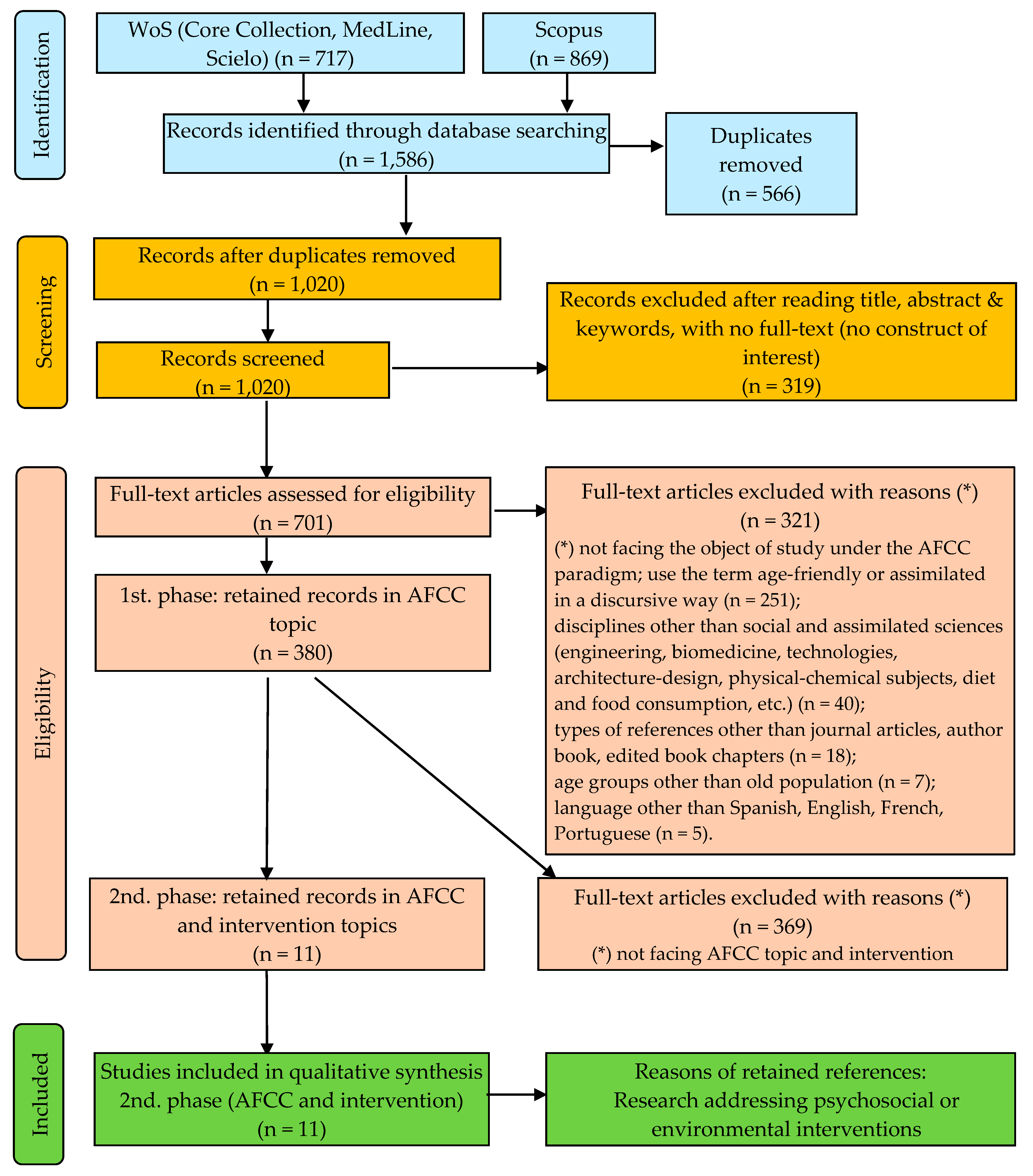
2.2. Study Selection and Quality Assessment
2.3. Eligibility Criteria
2.4. Data Collection and Risk of Bias
2.5. Summary Method
3. Results
3.1. Studies Included
3.2. Sample Characteristics
3.3. Intervention Characteristics
3.4. Strategies, Instruments and Measured Used
3.5. The Core Components and Elements of the Interventions
3.6. Effectiveness of Interventions
3.7. Dropout Rates
3.8. Type and Degree of Risk of Biased Results
3.9. Assessment of Methodological Quality
4. Discussion
4.1. Discussion: Study Characteristics
4.2. Discussion: Success of Interventions
4.3. Discussion: Study Quality
4.4. Limitations
5. Conclusions
5.1. Summary
5.2. Future Research Lines
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- United Nations (UN). The Vienna International Plan of Action on Aging Was Adopted by the World Assembly on Aging Held in Vienna, Austria from 26 July to 6 August 1982; United Nations: New York, NY, USA, 1982; p. 50. Available online: https://www.un.org/es/globalissues/ageing/docs/vipaa.pdf (accessed on 4 May 2019).
- United Nations (UN). Political Declaration and Madrid International Plan of Action on Ageing; United Nations: New York, NY, USA, 2002; p. 58. [Google Scholar]
- International Longevity Centre Brazil (ILC-BR). Active Ageing: A Policy Framework in Response to the Longevity Revolution; International Longevity Centre Brazil: Rio de Janeiro, Brazil, 2015; p. 116. Available online: http://ilcbrazil.org/portugues/wp-content/uploads/sites/4/2015/12/Active-Ageing-A-Policy-Framework-ILC-Brazil_web.pdf (accessed on 19 August 2016).
- World Health Organization (WHO). Decade of Healthy Ageing 2020–2030 (Zero Draft 12 June 2019); World Health Organization: Geneva, Switzerland, 2019; p. 27. Available online: https://tinyurl.com/yxkcxpd2 (accessed on 17 July 2019).
- World Health Organization (WHO). Global Age-Friendly Cities: A Guide; World Health Organization: Geneva, Switzerland, 2007; p. 82. [Google Scholar]
- World Health Organization (WHO). Global Strategy and Action Plan on Ageing and Health; WHO: Geneva, Switzerland, 2017; p. 46. [Google Scholar]
- World Health Organization (WHO). The Global Network for Age-Friendly Cities and Communities Looking Back over the Last Decade, Looking Forward to the Next; World Health Organization: Geneva, Switzerland, 2018; p. 35. Available online: https://apps.who.int/iris/bitstream/handle/10665/278981/WHO-FWC-ALC-18.4-spa.pdf?ua=1 (accessed on 9 August 2019).
- United Nations (UN). Transforming Our World: The 2030 Agenda for Sustainable Development (a/Res/70/1); United Nations: New York, NY, USA, 2015; p. 40. [Google Scholar]
- Economic Commission for Europe (ECE). Synthesis Report on the Implementation of the Madrid International Plan of Action on Ageing in the Ece Region between 2012 and 2017; Economic Commission for Europe, Working Group on Ageing: Lisbon, Portugal, 2017; pp. 1–91, ECE/AC.30/2017/Room document 1; Available online: https://tinyurl.com/y6s2y88j (accessed on 23 August 2020).
- Menec, V.; Brown, C. Facilitators and Barriers to Becoming Age-Friendly: A Review. J. Aging Soc. Policy 2018, 1–23. [Google Scholar] [CrossRef] [PubMed]
- De Oliveira, S.M.L.; Pessa, S.L.R.; Schenatto, F.J.; De Lourdes Bernartt, M. Cities and Population Aging: A Literature Review. In Congress of the International Ergonomics Association, Proceedings of the 20th Congress of the International Ergonomics Association (IEA; Florence, Italy, August 26-30, 2018). Volume VII: Ergonomics in Design, Design for All, Activity Theories for Work Analysis and Design, Affective Design, 2019; Bagnara, S., Tartaglia, R., Albolino, S., Alexander, T., Fujita, Y., Eds.; Springer International Publishing: Berlin/Heidelberg, Germany, 2019; pp. 1395–1404. [Google Scholar] [CrossRef]
- Fulmer, T.; Patel, P.; Levy, N.; Mate, K.; Berman, A.; Pelton, L.; Beard, J.; Kalache, A.; Auerbach, J. Moving toward a Global Age-Friendly Ecosystem. J. Am. Geriatr. Soc. 2020, 68, 1936–1940. [Google Scholar] [CrossRef] [PubMed]
- Torku, A.; Chan, A.P.C.; Yung, E.H.K. Age-Friendly Cities and Communities: A Review and Future Directions. Ageing Soc. 2019, 2, 1–38. [Google Scholar] [CrossRef]
- Huang, C.-Y.; Tsay, S.-F.; Lockwood, C.; Yang, B.-H.; Mu, P.-F. Policies That Promote Age-Friendly Cities and Enhance the Wellbeing of Inner City Dwelling Older Adults: A Systematic Review Protocol. JBI Database Syst. Rev. Implement. Rep. 2014, 12, 69–80. [Google Scholar] [CrossRef]
- Steels, S. Key Characteristics of Age-Friendly Cities and Communities: A Review. Cities 2015, 47, 45–52. [Google Scholar] [CrossRef]
- Neville, S.; Napier, S.; Adams, J.; Wham, C.; Jackson, D. An Integrative Review of the Factors Related to Building Age-Friendly Rural Communities. J. Clin. Nurs. 2016, 25, 2402–2412. [Google Scholar] [CrossRef]
- Lui, C.-W.; Everingham, J.-A.; Warburton, J.; Cuthill, M.; Bartlett, H. What Makes a Community Age-Friendly: A Review of International Literature. Australas. J. Ageing 2009, 28, 116–121. [Google Scholar] [CrossRef]
- Rogelj, V.; Bogataj, D. Social Infrastructure of Silver Economy: Literature Review and Research Agenda. IFAC-PapersOnLine 2019, 52, 2680–2685. [Google Scholar] [CrossRef]
- Buffel, T.; Rémillard-Boilard, S.; Phillipson, C. Social Isolation among Older People in Urban Areas. In A Review of the Literature for the Ambition for Ageing Programme in Greater Manchester; The University of Manchester; Institute for Collaborative Research Ageing: Manchester, UK, 2015; p. 31. Available online: https://tinyurl.com/y47dbozr (accessed on 9 September 2019).
- Syed, M.A.; McDonald, L.; Smirle, C.; Lau, K.; Mirza, R.M.; Hitzig, S.L. Social Isolation in Chinese Older Adults: Scoping Review for Age-Friendly Community Planning. Can. J. Aging-Rev. Can. Du Vieil. 2017, 36, 223–245. [Google Scholar] [CrossRef]
- Frochen, S.; Pynoos, J. Housing for the Elderly: Addressing Gaps in Knowledge through the Lens of Age-Friendly Communities. J. Hous. Elder. 2017, 31, 160–177. [Google Scholar] [CrossRef]
- Hwang, E. Impacts of Objective Neighborhood Built Environment on Older Adults’ Walking: Literature Review. Hous. Soc. 2017, 44, 141–155. [Google Scholar] [CrossRef]
- World Health Organization (WHO); Global Observatory for eHealth. Global Diffusion of Ehealth: Making Universal Health Coverage Achievable. Report of the Third Global Survey on Ehealth; World Health Organization: Geneva, Switzerland, 2016; p. 154. Available online: https://tinyurl.com/y2myqyd7 (accessed on 18 September 2020).
- Liaw, S.-T.; Ansari, S.; Jonnagaddala, J.; Narasimhan, P.; Ashraf, M.; Harris-Roxas, B.; Harris, M. A Systematic Review of the Use of Mobile Health to Promote Healthy Ageing and Support the Delivery of Age-Friendly Long-Term Healthcare Services. In Prospero, International Prospective Register of Systematic Reviews; Crd42017082383 Centre for Reviews and Dissemination, University of York: York, UK, 2017; Available online: https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42017082383 (accessed on 21 March 2020).
- Luciano, A.; Pascale, F.; Polverino, F.; Pooley, A. Measuring Age-Friendly Housing: A Framework. Sustainability 2020, 12, 848. [Google Scholar] [CrossRef]
- Ronzi, S.; Orton, L.; Pope, D.; Valtorta, N.K.; Bruce, N.G. What Is the Impact on Health and Wellbeing of Interventions That Foster Respect and Social Inclusion in Community-Residing Older Adults? A Systematic Review of Quantitative and Qualitative Studies. Syst. Rev. 2018, 7, 1–22. [Google Scholar] [CrossRef] [PubMed]
- Motealleh, P.; Moyle, W.; Jones, C.; Dupre, K. Creating a Dementia-Friendly Environment through the Use of Outdoor Natural Landscape Design Intervention in Long-Term Care Facilities: A Narrative Review. Health Place 2019, 58, 102148. [Google Scholar] [CrossRef]
- Neville, S.; Wright-St Clair, V.; Montayre, J.; Adams, J.; Larmer, P. Promoting Age-Friendly Communities: An Integrative Review of Inclusion for Older Immigrants. J. Cross-Cult. Gerontol. 2018, 33, 427–440. [Google Scholar] [CrossRef] [PubMed]
- Mihnovits, A.; Nisos, C.E. Measuring Healthy and Suitable Housing for Older People: A Review of International Indicators and Data Sets. Gerontechnology 2016, 15, 17–24. [Google Scholar] [CrossRef]
- Williams-Roberts, H.; Jeffery, B.; Johnson, S.; Muhajarine, N. The Effectiveness of Healthy Community Approaches on Positive Health Outcomes in Canada and the United States. Soc. Sci. 2016, 5, 3. [Google Scholar] [CrossRef]
- Dellamora, M.C.; Zecevic, A.A.; Baxter, D.; Cramp, A.; Fitzsimmons, D.; Kloseck, M. Review of Assessment Tools for Baseline and Follow-up Measurement of Age-Friendliness. Ageing Int. 2015, 40, 149–164. [Google Scholar] [CrossRef]
- Buckner, S.; Pope, D.; Mattocks, C.; Lafortune, L.; Dherani, M.; Bruce, N. Developing Age-Friendly Cities: An Evidence-Based Evaluation Tool. J. Popul. Ageing 2019, 12, 203–223. [Google Scholar] [CrossRef]
- Buffel, T.; McGarry, P.; Phillipson, C.; De Donder, L.; Dury, S.; De Witte, N.; Smetcoren, A.-S.; Verte, D. Developing Age-Friendly Cities: Case Studies from Brussels and Manchester and Implications for Policy and Practice. In Environmental Gerontology in Europe and Latin America: Policies and Perspectives on Environment and Aging; Sanchez Gonzalez, D., Rodriguez Rodriguez, V., Eds.; Springer: Berlin/Heidelberg, Germany, 2016; pp. 277–296. [Google Scholar] [CrossRef]
- Hernández Ruiz, B.; Valera i Pertegás, S. Psicología Social Aplicada e Intervención Psicosocial [Applied Social Psychology and Psychosocial Intervention]; Resma: Santa Cruz de Tenerife, Spain, 2001; p. 210. [Google Scholar]
- Clemson, L.; Mackenzie, L.; Ballinger, C.; Close, J.C.; Cumming, R.G. Environmental Interventions to Prevent Falls in Community-Dwelling Older People: A Meta-Analysis of Randomized Trials. J. Aging Health 2008, 20, 954–971. [Google Scholar] [CrossRef]
- Community Psychology: In Pursuit of Liberation and Well-Being; Nelson, G., Prilleltensky, I., Eds.; Palgrave Macmillan: New York, NY, USA, 2005. [Google Scholar]
- Intervención Psicosocial [Psychosocial Intervention]; Blanco, A., Rodríguez Marín, J., Eds.; Pearson Educación: Madrid, Spain, 2007; p. 606. [Google Scholar]
- Wahl, H.-W.; Weisman, G.D. Environmental Gerontology at the Beginning of the New Millennium: Reflections on Its Historical, Empirical, and Theoretical Development. Gerontologist 2003, 43, 616–627. [Google Scholar] [CrossRef] [PubMed]
- Lawton, M.P.; Nahemow, L. Ecology and the Aging Process. In The Psychology of Adult Development and Aging; American Psychological Association: Washington, DC, USA, 1973; pp. 619–674. [Google Scholar]
- Rodríguez-Rodríguez, V.; Sánchez-González, D. Approaches to Environmental Gerontology in the Mediterranean Europe and Latin America: Policy and Practice on Ageing and Place. In Environmental Gerontology in Europe and Latin America. Policies and Perspectives on Environment and Aging; Sánchez-González, D., Rodríguez-Rodríguez, V., Eds.; Col. International Perspectives on Aging; Springer: Berlin/Heidelberg, Germany, 2016; Volume 13, pp. 11–44. [Google Scholar] [CrossRef]
- Lawton, M.P. The Elderly in Context: Perspectives from Environmental Psychology and Gerontology. Environ. Behav. 1985, 17, 501–519. [Google Scholar] [CrossRef]
- Shigematsu, R.; Sallis, J.F.; Conway, T.L.; Saelens, B.E.; Frank, L.D.; Cain, K.L.; Chapman, J.E.; King, A.C. Age Differences in the Relation of Perceived Neighborhood Environment to Walking. Med. Sci. Sports Exerc. 2009, 41, 314–321. [Google Scholar] [CrossRef] [PubMed]
- Environmental Gerontology: Making Meaningful Places in Old Age; Rowles, G.D., Bernard, M.A., Eds.; Springer: Berlin/Heidelberg, Germany, 2013. [Google Scholar]
- Petrović, A.; Manley, D.; van Ham, M. Freedom from the Tyranny of Neighbourhood: Rethinking Sociospatial Context Effects. Prog. Hum. Geogr. 2020, 44, 1103–1123. [Google Scholar] [CrossRef]
- Smith, A.E. Ageing in Urban Neighbourhoods: Place Attachment and Social Exclusion; The Policy Press: Bristol, UK, 2009; p. 248. [Google Scholar]
- SánchezGonzález, D. Ambiente Físico-Social y Envejecimiento de la Población desde la Gerontología Ambiental y Geografía. Implicaciones Socioespaciales en América Latina [Physical-Social Environment and Ageing of the Population from Environmental Gerontology and Geography. Socio-spatial Implications in Latin America]. Rev. Geogr. Norte Gd. 2015, 97–114. [Google Scholar] [CrossRef]
- Pearce, S.; Rogers-Clark, C.; Doolan, J.M. A Comprehensive Systematic Review of Age-Friendly Nursing Interventions in the Management of Older People in Emergency Departments. JBI Evid. Synth. 2011, 9, 679–726. [Google Scholar] [CrossRef]
- Shamseer, L.; Moher, D.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A.; the PRISMA-P Group. Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols (Prisma-P) 2015: Elaboration and Explanation. BMJ 2015, 349, 1–25. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The Prisma Statement for Reporting Systematic Reviews and Meta-Analyses of Studies That Evaluate Healthcare Interventions: Explanation and Elaboration. PLoS Med. 2009, 6, e1000100. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; the PRISMA Group. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The Prisma Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- Chadegani, A.A.; Salehi, H.; Yunus, M.; Farhadi, H.; Fooladi, M.; Farhadi, M.; Ale Ebrahim, N. A Comparison between Two Main Academic Literature Collections: Web of Science and Scopus Databases. Asian Soc. Sci. 2013, 9, 18–26. [Google Scholar] [CrossRef]
- Zhu, J.; Liu, W. A Tale of Two Databases: The Use of Web of Science and Scopus in Academic Papers. Scientometrics 2020, 123, 321–335. [Google Scholar] [CrossRef]
- Joshi, A. Comparison between Scopus and Isi Web of Science. J. Glob. Values 2016, VII, 1–11. [Google Scholar]
- Harzing, A.-W.; Alakangas, S. Google Scholar, Scopus and the Web of Science: A Longitudinal and Cross-Disciplinary Comparison. Scientometrics 2016, 106, 787–804. [Google Scholar] [CrossRef]
- Martín-Martín, A.; Orduna-Malea, E.; Thelwall, M.; Delgado López-Cózar, E. Google Scholar, Web of Science, and Scopus: A Systematic Comparison of Citations in 252 Subject Categories. J. Informetr. 2018, 12, 1160–1177. [Google Scholar] [CrossRef]
- Clemson, L.; Stark, S.; Pighills, A.C.; Torgerson, D.J.; Sherrington, C.; Lamb, S.E. Environmental Interventions for Preventing Falls in Older People Living in the Community. Cochrane Database Syst. Rev. 2019, 2, CD013258. [Google Scholar] [CrossRef]
- Amador-Marin, B.; Guerra-Martin, M.D. Eficacia de las Intervenciones no Farmacológicas en la Calidad de Vida de las Personas Cuidadoras de Pacientes con Enfermedad De Alzheimer [Effectiveness of Non-Pharmacological Interventions in the Quality of Life of Caregivers of Alzheimer]. Gac. Sanit. 2017, 31, 154–160. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.C. The Cochrane Collaboration’s Tool for Assessing Risk of Bias in Randomised Trials. Br. Med. J. 2011, 343, d5928. [Google Scholar] [CrossRef]
- Stanulewicz, N.; Knox, E.; Narayanasamy, M.; Shivji, N.; Khunti, K.; Blake, H. Effectiveness of Lifestyle Health Promotion Interventions for Nurses: A Systematic Review. Int. J. Environ. Res. Public Health 2020, 17, 17. [Google Scholar] [CrossRef]
- Amoah, P.A.; Mok, K.H.; Wen, Z.; Li, L.W. Achieving the Age-Friendly City Agenda: An Interventional Study in Hong Kong’s Islands District. J. Asian Public Policy 2019, 1–20. [Google Scholar] [CrossRef]
- Atkins, M.T. Creating Age-Friendly Cities: Prioritizing Interventions with Q-Methodology. Int. Plan. Stud. 2019, 1–17. [Google Scholar] [CrossRef]
- Broome, K.; Worrall, L.; Fleming, J.; Boldy, D. Evaluation of Age-Friendly Guidelines for Public Buses. Transp. Res. Part A Policy Pract. 2013, 53, 68–80. [Google Scholar] [CrossRef]
- Gough, A.; Cassidy, K.L. Toward Psychosocial Health in Age-Friendly Communities: The Fountain of Health Peer-Led Education Series. Ment. Health Prev. 2017, 8, 14–19. [Google Scholar] [CrossRef]
- Jitramontree, N.; Chatchaisucha, S.; Thaweeboon, T.; Kutintara, B.; Intanasak, S. Action Research Development of a Fall Prevention Program for Thai Community-Dwelling Older Persons. Pac. Rim Int. J. Nurs. Res. 2015, 19, 69–79. [Google Scholar]
- Kam, P.K. Strengthening the Empowerment Approach in Social Work Practice: An Eps Model. J. Soc. Work 2020, 1–24. [Google Scholar] [CrossRef]
- Kuo, Y.-L.; Chen, I.J. Facilitating a Change Model in Age-Friendly Hospital Certification: Strategies and Effects. PLoS ONE 2019, 14, 1–14. [Google Scholar] [CrossRef]
- Lee, E.A.L.; Same, A.; McNamara, B.; Rosenwax, L. An Accessible and Affordable Transport Intervention for Older People Living in the Community. Home Health Care Manag. Pract. 2018, 30, 54–60. [Google Scholar] [CrossRef]
- Levert, M.-J.; Lefebvre, H.; Gelinas, I.; McKerall, M.; Roy, O.; Proulx, M. Expérience De Fréquentation Des Lieux Publics Par Des Personnes Âgées Ayant Subi Un Tcc En Présence D’un Accompagnateur-Citoyen: Projet Pilote. Can. J. Aging/La Revue Canadienne du Vieillissement 2016, 35, 229–241. [Google Scholar] [CrossRef]
- Pejner, M.N.; de Morais, W.O.; Lundstrom, J.; Laurell, H.; Skarsater, I. A Smart Home System for Information Sharing, Health Assessments, and Medication Self-Management for Older People: Protocol for a Mixed-Methods Study. JMIR Res. Protoc. 2019, 8, 1–9. [Google Scholar] [CrossRef]
- Thompson, C.W.; Curl, A.; Aspinall, P.; Alves, S.; Zuin, A. Do Changes to the Local Street Environment Alter Behaviour and Quality of Life of Older Adults? The ‘Diy Streets’ Intervention. Br. J. Sports Med. 2014, 48, 1–8. [Google Scholar] [CrossRef]
- Fernández-Mayoralas, G.; Rojo-Pérez, F.; Martínez-Martín, P.; Prieto-Flores, M.-E.; Rodríguez-Blázquez, C.; Martín-García, S.; Rojo-Abuín, J.-M.; Forjaz, M.-J. Active Ageing and Quality of Life: Factors Associated with Participation in Leisure Activities among Institutionalized Older Adults, with and without Dementia. Aging Ment. Health 2015, 19, 1031–1041. [Google Scholar] [CrossRef]
- del Barrio, E.; Marsillas, S.; Buffel, T.; Smetcoren, A.S.; Sancho, M. From Active Aging to Active Citizenship: The Role of (Age) Friendliness. Soc. Sci. 2018, 7, 134. [Google Scholar] [CrossRef]
- Rojo-Pérez, F.; Gallardo-Peralta, L.; Fernández-Mayoralas, G.; Rodríguez-Rodríguez, V.; Montes de Oca Zavala, V.; Prieto-Flores, M.E.; Lardiés Bosque, R. Envejecimiento Activo y Buen Envejecer en Iberoamérica. Una Revisión Bibliográfica [Active Aging and Ageing Well in Latin America. A Bibliographic Review]. In Envejecimiento Activo, Calidad de Vida y Género. Las Miradas Académica, Institucional y Social; Fernández-Mayoralas, G., Rojo-Pérez, F., Eds.; Tirant lo Blanch: Valencia, Spain, 2020. [Google Scholar]
- Rojo-Perez, F.; Fernández-Mayoralas, G.; Rodríguez-Rodríguez, V. Active Ageing and Quality of Life: A Literature Review. In Active Ageing and Quality of Later Life. From Concepts to Applications; Rojo-Perez, F., Fernandez-Mayoralas, G., Eds.; Series International Handbooks of Quality of Life; Springer: Berlin/Heidelberg, Germany, 2020. [Google Scholar]
- World Health Organization (WHO). World Report on Ageing and Health; World Health Organization: Geneva, Switzerland, 2015; p. 246. [Google Scholar]
- Kendig, H. Directions in Environmental Gerontology: A Multidisciplinary Field. Gerontologist 2003, 43, 611–615. [Google Scholar] [CrossRef]
- Hijas-Gómez, A.I.; Ayala, A.; Rodríguez-García, M.P.; Rodríguez-Blázquez, C.; Rodríguez-Rodríguez, V.; Rojo-Pérez, F.; Fernández-Mayoralas, G.; Rodríguez-Laso, A.; Calderón-Larrañaga, A.; Forjaz, M.J. The Who Active Ageing Pillars and Its Association with Survival: Findings from a Population-Based Study in Spain. Arch. Gerontol. Geriatr. 2020, 90, 1–15. [Google Scholar] [CrossRef]
- Envejecimiento Activo, Calidad de Vida y Género. Las Miradas Académica, Institucional y Social [Active Aging, Quality of Life and Gender. Academic, Institutional and Social Approaches]; Fernández-Mayoralas, G., Rojo-Pérez, F., Eds.; Tirant lo Blanch: Valencia, Spain, 2020. [Google Scholar]
- Cochrane Handbook for Systematic Reviews of Interventions (Version 5.1.0.) [Updated March 2011]; Higgins, J.P.T., Green, S., Eds.; The Cochrane Collaboration: Chichester, UK, 2011; p. 493. [Google Scholar]
- Buffel, T.; Phillipson, C. A Manifesto for the Age-Friendly Movement: Developing a New Urban Agenda. J. Aging Soc. Policy 2018, 30, 173–192. [Google Scholar] [CrossRef]
- Chaudhury, H.; Oswald, F. Advancing Understanding of Person-Environment Interaction in Later Life: One Step Further. J. Aging Stud. 2019, 51, 100821. [Google Scholar] [CrossRef]
- Grimshaw, J.; Campbell, M.; Eccles, M.; Steen, N. Experimental and Quasi-Experimental Designs for Evaluating Guideline Implementation Strategies. Fam. Pract. 2000, 17, S11–S18. [Google Scholar] [CrossRef]
- Golant, S.M. Aging in the Right Place; Health Professional Press: Baltimore, MD, USA, 2015. [Google Scholar]
- Wanka, A.; Moulaert, T.; Drilling, M. From Environmental Stress to Spatial Expulsion—Rethinking Concepts of Socio-Spatial Exclusion in Later Life. Int. J. Ageing Later Life 2018, 12, 25–51. [Google Scholar] [CrossRef]
- Rijnaard, M.D.; van Hoof, J.; Janssen, B.M.; Verbeek, H.; Pocornie, W.; Eijkelenboom, A.; Beerens, H.C.; Molony, S.L.; Wouters, E.J. The Factors Influencing the Sense of Home in Nursing Homes: A Systematic Review from the Perspective of Residents. J. Aging Res. 2016, 6143645, 1–16. [Google Scholar] [CrossRef]
- Sánchez González, D.; Chávez Alvarado, R. Ciudades Amigables para un Envejecimiento Activo: Aproximaciones Teóricas y Metodológicas [Age-Friendly Cities for an Active Aging: Theoretical and Methodological Approaches]. In Ciudades Amigables. Perspectivas, Políticas, Prácticas; Egea Jiménez, C., Sánchez González, D., Eds.; Comares: Granada, Spain, 2016; pp. 13–27. [Google Scholar]
- Erickson, L.D.; Call, V.R.; Brown, R.B. Sos-Satisfied or Stuck, Why Older Rural Residents Tay Put: Aging in Place or Stuck in Place in Rural Utah. Rural Sociol. 2012, 77, 408–434. [Google Scholar] [CrossRef]
- Scharlach, A.E.; Diaz-Moore, K. Aging in Place. In Handbook of Theories of Aging; Bengtson, V.L., Settersten, R.A., Jr., Eds.; Springer: Berlin/Heidelberg, Germany, 2016; pp. 407–425. [Google Scholar]
- Black, K.; Hyer, K. Generational Distinctions on the Importance of Age-Friendly Community Features by Older Age Groups. J. Appl. Gerontol. 2020, 39, 1025–1034. [Google Scholar] [CrossRef]
- Fernández-Mayoralas, G.; Schettini, R.; Sánchez-Román, M.; Rojo-Pérez, F.; Agulló, M.S.; Forjaz, M.J. El Papel del Género en el Buen Envejecer. Una Revisión Sistemática desde la Perspectiva Científica [The Role of Gender in Ageing Well. A Systematic Review from a Scientific Approach]. Prism. Soc. 2018, 21, 149–176. [Google Scholar]
- Kerr, J.; Norman, G.; Millstein, R.; Adams, M.A.; Morgan, C.; Langer, R.D.; Allison, M. Neighborhood Environment and Physical Activity among Older Women: Findings from the San Diego Cohort of the Women’s Health Initiative. J. Phys. Act. Health 2014, 11, 1070–1077. [Google Scholar] [CrossRef]
- Buffel, T.; Phillipson, C.; Rémillard-Boilard, S. Age-Friendly Cities and Communities: New Directions for Research and Policy. In Encyclopedia of Gerontology and Population Aging; Gu, D., Dupre, M.E., Eds.; Springer Nature Switzerland: Berlin/Heidelberg, Germany, 2019; pp. 1–10. [Google Scholar] [CrossRef]
- Sánchez González, D.; Chavez Alvarado, R. Envejecimiento de la Población y Cambio Climático. Vulnerabilidad y Resiliencia desde la Gerontología Ambiental [Ageing of and Climate Change. Vulnerability and Resilience from Environmental Gerontology]; Comares: Granada, Spain, 2019; p. 288. [Google Scholar]
- Wilson, D.M.; Marin, A.; Bhardwaj, P.; Lichlyter, B.; Thurston, A.; Mohankumar, D.A. Hope Intervention Compared to Friendly Visitors as a Technique to Reduce Depression among Older Nursing Home Residents. Nurs. Res. Pract. 2010, 676351. [Google Scholar] [CrossRef]
- Phillipson, C. Developing Age-Friendly Communities: New Approaches to Growing Old in Urban Environments. In Handbook of Sociology of Aging; Settersten, R.A., Angel, J.L., Eds.; Springer: Berlin/Heidelberg, Germany, 2011; pp. 279–293. [Google Scholar] [CrossRef]
- Moulaert, T.; Garon, S. Introduction: Toward a Better Understanding of Afcc. In Age-Friendly Cities and Communities in International Comparison: Political Lessons, Scientific Avenues, and Democratic Issues; Moulaert, T., Garon, S., Eds.; Springer: Berlin/Heidelberg, Germany, 2016; pp. 1–16. [Google Scholar] [CrossRef]
- Gonzales, E.; Morrow-Howell, N. Productive Engagement in Aging-Friendly Communities a Natural Intersection. Gener. J. Am. Soc. Aging 2009, 33, 51–58. [Google Scholar]
- Gardner, B.; Lally, P.; Wardle, J. Making Health Habitual: The Psychology of ‘Habit-Formation’ and General Practice. Br. J. Gen. Pract. 2012, 62, 664–666. [Google Scholar] [CrossRef]
- Walker, A. Why Involve Older People in Research? Age Ageing 2007, 36, 481–482. [Google Scholar] [CrossRef]
- Awa, W.L.; Plaumann, M.; Walter, U. Burnout Prevention: A Review of Intervention Programs. Patient Educ. Couns. 2010, 78, 184–190. [Google Scholar] [CrossRef]
- Home and Identity in Late Life: International Perspectives; Rowles, G.D., Chaudhury, H., Eds.; Springer: Berlin/Heidelberg, Germany, 2005. [Google Scholar]
- Barusch, A.S. Age-Friendly Cities: A Social Work Perspective. J. Gerontol. Soc. Work 2013, 56, 465–472. [Google Scholar] [CrossRef]
- Bindels, J.; Baur, V.; Cox, K.; Heijing, S.; Abma, T. Older People as Co-Researchers: A Collaborative Journey. Ageing Soc. 2014, 34, 951–973. [Google Scholar] [CrossRef]
- Moulaert, T.; Garon, S. Researchers Behind Policy Development: Comparing ‘Age-Friendly Cities’ Models in Quebec and Wallonia. J. Soc. Work Pract. 2015, 29, 23–35. [Google Scholar] [CrossRef]
- Øien, H.; Jakobsson, N.; Bonander, C. The Impact of Community-Based Interventions for the Older Population: A Quasi-Experimental Study of a Hip-Fracture Prevention Program in Norway. BMC Geriatr. 2018, 18, 311. [Google Scholar] [CrossRef] [PubMed]
- McClure, R.J.; Mack, K.; Wilkins, N.; Davey, T.M. Injury Prevention as Social Change. Inj. Prev. 2016, 22, 226–229. [Google Scholar] [CrossRef]
- Alidoust, S.; Bosman, C.; Holden, G.; Shearer, H.; Shutter, L. The Spatial Dimensions of Neighbourhood: How Older People Define It. J. Urban Des. 2017, 22, 547–567. [Google Scholar] [CrossRef]
- Sánchez-González, D. Environmental Context and the Spatial Experience of Ageing in the Place of Origin: The Case of Granada. Papeles de Población 2009, 15, 162–198. [Google Scholar]
- Scharlach, A.; Lehning, A. Creating Aging-Friendly Communitie; Oxford University Press: Oxford, UK, 2016; p. 289. [Google Scholar]
- Yeh, J.C. A Critical Analysis of Aging in Place and Age-Friendly Efforts. Innov. Aging 2017, 1 (Suppl. S1), 331. [Google Scholar] [CrossRef]
- Age-Friendly Cities and Communities. A Global Perspective; Buffel, T., Handler, S., Phillipson, C., Eds.; Policy Press, Series Ageing in a Global Context: Bristol, UK, 2018; p. 276. [Google Scholar]
- García-Valdez, M.T.; Sánchez-González, D.; Román-Pérez, R. Envejecimiento y Estrategias de Adaptación a los Entornos Urbanos desde la Gerontología Ambiental [Ageing and Adaptation Strategies to Urban Environments from Environmental Gerontology]. Estudios Demográficos y Urbanos 2019, 34, 101–128. [Google Scholar] [CrossRef]
- Greenfield, E.A. Getting started: An empirically derived logic model for age-friendly community initiatives in the early planning phase. J. Gerontol. Soc. Work 2018, 61, 295–312. [Google Scholar] [CrossRef] [PubMed]
- Seah, B.; Kowitlawakul, Y.; Jiang, Y.; Ang, E.; Chokkanathan, S.; Wang, W. A review on healthy ageing interventions addressing physical, mental and social health of independent community-dwelling older adults. Geriatr. Nurs. 2019, 40, 37–50. [Google Scholar] [CrossRef]
- Sánchez-González, D.; Egea-Jiménez, C. Outdoor Green Spaces and Active Ageing from the Perspective of Environmental Gerontology. In Active Ageing and Quality of Later Life. From Concepts to Applications; Rojo-Perez, F., Fernandez-Mayoralas, G., Eds.; Series International Handbooks of Quality of Life; Springer: Berlin/Heidelberg, Germany, 2020. [Google Scholar] [CrossRef]
- Glicksman, A.; Ring, L. Defining the goals of age-friendly interventions. J. Hous. Elder. 2017, 31, 93–98. [Google Scholar] [CrossRef]
- The Measurement and Valuation of Health Status Using Eq-5d: A European Perspective: Evidence from the Euroqol Bio Med Research Programme; Brooks, R., Rabin, R., De Charro, F., Eds.; Kluwer Academic Publishers: Dordrecht, The Netherlands, 2003; p. 299. [Google Scholar]
- Hyde, M.; Wiggins, R.D.; Higgs, P.; Blane, D.B. A Measure of Quality of Life in Early Old Age: The Theory, Development and Properties of a Needs Satisfaction Model (CASP-19). Aging Ment. Health 2003, 7, 186–194. [Google Scholar] [CrossRef]
- Iwarsson, S.; Slaug, B.; Fänge, A.M. The Housing Enabler Screening Tool: Feasibility and Interrater Agreement in a Real Estate Company Practice Context. J. Appl. Gerontol. 2012, 31, 641–660. [Google Scholar] [CrossRef]
- Reuben, D.B.; Lee, M.; Davis, J.W.; Eslami, M.S.; Osterweil, D.G.; Melchiore, S.; Weintraub, N.T. Development and Validation of a Geriatrics Attitudes Scale for Primary Care Residents. J. Am. Geriatr. Soc. 1998, 46, 1425–1430. [Google Scholar] [CrossRef] [PubMed]
- Sugiyama, T.; Thompson, C.W. Older People’s Health, Outdoor Activity and Supportiveness of Neighbourhood Environments. Landsc. Urban Plan. 2007, 83, 168–175. [Google Scholar] [CrossRef]
- Thiamwong, L.; Thamarpirat, J.; Maneesriwongul, W.; Jitapunkul, S. Thai Falls Risk Assessment Test (Thai-Frat) Developed for Community-Dwelling Thai Elderly. J. Med. Assoc. Thail. 2008, 91, 1823–1831. [Google Scholar]
- Penney, L. The Uncertain Bodies and Spaces of Aging in Place. Anthropol. Aging Q. 2013, 34, 113–125. [Google Scholar] [CrossRef][Green Version]
- Plouffe, L.; Kalache, A.; Voelcker, I. A Critical Review of the Who Age-Friendly Cities Methodology and Its Implementation. In Age-Friendly Cities and Communities in International Comparison: Political Lessons, Scientific Avenues, and Democratic Issues; Moulaert, T., Garon, S., Eds.; Springer: Berlin/Heidelberg, Germany, 2016; pp. 19–36. [Google Scholar] [CrossRef]
- Ronzi, S.; Pope, D.; Orton, L.; Bruce, N. Using Photovoice Methods to Explore Older People’s Perceptions of Respect Crossmark and Social Inclusion in Cities: Opportunities, Challenges and Solutions. SSM-Popul. Health 2016, 2, 732–744. [Google Scholar] [CrossRef]
- Fukuoka, Y.; Gay, C.; Haskell, W.; Arai, S.; Vittinghoff, E. Identifying Factors Associated with Dropout During Prerandomization Run-in Period from an Mhealth Physical Activity Education Study: The mPED Trial. JMIR mHealth uHealth 2015, 3, e34. [Google Scholar] [CrossRef]
- Garon, S.; Paris, M.; Beaulieu, M.; Veil, A.; Laliberte, A. Collaborative Partnership in Age-Friendly Cities: Two Case Studies from Quebec, Canada. J. Aging Soc. Policy 2014, 26, 73–87. [Google Scholar] [CrossRef]
- Koohsari, M.J.; Mavoa, S.; Villanueva, K.; Sugiyama, T.; Badland, H.; Kaczynski, A.T.; Owen, N.; Giles-Corti, B. Public Open Space, Physical Activity, Urban Design and Public Health: Concepts, Methods and Research Agenda. Health Place 2015, 33 (Suppl. SC), 75–82. [Google Scholar] [CrossRef]
- Noordzij, J.M.; Beenackers, M.A.; Roux, A.V.D.; van Lenthe, F.J. Age-Friendly Cities: Challenges for Future Research. Bull. World Health Organ. 2019, 97, 436–437. [Google Scholar] [CrossRef]
- International Perspectives on Age-Friendly Cities; Caro, F.G., Fitzgerald, K.G., Eds.; Routledge: New York, NY, USA; London, UK, 2015; p. 286. [Google Scholar]
- Menec, V.H.; Hutton, L.; Newall, N.; Nowicki, S.; Spina, J.; Veselyuk, D. How ‘Age-Friendly’ Are Rural Communities and What Community Characteristics Are Related to Age-Friendliness? The Case of Rural Manitoba, Canada. Ageing Soc. 2015, 35, 203–223. [Google Scholar] [CrossRef]
- United Nations Development Programme (UNDP). Sustainable Development Goals; UNDP—United Nations Development Programme: New York, NY, USA, 2019; p. 20. Available online: https://www.undp.org/content/undp/en/home/sustainable-development-goals.html (accessed on 24 January 2020).
- United Nations Economic Commission for Europe (UNECE), Working Group on Ageing. Ageing in Sustainable and Smart Cities. Policy Briefs 2020, 24, 1–21. [Google Scholar]


{kind=link}
| Search in the Web of Science (databases: Core collection; MedLine; Scielo) |
| ((TS = ((Friendl* near (age or ages or aged or aging or ageing or elderly) near (city or cities or communit* or environment* or neighb* or rural or urban*)) or (aged-friend* or age-friend* or ageing-friend* or aging-friend* or elderly-friend*)) and py = 2007–2020)) Refined by: DOCUMENT TYPES (Article OR Review OR Book) AND LANGUAGE (English OR Portuguese OR French OR Spanish) |
| Search in Scopus |
| TITLE-ABS-KEY ((aged-friend* OR age-friend* OR ageing-friend* OR aging-friend* OR elderly-friend*) OR (friendl* W/15 (age OR ages OR aged OR aging OR ageing OR elderly) W/15 (city OR cities OR communit* OR environment* OR neighb* OR rural OR urban*))) AND PUBYEAR > 2006 AND (LIMIT-TO (DOCTYPE, “ar”) OR LIMIT-TO (DOCTYPE, “ch”) OR LIMIT-TO (DOCTYPE, “re”) OR LIMIT-TO (DOCTYPE, “bk”)) AND (LIMIT-TO (LANGUAGE, “English”) OR LIMIT-TO (LANGUAGE, “French”) OR LIMIT-TO (LANGUAGE, “Spanish”) OR LIMIT-TO (LANGUAGE, “Portuguese”)) |
| ID. | Authors and Year | Objectives | Geographical Context and Length | Design and Approaches | Participants | Interventions | Instruments and Measures | Effectiveness |
|---|---|---|---|---|---|---|---|---|
| [60] | Amoah et al., 2019 | To study how conscious and collaborative interventions affect the older persons’ perception of age-friendliness of various AFC domains and the implications for health-related well-being over time | Urban (Hong Kong’s Islands District) 17 months | NC AFCC | NI: 946 PA: ≥50 MA: 71.4% W: 78.1% Randomness: NR | TY: Environmental AP: Risk reduction; environmental adaptations ST: Prevention; management Domain: H; T; OS; CS; SP; RS; CP; IC FI: Individually based | Quantitative methods: pre- and post-intervention study M: self-rated health (Likert scale) DA: Binary logistic regression | HE: with no improvement in self-rated health BE: more participation DE: improvement in 5 domains of AFCC TEE: short term |
| [61] | Atkins, 2019 | To examine how stakeholders (government, peak bodies and the not-for-profit sectors) prioritize age-friendly communities through interventions to improve older people’s well-being | Metropolitan (metropolitan area of Perth, Australia) 2 months | NC AFCC | NI: 117 NG: 23 PA: n/d MA: n/d %W: n/d Randomness: NR | TY: Environmental AP: Risk reduction ST: Prevention Domain: H; T; OS; CS; SP; RS; CP; IC FI: Group format | Quantitative and qualitative methods: Q methodology; semi-structured interviews; focus groups M: n/d DA: Factor analysis | HE: n/d BE: more social participation among older adults DE: ease of use of transport TEE: short term |
| [62] | Broome et al., 2013 | To evaluate the impact of implementing age-friendly guidelines for public buses on bus use, usability and social participation for older persons | Urban (Hervey Bay and North of Brisbane, Queensland, Australia) 24 months | NRC AFCC | N: 335 NI: 100 (users and non-users) PA: ≥60 MA: 72.4 % W:78.9% Randomness: NR | TY: Environmental AP: Risk reduction; socials. ST: Prevention; management Domain: T FI: Individually based | Quantitative methods: pre- and post-intervention study; data were compared with nominal group technique data collected from a previous study M: Social Activities Participation (based on the Social Activities Checklist: SOCACT: frequency and satisfaction scale) DA: Multinomial logistic regression | HE: n/d BE: the frequency of use of transport for older adults Does not increaseDE: improvement the ease of use of transportation TEE: short term |
| [63] | Gough and Cassidy, 2017 | In the context of the Fountain of Health Initiative for Optimal Ageing, related to the AFCC, this paper aimed at assessing the effectiveness of the peer-led educational groups to promote health knowledge and behaviours at the community level | Urban areas (Halifax Regional Municipality) and rural areas (Annapolis Valley, Nova Scotia), Canada 6 weeks (90 min per series) | NRCr AFCC through the Fountain of Health Initiative for Optimal Ageing areas, related to AFCC | Ni: 51 PA: ≥50 MA: n/d %W: 75.3% Randomness: NR | TY: Multicomponent AP: Information and education ST: Management Domain: SP; RS FI: Group format | Quantitative and qualitative methods: pre- and post-intervention study; peer-led education series M: Self-perception of aging based on the Attitudes Towards Own Aging subscale. DA: Chi squared; paired samples t-test. | HE: n/d BE: improvement attitudes towards ageing DE: more social participation TEE: short term |
| [64] | Jitramontree et al., 2015 | To develop and implement a Multifactorial Age-friendly Fall Prevention program (MAFPP) among older people living in the community | Intraurban (west of Bangkok, Thailand) Several months (no specification) | NC AFCC Through the Multifactorial Age-friendly Fall Prevention Program (MAFPP) | NI: 50 NF: 20 NP: 10 PA: ≥60 MA: n/d %W: n/d Randomness: NR | TY: Multicomponent AP: Risk reduction; support groups. ST: Prevention; management Domain: H; CP FI: Group format | Qualitative methods: focus groups and in-depth interviews M: Thai Fall Risk Assessment Test (Thai-FRAT) DA: thematic analysis | HE: improvement in the prevention of falls BE: better communication DE: decrease environmental risk in housing TEE: short term |
| [65] | Kam, 2020 | Evaluate the effectiveness of the EPS (Empowerment, Participation and Strengths) intervention model in older users of the public transport system | Intraurban (Hong Kong districts) Several months (no specification) | NC AFCCthrough the EPS principles (Empowerment, Participation and Strength) | N: 1683 NI: 30 PA: ≥60 MA: n/d %W: n/d Randomness: NR | TY: Psychosocial AP: Socials ST: Prevention Domain: T FI: Group format | Quantitative and qualitative methods: survey; focus groups; observational study through site visits; M: structured questionnaireDA: n/d | HE: n/d BE: user satisfaction; empowerment DE: transport service adaptation improvements TEE: short term |
| [66] | Kuo and Chen, 2019 | Under the assumption of the knowledge and attitudes of employees toward ageing are important for successful of Age-Friendly Hospital (AFH), this observational study aimed at examining the certification process of an AFH using John Kotter’s change model and evaluating the changes in employees’ knowledge of ageing and their attitudes towards the elderly | Building (the Cardinal Tien Hospital, Taipei, Taiwan, as a teaching hospital) 8 months | RCr AFCC based on the Age-Friendly Hospital certification process | N: 336 Ni: 163 PA: ≥20 MA: 39.2 %W: n/d Randomness: R | TY: Psychosocial AP: Training ST: Management Domain: CS; RS FI: Individually based and Group format | Quantitative and qualitative methods: self-administered online questionnaire pre- and post-intervention; observational study M: Facts on Ageing Quiz (FAQ1) scale assess physical, psychological and social factors; the Geriatric Attitudes Scale (GAS); change evaluation through SWOT analysis DA: Paired samples t-test. | HE: n/d BE: positive effect of employees’ attitude towards ageing DE: improvements in health service SO: improvements in organization and management TEE: short term |
| [67] | Lee et al., 2018 | To evaluate the impact of a community transport intervention on the independence and well-being of older people living in an urban community | Urban (Perth, Australia) 4 months | NC AFCC | NI: 32 (functional disability, no cognitive impairment) PA: ≥65 MA: n/d %W: 75% Randomness: n/d | TY: Environmental AP: Risk reduction; environmental adaptations ST: Prevention Domain: T FI: Individually based | Longitudinal analysis based on quantitative and qualitative methods: pre- and post-intervention interviews, in-depth interviews M: The Personal Component of the Housing Enabler (Functional Limitations and Dependence on Mobility devices) DA: descriptive analyses. Qualitative analysis through NVivo software | HE: no health improvements BE: improves independence and the perception of safety at exits. No communications improvements DE: relative effectiveness of the transport service adaptation improvements TEE: short term |
| [68] | Levert et al., 2016 | This observational analysis aimed at adapting, implementing and evaluating an intervention based on personalized citizen support (Citizen Intervention in Community Living project) for older people with traumatic brain injury (TBI), in order to know the facilitators or the barriers in their use of public spaces in the residential environment. | Intraurban (Montreal, Canadá) 20 h | RCr AFCC | NI: 3 PA: ≥65 MA: 85.3 %W: 66.6% Randomness: R | TY: Multicomponent AP: Risk reduction; socials ST: Prevention Domain: H; T; SP; RS FI: Individually based | Qualitative methods: direct observational study with inductive approach through site visits M: fieldwork script DA: Thematic and cross-sectional analysis | HE: n/d BE: proactive behaviour in exits; preventive social support DE: social participation improvement TEE: short term |
| [69] | Pejner et al., 2019 | To develop and evaluate healthcare technologies through designing, developing and evaluating an age-friendly smart home that uses smart technologies to collect and compile health-related evidence in order to support decision making and communication regarding medication self-managing among older people | Urban (municipalities of Halmstad and Hylte, Halland, Sweden) 3 months (3 h per session) | NRCr AFCC through the Intelligent Age-Friendly Home (IAFH) | NI: 10 participants with polypharmacy and home care NF: 10 NP: 10 PA: ≥65 MA: n/d %W: 69% Randomness: NR | TY: Multicomponent AP: Risk reduction; environmental adaptations; incorporation of assistive technology; training ST: Prevention; management Domain: CS FI: Individually based and group format | Quantitative and qualitative methods: survey; focus groups; participatory design. Several phases: conceptualization of the system; development; pilot study; full-scale intervention M: Morisky Medication Adherence Scale; Personal Well-being Index-Adult; Satisfaction with Life Scale; Serenity Scale DA: n/d | HE: relative effectiveness of adherence to medication BE: relative effectiveness due to an unwilling attitude to the use of assistive technology DE: relative effectiveness of technological systems in the home TEE: short term |
| [70] | Thompson et al., 2014 | To evaluate the effects of residential streets improvements for the support of physical activity and well-being among older adults | Intraurban in locations of England, Wales and Scotland 30 months | NRC AFCC | N: 96 NI: 56 (residents); 40 (non-residents) PA: ≥65 MA: 75.2 %W: 60.4% Randomness: NR | TY: Multicomponent AP: Risk reduction; environmental adaptations; socials ST: Prevention; Management Domain: OS FI: Individually based | Quantitative methods: pre- and post-intervention surveys; Accelerometry. M: general health (EQ-5D) scale; quality of life (CASP-19); frequency of outdoor visits (walking, recreational walking, gardening, outdoor sports, other outdoor activities); Instrumental Activities of Daily Living (IADL); neighbourhood open space (NOS) scale AD: Paired samples t-test; factor analysis; hierarchical blocked linear regressions; non-parametric tests (Mann–Whitney U or Kruskal–Wallis) | HE: no health improvements BE: no improvements in activity participation DE: street safety perception improvement TEE: medium term (between 3 and 6 months) |
| Type of Effectiveness | Significant Changes Reported in the Studies | Success Rate of Interventions | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Environmental Intervention | Psychosocial Intervention | Multicomponent | Total | |||||||||
| Author/Year | N | Studies | SR | Studies | SR | Studies | SR | |||||
| N | N | % | N | N | % | N | N | % | % | |||
| Improvement of risk factors for health | Amoah et al., 2019; Atkins, 2019; Gough and Cassidy, 2017; Jitramontree et al., 2015; Lee et al., 2018; Pejner et al., 2019; Thompson et al., 2014 | 7 | 3 | 1 | 33.3 | 0 | 0 | 0.0 | 4 | 2 | 50.0 | 42.8 |
| Positive behavioural lifestyle changes | Amoah et al., 2019; Atkins, 2019; Broome et al., 2013; Gough and Cassidy, 2017; Jitramontree et al., 2015; Kam, 2020; Lee et al., 2018; Levert et al., 2016; Pejner et al., 2019; Thompson et al., 2014 | 10 | 4 | 3 | 75.0 | 0 | 0 | 0.0 | 5 | 3 | 60.0 | 70.0 |
| Changes in organizational results | Kuo and Chen, 2019 | 1 | 0 | 0 | 0.0 | 1 | 1 | 100.0 | 0 | 0 | 0.0 | 100.0 |
| Changes in the results of the Age-Friendly Cities and Communities domains | Amoah et al., 2019; Atkins, 2019; Broome et al., 2013; Gough and Cassidy, 2017; Jitramontree et al., 2015; Kam, 2020; Kuo and Chen, 2019; Lee et al., 2018; Levert et al., 2016; Pejner et al., 2019; Thompson et al., 2014 | 11 | 4 | 2 | 50.0 | 2 | 2 | 100.0 | 5 | 4 | 80.0 | 72.7 |
| ID | Authors/Year | Design | Dropout Rates (%) | Risk of Bias | ||||
|---|---|---|---|---|---|---|---|---|
| Absence of Randomness | Insufficient Information Regarding Participant Characteristics | Insufficient Information Regarding the Instruments and Measures Implemented | Insufficient Information Regarding Results Associated Intervention Effectiveness | Total | ||||
| (Degree) | (Degree) | (Degree) | (Degree) | (Degree) | ||||
| [60] | Amoah et al., 2019 | NC | n/d | High | Low | Moderated | Moderated | Moderated |
| [61] | Atkins, 2019 | NC | n/d | High | High | High | High | High |
| [62] | Broome et al., 2013 | NRC | n/d | High | Moderated | Low | Moderated | Moderated |
| [63] | Gough and Cassidy, 2017 | NRCr | 52.9 | High | Moderated | Moderated | High | High-Moderated |
| [64] | Jitramontree et al., 2015 | NC | n/d | High | High | High | High | High |
| [65] | Kam, 2020 | NC | n/d | Moderated | High | High | High | High-moderated |
| [66] | Kuo and Chen, 2019 | RCr | 51.5 | Low | Moderated | Low | Moderated | Low-Moderated |
| [67] | Lee et al., 2018 | NC | 34.4 | High | High | Moderated | Moderated | High-Moderated |
| [68] | Levert et al., 2016 | RCr | 0.0 | Moderated | Low | High | High | High-moderated |
| [69] | Pejner et al., 2019 | NRCr | n/d | High | Low | High | High | High-moderated |
| [70] | Thompson et al., 2014 | NRC | 53.2 | Moderated | Low | Low | Low | Low |
| Total | High | Moderated | Moderated-High | High | High-Moderated | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sánchez-González, D.; Rojo-Pérez, F.; Rodríguez-Rodríguez, V.; Fernández-Mayoralas, G. Environmental and Psychosocial Interventions in Age-Friendly Communities and Active Ageing: A Systematic Review. Int. J. Environ. Res. Public Health 2020, 17, 8305. https://doi.org/10.3390/ijerph17228305
Sánchez-González D, Rojo-Pérez F, Rodríguez-Rodríguez V, Fernández-Mayoralas G. Environmental and Psychosocial Interventions in Age-Friendly Communities and Active Ageing: A Systematic Review. International Journal of Environmental Research and Public Health. 2020; 17(22):8305. https://doi.org/10.3390/ijerph17228305
Chicago/Turabian StyleSánchez-González, Diego, Fermina Rojo-Pérez, Vicente Rodríguez-Rodríguez, and Gloria Fernández-Mayoralas. 2020. "Environmental and Psychosocial Interventions in Age-Friendly Communities and Active Ageing: A Systematic Review" International Journal of Environmental Research and Public Health 17, no. 22: 8305. https://doi.org/10.3390/ijerph17228305
APA StyleSánchez-González, D., Rojo-Pérez, F., Rodríguez-Rodríguez, V., & Fernández-Mayoralas, G. (2020). Environmental and Psychosocial Interventions in Age-Friendly Communities and Active Ageing: A Systematic Review. International Journal of Environmental Research and Public Health, 17(22), 8305. https://doi.org/10.3390/ijerph17228305