Guidelines for Pregnancy Management During the COVID-19 Pandemic: A Public Health Conundrum


Abstract
1. Introduction
2. Materials and Methods
2.1. Team
2.2. Guidelines
2.3. Domains
2.4. The Process: From Conceptualization to Analysis
3. Results
3.1. Timeliness
3.2. Accessibility
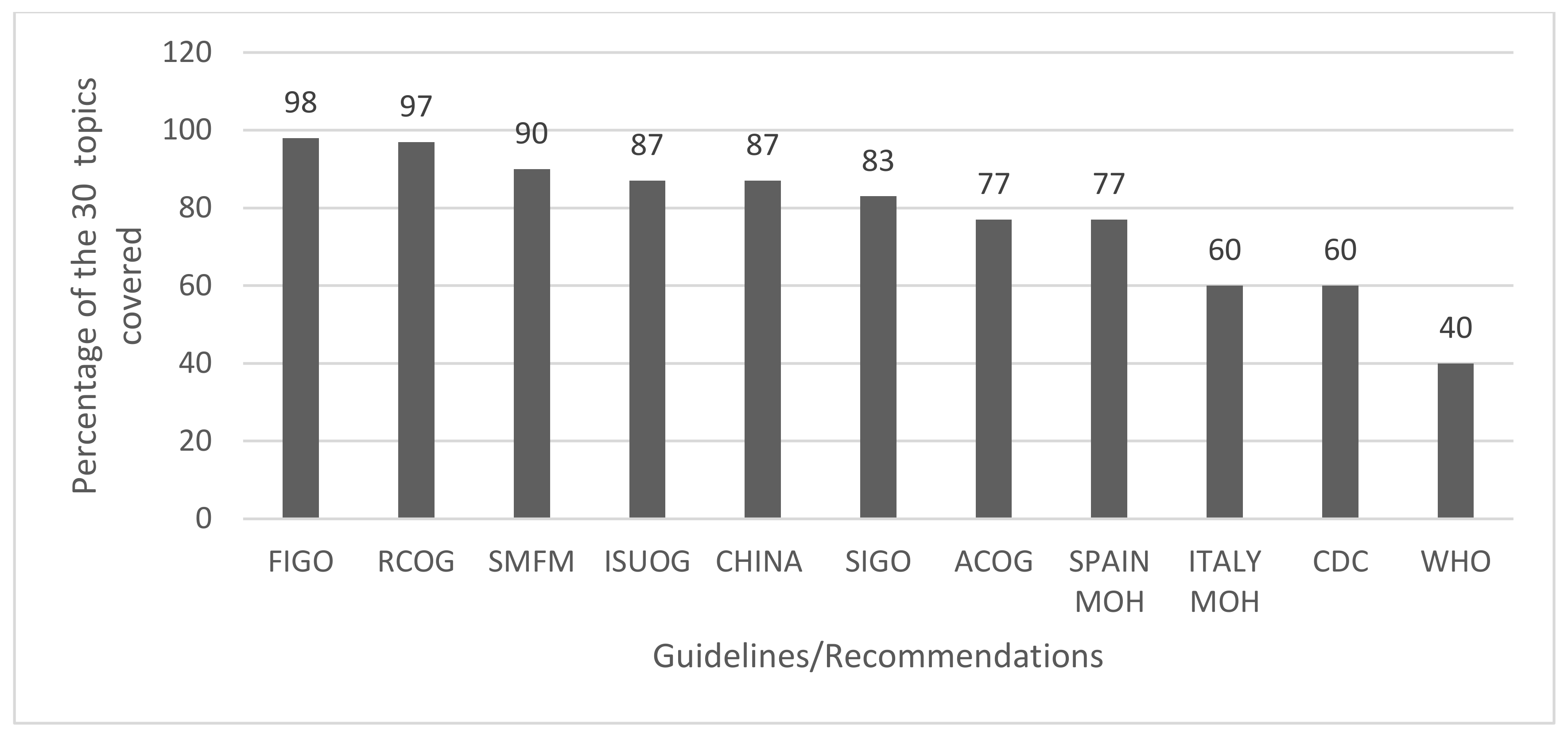
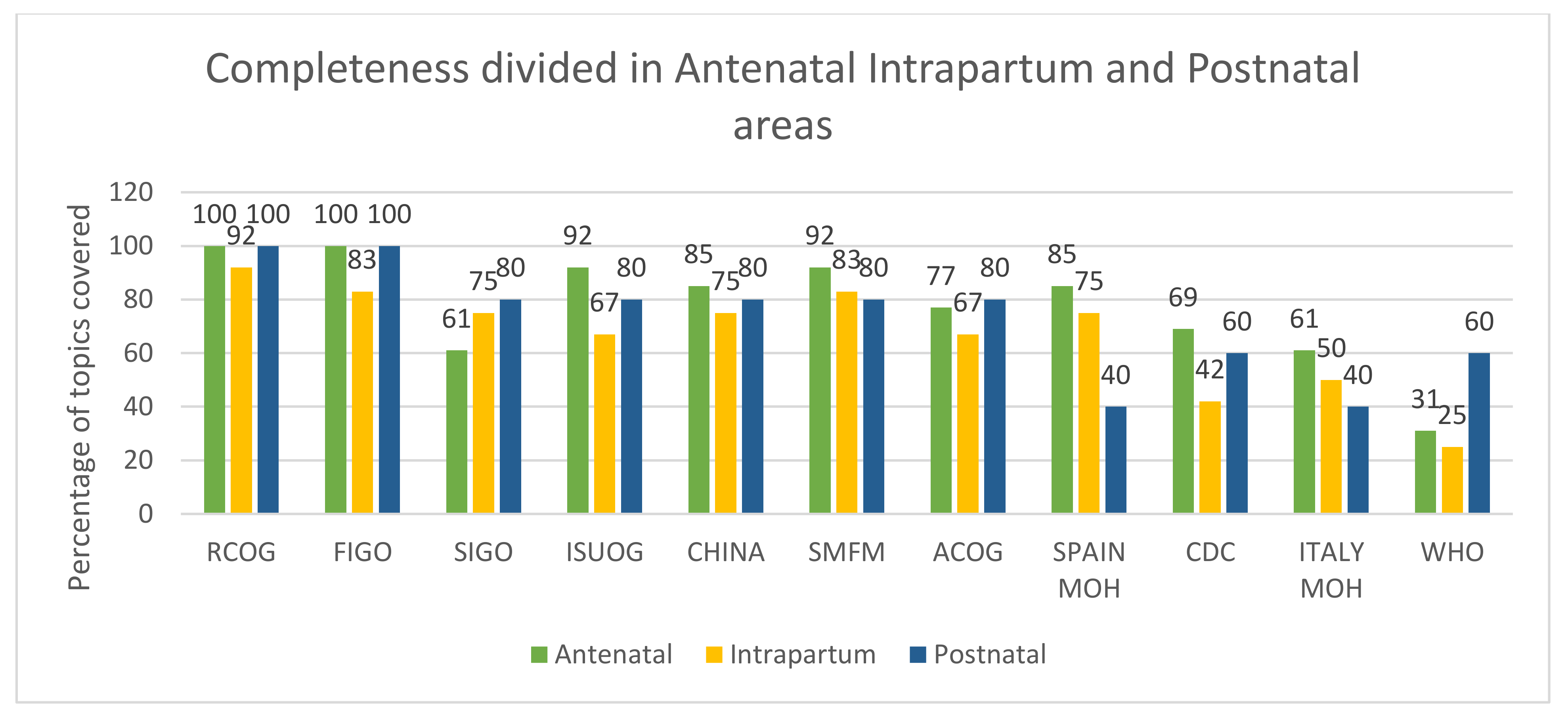
3.3. Completeness
3.4. Consistency
3.4.1. Antenatal Care
3.4.2. Intrapartum Care
3.4.3. Postnatal/Postpartum Care
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Su, S.; Wong, G.; Shi, W.; Liu, J.; Lai, A.C.; Zhou, J.; Liu, W.; Bi, Y.; Gao, G.F. Epidemiology, Genetic Recombination, and Pathogenesis of Coronaviruses. Trends Microbiol. 2016, 24, 490–502. [Google Scholar] [CrossRef] [PubMed]
- WORLDOMETER. COVID-19 CORONAVIRUS PANDEMIC. 2020. Available online: https://www.worldometers.info/coronavirus/ (accessed on 16 April 2020).
- WHO. Summary of Probable SARS Cases with Onset of Illness from 1 November 2002 to 31 July 2003. 2020. Available online: https://www.who.int/publications/m/item/summary-of-probable-sars-cases-with-onset-of-illness-from-1-november-2002-to-31-july-2003 (accessed on 16 April 2020).
- WHO. Coronavirus Disease 2019 (COVID-19) Situation Report. 2020. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/situation-reports (accessed on 17 April 2020).
- Zhao, X.; Jiang, Y.; Zhao, Y.; Xi, H.; Liu, C.; Qu, F.; Feng, X. Analysis of the susceptibility to COVID-19 in pregnancy and recommendations on potential drug screening. Eur. J. Clin. Microbiol. Infect. Dis. 2020, 39, 1209–1220. [Google Scholar] [CrossRef] [PubMed]
- Di Mascio, D.; Khalil, A.; Saccone, G.; Rizzo, G.; Buca, D.; Liberati, M.; Vecchiet, J.; Nappi, L.; Scambia, G.; Berghella, V.; et al. Outcome of coronavirus spectrum infections (SARS, MERS, COVID-19) during pregnancy: A systematic review and meta-analysis. Am. J. Obstet. Gynecol. MFM 2020, 2, 100107. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.; Guo, L.; Chen, L.; Liu, W.; Cao, Y.; Zhang, J.; Feng, L. A case report of neonatal COVID-19 infection in China. Clin. Infect. Dis. 2020, 71, 853–857. [Google Scholar] [CrossRef] [PubMed]
- Zeng, H.; Xu, C.; Fan, J.; Tang, Y.; Deng, Q.; Zhang, W.; Long, X. Antibodies in Infants Born to Mothers With COVID-19 Pneumonia. JAMA 2020, 323, 1848–1849. [Google Scholar] [CrossRef] [PubMed]
- Prochaska, E.; Jang, M.; Burd, I. COVID-19 in pregnancy: Placental and neonatal involvement. Am. J. Reprod. Immunol. 2020, 84, e13306. [Google Scholar] [CrossRef] [PubMed]
- Baud, D.; Greub, G.; Favre, G.; Gengler, C.; Jaton, K.; Dubruc, E.; Pomar, L. Second-Trimester Miscarriage in a Pregnant Woman With SARS-CoV-2 Infection. JAMA 2020, 323, 2198–2200. [Google Scholar] [CrossRef] [PubMed]
- Juusela, A.; Nazir, M.; Gimovsky, M. Two cases of coronavirus 2019–related cardiomyopathy in pregnancy. Am. J. Obstet. Gynecol. MFM 2020, 2, 100113. [Google Scholar] [CrossRef] [PubMed]
- Zaigham, M.; Andersson, O. Maternal and perinatal outcomes with COVID-19: A systematic review of 108 pregnancies. Acta Obstet. Gynecol. Scand. 2020, 99, 823–829. [Google Scholar] [CrossRef] [PubMed]
- Della Gatta, A.N.; Rizzo, R.; Pilu, G.; Simonazzi, G. Coronavirus Disease 2019 during pregnancy: A systematic review of reported cases. Am. J. Obstet. Gynecol. 2020, 223, 36–41. [Google Scholar] [CrossRef] [PubMed]
- Airicerca. AIRICERCA. Available online: http://airicerca.org/ (accessed on 9 May 2020).
- Airicerca. Airiclip. 2020. Available online: https://informa.airicerca.org/it/category/airiclip/ (accessed on 9 May 2020).
- OGGETTO: COVID-19: Indicazioni per Gravida-Partoriente, Puerpera, Neonato e Allattamento. 2020. Available online: http://www.salute.gov.it/portale/news/p3_2_1_1_1.jsp?lingua=italiano&menu=notizie&p=dalministero&id=4376 (accessed on 10 May 2020).
- Health, Spanish. Ministry of Manejo de la Mujer Embarazada y el Recién Nacido con COVID-19. 2020. Available online: https://www.mscbs.gob.es/profesionales/saludPublica/ccayes/alertasActual/nCov-China/documentos/Documento_manejo_embarazo_recien_nacido.pdf (accessed on 16 April 2020).
- SIGO. La Gravidanza al Tempo del Coronavirus; Societa’ Italiana di Ginecologia ed Ostetricia. 2020. Available online: https://www.sigo.it/wp-content/uploads/2020/04/SIGO-AOGOI_Coronavirus-donne.pdf (accessed on 4 April 2020).
- SMFM. Coronavirus (COVID-19) and Pregnancy: What Maternal-Fetal Medicine Subspecialists Need to Know; SMFM: Washington, DC, USA, 2020. [Google Scholar]
- Chen, D.; Yang, H.; Cao, Y.; Cheng, W.; Duan, T.; Fan, C.; Fan, S.; Feng, L.; Gao, Y.; He, F.; et al. Expert consensus for managing pregnant women and neonates born to mothers with suspected or confirmed novel coronavirus (COVID-19) infection. Int. J. Gynecol. Obstet. 2020, 149, 130–136. [Google Scholar] [CrossRef] [PubMed]
- RCOG. Coronavirus (COVID-19) Infection in Pregnancy. 2020. Available online: https://www.rcog.org.uk/globalassets/documents/guidelines/2020-04-09-coronavirus-covid-19-infection-in-pregnancy.pdf (accessed on 9 April 2020).
- Poon, L.C.; Yang, H.; Kapur, A.; Melamed, N.; Dao, B.; Divakar, H.; McIntyre, H.D.; Kihara, A.B.; Ayres-De-Campos, D.; Ferrazzi, E.M.; et al. Global interim guidance on coronavirus disease 2019 (COVID-19) during pregnancy and puerperium from FIGO and allied partners: Information for healthcare professionals. Int. J. Gynecol. Obstet. 2020, 149, 273–286. [Google Scholar] [CrossRef] [PubMed]
- ACOG. Novel Coronavirus 2019 (COVID-19)—Practice Advisory. 2020. Available online: https://www.acog.org/clinical/clinical-guidance/practice-advisory/articles/2020/03/novel-coronavirus-2019 (accessed on 16 April 2020).
- Poon, L.C.; Yang, H.; Lee, J.C.S.; Copel, J.A.; Leung, T.Y.; Zhang, Y.; Chen, D.; Prefumo, F. ISUOG Interim Guidance on 2019 novel coronavirus infection during pregnancy and puerperium: Information for healthcare professionals. Ultrasound Obstet. Gynecol. 2020, 55, 700–708. [Google Scholar] [CrossRef] [PubMed]
- WHO. Q&A on COVID-19 and Pregnancy and Childbirth. 2020. Available online: https://www.who.int/news-room/q-a-detail/coronavirus-disease-covid-19-pregnancy-and-childbirth (accessed on 16 April 2020).
- CDC. Considerations for Inpatient Obstetric Healthcare Settings. 2020. Available online: https://www.cdc.gov/coronavirus/2019-ncov/hcp/inpatient-obstetric-healthcare-guidance.html (accessed on 16 April 2020).
- Rabi, D.M.; Kunneman, M.; Montori, V.M. When Guidelines Recommend Shared Decision-making. JAMA 2020, 323, 1345. [Google Scholar] [CrossRef] [PubMed]
- Rosenfeld, R.M.; Shiffman, R.N.; Robertson, P. Department of Otolaryngology State University of New York Downstate. Clinical Practice Guideline Development Manual, Third Edition: A quality-driven approach for translating evidence into action. Otolaryngol. Head Neck Surg. 2013, 148 (Suppl. 1), S1–S55. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Releasing Institution | Country | Release Format | Type of Edition | Publication Title | Publication Date (dd/mm) | Last Update (dd/mm) | Number of Updated Versions | Accessibility (N of Clicks) | Number of Topics Covered | Metalinks for Additional Information | No. of References (If Described) |
|---|---|---|---|---|---|---|---|---|---|---|---|
| RCOG | UK | WEBPAGE | GUIDELINES | Coronavirus (COVID-19) Infection in Pregnancy | 09/03 | 09/04 | 7 | 2 | 29/30 | 60 | 45 |
| ISUOG | N.A. | WEBPAGE | INTERIM GUIDANCE | ISUOG Interim Guidance on 2019 novel coronavirus infection during pregnancy and puerperium: information for healthcare professionals | 11/03 | - | - | 2 | 26/30 | 0 | 64 |
| ACOG | USA | WEBPAGE | PRACTICE ADVICE | Outpatient Assessment and Management for Pregnant Women with Suspected or Confirmed Novel Coronavirus (COVID-19) | 13/03 | 10/04 | 1 | 1 | 23/30 | 15 | 1 |
| CDC | WEBPAGE | PRACTICE ADVICE | Considerations for Inpatient Obstetric Healthcare Settings | 17/03 | 06/04 | 1 | 1 | 18/30 | 76 | ||
| SMFM | WEBPAGE | COMMENTARY | Coronavirus (COVID-19) and Pregnancy: What Maternal–Fetal Medicine Subspecialists Need to Know | 17/03 | 11/04 | 1 | 3 | 27/30 | 18 | ||
| Spanish Ministry of Health | SPAIN | WEBPAGE | GUIDELINES | Management of pregnant women and newborns with COVID-19 | 17/03 | - | - | 2 | 23/30 | 2 | 31 |
| WHO | N.A. | WEBPAGE | QUESTIONS AND ANSWERS | Q & A on COVID-19, pregnancy, childbirth and breastfeeding | 18/03 | - | - | 1 | 12/30 | 3 | 0 |
| Chinese Expert Consensus | China | WEBPAGE | EXPERT CONSENSUS | Expert consensus for managing pregnant women and neonates born to mothers with suspected or confirmed novel Coronavirus (COVID-19) infection | 20/03 | - | - | 1 | 26/30 | 0 | 44 |
| Italian Ministry of Health | ITALY | WEBPAGE | COMMUNICATION | COVID-19: guidance for pregnancy, labour, newborns and breastfeeding | 31/03 | - | - | 7 | 18/30 | n.a. | n.a. |
| SIGO/AOGOI | POSTER | Pregnancy at the time of Coronavirus | 04/04 | n.a. | 25/30 | 0 | n.a. | ||||
| FIGO | N.A. | WEBPAGE | INTERIM GUIDANCE | Global interim guidance on coronavirus disease 2019 (COVID-19) during pregnancy and puerperium | 04/04 | - | - | 3 | 29/30 | 0 | 72 |
| Topics | General Recommendations and Antenatal Care | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| RCOG | ISUOG | ACOG | SMFM | CDC | Spain MoH | WHO | Chinese Expert Consensus | MoH Italy | SIGO/AOGOI | FIGO | |
| Personal hygiene | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ |
| Social Hygiene (mask) | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ |
| Symptoms | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ |
| Organization of the visits | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ |
| Partner/visitors | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | |||
| Triage point | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ||||
| IPC | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | |
| Organization of the place of care | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | |||
| Diagnostic (imaging) | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | |||
| Treatment | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | |||
| Fetal monitoring | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ||||
| Mental health | ✓ | ✓ | ✓ | ✓ | |||||||
| Telehealth | ✓ | ✓ | ✓ | ✓ | ✓ | ||||||
| Intrapartum Care | |||||||||||
| IPC | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ |
| Delivery ward organization | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ||
| Partner | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | |||||
| Biohazardous material | ✓ | ✓ | ✓ | ✓ | |||||||
| Transportation | ✓ | ✓ | |||||||||
| Corticosteroids | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | |||
| Timing of delivery | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ |
| Mode of delivery | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ |
| Analgesia | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | |
| Management of labor and fetal monitoring | ✓ | ✓ | ✓ | ✓ | |||||||
| Cord clamping | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ||
| MgS04, anticoagulants | ✓ | ✓ | ✓ | ||||||||
| Postnatal Care | |||||||||||
| Mother/child separation | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ |
| Breastfeeding | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ |
| Breast pump | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | |||
| IPC | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ |
| Postpartum visits | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | |||
| Family planning | |||||||||||
| Topics | RCOG | ISUOG | CHINA | SPAIN MOH | AOGOI/SIGO/Italian MOH | ACOG/CDC/SMFM | FIGO | WHO |
| ANTENATAL CARE | ||||||||
| Mask Wearing | Pregnant women screened positive for SARS-CoV-2 infection | Apply local guidance | Apply local guidance | Women with acute respiratory symptoms | Pregnant women screened positive for SARS-CoV-2 infection | Women who test positive/PUI women at all times as clinically able * | People visiting a hospital or other high-risk area | NR |
| Personal/social Hygiene | Especially >28 weeks of gestation, distance of at least two meters between individuals | Distance of at least one meter between individuals | Reduce social interactions | Reduce social interactions | Distance of at least one meter between individuals | Reduce social interactions | Distance of at least two meters or six feet between individuals | Reduce social interactions |
| Antenatal visits | Delay visits until the end of self-confinement period | Postpone routine follow-up appointments by 14 days or until positive/two consecutive negative test results | NR | NR | When possible postpone visits, by taking note into the clinical file. | NR | Offer all visits for obstetric emergencies **/postpone routine follow-up appointments by 14 days or until positive/two consecutive negative test results | Guarantee to all pregnant women, including those with confirmed/suspected COVID-19, high quality of care before, during, and after childbirth (including mental health care) |
| Partner/companion | Come alone to the visits or with one person maximum | Consider reducing the number of visitors to the department | Consider reducing the number of visitors to the department. | Come alone to the visits or with one person maximum | Positive partner: notify your obstetric team: access forbidden | Consider reducing the number of visitors to the department *** | Come alone to the visits | NR |
| RCOG | ISUOG | CHINA | SPAIN MOH | AOGOI/SIGO/Italian MOH | ACOG/CDC/SMFM | FIGO | WHO | |
| INTRAPARTUM CARE | ||||||||
| Antenatal Corticosteroids | - Steroids for standard care - Do not delay urgent intervention to allow steroid administration | - Avoid steroids in critical patients - Discuss steroids administration with MDC - Avoid tocolysis | Steroids to all viable premature fetuses | - Steroids administration on individual basis - Discuss steroids administration with MTD | NR | - Steroids administration on individual basis - Particular caution for critically ill women in ICU setting | - Avoid steroids in critical patients - Discuss steroids administration with MDC - Avoid tocolysis | NR |
| Respiratory Analgesia | Entonox allowed (with disposable filter) | NR | NR | Respiratory analgesia is not recommended | NR | Consider suspending use of nitrous oxide | NR | NR |
| Cord Clamping | Delayed cord clamping recommended | Prompt cord clamping | Delayed cord-clamping not recommended for women infected with COVID-19 | Delayed clamping allowed if maternal and newborn isolation can be done properly | Prompt cord clamping | NR | Prompt cord clamping | NR |
| Skin to skin practice | NR | NR | NR | Skin to skin is allowed if maternal and newborn isolation can be done properly | Avoid skin to skin | NR | NR | Skin to skin is allowed |
| RCOG | ISUOG | CHINA | SPAIN MOH | AOGOI/SIGO/Italian MOH | ACOG/CDC/SMFM | FIGO | WHO | |
| POSTPARTUM CARE | ||||||||
| Mother/child separation | Healthy babies stay with their mothers | Separation for severely/critically ill mothers | Infants isolated and monitored for 14 days | Separation based on maternal test and symptoms | Separation based on maternal test and symptoms | Separation based on maternal test, symptoms, and willingness. | Separation for severely/critically ill mothers | Women should be supported to share a room with their baby |
| Breastfeeding | The benefits outweigh any potential risks of transmission of the virus | Can be considered for asymptomatic/mildly affected patients **** | Avoid direct breastfeeding | Allowed depending on maternal clinical state symptoms | Allowed **** /*** | Pumping recommended for SARS-CoV-2 positive/PUI women **** | Can be considered for asymptomatic/mildly affected patients **** | Women can breastfeed safely **/**** |
| RCOG | ISUOG | CHINA | SPAIN MOH | AOGOI/SIGO/Italian MOH | ACOG/CDC/SMFM | FIGO | WHO | |
| ANTENATAL CARE | ||||||||
| Mask Wearing | Pregnant women screened positive for SARS-CoV-2 infection | Apply local guidance | Apply local guidance | Women with acute respiratory symptoms | Pregnant women screened positive for SARS-CoV-2 infection | Women who test positive/PUI women at all times as clinically able * | People visiting a hospital or other high-risk area | NR |
| Personal/social Hygiene | Especially > 28 weeks of gestation, distance of at least two meters between individuals | Distance of at least one meter between individuals | Reduce social interactions | Reduce social interactions | Distance of at least one meter between individuals | Reduce social interactions | Distance of at least two meters or six feet between individuals | Reduce social interactions |
| Antenatal visits | Delay visits until the end of self-confinement period | Postpone routine follow-up appointments by 14 days or until positive/two consecutive negative test results | NR | NR | When possible postpone visits by taking note into the clinical file. | NR | Offer all visits for obstetric emergencies **/postpone routine follow-up appointments by 14 days or until positive/two consecutive negative test results | Guarantee to all pregnant women, including those with confirmed/suspected COVID-19, high quality of care before, during and after childbirth |
| Partner/companion | Come alone to the visits or with one person maximum | Consider reducing the number of visitors to the department | Consider reducing the number of visitors to the department. | Come alone to the visits or with one person maximum | Positive partner: notify your obstetric team: access forbidden | Consider reducing the number of visitors to the department *** | Come alone to the visits | NR |
| RCOG | ISUOG | CHINA | SPAIN MOH | AOGOI/SIGO/Italian MOH | ACOG/CDC/SMFM | FIGO | WHO | |
| INTRAPARTUM CARE | ||||||||
| Antenatal Corticosteroids | - Steroids for standard care - Do not delay urgent intervention to allow steroid administration | - Avoid steroids in critical patients - Discuss steroids administration with MDC - Avoid tocolysis | Steroids to all viable premature fetuses | - Steroids administration on individual basis - Discuss steroids administration with MTD | NR | - Steroids administration on individual basis - Particular caution for critically ill women in ICU setting | - Avoid steroids in critical patients - Discuss steroids administration with MDC - Avoid tocolysis | NR |
| Respiratory Analgesia | Entonox allowed (with disposable filter) | NR | NR | Respiratory analgesia is not recommended | NR | Consider suspending use of nitrous oxide | NR | NR |
| Cord Clamping | Delayed cord clamping recommended | Prompt cord clamping | Delayed cord clamping not recommended for women infected with COVID-19 | Delayed clamping allowed if maternal and newborn isolation can be done properly | Prompt cord clamping | NR | Prompt cord clamping | NR |
| Skin to skin practice | NR | NR | NR | Skin to skin is allowed if maternal and newborn isolation can be done properly | Avoid skin to skin | NR | NR | Skin to skin is allowed |
| RCOG | ISUOG | CHINA | SPAIN MOH | AOGOI/SIGO/Italian MOH | ACOG/CDC/SMFM | FIGO | WHO | |
| POSTPARTUM CARE | ||||||||
| Mother/child separation | Healthy babies stay with their mothers | Separation for severely/critically ill mothers | Infants isolated and monitored for 14 days | Separation based on maternal test and symptoms | Separation based on maternal test and symptoms | Separation based on maternal test, symptoms, and willingness | Separation for severely/critically ill mothers | Women should be supported to share a room with their baby |
| Breastfeeding | The benefits outweigh any potential risks of transmission of the virus | Can be considered for asymptomatic/mildly affected patients **** | Avoid direct breastfeeding | Allowed depending on maternal clinical state symptoms | Allowed ****/***** | Pumping recommended for SARS-CoV-2 positive/PUI women **** | Can be considered for asymptomatic/mildly affected patients **** | Women can breastfeed safely ****/****** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Benski, C.; Di Filippo, D.; Taraschi, G.; Reich, M.R. Guidelines for Pregnancy Management During the COVID-19 Pandemic: A Public Health Conundrum. Int. J. Environ. Res. Public Health 2020, 17, 8277. https://doi.org/10.3390/ijerph17218277
Benski C, Di Filippo D, Taraschi G, Reich MR. Guidelines for Pregnancy Management During the COVID-19 Pandemic: A Public Health Conundrum. International Journal of Environmental Research and Public Health. 2020; 17(21):8277. https://doi.org/10.3390/ijerph17218277
Chicago/Turabian StyleBenski, Caroline, Daria Di Filippo, Gianmarco Taraschi, and Michael R. Reich. 2020. "Guidelines for Pregnancy Management During the COVID-19 Pandemic: A Public Health Conundrum" International Journal of Environmental Research and Public Health 17, no. 21: 8277. https://doi.org/10.3390/ijerph17218277
APA StyleBenski, C., Di Filippo, D., Taraschi, G., & Reich, M. R. (2020). Guidelines for Pregnancy Management During the COVID-19 Pandemic: A Public Health Conundrum. International Journal of Environmental Research and Public Health, 17(21), 8277. https://doi.org/10.3390/ijerph17218277