Maitjara Wangkanyi: Insights from an Ethnographic Study of Food Practices of Households in Remote Australian Aboriginal Communities


 , , and
, , and
Abstract
1. Introduction
Study Conceptualization and Aims
- What food and drinks Anangu families are eating; and
- Factors that influence these food choices.
2. Materials and Methods
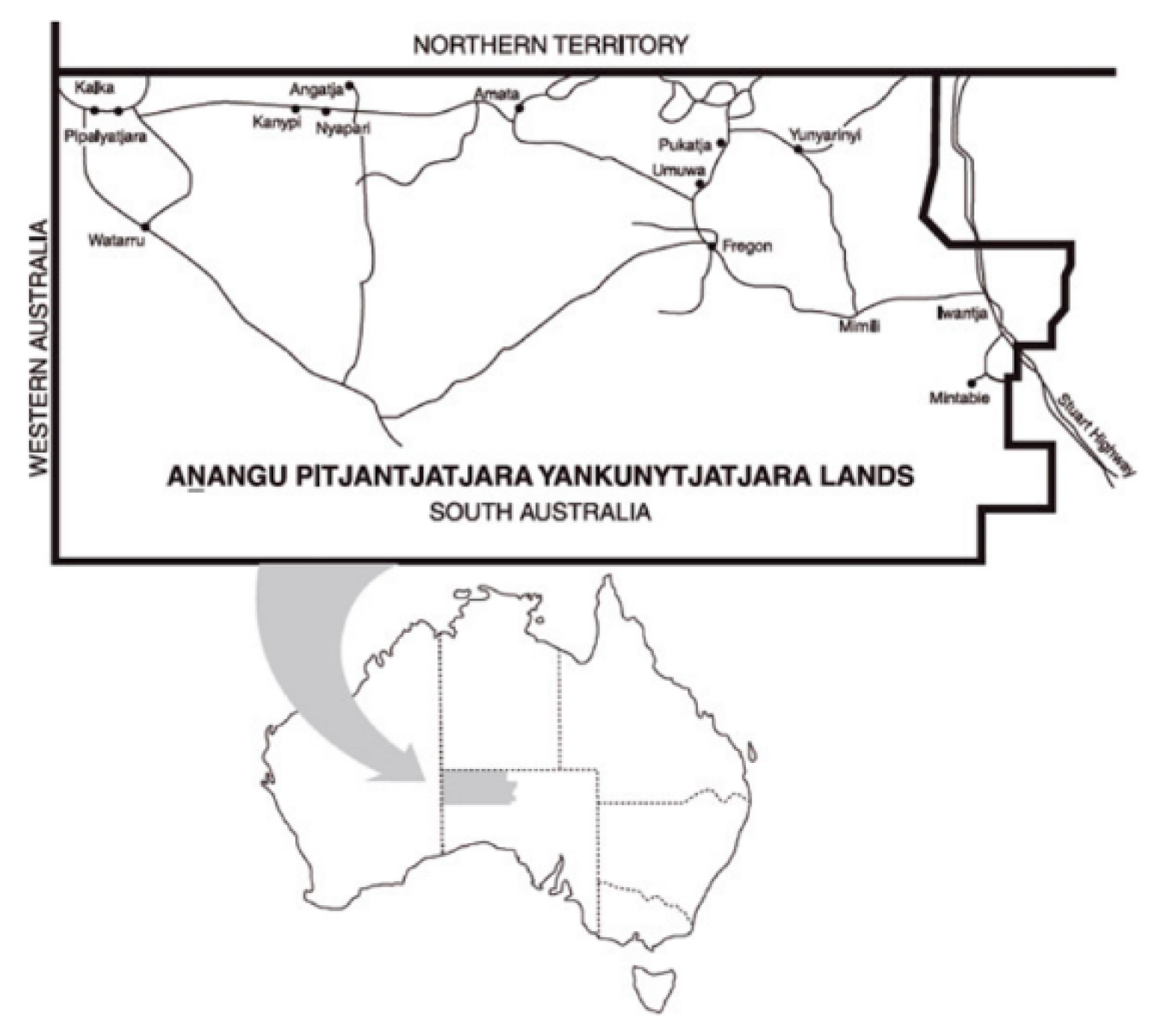
2.1. The Setting
2.2. Study Approach
2.3. Ethics and Privacy
2.4. Positionality of the Researchers
2.5. Study Participants
2.6. Data Collection
2.7. Data Analysis
3. Results
3.1. Household Composition and Income
3.2. Household Food and Drink Purchases
3.3. Dietary Intake
3.4. Eating Patterns Reported by Anangu
3.5. Factors Influencing Food and Drink Choices
4. Discussion
4.1. Study Strengths and Limitations
4.2. What Anangu Were Eating and Why
4.3. Traditional Foods
4.4. Factors Affecting Dietary Choice: Availability and Convenience
4.5. Factors Affecting Dietary Choice: Income
4.6. Factors Affecting Dietary Choice: Household Composition and Organization
4.7. Implications
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Lee, A.; Ride, K. Review of nutrition among Aboriginal and Torres Strait Islander people. Aust. Indig. Health Bull. 2018, 18, 1–47. [Google Scholar]
- Sebastian, T.; Donelly, M. Policy influences affecting the food practices of Indigenous Australians since colonisation. Aust. Aborig. Stud. 2013, 2, 59–75. [Google Scholar]
- Lee, A.; Rainow, S.; Tregenza, J.; Tregenza, L.; Balmer, L.; Bryce, S.; Paddy, M.; Sheard, J.; Schomburgk, D. Nutrition in remote Aboriginal communities: Lessons from Mai Wiru and the Anangu Pitjantjatjara Yankunytjatjara Lands. Aust. N. Z. J. Public Health 2016, 40, S81–S88. [Google Scholar] [CrossRef]
- Lee, A. The transition of Australian Aboriginal diet and nutritional health. In Metabolic Consequences of Changing Dietary Patterns; Simopoulos, A.P., Ed.; World Review of Nutrition and Dietetics: Washington, DC, USA, 1996; pp. 1–52. [Google Scholar] [CrossRef]
- O’Dea, K.; Jewell, P.A.; Whiten, A.; Altmann, S.A.; Strickland, S.S.; Oftedal, O.T. Traditional Diet and Food Preferences of Australian Aboriginal Hunter-Gatherers. Philos. Trans. R. Soc. B Biol. Sci. 1991, 334, 233–241. [Google Scholar] [CrossRef]
- Australian Institute of Health and Welfare. Australian Burden of Disease Study: Impact and Causes of Illness and Death in Aboriginal and Torres Strait Islander People 2011; AIHW: Canberra, Australia, 2016.
- Australian Institute of Health and Welfare. Cardiovascular Disease, Diabetes and Chronic Kidney Disease—Australian Facts: Aboriginal and Torres Strait Islander People; AIHW: Canberra, Australia, 2015.
- Brimblecombe, J.; van den Boogaard, C.; Wood, B.; Liberato, S.C.; Brown, J.; Barnes, A.; Rogers, A.; Coveney, J.; Ritchie, J.; Bailie, R. Development of the good food planning tool: A food system approach to food security in indigenous Australian remote communities. Health Place 2015, 34, 54–62. [Google Scholar] [CrossRef] [PubMed]
- Brimblecombe, J.K.; Ferguson, M.M.; Liberato, S.C.; O’Dea, K. Characteristics of the community-level diet of Aboriginal people in remote northern Australia. Med. J. Aust. 2013, 198, 380–384. [Google Scholar] [CrossRef] [PubMed]
- Rogers, A.; Ferguson, M.; Ritchie, J.; Van Den Boogaard, C.; Brimblecombe, J. Strengthening food systems with remote Indigenous Australians: Stakeholders’ perspectives. Health Promot. Int. 2018, 33, 38–48. [Google Scholar] [CrossRef] [PubMed]
- Torzillo, P.J.; Pholeros, P.; Rainow, S.; Barker, G.; Sowerbutts, T.; Short, T.; Irvine, A. The state of health hardware in Aboriginal communities in rural and remote Australia. Aust. N. Z. J. Public Health 2008, 32, 7–11. [Google Scholar] [CrossRef] [PubMed]
- Australian Institute of Health and Welfare. Aboriginal and Torres Strait Islander Health Performance Framework (HPF) Report 2017; AIHW: Canberra, Australia, 2018.
- Henryks, J.; Brimblecombe, J. Mapping Point-of-Purchase Influencers of Food Choice in Australian Remote Indigenous Communities: A Review of the Literature. SAGE Open 2016, 6. [Google Scholar] [CrossRef]
- Ferguson, M.; O’Dea, K.; Chatfield, M.; Moodie, M.; Altman, J.; Brimblecombe, J. The comparative cost of food and beverages at remote Indigenous communities, Northern Territory, Australia. Aust. N. Z. J. Public Health 2016, 40, S21–S26. [Google Scholar] [CrossRef] [PubMed]
- Thurber, K.A.; Banwell, C.; Neeman, T.; Dobbins, T.; Pescud, M.; Lovett, R.; Banks, E. Understanding barriers to fruit and vegetable intake in the Australian Longitudinal Study of Indigenous Children: A mixed-methods approach. Public Health Nutr. 2017, 20, 832–847. [Google Scholar] [CrossRef]
- Colles, S.L.; Maypilama, E.; Brimblecombe, J. Food, food choice and nutrition promotion in a remote Australian Aboriginal community. Aust. J. Prim. Health 2014, 20, 365–372. [Google Scholar] [CrossRef]
- Brimblecombe, J.; Maypilama, E.; Colles, S.; Scarlett, M.; Dhurrkay, J.G.; Ritchie, J.; O’Dea, K. Factors Influencing Food Choice in an Australian Aboriginal Community. Qual. Health Res. 2014, 24, 387–400. [Google Scholar] [CrossRef]
- Saethre, E. Demand sharing, nutrition and Warlpiri health: The social and economic strategies of food choice. In Ethnography the Production of Anthropological Knowledge: Essays in Honour of Nicolas Peterson; Musharbash, Y., Barber, M., Eds.; ANUE Press: Canberra, Australia, 2011; p. 175. [Google Scholar]
- Australian Bureau of Statistics. 4727.0.55.005—Australian Aboriginal and Torres Strait Islander Health Survey: Nutrition Results—Food and Nutrients, 2012–2013; ABS: Canberra, Australia, 2015.
- National Health and Medical Research Council. Australian Dietary Guidelines—Providing the Scientific Evidence for Healthier Australian Diets; National Health and Medical Research Council: Canberra, Australia, 2013.
- Food and Agriculture Organization of the United Nations. Rome Declaration on World Food Security and the World Food Summit Plan of Action; UN: Rome, Italy, 1996. [Google Scholar]
- Browne, J.; Hayes, R.; Gleeson, D. Aboriginal health policy: Is nutrition the ‘gap’ in ‘Closing the Gap’? Aust. N. Z. J. Public Health 2014, 38, 362–369. [Google Scholar] [CrossRef]
- Rowley, K.G.; Daniel, M.; Skinner, K.; Skinner, M.; White, G.A.; O’Dea, K. Effectiveness of a community-directed ‘healthy lifestyle’ program in a remote Australian Aboriginal community. Aust. N. Z. J. Public Health 2000, 24, 136–144. [Google Scholar] [CrossRef]
- Gwynn, J.; Sim, K.; Searle, T.; Senior, A.; Lee, A.; Brimblecombe, J. Effect of nutrition interventions on diet-related and health outcomes of Aboriginal and Torres Strait Islander Australians: A systematic review. BMJ Open 2019, 9. [Google Scholar] [CrossRef]
- Browne, J.; Adams, K.; Atkinson, P.; Gleeson, D.; Hayes, R. Food and nutrition programs for Aboriginal and Torres Strait Islander Australians: An overview of systematic reviews. Aust. Health Rev. 2018, 42, 689–697. [Google Scholar] [CrossRef]
- Lee, A.; Ride, K. Review of programs and services to improve Aboriginal and Torres Strait Islander nutrition and food security. Aust. Indig. Health Bull. 2018, 18, 1–22. [Google Scholar]
- Devitt, J. Contemporary Aboriginal Women and Subsistence in Remote, Arid Australia. Ph.D. Thesis, The University of Queensland, Brisbane, Australia, 1988, unpublished. [Google Scholar]
- Lee, A.J.; Smith, A.; Bryce, S.; O’Dea, K.; Rutishauser, I.H.E.; Mathews, J.D. Measuring dietary intake in remote Australian Aboriginal communities. Ecol. Food Nutr. 1995, 34, 19–31. [Google Scholar] [CrossRef]
- Coles-Rutishauser, I. Food Intake Studies in Australian Aborigines: Some methodological considerations. In Proceedings of 13th International Congress of Nutrition; John Libbey & Co Ltd.: London, UK, 1986; pp. 706–710. [Google Scholar]
- Worsley, A.; Baghurst, K.I.; Leitch, D.R. Social desirability response bias and dietary inventory responses. Hum. Nutr. Appl. Nutr. 1984, 38, 29–35. [Google Scholar]
- McMahon, E.; Wycherley, T.; O’Dea, K.; Brimblecombe, J. A comparison of dietary estimates from the National Aboriginal and Torres Strait Islander Health Survey to food and beverage purchase data. Aust. N. Z. J. Public Health 2017, 41, 598–603. [Google Scholar] [CrossRef]
- Tonkin, E.; Kennedy, D.; Hanieh, S.; Biggs, B.-A.; Kearns, T.; Gondarra, V.; Dhurrkay, R.; Brimblecombe, J. Dietary intake of Aboriginal Australian children aged 6–36 months in a remote community: A cross-sectional study. Nutr. J. 2020, 19, 1–12. [Google Scholar] [CrossRef]
- Australian Bureau of Statistics. 2016 Census of Population and Housing Storybook: Anangu Pitjantjatjara Yankunytjatjara Lands. Available online: https://www.abs.gov.au/AUSSTATS/abs@.nsf/DetailsPage/2076.02016?OpenDocument (accessed on 12 November 2019).
- Australian Bureau of Statistics. Region Data Summary: APY Lands (SA2) (406021138). Available online: https://itt.abs.gov.au/itt/r.jsp?RegionSummary®ion=406021138&dataset=ABS_REGIONAL_ASGS2016&geoconcept=ASGS_2016&measure=MEASURE&datasetASGS=ABS_REGIONAL_ASGS2016&datasetLGA=ABS_REGIONAL_LGA2018®ionLGA=LGA_2018®ionASGS=ASGS_2016 (accessed on 28 July 2020).
- Nganampa Health Council. UPK—Environmental Health. Available online: https://www.nganampahealth.com.au/nganampa-health-upk (accessed on 13 November 2019).
- Ngaanyatjarra Pitjantjatjara Yankunytjatjara (NPY) Women’s Council. Child and Family Well-Being Service. Available online: https://www.npywc.org.au/what-we-do/child-and-family-well-being/ (accessed on 13 November 2019).
- National Health and Medical Research Council. Ethical Conduct in Research with Aboriginal and Torres Strait Islander Peoples and Communities: Guidelines for Researchers and Stakeholders; Commonwealth of Australia: Canberra, Australia, 2018.
- Smith, L.T. Decolonizing Methodologies: Research and Indigenous Peoples, 2nd ed.; Zed Books Ltd.: London, UK, 2012. [Google Scholar]
- Martin, K.; Mirraboopa, B. Ways of knowing, being and doing: A theoretical framework and methods for indigenous and indigenist re-search. J. Aust. Stud. 2003, 27, 203–214. [Google Scholar] [CrossRef]
- Hammersley, M.; Atkinson, P. Ethnography Principles in Practice; Taylor & Francis: Hoboken, NJ, USA, 2007. [Google Scholar]
- Drawson, A.S.; Toombs, E.; Mushquash, C.J. Indigenous research methods: A systematic review. Int. Indig. Policy J. 2017, 8. [Google Scholar] [CrossRef]
- Rigney, L.-I. Indigenist Research and Aboriginal Australia. In Indigenous Peoples’ Wisdom and Power: Affirming Our Knowledge through Narratives; Kunnie, J., Nomalungelo, I.G., Eds.; Ashgate Publishing: Hampshire, UK, 2006; p. 32. [Google Scholar]
- Bessarab, D.; Ng’Andu, B. Yarning About Yarning as a Legitimate Method in Indigenous Research. Int. J. Crit. Indig. Stud. 2010, 3, 37–50. [Google Scholar] [CrossRef]
- Wilson, S. Research is Ceremony: Indigenous Research Methods; Fernwood Publishing: Black Point, NS, USA, 2008. [Google Scholar]
- Datta, R. Traditional storytelling: An effective Indigenous research methodology and its implications for environmental research. Int. J. Indig. Peoples 2018, 14, 35–44. [Google Scholar] [CrossRef]
- Wilson, S. Guest Editorial: What is an Indigenist Research Paradigm? Can. J. Nativ. Educ. 2007, 30, 193–195. [Google Scholar]
- Banks, J.A. The Lives and Values of Researchers: Implications for Educating Citizens in a Multicultural Society. Educ. Res. 1998, 27, 4–17. [Google Scholar] [CrossRef]
- Chavez, C. Conceptualizing from the inside: Advantages, complications, and demands on insider positionality. Qual. Rep. 2008, 13, 474. [Google Scholar]
- Max, K. Chapter Four: Anti-colonial Research: Working as an ally with Aboriginal Peoples. Counterpoints 2005, 252, 79–94. [Google Scholar]
- Krusz, E.; Davey, T.; Wigginton, B.; Hall, N. What Contributions, if Any, Can Non-Indigenous Researchers Offer Toward Decolonizing Health Research? Qual. Health Res. 2019, 30, 201–216. [Google Scholar] [CrossRef]
- Australian Bureau of Statistics. 2016 Census QuickStats: APY Lands. Available online: https://quickstats.censusdata.abs.gov.au/census_services/getproduct/census/2016/quickstat/406021138 (accessed on 20 July 2020).
- Government of South Australia. Liquor Licensing Act; Government of South Australia: Adelaide, Australia, 1997.
- Kovach, M. Conversational method in Indigenous research. First Peoples Child Fam. Rev. 2010, 14, 123–136. [Google Scholar]
- O’Reilly, K. Ethnographic Methods; Routledge: Abingdon, England, 2012. [Google Scholar]
- Xyris Pty Ltd. FoodWorks7 Professional; Xyris Software (Australia) Pty Ltd.: Brisbane, Australia, 2012. [Google Scholar]
- Tumilowicz, A.; Neufeld, L.M.; Pelto, G.H. Using ethnography in implementation research to improve nutrition interventions in populations. Matern. Child Nutr. 2015, 11, 55–72. [Google Scholar] [CrossRef] [PubMed]
- Ottrey, E.; Jong, J.; Porter, J. Ethnography in Nutrition and Dietetics Research: A Systematic Review. J. Acad. Nutr. Diet. 2018, 118, 1903. [Google Scholar] [CrossRef]
- Lee, A.J.; Bailey, A.P.V.; Yarmirr, D.; O’ Dea, K.; Mathews, J.D. Survival tucker: Improved diet and health indicators in an Aboriginal community. Aust. J. Public Health 1994, 18, 277–285. [Google Scholar] [CrossRef] [PubMed]
- Kruske, S.; Belton, S.; Wardaguga, M.; Narjic, C. Growing Up Our Way: The First Year of Life in Remote Aboriginal Australia. Qual. Health Res. 2012, 22, 777–787. [Google Scholar] [CrossRef]
- Australian Bureau of Statistics. 4727.0.55.008—Australian Aboriginal and Torres Strait Islander Health Survey: Consumption of Food Groups from the Australian Dietary Guidelines, 2012–2013. Available online: https://www.abs.gov.au/ausstats/abs@.nsf/Lookup/by%20Subject/4727.0.55.008~2012-13~Main%20Features~Key%20Findings~1 (accessed on 20 November 2019).
- Brimblecombe, J.K.; O’Dea, K. The role of energy cost in food choices for an Aboriginal population in northern Australia. Med. J. Aust. 2009, 190, 549–551. [Google Scholar] [CrossRef] [PubMed]
- Lee, A.J.; O’Dea, K.; Mathews, J.D. Apparent dietary intake in remote Aboriginal communities. Aust. J. Public Health 1994, 18, 190–197. [Google Scholar] [CrossRef]
- Lee, A. The Transition of Australian Aboriginal Diet and Nutritional Health. World Rev. Nutr. Diet. 1996, 79, 1–52. [Google Scholar] [CrossRef]
- Livingstone, K.M.; Olstad, D.L.; Leech, R.M.; Ball, K.; Meertens, B.; Potter, J.; Cleanthous, X.; Reynolds, R.; McNaughton, S.A. Socioeconomic Inequities in Diet Quality and Nutrient Intakes among Australian Adults: Findings from a Nationally Representative Cross-Sectional Study. Nutrients 2017, 9, 1092. [Google Scholar] [CrossRef]
- Adams, K.; Burns, C.; Liebzeit, A.; Ryschka, J.; Thorpe, S.; Browne, J. Use of participatory research and photo-voice to support urban Aboriginal healthy eating. Health Soc. Care Community 2012, 20, 497–505. [Google Scholar] [CrossRef]
- Carlson, A.; Frazao, E. Are Healthy Foods Really More Expensive? It Depends on How You Measure the Price; Economic Information Bulletin 96; US Department of Agriculture: Washington, DC, USA, 2012.
- Bryce, S. Women’s Gathering and Hunting in the Pitjantjatjara Homelands; Institute for Aboriginal Development: Alice Springs, Australia, 1996. [Google Scholar]
- Thurber, K.A.; Bagheri, N.; Banwell, C. Social determinants of sugar-sweetened beverage consumption in the longitudinal study of indigenous children. Fam. Matters 2014, 95, 51–61. [Google Scholar]
- Thompson, S.J.; Gifford, S.M.; Thorpe, L. The Social and Cultural Context of Risk and Prevention: Food and Physical Activity in an Urban Aboriginal Community. Health Educ. Behav. 2000, 27, 725–743. [Google Scholar] [CrossRef]
- Saethre, E. Nutrition, Economics and Food Distribution in an Australian Aboriginal Community. Anthropol. Forum 2005, 15, 151–169. [Google Scholar] [CrossRef]
- Kouris-Blazos, A.; Wahlqvist, M. Indigenous Australian food culture on cattle stations prior to the 1960s and food intake of older Aborigines in a community studied in 1988. Asia Pac. J. Clin. Nutr. 2000, 9, 224–231. [Google Scholar] [CrossRef] [PubMed]
- Counihan, C.; Højlund, S. (Eds.) Making Taste Public: Ethnographies of Food and the Senses; Bloomsbury Publishing: London, UK, 2018. [Google Scholar]
- Altman, J. A Genealogy of ‘Demand Sharing’: From pure anthropology to public policy. In Ethnography the Production of Anthropological Knowledge; Musharbash, Y., Barber, M., Eds.; ANU Press: Canberra, Australia, 2011; pp. 187–200. [Google Scholar]
- Davidson, P.; Saunders, P.; Bradbury, B.; Wong, M. Poverty in Australia 2020: Part 1, Overview. ACOSS/UNSW Poverty and Inequality Partnership Report No.3; ACOSS: Sydney, Australia, 2020. [Google Scholar]
- Rowse, T.; Scrimgeour, D.; Knight, S.; Thomas, D. Food-purchasing behaviour in an Aboriginal community. 1. Results of a survey. Aust. J. Public Health 1994, 18, 63–67. [Google Scholar] [CrossRef]
- Australian Bureau of Statistics. 2076.0—Census of Population and Housing: Characteristics of Aboriginal and Torres Strait Islander Australians 2016; ABS: Canberra, Australia, 2018.
- Australian Institute of Health and Welfare. Aboriginal and Torres Strait Islander People: A Focus Report on Housing and Homelessness. Cat. No. HOU 301; AIHW: Canberra, Australia, 2019.
- Memmott, P.; Birdsall-Jones, C.; Greenop, K. Australian Indigenous House Crowding, AHURI Final Report No.194; Australian Housing and Urban Research Institute: Melbourne, Australia, 2012. [Google Scholar]
- Australian Institute of Health and Welfare. Housing Circumstances of Indigenous Households: Tenure and Overcrowding; AIHW: Canberra, Australia, 2014.
- Payne, G.; Payne, J. The Hawthorne Effect. In Key Concepts in Social Research; Payne, G., Payne, J., Eds.; SAGE Publications Ltd.: London, UK, 2004. [Google Scholar]
- Lee, A.J.; Bonson, A.P.V.; Yarmirr, D.; O’Dea, K.; Mathews, J.D. Sustainability of a successful health and nutrition program in a remote Aboriginal community. Med. J. Aust. 1995, 162, 632–635. [Google Scholar] [CrossRef]
- Lee, A.; Rainow, S.; Balmer, L.; Scholz, R.; Hutchinson, R.; Bryce, S.; Woods, S.; Lewis, M.; Elliott, K.; Parnell Harrison, E.; et al. Making it on the Breadline—Coordinated, Community-Led Nutrition Initiatives Improve Food Security and Diet in Remote Australian Aboriginal Communities. Unpublished (in Development). 2020. [Google Scholar]


{kind=link}
| Household | Days Observed (n) | Composition: Number of Females (F), Males (M), Children (C) | Variability in Household Size During Data Collection Period * | Approximate Household Weekly Income | Total Household Expenditure on Food and Drinks During Data Collection Period | Hungry Days (n) | Food Storage, Preparation and Cooking Equipment | Observations and Comments |
|---|---|---|---|---|---|---|---|---|
| A1 | 7 | 10: 5F 2M 3C | Low | $1350 | $92.08 | 2 | No fridge; several saucepans | On 5 nights, healthy meat and vegetable meals were reported. F1 described eating well during childhood and had learned to cook from her mother (who had run a community kitchen). Household included long-term visitors (1F and 2C). |
| A2 | 8 | 9: 3F 3M 3C | Medium | $1635 | $197.67 | 2 | Fridge (large, working, empty); stove not working; fry pan purchased during study | Very little cooking observed or reported; only 4 main meals (lunch or dinner) reported in 8 days. Up to 15 people in household—some family members sleeping outside in tents. Large vehicle available so much family movement between communities; 4 members were away for 4 days. Household members went hunting one day–no kangaroo, had only honey ants. F1 spent most of an emergency relief fund payment on lollies and cake “because the kids were crying”. |
| A3 | 7 | 4: 2F 2M | Low | $985 | $74.71 | 2 | Fridge (recently purchased); stove; fry pan; kettle; toaster; electric sandwich maker. No saucepans or cutlery. | In 7 days, 6 main meals reported, most comprising tinned meat, bread and/or noodles. A visiting daughter, who was learning to cook at trade school, prepared prawns and salad one night. F1 bought a high number of discretionary items, explaining it was to “please” her son with snacks and drinks he likes. F1 is diabetic and reported little food intake e.g., only a mandarin and banana one day. One night another household gave F1 food for dinner. |
| B1 | 6 | 6: 2F 2M 2C | Low | $555 | $518.79 | 2 | Hotplates; two small saucepans and a billycan (bought on day 1); bowls and cutlery and stockpot and additional chopping board (also bought during data collection). No fridge; not using kitchen cupboards for storage due to cockroaches. | Household included two couples, one with two children. The couple without children had insecure income and often did not eat with the other family (had at least two hungry days). For the couple with children, meat (fresh or tinned) with damper or bread was the most common meal. Vegetables (particularly pumpkin) reported in several meals (home-made stews). Two-minute noodles common on days when there was less money. Children ate lots of Weet-BixTM. F1 purchased cooking and eating equipment during observation period. I.S. encouraged husband to join in with cooking; he asked for the recipe and reported later that they had repeated the meal. |
| B2 | 6 | 9: 4F 2M 3C | Low | $1780 | $262.53 | 1 | Fridge, stove, fry pan, electric flat grill, microwave, wok, deep fryer, sandwich maker | In 6 days observed, six dinner meals reported. Household reported eating a lot of chicken (bought frozen) and damper (one night had chicken with home-fried chips and salad pack), and vegetables on 3 days (included in stews). Children had breakfast and lunch at school, including fruit (bananas and oranges) and Weet-BixTM. F1 reported driving to store 30km away for “cheaper shopping”. |
| C1 | 11 | 10: 3F 4M 3C | High | $2275 | $604.71 | 1 | Small fridge in main kitchen; concealed fridge in bedroom; oven and stovetop (working); cooking fire outside; pots | Household included one family of visitors (5A, 2C). Recalled lots of snacks of take-away foods e.g., pies, pizzas; and lots of tinned meat and Weet-BixTM reported. Household was gifted fresh bullock meat (two meals). When matriarch was sick on days 6 and 7 the family food supply was impacted (no food intake reported one day). |
| C2 | 8 | 4: 2F 1M 1C | High | $1460 | $252.83 | 1 | Stovetop Fridge broken | One female and one child stayed only two days. Matriarch (grandmother) reported a lot of meat and vegetables/salad and fruit–but that did not accord with shopping dockets, which indicated high purchase of discretionary food and drinks. Matriarch received supported meal (lunch), which was her only meal some days. When asked about other meals she explained there was “no mai [food]; it’s a drought here”. |
| C3 | 4 | 4: 2F 2M | Low | $570 | No dockets collected | 1 | Fry pan, saucepan, toaster, freezer | Household had been using freezer as fridge and not eating food as it had “turned to stone” and was “old food”, not fresh. Household members went hunting; made a meal of maku (witchety grubs) and water. |
| C4 | 8 | 9: 4F 2M 3C | Medium | $1665 | $352.22 | 2 | (Not recorded) | Two female household members away much of the period. In 7 days, 4 dinners reported. Day one was hungry day–adults had arngu or nothing; after income received, they bought kangaroo tail and vegetables and family members ate takeaway at shop; the next day–only arngu; two days later when more income was received, they purchased food including vegetables, and reported home-made meals. |
| C5 | 8 | 13: 6F 3M 4C (1 baby) | High | $975 | $162.98 | Fridge (broken); 2 electric fry pans, 4 saucepans, 2 fry pans, kettle, toaster. | One family (couple and baby) went to Alice Springs (leaving another child); another family (1M, 1F, 3C) moved into the house. Over 8 days, household reported 7 dinners, 4 containing vegetables. No income or food on day 4, but the children ate at school and adults ate at the Arts Centre/office BBQ. Two matriarchs expressed interest in improving diet to lose weight. | |
| C6 | 8 | 8: 3F 5M 1C (baby) | High | $1000 | $141.08 58% kJ 65% $ | 1 | (Not recorded) | Two family groups–some shared and some independent eating; 2 M visiting; one F away half the observation period. Five dinners reported, some vegetables. Good breakfasts (mostly porridge). One hungry day for most–only bread and biscuits reported. |
| C7 | 5 | 13: 2F 2M 9C | Medium | $2550 | $359.64 | Fridge; locked cupboard and small fridge in bedroom; kitchen cupboards. | Two matriarchs (sisters), both working in community and bringing in wages. Breakfasts and lunches reported for most days, but not much evidence of dinners. Food stored in bedroom to conceal from children and visitors. F1 (mother of 2 of the children, Aunty of 7) saves her pay from Thursday to do “big shop” on Saturday, and has access to two other family members’ BasicsCards to buy food for children. F2 makes damper every day when present. F2 was away for most of the period; F1 also away a whole day and overnight to buy tires and food in Alice. One family (1F, 1M + 3C)—moved to another household during observation period. | |
| C8 | 4 | 4: 2F 2C | Low | $1490 | $905.90 | (Not recorded) | Purchased large quantities of meat (fresh and tinned). Two dinners of meat and vegetable curry reported. One day F1 spent $495 on shopping, including a whole box of bread; the next day she was upset that all the food purchased had been eaten or taken. | |
| C9 | 5 | 6: 2F 1M 3C | Low | $520 | $627.31 | Fridge and freezer, frying pan, no saucepans, some plates and cutlery | Household members visited the store daily and on most days purchased takeaway meals they consumed there. Dockets show on one day that both women shopped, F1 (paternal grandmother, who had been a HAAC cook) bought fish and vegetables; F2 purchased only take-away food and confectionary. F1 asked for dietary advice as she was diabetic. |
| Food Category (Per ADG Food Groupings) | Households | |||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| A1 | A2 | A3 | B1 | B2 | C1 | C2 | C4 | C5 | C6 | C7 | C8 | C9 | Mean | SD | Median | Q1 | Q3 | |
| Grain (Cereal) Foods (Mostly Wholegrain) | $8.91 | $9.85 | $14.10 | $106.10 | $38.61 | $68.55 | $24.05 | $31.86 | $38.91 | $12.14 | $39.48 | $80.87 | $146.51 | $47.69 | $41.91 | $38.61 | $14.10 | $68.55 |
| (10%) | (5%) | (19%) | (20%) | (15%) | (11%) | (10%) | (9%) | (24%) | (9%) | (11%) | (9%) | (23%) | (13%) | (6%) | (11%) | (9%) | (19%) | |
| Milk, Yoghurt, Cheese | $16.21 | - | - | $33.26 | $12.07 | $48.36 | $14.54 | $25.04 | $2.19 | $15.38 | $47.56 | $54.07 | $29.50 | $22.94 | $18.60 | $16.21 | $12.07 | $33.26 |
| (18%) | (0%) | (0%) | (6%) | (5%) | (8%) | (6%) | (7%) | (1%) | (11%) | (13%) | (6%) | (5%) | (7%) | (5%) | (6%) | (5%) | (8%) | |
| Fruit | $5.92 | $19.74 | $7.96 | $26.89 | $12.65 | $1.34 | $0.95 | $13.71 | $4.37 | $14.39 | $16.73 | $30.21 | $35.81 | $14.67 | $11.05 | $13.71 | $5.92 | $19.74 |
| (6%) | (10%) | (11%) | (5%) | (5%) | (0.1%) | (0.1%) | (4%) | (3%) | (10%) | (5%) | (3%) | (6%) | (5%) | (3%) | (5%) | (3%) | (6%) | |
| Vegetables and Legumes/beans | $9.93 | - | $5.91 | $34.14 | $26.30 | $68.84 | $13.83 | $17.64 | $25.36 | $3.20 | $76.02 | $116.43 | $65.52 | $35.62 | $35.37 | $25.36 | $9.93 | $65.52 |
| (11%) | (0%) | (8%) | (7%) | (10%) | (11%) | (5%) | (5%) | (16%) | (2%) | (21%) | (13%) | (10%) | (9%) | (6%) | (10%) | (5%) | (0%) | |
| Lean Meats and Poultry, Fish, Eggs, etc. | $21.80 | $30.73 | $15.16 | $168.80 | $31.33 | $116.28 | $18.42 | $84.22 | $58.14 | $4.20 | $14.14 | $136.56 | $105.01 | $61.91 | $54.41 | $31.33 | $18.42 | $105.01 |
| (24%) | (16%) | (20%) | (33%) | (12%) | (19%) | (7%) | (24%) | (36%) | (3%) | (4%) | (15%) | (17%) | (18%) | (10%) | (17%) | (12%) | (24%) | |
| Healthy Oils and Spreads (Unsaturated) | $5.33 | - | $2.94 | $5.88 | $3.33 | $30.57 | - | $5.26 | - | - | - | $39.47 | $19.09 | $8.61 | $12.92 | $3.33 | - | $5.88 |
| (6%) | (0%) | (4%) | (1%) | (1%) | (5%) | (0%) | (1%) | (0%) | (0%) | (0%) | (4%) | (3%) | (2%) | (2%) | (1%) | (0%) | (4%) | |
| Discretionary Food and Drinks | $23.98 | $137.35 | $28.64 | $143.74 | $138.23 | $270.78 | $181.04 | $174.49 | $34.01 | $91.77 | $165.72 | $448.30 | $225.87 | $158.76 | $114.72 | $143.74 | $91.77 | $181.04 |
| (26%) | (69%) | (38%) | (28%) | (53%) | (45%) | (72%) | (50%) | (21%) | (65%) | (46%) | (49%) | (36%) | (46%) | (16%) | (46%) | (36%) | (53%) | |
| TOTAL | $92.08 | $197.67 | $74.71 | $518.79 | $262.53 | $604.71 | $252.83 | $352.22 | $162.98 | $141.08 | $359.64 | $905.90 | $627.31 | $350.19 | $248.43 | $262.53 | $162.98 | $518.79 |
| Number of Days of Data Collection | 7 | 8 | 7 | 6 | 6 | 11 | 8 | 8 | 8 | 8 | 5 | 4 | 5 | 7.0 | 1.9 | 7.0 | 5.3 | 8.0 |
| Food Category | Households | |||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| A1 | A2 | A3 | B1 | B2 | C1 | C2 | C4 | C5 | C6 | C7 | C8 | C9 | Mean | SD | Median | Q1 | Q3 | |
| Grain (cereal) foods | 19% | 18% | 45% | 58% | 31% | 31% | 20% | 25% | 57% | 27% | 28% | 25% | 36% | 32% | 13% | 28% | 25% | 36% |
| Milk, yoghurt, cheese, and/or alternatives | 10% | 0% | 0% | 4% | 5% | 11% | 7% | 6% | 2% | 9% | 13% | 7% | 6% | 6% | 4% | 6% | 4% | 9% |
| Fruit | 2% | 5% | 5% | 1% | 2% | 0% | 0% | 1% | 1% | 5% | 3% | 1% | 3% | 2% | 2% | 2% | 1% | 3% |
| Vegetables and legumes/beans | 3% | 0% | 6% | 0% | 4% | 5% | 3% | 3% | 14% | 1% | 2% | 5% | 5% | 4% | 4% | 3% | 2% | 5% |
| Lean meats and poultry, fish, eggs, etc. | 12% | 14% | 15% | 10% | 6% | 11% | 4% | 10% | 14% | 1% | 11% | 10% | 9% | 10% | 4% | 10% | 9% | 12% |
| Healthy oils and spreads (unsaturated) | 0% | 0% | 0% | 0% | 0% | 0% | 0% | 0% | 0% | 0% | 0% | 0% | 0% | 0% | 0% | 0% | 0% | 0% |
| Discretionary food and drinks | 54% | 62% | 31% | 25% | 52% | 42% | 65% | 53% | 12% | 58% | 44% | 52% | 42% | 46% | 15% | 52% | 42% | 54% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bryce, S.; Scales, I.; Herron, L.-M.; Wigginton, B.; Lewis, M.; Lee, A.; Ngaanyatjarra Pitjantjatjara Yankunytjatjara (NPY) Women’s Council. Maitjara Wangkanyi: Insights from an Ethnographic Study of Food Practices of Households in Remote Australian Aboriginal Communities. Int. J. Environ. Res. Public Health 2020, 17, 8109. https://doi.org/10.3390/ijerph17218109
Bryce S, Scales I, Herron L-M, Wigginton B, Lewis M, Lee A, Ngaanyatjarra Pitjantjatjara Yankunytjatjara (NPY) Women’s Council. Maitjara Wangkanyi: Insights from an Ethnographic Study of Food Practices of Households in Remote Australian Aboriginal Communities. International Journal of Environmental Research and Public Health. 2020; 17(21):8109. https://doi.org/10.3390/ijerph17218109
Chicago/Turabian StyleBryce, Suzanne, Inawantji Scales, Lisa-Maree Herron, Britta Wigginton, Meron Lewis, Amanda Lee, and Ngaanyatjarra Pitjantjatjara Yankunytjatjara (NPY) Women’s Council. 2020. "Maitjara Wangkanyi: Insights from an Ethnographic Study of Food Practices of Households in Remote Australian Aboriginal Communities" International Journal of Environmental Research and Public Health 17, no. 21: 8109. https://doi.org/10.3390/ijerph17218109
APA StyleBryce, S., Scales, I., Herron, L.-M., Wigginton, B., Lewis, M., Lee, A., & Ngaanyatjarra Pitjantjatjara Yankunytjatjara (NPY) Women’s Council. (2020). Maitjara Wangkanyi: Insights from an Ethnographic Study of Food Practices of Households in Remote Australian Aboriginal Communities. International Journal of Environmental Research and Public Health, 17(21), 8109. https://doi.org/10.3390/ijerph17218109