Common Running Musculoskeletal Injuries and Associated Factors among Recreational Gorge Marathon Runners: An Investigation from 2013 to 2018 Taroko Gorge Marathons


Abstract
1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Characteristics of Taroko Gorge Marathon
2.3. Instrument
2.4. Statistical Analysis
3. Results
3.1. Basic Characteristics
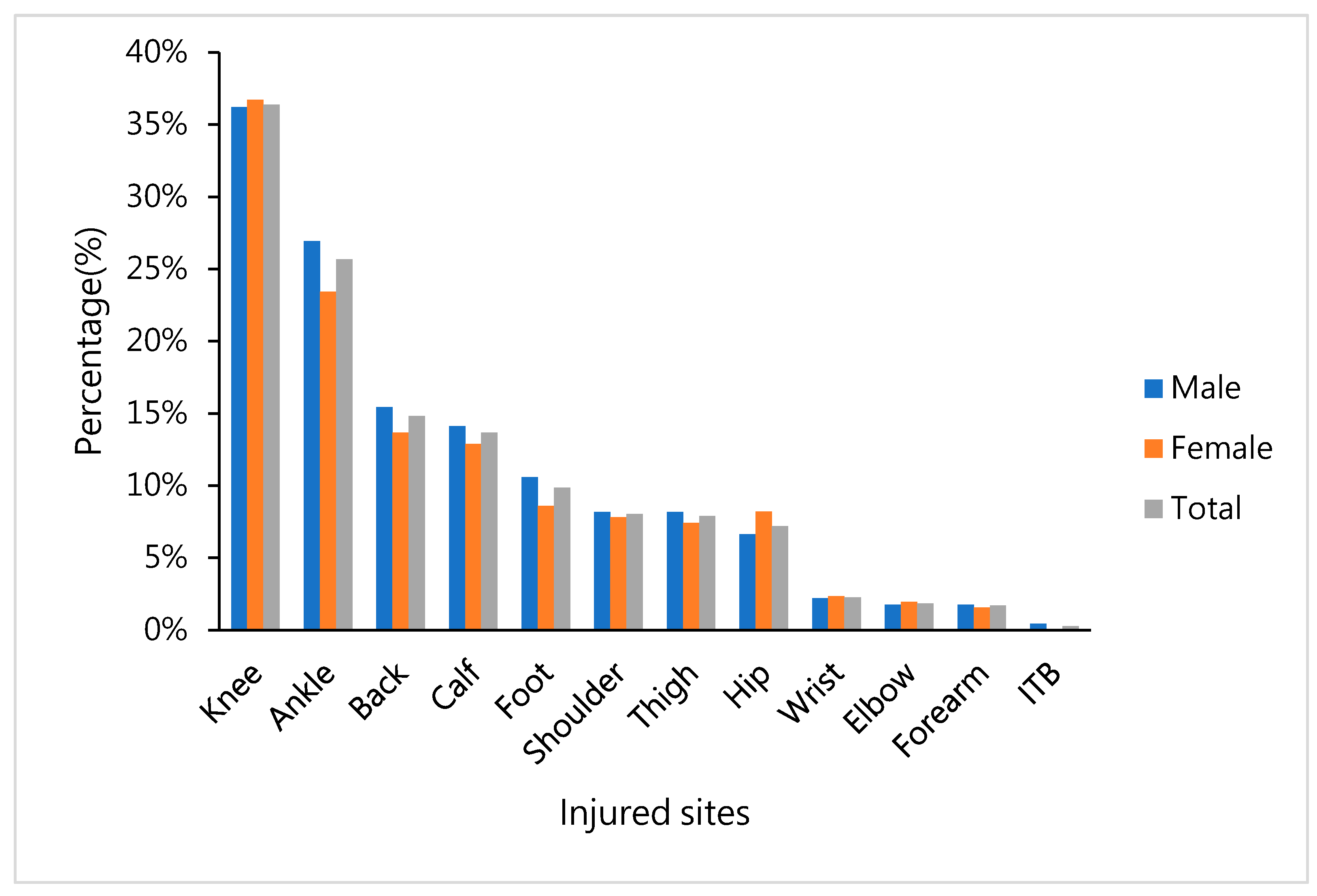
3.2. Previous Injured Sites of the Body before Gorge Marathon
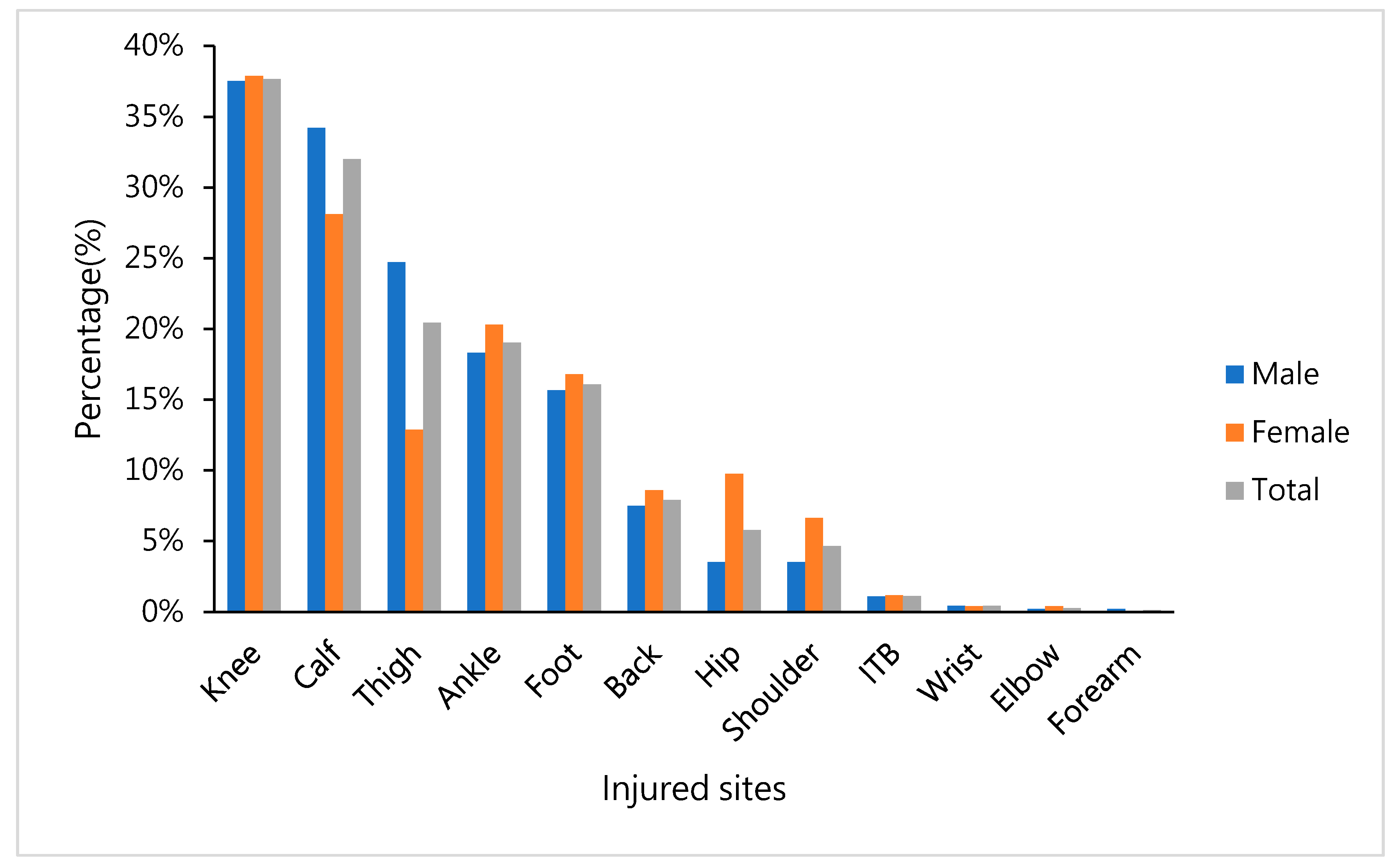
3.3. Proportion of Injured Sites of the Body after the Gorge Marathon
3.4. Comparing the Proportions of Injured Sites before the Gorge Marathon
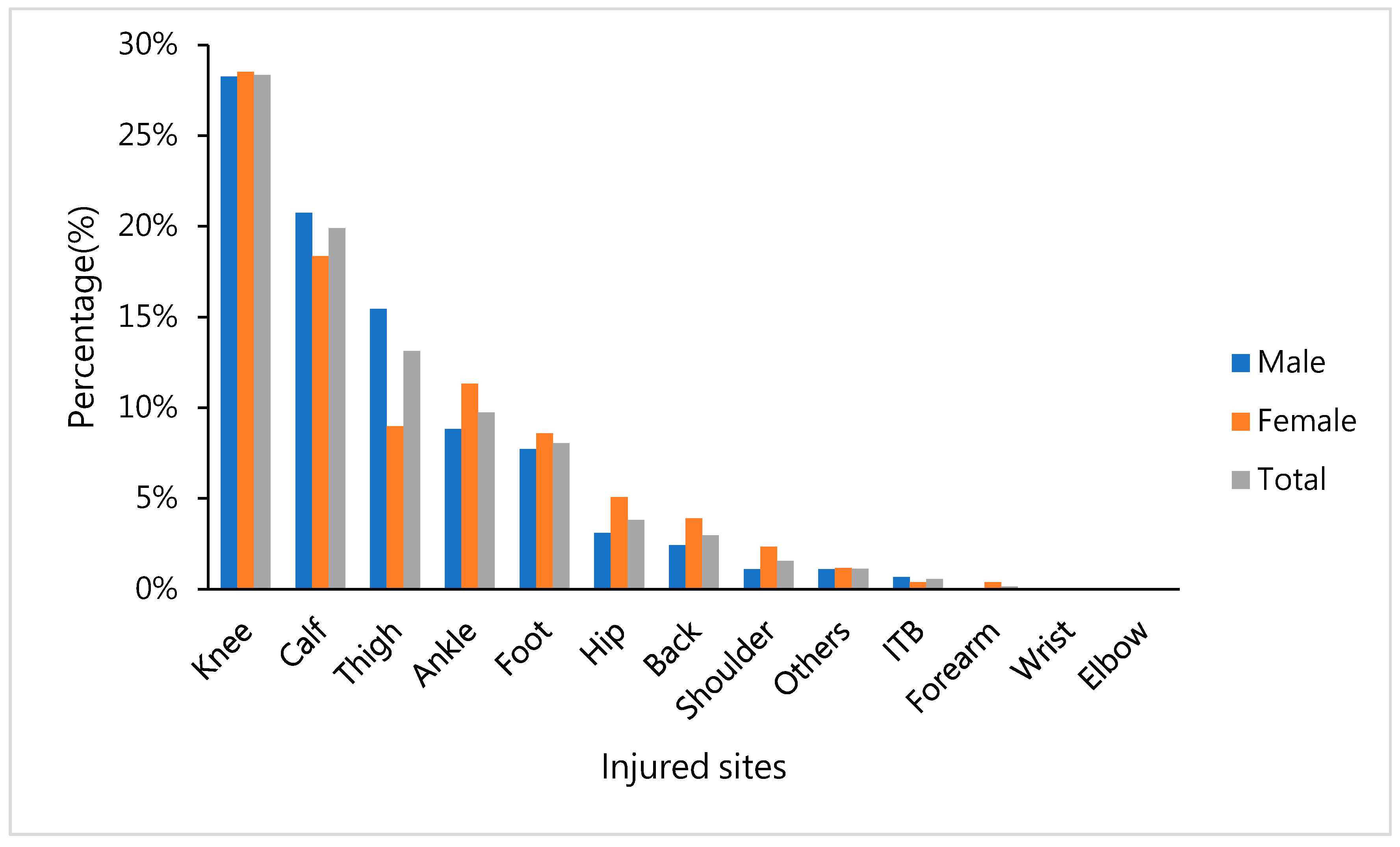
3.5. Influenced Sites of the Body after the Gorge Marathon
3.6. Factors Associated with Injury
4. Discussion
4.1. Running Injury Incidence and Injury Location
4.2. Risk Factors for Running Injuries
4.2.1. Sex
4.2.2. BMI
4.2.3. Running Training Factors Include Running Experience, Training Frequency, and Running Distance
4.2.4. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Van Middelkoop, M.; Kolkman, J.; Van Ochten, J.; Bierma-Zeinstra, S.M.; Koes, B. Prevalence and incidence of lower extremity injuries in male marathon runners. Scand. J. Med. Sci. Sports 2008, 18, 140–144. [Google Scholar] [CrossRef] [PubMed]
- van Gent, R.N.; Siem, D.; van Middelkoop, M.; van Os, A.G.; Bierma-Zeinstra, S.M.; Koes, B.W. Incidence and determinants of lower extremity running injuries in long distance runners: A systematic review. Br. J. Sports Med. 2007, 41, 469–480; discussion 480. [Google Scholar] [CrossRef] [PubMed]
- Hespanhol Junior, L.C.; Pena Costa, L.O.; Lopes, A.D. Previous injuries and some training characteristics predict running-related injuries in recreational runners: A prospective cohort study. J. Physiother. 2013, 59, 263–269. [Google Scholar] [CrossRef]
- Chang, W.L.; Shih, Y.F.; Chen, W.Y. Running injuries and associated factors in participants of ING Taipei Marathon. Phys. Ther. Sport. 2012, 13, 170–174. [Google Scholar] [CrossRef] [PubMed]
- Lopes, A.D.; Hespanhol, L.C.; Yeung, S.S.; Costa, L.O.P. What are the main running-related musculoskeletal injuries? A systematic review. Sports Med. 2012, 42, 891–905. [Google Scholar] [CrossRef]
- van Poppel, D.; Scholten-Peeters, G.G.; van Middelkoop, M.; Verhagen, A.P. Prevalence, incidence and course of lower extremity injuries in runners during a 12-month follow-up period. Scand. J. Med. Sci. Sports 2014, 24, 943–949. [Google Scholar] [CrossRef] [PubMed]
- Van Middelkoop, M.; Kolkman, J.; Van Ochten, J.; Bierma-Zeinstra, S.M.; Koes, B.W. Risk factors for lower extremity injuries among male marathon runners. Scand. J. Med. Sci. Sports 2008, 18, 691–697. [Google Scholar] [CrossRef]
- Gajda, R.; Walasek, P.; Jarmuszewski, M. Right knee-The weakest point of the best ultramarathon runners of the world? A case study. Int. J. Environ. Res. Public Health 2020, 17, 5955. [Google Scholar] [CrossRef]
- Hreljac, A. Etiology, prevention, and early intervention of overuse injuries in runners: A biomechanical perspective. Phys. Med. Rehabil. Clin. N. Am. 2005, 16, 651–667. [Google Scholar] [CrossRef] [PubMed]
- Saragiotto, B.T.; Yamato, T.P.; Junior, H.L.C.; Rainbow, M.J.; Davis, I.S.; Lopes, A.D. What are the main risk factors for running-related injuries? Sports Med. 2014, 44, 1153–1163. [Google Scholar] [CrossRef] [PubMed]
- Benca, E.P.Z.; von Skrbensky, G.; Ahmetović, A.; Windhager, R.; Krpo, S. Runining injuries. Med. Žurnal 2013, 19, 345–353. [Google Scholar]
- van Poppel, D.; van der Worp, M.; Slabbekoorn, A.; van den Heuvel, S.S.P.; van Middelkoop, M.; Koes, B.W.; Verhagen, A.P.; Scholten-Peeters, G.G.M. Risk factors for overuse injuries in short- and long-distance running: A systematic review. J. Sport. Health Sci. 2020. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, R.O.; Buist, I.; Sørensen, H.; Lind, M.; Rasmussen, S. Training errors and running related injuries: A systematic review. Int. J. Sports Phys. Ther. 2012, 7, 58–75. [Google Scholar]
- Buist, I.; Bredeweg, S.W.; Bessem, B.; van Mechelen, W.; Lemmink, K.A.; Diercks, R.L. Incidence and risk factors of running-related injuries during preparation for a 4-mile recreational running event. Br. J. Sports Med. 2010, 44, 598–604. [Google Scholar] [CrossRef] [PubMed]
- Wen, D.Y. Risk factors for overuse injuries in runners. Curr. Sports Med. Rep. 2007, 6, 307–313. [Google Scholar] [CrossRef]
- Buist, I.; Bredeweg, S.W.; Lemmink, K.A.; van Mechelen, W.; Diercks, R.L. Predictors of running-related injuries in novice runners enrolled in a systematic training program: A prospective cohort study. Am. J. Sports Med. 2010, 38, 273–280. [Google Scholar] [CrossRef]
- van Mechelen, W.; Hlobil, H.; Kemper, H.C.; Voorn, W.J.; de Jongh, H.R. Prevention of running injuries by warm-up, cool-down, and stretching exercises. Am. J. Sports Med. 1993, 21, 711–719. [Google Scholar] [CrossRef] [PubMed]
- Hofstede, H.; Franke, T.P.C.; van Eijk, R.P.A.; Backx, F.J.G.; Kemler, E.; Huisstede, B.M.A. In training for a marathon: Runners and running-related injury prevention. Phys. Ther. Sport. 2020, 41, 80–86. [Google Scholar] [CrossRef]
- Beck, B.R.; Rudolph, K.; Matheson, G.O.; Bergman, A.G.; Norling, T.L. Risk factors for tibial stress injuries: A case-control study. Clin. J. Sport. Med. 2015, 25, 230–236. [Google Scholar] [CrossRef]
- Giovanelli, N.; Taboga, P.; Rejc, E.; Simunic, B.; Antonutto, G.; Lazzer, S. Effects of an uphill marathon on running mechanics and lower-limb muscle fatigue. Int. J. Sports Physiol. Perform. 2016, 11, 522–529. [Google Scholar] [CrossRef]
- Carmona, G.; Roca, E.; Guerrero, M.; Cusso, R.; Irurtia, A.; Nescolarde, L.; Brotons, D.; Bedini, J.L.; Cadefau, J.A. Sarcomere disruptions of slow fiber resulting from mountain ultramarathon. Int. J. Sports Physiol. Perform. 2015, 10, 1041–1047. [Google Scholar] [CrossRef][Green Version]
- Linton, L.; Valentin, S. Running with injury: A study of UK novice and recreational runners and factors associated with running related injury. J. Sci. Med. Sport. 2018, 21, 1221–1225. [Google Scholar] [CrossRef]
- Telhan, G.; Franz, J.R.; Dicharry, J.; Wilder, R.P.; Riley, P.O.; Kerrigan, D.C. Lower limb joint kinetics during moderately sloped running. J. Athl. Train. 2010, 45, 16–21. [Google Scholar] [CrossRef]
- Vernillo, G.; Giandolini, M.; Edwards, W.B.; Morin, J.B.; Samozino, P.; Horvais, N.; Millet, G.Y. Biomechanics and physiology of uphill and downhill running. Sports Med. 2017, 47, 615–629. [Google Scholar] [CrossRef]
- Steinacker, T.; Steuer, M.; Höltke, V. Orthopedic problems in older marathon runners. Sportverletz. Sportschaden 2001, 15, 12–15. [Google Scholar] [CrossRef]
- Ellapen, T.J.; Satyendra, S.; Morris, J.; Van Heerden, H.J. Common running musculoskeletal injuries among recreational half-marathon runners in KwaZulu-Natal. S. Afr. J. Sports Med. 2013, 25. [Google Scholar] [CrossRef]
- Mayooran, S.; Nanayakkara, S.D.I.; Rajaratne, A.A.J.; HMSRB, K. Prevalence and associated factors of injuries related to running: A study among runners in Sri Lanka. Am. J. Sports Sci. Med. 2019, 7, 28–33. [Google Scholar] [CrossRef][Green Version]
- Francis, P.; Whatman, C.; Sheerin, K.; Hume, P.; Johnson, M.I. The proportion of lower limb running injuries by gender, anatomical location and specific pathology: A systematic review. J. Sports Sci. Med. 2019, 18, 21–31. [Google Scholar]
- Mallaropoulos, N.M.D.; Tsaklis, P. Prevalence of injury in ultra-trail running. Hum. Mov. Sci. 2015, 16, 52–59. [Google Scholar] [CrossRef]
- Vitez, L.P.Z.; Zadnik, V.; Drobnič, M. Running injuries in the participants of Ljubljana Marathon. Zdr. Varst. 2017, 56, 196–202. [Google Scholar] [CrossRef][Green Version]
- van Poppel, D.; de Koning, J.; Verhagen, A.P.; Scholten-Peeters, G.G.M. Risk factors for lower extremity injuries among half marathon and marathon runners of the Lage Landen Marathon Eindhoven 2012: A prospective cohort study in the Netherlands. Scand. J. Med. Sci. Sports 2015, 26, 226–234. [Google Scholar] [CrossRef]
- Rasmussen, C.H.; Nielsen, R.Ø.; Juul, M.S.; Rasmussen, S. Weekly running volume and risk of running related injuries among marathon runners. Int. J. Sports Phys. 2013, 8, 111. [Google Scholar]
- Nielsen, R.O.; Bertelsen, M.L.; Parner, E.T.; Sørensen, H.; Lind, M.; Rasmussen, S. Running more than three kilometers during the first week of a running regimen may be associated with increased risk of injury in obese novice runners. Int. J. Sports Phys. 2014, 9, 338. [Google Scholar]
- Bertelsen, M.L.; Hulme, A.; Petersen, J.; Brund, R.K.; Sorensen, H.; Finch, C.F.; Parner, E.T.; Nielsen, R.O. A framework for the etiology of running-related injuries. Scand. J. Med. Sci. Sports 2017, 27, 1170–1180. [Google Scholar] [CrossRef]
- van der Worp, M.P.; ten Haaf, D.S.; van Cingel, R.; de Wijer, A.; der Sanden, N.M.W.; Staal, J.B. Injuries in runners: A systematic review on risk factors and sex differences. PLoS ONE 2015, 10, e0114937. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | Male | Female | Total | p Value |
|---|---|---|---|---|
| N | 453 | 256 | 709 | |
| Year | - | - | - | 0.517 |
| 2013 | 74 (16.3%) | 40 (15.6%) | 114 (16.1%) | |
| 2014 | 67 (14.8%) | 39 (15.2%) | 106 (15.0%) | |
| 2015 | 83 (18.3%) | 43 (16.8%) | 126 (17.8%) | |
| 2016 | 88 (19.4%) | 38 (14.8%) | 126 (17.8%) | |
| 2017 | 82 (18.1%) | 55 (21.5%) | 137 (19.3%) | |
| 2018 | 59 (13.0%) | 41(16.0%) | 100 (14.1%) | |
| Age | 34.56 ± 9.98 | 33.09 ± 9.71 | 34.03 ± 9.91 | 0.063 |
| BMI | 23.59 ± 3.06 | 20.81 ± 2.17 | 22.62 ± 3.08 | <0.001* |
| BMI group | - | - | - | <0.001 * |
| Normal | 259 (58.5%) | 187 (79.2%) | 446 (65.7%) | |
| Underweight | 9 (2.0%) | 29 (12.3%) | 38 (5.6%) | |
| Overweight | 124 (28.0%) | 18 (7.6%) | 142 (20.9%) | |
| Obese | 51 (11.5%) | 2 (0.8%) | 53 (7.8%) | |
| Education | - | - | - | 0.001 * |
| High school degree or below | 35 (8.0%) | 19 (7.7%) | 54 (7.9%) | |
| College degree | 224 (51.5%) | 161 (65.4%) | 385 (56.5%) | |
| Master’s degree or above | 176 (40.5%) | 66 (26.8%) | 242 (35.5%) | |
| Type | - | - | - | <0.001 * |
| Mini-marathon (5K) | 10 (2.5%) | 22 (9.8%) | 32 (5.1%) | |
| Half-marathon | 325 (79.9%) | 191 (85.3%) | 516 (81.8%) | |
| Marathon | 72 (17.7%) | 11 (4.9%) | 83 (13.2%) | |
| Experience of running | - | - | - | |
| Mountain road marathon (%) | 194 (46.1%) | 82 (34.6%) | 276 (41.9%) | 0.004 * |
| Self-training (%) | 87 (22.5%) | 40 (18.5%) | 127 (21.1%) | 0.253 |
| Previous sports injuries (%) | 322 (75.6%) | 184 (76.0%) | 506 (75.7%) | 0.897 |
| Current running injury (%) | 405 (96.4%) | 232 (97.5%) | 637 (96.8%) | 0.461 |
| Attributed to Taroko Marathon (%) | 271 (69.0%) | 150 (65.8%) | 421(67.8%) | 0.416 |
| Marathon experience (years) | 2.22 ± 1.8 | 1.85 ± 1.65 | 2.09 ± 1.76 | 0.010* |
| Number of participations in marathons (times/year) | 5.8 ± 13.01 | 4.28 ± 6.76 | 5.26 ± 11.24 | 0.140 |
| Normal running (times/week) | 2.73 ± 2.01 | 2.33 ± 1.71 | 2.59 ± 1.92 | 0.013 * |
| Weekly running distance (km) | 8.46 ± 11.39 | 6.33 ± 3.3 | 7.75 ± 9.54 | 0.021 * |
| Weekly running time (min) | 50.02 ± 25.45 | 43.17 ± 23.46 | 47.68 ± 24.96 | 0.026 * |
| Mountain marathon times | 5.16 ± 12.06 | 3.63 ± 11.69 | 4.69 ± 11.95 | 0.362 |
| Number of self-training sessions (times/week) | 3.17 ± 2.3 | 2.32 ± 1.56 | 2.94 ± 2.15 | 0.061 |
| Self-training distance (km) | 11.89 ± 21.91 | 10 ± 5.32 | 11.41 ± 19.11 | 0.659 |
| Warmup time (min) | 14.75 ± 14.97 | 13.18 ± 12.26 | 14.19 ± 14.07 | 0.168 |
| Need to warm up more | 12.77 ± 9.5 | 11.9 ± 8.66 | 12.49 ± 9.22 | 0.546 |
| Satisfaction of service provided by physical therapy | 4.88 ± 0.42 | 4.87 ± 0.43 | 4.88 ± 0.42 | 0.774 |
| VAS (Pre) | 5.87 ± 1.76 | 5.76 ± 1.91 | 5.83 ± 1.82 | 0.459 |
| VAS (Post) | 2.28 ± 1.55 | 2.29 ± 1.57 | 2.28 ± 1.55 | 0.929 |
| Characteristics | Calf | Thigh | Knee | |||
|---|---|---|---|---|---|---|
| Odds Ratio (95% CI) | p Value | Odds Ratio (95% CI) | p Value | Odds Ratio (95% CI) | p Value | |
| Age | 1.00 (0.98,1.02) | 0.704 | 0.98 (0.96,1.00) | 0.103 | 0.98 (0.96,0.99) | 0.019 * |
| Sex | - | - | - | - | - | - |
| Female | References | NA | References | NA | References | NA |
| Male | 1.31 (0.86,2.00) | 0.208 | 2.42 (1.40,4.19) | 0.002 * | 0.78 (0.51,1.19) | 0.241 |
| BMI Group | - | - | - | - | - | - |
| Normal | References | NA | References | NA | References | NA |
| Underweight | 1.66 (0.76,3.61) | 0.203 | 3.35 (1.41,8.01) | 0.006 * | 0.32 (0.12,0.81) | 0.017 * |
| Overweight | 1.00 (0.63,1.60) | 0.993 | 1.16 (0.67,1.99) | 0.593 | 1.11 (0.69,1.79) | 0.666 |
| Obese | 1.79 (0.92,3.49) | 0.088 | 1.49 (0.70,3.15) | 0.303 | 1.25 (0.61,2.56) | 0.540 |
| Education | - | - | - | - | - | - |
| high school degree or below | References | NA | References | NA | References | NA |
| College degree | 1.05 (0.51,2.17) | 0.888 | 0.91 (0.38,2.14) | 0.824 | 0.79 (0.37,1.70) | 0.553 |
| Master’s degree or above | 0.98 (0.47,2.06) | 0.967 | 1.16 (0.49,2.75) | 0.743 | 0.91 (0.42,1.97) | 0.803 |
| Type | - | - | - | - | - | - |
| Mini-marathon | References | NA | References | NA | References | NA |
| Half-marathon | 1.22 (0.52,2.87) | 0.653 | 1.14 (0.39,3.33) | 0.817 | 1.11 (0.46,2.66) | 0.815 |
| Marathon | 0.91 (0.34,2.44) | 0.843 | 1.56 (0.47,5.15) | 0.466 | 0.92 (0.34,2.53) | 0.874 |
| Previous sports injuries | - | - | - | - | - | - |
| No | References | NA | References | NA | References | NA |
| Yes | 4.02 (2.44,6.60) | <0.001 * | 9.66 (4.84,19.27) | <0.001 * | 5.65 (3.88,8.20) | <0.001 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hsu, C.-L.; Yang, C.-H.; Wang, J.-H.; Liang, C.-C. Common Running Musculoskeletal Injuries and Associated Factors among Recreational Gorge Marathon Runners: An Investigation from 2013 to 2018 Taroko Gorge Marathons. Int. J. Environ. Res. Public Health 2020, 17, 8101. https://doi.org/10.3390/ijerph17218101
Hsu C-L, Yang C-H, Wang J-H, Liang C-C. Common Running Musculoskeletal Injuries and Associated Factors among Recreational Gorge Marathon Runners: An Investigation from 2013 to 2018 Taroko Gorge Marathons. International Journal of Environmental Research and Public Health. 2020; 17(21):8101. https://doi.org/10.3390/ijerph17218101
Chicago/Turabian StyleHsu, Chia-Li, Chich-Haung Yang, Jen-Hung Wang, and Chung-Chao Liang. 2020. "Common Running Musculoskeletal Injuries and Associated Factors among Recreational Gorge Marathon Runners: An Investigation from 2013 to 2018 Taroko Gorge Marathons" International Journal of Environmental Research and Public Health 17, no. 21: 8101. https://doi.org/10.3390/ijerph17218101
APA StyleHsu, C.-L., Yang, C.-H., Wang, J.-H., & Liang, C.-C. (2020). Common Running Musculoskeletal Injuries and Associated Factors among Recreational Gorge Marathon Runners: An Investigation from 2013 to 2018 Taroko Gorge Marathons. International Journal of Environmental Research and Public Health, 17(21), 8101. https://doi.org/10.3390/ijerph17218101