Associations between Household-Level Exposures and All-Cause Diarrhea and Pathogen-Specific Enteric Infections in Children Enrolled in Five Sentinel Surveillance Studies

 ,
,  , , , ,
, , , ,
Abstract
1. Introduction
2. Materials and Methods
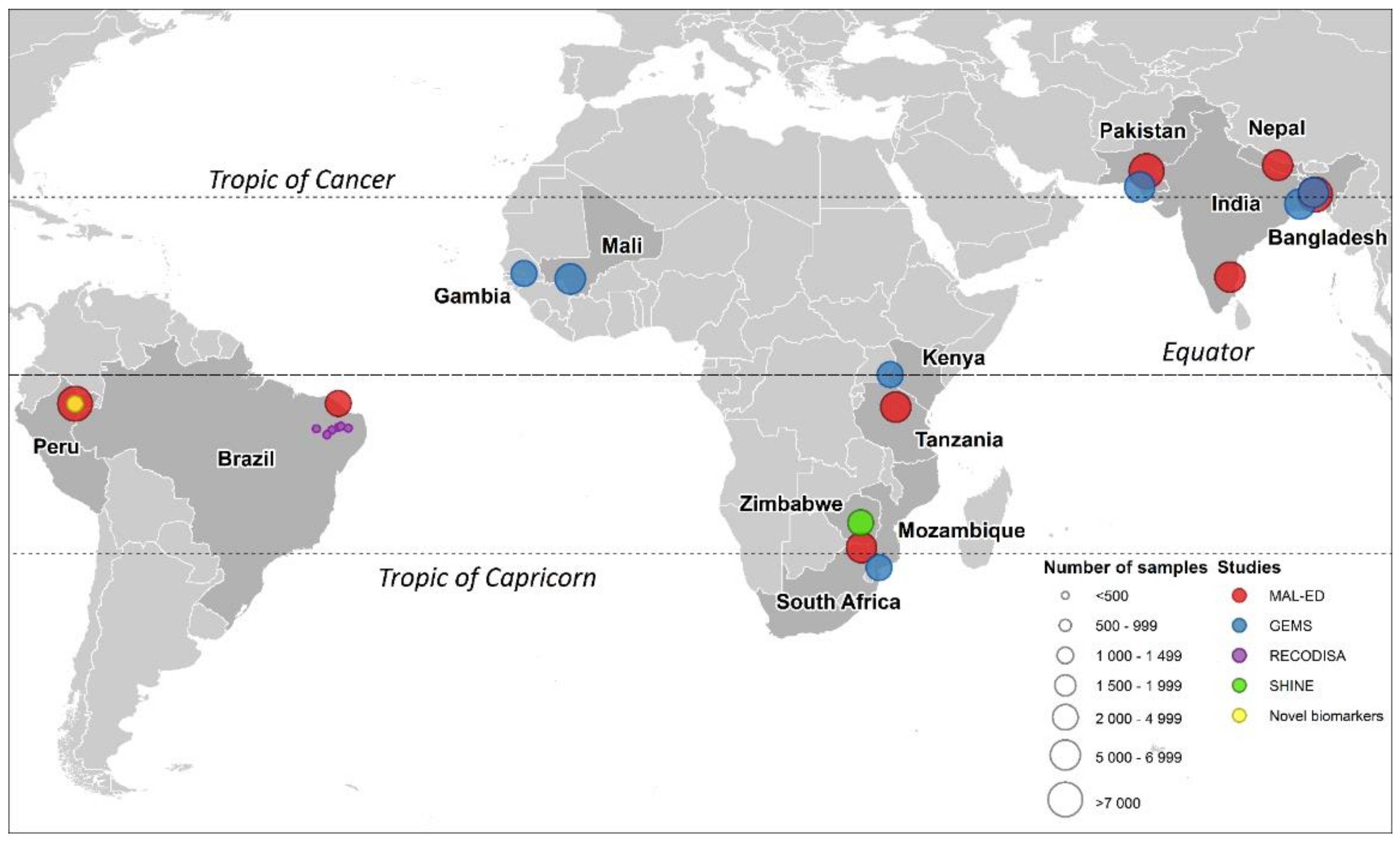
2.1. Study Population
2.2. Outcome Variable
2.3. Covariates
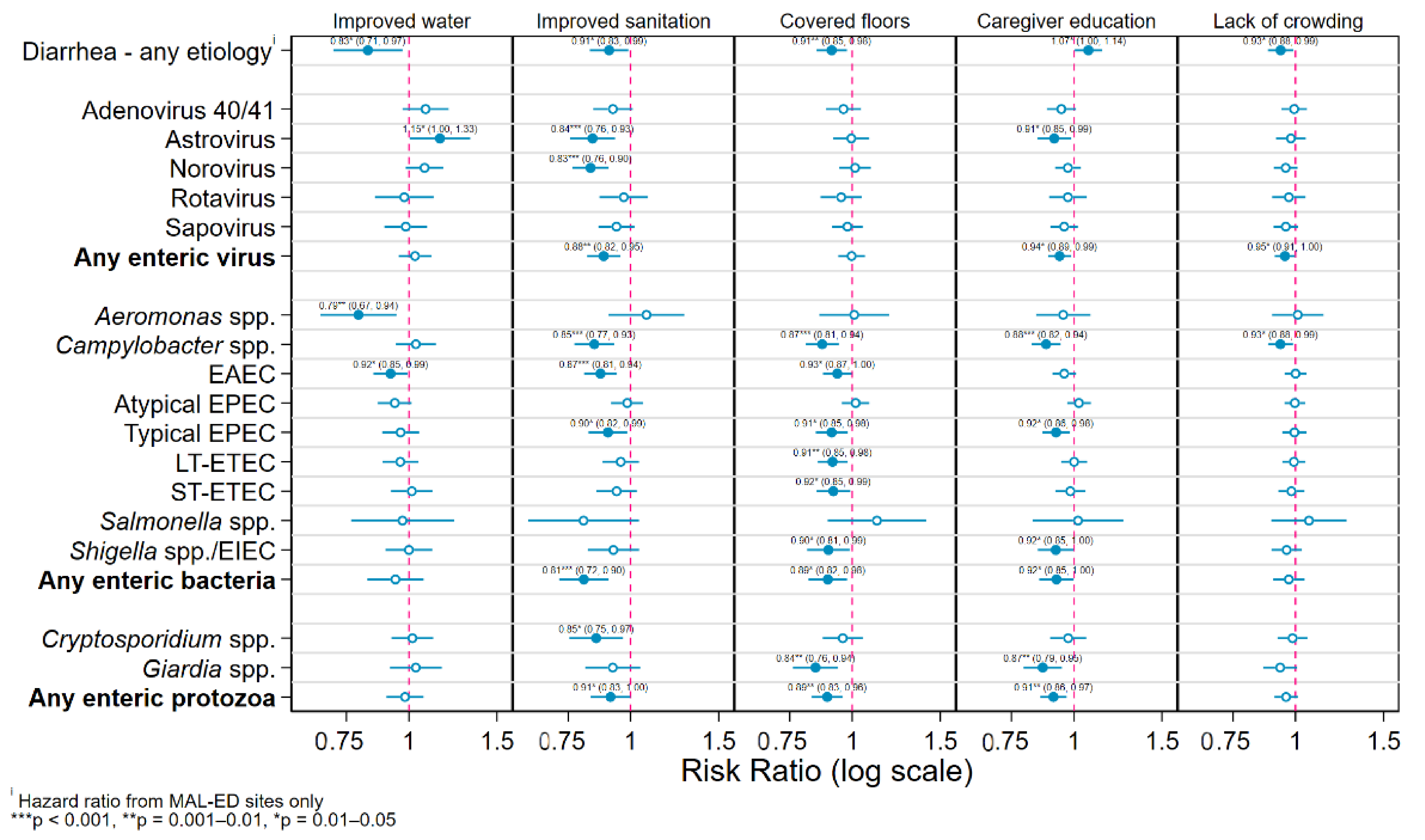
- Drinking water: whether or not the subject resided in a household with access to an improved drinking water source (with potential to deliver safe water by nature of its design and construction such as piped water or protected tubewells, boreholes, dug wells, or springs) [34].
- Sanitation: whether or not the subject resided in a household with access to an improved, non-shared sanitation facility (“improved” meaning designed to hygienically separate excreta from human contact) [34].
- Flooring material: whether or not the subject resided in a household that had a covered (“improved”—rudimentary or finished) as opposed to natural (“unimproved”—earth or sand) floor [35].
- Caregiver education: a binary variable indicating whether or not the subject’s caregiver had completed primary education (≥6 completed years of schooling [25]).
- Household crowding: a binary variable indicating whether or not the subject resided in a household with 3 or more residents per bedroom [22].
- Site: a categorical variable indicating at which of the 22 study sites the subject was enrolled, included to adjust both for between-site differences in background pathogen transmission levels and for potential confounding engendered by differences in surveillance methods between the 5 studies.
- Sample type: whether the stool sample was collected during a diarrheal episode (cases of diarrhea in GEMS and RECODISA, diarrheal collections in MAL-ED, Novel Biomarkers and SHINE) or while the subject was asymptomatic (controls in GEMS and RECODISA, surveillance samples in MAL-ED, Novel Biomarkers and SHINE).
- Age: the subjects’ age in continuous months at the time of stool sample collection, modeled using linear, quadratic, and cubic terms to account for non-linearity of association with enteric pathogen presence.
- Feeding status: a categorical variable indicating whether the child was being exclusively breastfed, partially breastfed or had been fully weaned (no longer receiving any breastmilk) at the time of sample collection.
- Nutritional status: two binary variables indicating whether or not the child was moderately or severely stunted or underweight (respectively, a length-for-age and weight-for-age Z-score of ≤−2.0) to adjust for both the impact of nutritional status on susceptibility to infections [36] and potential unobserved confounding by socio-economic status.
2.4. Statistical Methods
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Liu, L.; Oza, S.; Hogan, D.; Chu, Y.; Perin, J.; Zhu, J.; Lawn, J.E.; Cousens, S.; Mathers, C.; Black, R.E. Global, regional, and national causes of under-5 mortality in 2000–15: An updated systematic analysis with implications for the Sustainable Development Goals. Lancet 2016, 388, 3027–3035. [Google Scholar] [CrossRef]
- Kotloff, K.; Nataro, J.P.; Blackwelder, W.C.; Nasrin, D.; Farag, T.H.; Panchalingam, S.; Wu, Y.; Sow, S.; Sur, D.; Breiman, R.F.; et al. Burden and aetiology of diarrhoeal disease in infants and young children in developing countries (the Global Enteric Multicenter Study, GEMS): A prospective, case-control study. Lancet 2013, 382, 209–222. [Google Scholar] [CrossRef]
- Troeger, C.; Forouzanfar, M.; Rao, P.C.; Khalil, I.; Brown, A.; Reiner, R.C.; Fullman, N.; Thompson, R.L.; Abajobir, A.; Ahmed, M.B.; et al. Estimates of global, regional, and national morbidity, mortality, and aetiologies of diarrhoeal diseases: A systematic analysis for the Global Burden of Disease Study 2015. Lancet Infect. Dis. 2017, 17, 909–948. [Google Scholar] [CrossRef]
- McGovern, M.E.; Krishna, A.; Aguayo, V.M.; Subramanian, S.V. A review of the evidence linking child stunting to economic outcomes. Int. J. Epidemiol. 2017, 46, 1171–1191. [Google Scholar] [CrossRef] [PubMed]
- Dewey, K.G.; Begum, K. Long-term consequences of stunting in early life. Matern. Child Nutr. 2011, 7, 5–18. [Google Scholar] [CrossRef]
- Kotloff, K.L. The Burden and Etiology of Diarrheal Illness in Developing Countries. Pediatr. Clin. North Am. 2017, 64, 799–814. [Google Scholar] [CrossRef] [PubMed]
- Platts-Mills, J.A.; Liu, J.; Rogawski, E.T.; Kabir, F.; Lertsethtakarn, P.; Siguas, M.; Khan, S.S.; Praharaj, I.; Murei, A.; Nshama, R.; et al. Use of quantitative molecular diagnostic methods to assess the aetiology, burden, and clinical characteristics of diarrhoea in children in low-resource settings: A reanalysis of the MAL-ED cohort study. Lancet Glob. Health 2018, 6, e1309–e1318. [Google Scholar] [CrossRef]
- Lima, A.A.; Oliveira, D.B.; Quetz, J.S.; Havt, A.; Prata, M.M.G.; Lima, I.F.N.; Soares, A.M.; Filho, J.Q.; Lima, N.L.; Medeiros, P.H.Q.S.; et al. Etiology and severity of diarrheal diseases in infants at the semiarid region of Brazil: A case-control study. PLoS Negl. Trop. Dis. 2019, 13, e0007154. [Google Scholar] [CrossRef]
- Colston, J.M.; Francois, R.; Pisanic, N.; Yori, P.P.; McCormick, B.J.J.; Olortegui, M.P.; Gazi, A.; Svensen, E.; Ahmed, M.M.M.; Mduma, E.; et al. Effects of Child and Maternal Histo-Blood Group Antigen Status on Symptomatic and Asymptomatic Enteric Infections in Early Childhood. J. Infect. Dis. 2019, 220, 151–162. [Google Scholar] [CrossRef] [PubMed]
- Chao, D.L.; Roose, A.; Roh, M.K.; Kotloff, K.L.; Proctor, J.L. The seasonality of diarrheal pathogens: A retrospective study of seven sites over three years. PLoS Negl. Trop. Dis. 2019, 13, e0007211. [Google Scholar] [CrossRef] [PubMed]
- Eisenberg, J.N.S.; Trostle, J.; Sorensen, R.J.; Shields, K.F. Toward a systems approach to enteric pathogen transmission: From individual independence to community interdependence. Annu. Rev. Public Health 2012, 33, 239–257. [Google Scholar] [CrossRef] [PubMed]
- Lopman, B.; Gastañaduy, P.; Park, G.W.; Hall, A.J.; Parashar, U.D.; Vinjé, J. Environmental transmission of norovirus gastroenteritis. Curr. Opin. Virol. 2012, 2, 96–102. [Google Scholar] [CrossRef]
- Wolf, J.; Hunter, P.R.; Freeman, M.C.; Cumming, O.; Clasen, T.; Bartram, J.; Higgins, J.P.T.; Johnston, R.; Medlicott, K.; Boisson, S.; et al. Impact of drinking water, sanitation and handwashing with soap on childhood diarrhoeal disease: Updated meta-analysis and meta-regression. Trop. Med. Int. Health 2018, 23, 508–525. [Google Scholar] [CrossRef] [PubMed]
- Wolf, J.; Prüss-Ustün, A.; Cumming, O.; Bartram, J.; Bonjour, S.; Cairncross, S.; Clasen, T.; Colford, J.M., Jr.; Curtis, V.; De France, J.; et al. Systematic review: Assessing the impact of drinking water and sanitation on diarrhoeal disease in low- and middle-income settings: Systematic review and meta-regression. Trop. Med. Int. Health 2014, 19, 928–942. [Google Scholar] [CrossRef] [PubMed]
- Cumming, O.; Arnold, B.F.; Ban, R.; Clasen, T.F.; Mills, J.E.; Freeman, M.C.; Gordon, B.; Guiteras, R.; Howard, G.; Hunter, P.R.; et al. The implications of three major new trials for the effect of water, sanitation and hygiene on childhood diarrhea and stunting: A consensus statement. BMC Med. 2019, 17, 173. [Google Scholar] [CrossRef]
- Crawford, S.E.; Ramani, S.; Tate, J.E.; Parashar, U.D.; Svensson, L.; Hagbom, M.; Franco, M.A.; Greenberg, H.B.; O’Ryan, M.; Kang, G.; et al. Rotavirus infection. Nat. Rev. Dis. Prim. 2017, 3, 17084. [Google Scholar] [CrossRef] [PubMed]
- Lanata, C.F.; Fischer-Walker, C.L.; Olascoaga, A.C.; Torres, C.X.; Aryee, M.J.; Black, R.E.; Child Health Epidemiology Reference Group of the World Health Organization and UNICEF. Global Causes of Diarrheal Disease Mortality in Children <5 years of age: A systematic review. PLoS ONE 2013, 8, e72788. [Google Scholar] [CrossRef]
- Platts-Mills, J.A.; Rogawski, E.T.; Kosek, M.N.; Houpt, E.R. Aetiology, burden and clinical characteristics of diarrhoea in children in low-resource settings using quantitative molecular diagnostics: Results from the MAL-ED cohort study. Lancet Glob. Health 2018, in press. [Google Scholar] [CrossRef]
- Braun-Falco, M.; Mankin, H.J.; Wenger, S.L.; Kendall, S.D.; Blobe, G.C.; Weber, C.K.; Lorenz, R.; Adler, G.; Whitcomb, D.C.; Yadav, D.; et al. PAP. In Encyclopedia of Molecular Mechanisms of Disease; Springer: Berlin/Heidelberg, Germany, 2009; p. 1573. [Google Scholar]
- Null, C.; Stewart, C.P.; Pickering, A.J.; Dentz, H.N.; Arnold, B.F.; Arnold, C.D.; Benjamin-Chung, J.; Clasen, T.; Dewey, K.G.; Fernald, L.C.H.; et al. Effects of water quality, sanitation, handwashing, and nutritional interventions on diarrhoea and child growth in rural Kenya: A cluster-randomised controlled trial. Lancet Glob. Health 2018, 6, e316–e329. [Google Scholar] [CrossRef]
- Exum, N.G.; Olórtegui, M.P.; Yori, P.P.; Davis, M.F.; Heaney, C.D.; Kosek, M.N.; Schwab, K.J. Floors and Toilets: Association of Floors and Sanitation Practices with Fecal Contamination in Peruvian Amazon Peri-Urban Households. Environ. Sci. Technol. 2016, 50, 7373–7381. [Google Scholar] [CrossRef]
- Knee, J.; Sumner, T.; Adriano, Z.; Berendes, D.; De Bruijn, E.; Schmidt, W.-P.; Nalá, R.; Cumming, O.; Brown, J. Risk factors for childhood enteric infection in urban Maputo, Mozambique: A cross-sectional study. PLoS Negl. Trop. Dis. 2018, 12, e0006956. [Google Scholar] [CrossRef] [PubMed]
- Caldwell, J.C. How Is Greater Maternal Education Translated into Lower Child Mortality? Health Transit. Rev. 1994, 4, 224–229. Available online: https://www.jstor.org/stable/40652138 (accessed on 25 April 2019).
- Gakidou, E.; Cowling, K.; Lozano, R.; Murray, C.J.L. Increased educational attainment and its effect on child mortality in 175 countries between 1970 and 2009: A systematic analysis. Lancet 2010, 376, 959–974. [Google Scholar] [CrossRef]
- Graetz, N.; Friedman, J.; Osgood-Zimmerman, A.; Burstein, R.; Biehl, M.H.; Shields, C.; Mosser, J.F.; Casey, D.C.; Deshpande, A.; Earl, L.; et al. Mapping local variation in educational attainment across Africa. Nature 2018, 555, 48–53. [Google Scholar] [CrossRef]
- Basu, A.M.; Stephenson, R. Low levels of maternal education and the proximate determinants of childhood mortality: A little learning is not a dangerous thing. Soc. Sci. Med. 2005, 60, 2011–2023. [Google Scholar] [CrossRef]
- World Health Organization. WHO Housing and Health Guidelines; World Health Organization: Geneva, Switzerland, 2018; Available online: http://apps.who.int/bookorders (accessed on 28 September 2020).
- Berendes, D.; Leon, J.; Kirby, A.E.; Clennon, J.; Raj, S.; Yakubu, H.; Robb, K.; Kartikeyan, A.; Hemavathy, P.; Gunasekaran, A.; et al. Household sanitation is associated with lower risk of bacterial and protozoal enteric infections, but not viral infections and diarrhoea, in a cohort study in a low-income urban neighbourhood in Vellore, India. Trop. Med. Int. Health 2017, 22, 1119–1129. [Google Scholar] [CrossRef]
- McQuade, E.T.R.; Platts-Mills, J.A.; Gratz, J.; Zhang, J.; Moulton, L.H.; Mutasa, K.; Majo, F.D.; Tavengwa, N.; Ntozini, R.; Prendergast, A.J.; et al. Impact of Water Quality, Sanitation, Handwashing, and Nutritional Interventions on Enteric Infections in Rural Zimbabwe: The Sanitation Hygiene Infant Nutrition Efficacy (SHINE) Trial. J. Infect. Dis. 2019. [Google Scholar] [CrossRef]
- MAL-ED. The Interactions of Malnutrition and Enteric Infections: Consequences for Child Health and Development. 2015. Available online: http://mal-ed.fnih.org/ (accessed on 25 October 2015).
- Kotloff, K.; Blackwelder, W.C.; Nasrin, D.; Nataro, J.P.; Farag, T.H.; Van Eijk, A.M.; Adegbola, R.A.; Alonso, P.L.; Breiman, R.F.; Faruque, A.S.G.; et al. The Global Enteric Multicenter Study (GEMS) of Diarrheal Disease in Infants and Young Children in Developing Countries: Epidemiologic and Clinical Methods of the Case/Control Study. Clin. Infect. Dis. 2012, 55, S232–S245. [Google Scholar] [CrossRef]
- Humphrey, J.H.; Jones, A.D.; Manges, A.; Mangwadu, G.; Maluccio, J.A.; Mbuya, M.N.N.; Moulton, L.H.; Ntozini, R.; Prendergast, A.J.; The Sanitation Hygiene Infant Nutrition Efficacy (SHINE) Trial Team; et al. The Sanitation Hygiene Infant Nutrition Efficacy (SHINE) Trial: Rationale, Design, and Methods. Clin. Infect. Dis. 2015, 61, S685–S702. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Gratz, J.; Amour, C.; Nshama, R.; Walongo, T.; Maro, A.; Mduma, E.; Platts-Mills, J.; Boisen, N.; Nataro, J.; et al. Optimization of Quantitative PCR Methods for Enteropathogen Detection. PLoS ONE 2016, 11, e0158199. [Google Scholar] [CrossRef]
- World Health Organization. UNICEF. Joint Monitoring Programme (JMP) for Water Supply and Sanitation. 2019. Available online: https://washdata.org/ (accessed on 26 April 2013).
- Florey, L.; Taylor, C. Using Household Survey Data to Explore the Effects of Improved Housing Conditions on Malaria Infection in Children in Sub-Saharan Africa; ICF International: Rockville, MD, USA, 2016; Available online: https://dhsprogram.com/publications/publication-AS61-Analytical-Studies.cfm (accessed on 30 May 2019).
- Tickell, K.D.; Sharmin, R.; Deichsel, E.L.; Lamberti, L.M.; Walson, J.L.; Faruque, A.S.G.; Pavlinac, P.B.; Kotloff, K.L.; Chisti, M.J. The effect of acute malnutrition on enteric pathogens, moderate-to-severe diarrhoea, and associated mortality in the Global Enteric Multicenter Study cohort: A post-hoc analysis. Lancet Glob. Health 2020, 8, e215–e224. [Google Scholar] [CrossRef]
- Zou, G.Y. A modified poisson regression approach to prospective studies with binary data. Am. J. Epidemiol. 2004, 159, 702–706. [Google Scholar] [CrossRef]
- StataCorp. Stata Statistical Software: Release 16; StataCorp LLC: College Station, TX, USA, 2019. [Google Scholar]
- Brown, J.; Cumming, O. Perspective Piece Stool-Based Pathogen Detection Offers Advantages as an Outcome Measure for Water, Sanitation, and Hygiene Trials. Am. J. Trop. Med. Hyg. 2019, 102, 1–2. [Google Scholar] [CrossRef]
- Humphrey, J.H.; Mbuya, M.N.N.; Ntozini, R.; Moulton, L.H.; Stoltzfus, R.J.; Tavengwa, N.V.; Mutasa, K.; Majo, F.; Mutasa, B.; Mangwadu, G.; et al. Independent and combined effects of improved water, sanitation, and hygiene, and improved complementary feeding, on child stunting and anaemia in rural Zimbabwe: A cluster-randomised trial. Lancet Glob. Health 2019, 7, e132–e147. [Google Scholar] [CrossRef]
- Berendes, D.; Leon, J.S.; Kirby, A.E.; Clennon, J.A.; Raj, S.J.; Yakubu, H.; Robb, K.A.; Kartikeyan, A.; Hemavathy, P.; Gunasekaran, A.; et al. Associations between open drain flooding and pediatric enteric infections in the MAL-ED cohort in a low-income, urban neighborhood in Vellore, India. BMC Public Health 2019, 19, 926. [Google Scholar] [CrossRef] [PubMed]
- Qamar, F.N.; Nisar, M.I.; Quadri, F.; Shakoor, S.; Sow, S.; Nasrin, D.; Blackwelder, W.C.; Wu, Y.; Farag, T.; Panchalingham, S.; et al. Aeromonas-Associated Diarrhea in Children under 5 Years: The GEMS Experience. Am. J. Trop. Med. Hyg. 2016, 95, 774–780. [Google Scholar] [CrossRef]
- George, C.M.; Perin, J.; Talukder, K.A.; Biswas, S.K.; Oldja, L.; Azmi, I.J.; Faruque, A.G.; Bhuyian, S.I.; Parvin, T.; Sack, R.B.; et al. Fecal Markers of Environmental Enteropathy are Associated with Animal Exposure and Caregiver Hygiene in Bangladesh. Am. J. Trop. Med. Hyg. 2015, 93, 269–275. [Google Scholar] [CrossRef]
- Whiley, H.; Akker, B.V.D.; Giglio, S.; Bentham, R. The Role of Environmental Reservoirs in Human Campylobacteriosis. Int. J. Environ. Res. Public Health 2013, 10, 5886–5907. [Google Scholar] [CrossRef]
- Marquis, G.S.; Ventura, G.; Gilman, R.H.; Porras, E.; Miranda, E.; Carbajal, L.; Pentafiel, M. Fecal contamination of shanty town toddlers in households with non-corralled poultry, Lima, Peru. Am. J. Public Health 1990, 80, 146–149. [Google Scholar] [CrossRef]
- Berrang, M.E.; Northcutt, J.K.; Cason, J.A. Recovery of Campylobacter from Broiler Feces During Extended Storage of Transport Cages. Poult. Sci. 2004, 83, 1213–1217. [Google Scholar] [CrossRef]
- Carron, M.; Chang, Y.-M.; Momanyi, K.; Akoko, J.; Kiiru, J.; Bettridge, J.; Chaloner, G.; Rushton, J.; O’Brien, S.; Williams, N.J.; et al. Campylobacter, a zoonotic pathogen of global importance: Prevalence and risk factors in the fast-evolving chicken meat system of Nairobi, Kenya. PLoS Negl. Trop. Dis. 2018, 12, e0006658. [Google Scholar] [CrossRef]
- Cardinale, E.; Tall, F.; Guèye, E.; Cisse, M.; Salvat, G. Risk factors for Campylobacter spp. infection in Senegalese broiler-chicken flocks. Prev. Vet. Med. 2004, 64, 15–25. Available online: https://linkinghub.elsevier.com/retrieve/pii/S016758770400087X (accessed on 8 April 2020). [CrossRef] [PubMed]
- Ngure, F.; Gelli, A.; Becquey, E.; Ganaba, R.; Headey, D.; Huybregts, L.; Pedehombga, A.; Sanou, A.; Traore, A.; Zongo, F.; et al. Exposure to Livestock Feces and Water Quality, Sanitation, and Hygiene (WASH) Conditions among Caregivers and Young Children: Formative Research in Rural Burkina Faso. Am. J. Trop. Med. Hyg. 2019, 100, 998–1004. [Google Scholar] [CrossRef]
- Sultana, R.; Nahar, N.; Rimi, N.A.; Azad, S.; Islam, M.S.; Gurley, E.S.; Luby, S.P. Backyard poultry raising in Bangladesh: A valued resource for the villagers and a setting for zoonotic transmission of avian influenza. A qualitative study. Rural. Remote Health 2012, 12, 1927. [Google Scholar]
- Penakalapati, G.; Swarthout, J.; Delahoy, M.J.; McAliley, L.; Wodnik, B.; Levy, K.; Freeman, M.C. Exposure to Animal Feces and Human Health: A Systematic Review and Proposed Research Priorities. Environ. Sci. Technol. 2017, 51, 11537–11552. [Google Scholar] [CrossRef] [PubMed]
- Psaki, S.R.; Seidman, J.C.; Miller, M.A.; Gottlieb, M.; A Bhutta, Z.; Ahmed, T.; Ahmed, A.S.; Bessong, P.O.; John, S.; Kang, G.; et al. Measuring socioeconomic status in multicountry studies: Results from the eight-country MAL-ED study. Popul. Health Metrics 2014, 12, 8. [Google Scholar] [CrossRef]
- Rosenbaum, P.R.; Rubin, D.B. The Central Role of the Propensity Score in Observational Studies for Causal Effects. Biom. JSTOR 1983, 70, 41. [Google Scholar] [CrossRef]
- Clasen, T.F.; Alexander, K.T.; Sinclair, D.; Boisson, S.; Peletz, R.; Chang, H.H.; Majorin, F.; Cairncross, S. Interventions to improve water quality for preventing diarrhoea. Cochrane Database Syst. Rev. 2015, 1–201. [Google Scholar] [CrossRef] [PubMed]
- Burnett, E.; Jonesteller, C.L.; Tate, J.E.; Yen, C.; Parashar, U.D. Global Impact of Rotavirus Vaccination on Childhood Hospitalizations and Mortality From Diarrhea. J. Infect. Dis. 2017, 215, 1666–1672. [Google Scholar] [CrossRef]
- Colston, J.; Olortegui, M.P.; Zaitchik, B.F.; Yori, P.P.; Kang, G.; Ahmed, T.; Bessong, P.O.; Mduma, E.; Bhutta, Z.A.; Shrestha, P.S.; et al. Pathogen-Specific Impacts of the 2011–2012 La Niña-Associated Floods on Enteric Infections in the MAL-ED Peru Cohort: A Comparative Interrupted Time Series Analysis. Int. J. Environ. Res. Public Health 2020, 17, 487. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Adenovirus 40/41 | Astrovirus | Norovirus | Rotavirus | Sapovirus | Aeromonas spp. | Campylo-bacter spp. | EAEC | |
|---|---|---|---|---|---|---|---|---|
| Bamako, Mali | 460 (26.3) | 136 (7.7) | 351 (19.9) | 216 (12.3) | 238 (13.5) | 41 (2.3) | 899 (50.8) | 1151 (65.1) |
| Basse, The Gambia | 373 (25.4) | 98 (6.4) | 250 (16.3) | 227 (14.8) | 201 (13.1) | 19 (1.3) | 787 (52.2) | 873 (58.7) |
| Bhaktapur, Nepal | 348 (5.9) | 301 (5.1) | 714 (12.0) | 249 (4.2) | 651 (11.1) | 149 (2.5) | 1256 (22.3) | 2690 (47.0) |
| Cajazeiras, Brazil | 1 (0.5) | 9 (4.5) | 8 (4.0) | 12 (6.0) | 9 (4.5) | 6 (3.0) | 6 (3.0) | 68 (34.0) |
| Crato, Brazil | 5 (2.5) | 4 (2.0) | 2 (1.0) | 46 (23.0) | 6 (3.0) | 12 (6.0) | 26 (13.0) | 83 (41.5) |
| Dhaka, Bangladesh | 1306 (23.5) | 1142 (20.3) | 1086 (19.0) | 578 (10.2) | 1054 (18.8) | 162 (2.8) | 1730 (33.8) | 2245 (41.1) |
| Fortaleza, Brazil | 137 (4.7) | 52 (1.8) | 187 (6.4) | 40 (1.5) | 132 (4.5) | 40 (1.4) | 401 (13.8) | 883 (30.1) |
| Haydom, Tanzania | 365 (8.3) | 282 (6.4) | 735 (16.6) | 227 (5.2) | 482 (11.0) | 131 (3.0) | 1818 (45.9) | 2843 (65.1) |
| Karachi, Pakistan | 366 (22.4) | 191 (11.6) | 393 (23.8) | 161 (9.8) | 306 (18.5) | 122 (7.5) | 1023 (62.9) | 1132 (68.9) |
| Kolkota, India | 734 (41.5) | 101 (5.8) | 316 (18.0) | 321 (18.3) | 201 (11.4) | 193 (10.9) | 824 (46.6) | 1028 (58.1) |
| Loreto, Peru | 1380 (21.0) | 1049 (15.7) | 1230 (18.0) | 261 (4.0) | 975 (14.9) | 177 (2.6) | 1293 (20.3) | 3174 (55.6) |
| Manhiça, Mozambique | 377 (36.3) | 41 (4.0) | 151 (14.7) | 202 (19.7) | 120 (11.7) | 50 (4.8) | 462 (44.5) | 817 (78.7) |
| Midlands, Zimbabwe | 198 (8.3) | 66 (2.8) | 277 (11.7) | 122 (5.1) | 155 (6.5) | 36 (1.5) | 602 (25.5) | 1361 (57.6) |
| Mirzapur, Bangladesh | 443 (24.7) | 89 (5.0) | 243 (13.6) | 392 (21.9) | 183 (10.2) | 59 (3.3) | 434 (24.2) | 992 (55.3) |
| N. Feroze, Pakistan | 823 (12.8) | 930 (14.6) | 1388 (21.4) | 274 (4.2) | 1063 (16.6) | 35 (0.5) | 1667 (27.0) | 2288 (36.5) |
| Nyanza, Kenya | 165 (9.1) | 61 (3.4) | 250 (13.9) | 160 (9.0) | 179 (10.0) | 109 (6.0) | 662 (36.5) | 952 (53.1) |
| Ouricuri, Brazil | 7 (3.5) | 9 (4.5) | 12 (6.0) | 5 (2.5) | 6 (3.0) | 11 (5.5) | 17 (8.5) | 52 (26.1) |
| Patos, Brazil | 6 (3.0) | 0 (0.0) | 4 (2.0) | 6 (3.0) | 1 (0.5) | 3 (1.5) | 10 (5.0) | 194 (97.0) |
| Picos, Brazil | 3 (1.8) | 0 (0.0) | 0 (0.0) | 14 (8.5) | 8 (4.9) | 2 (1.0) | 15 (7.5) | 92 (46.0) |
| Souza, Brazil | 2 (1.0) | 0 (0.0) | 10 (5.1) | 3 (1.5) | 5 (2.5) | 2 (1.1) | 12 (6.3) | 161 (83.9) |
| Vellore, India | 921 (17.1) | 622 (11.6) | 822 (15.2) | 434 (8.1) | 789 (14.7) | 275 (5.1) | 1144 (22.0) | 3283 (62.5) |
| Venda, South Africa | 503 (10.7) | 332 (7.1) | 529 (11.2) | 92 (2.1) | 517 (11.0) | 24 (0.5) | 535 (11.4) | 1698 (36.0) |
| Total positive | 8923 (15.7) | 5515 (9.7) | 8958 (15.6) | 4042 (7.2) | 7281 (12.8) | 1658 (2.9) | 15,623 (28.4) | 28,060 (50.8) |
| Total stools | 56,704 | 56,828 | 57,350 | 56,168 | 56,668 | 57,185 | 54,923 | 55,280 |
| Atypical EPEC | Typical EPEC | LT-ETEC | ST-ETEC | Salmonella spp. | Shigella spp./EIEC | Crypto-sporidium spp. | Giardia spp. | |
| Bamako, Mali | 382 (21.6) | 588 (33.2) | 511 (29.0) | 319 (18.1) | 52 (2.9) | 567 (32.1) | 522 (29.5) | 1233 (70.8) |
| Basse, The Gambia | 330 (22.0) | 461 (30.8) | 370 (24.8) | 289 (19.3) | 82 (5.5) | 480 (32.7) | 279 (18.5) | 630 (42.4) |
| Bhaktapur, Nepal | 1673 (28.5) | 403 (6.8) | 575 (9.7) | 620 (10.5) | 55 (0.9) | 376 (6.3) | 272 (4.6) | 545 (10.3) |
| Cajazeiras, Brazil | 34 (17.0) | 3 (1.5) | 7 (3.5) | 0 (0.0) | 7 (3.5) | 10 (5.1) | 24 (12.1) | 66 (33.3) |
| Crato, Brazil | 66 (33.0) | 13 (6.5) | 33 (16.5) | 0 (0.0) | 78 (39.0) | 76 (38.0) | 13 (6.5) | 55 (27.5) |
| Dhaka, Bangladesh | 1328 (23.6) | 1075 (19.1) | 849 (15.0) | 1799 (32.6) | 57 (1.0) | 865 (15.4) | 380 (6.8) | 661 (12.8) |
| Fortaleza, Brazil | 764 (25.9) | 100 (3.4) | 129 (4.4) | 73 (2.5) | 27 (0.9) | 158 (5.4) | 37 (1.3) | 266 (9.7) |
| Haydom, Tanzania | 1266 (28.6) | 821 (18.6) | 1141 (26.1) | 1242 (28.3) | 19 (0.4) | 790 (17.9) | 514 (12.0) | 931 (27.3) |
| Karachi, Pakistan | 358 (21.8) | 545 (33.2) | 404 (24.7) | 356 (21.8) | 22 (1.3) | 543 (32.9) | 383 (23.4) | 931 (57.0) |
| Kolkota, India | 519 (29.4) | 367 (20.8) | 392 (22.2) | 293 (16.6) | 23 (1.3) | 533 (30.1) | 275 (15.6) | 1076 (62.2) |
| Loreto, Peru | 1548 (24.1) | 807 (12.1) | 1137 (17.2) | 763 (11.4) | 85 (1.3) | 786 (11.8) | 633 (9.6) | 1415 (26.1) |
| Manhiça, Mozambique | 279 (26.9) | 318 (30.7) | 280 (27.0) | 329 (31.7) | 41 (4.0) | 328 (31.6) | 323 (31.2) | 726 (70.9) |
| Midlands, Zimbabwe | 608 (25.7) | 219 (9.2) | 464 (19.6) | 231 (9.7) | 42 (1.8) | 93 (3.9) | 210 (8.9) | 348 (15.1) |
| Mirzapur, Bangladesh | 430 (24.0) | 209 (11.6) | 337 (18.8) | 95 (5.3) | 22 (1.2) | 648 (36.1) | 80 (4.5) | 377 (21.1) |
| N. Feroze, Pakistan | 869 (13.4) | 683 (10.6) | 578 (8.9) | 605 (9.4) | 4 (0.1) | 445 (6.9) | 402 (6.3) | 1585 (34.4) |
| Nyanza, Kenya | 453 (25.0) | 440 (24.3) | 555 (31.0) | 278 (15.3) | 39 (2.1) | 421 (23.2) | 336 (18.5) | 735 (40.8) |
| Ouricuri, Brazil | 27 (13.6) | 1 (0.5) | 6 (3.0) | 0 (0.0) | 28 (14.0) | 22 (11.0) | 1 (0.5) | 22 (11.0) |
| Patos, Brazil | 76 (38.0) | 4 (2.0) | 17 (8.5) | 7 (3.5) | 13 (6.5) | 8 (4.0) | 10 (5.0) | 21 (10.6) |
| Picos, Brazil | 21 (10.5) | 5 (2.5) | 5 (2.5) | 0 (0.0) | 26 (13.0) | 21 (10.5) | 11 (5.5) | 58 (29.0) |
| Souza, Brazil | 86 (44.8) | 3 (1.6) | 12 (6.3) | 5 (2.6) | 17 (8.9) | 10 (5.3) | 17 (8.9) | 30 (15.8) |
| Vellore, India | 1440 (26.7) | 870 (16.2) | 877 (16.4) | 717 (13.4) | 67 (1.2) | 701 (13.0) | 278 (5.2) | 1039 (23.2) |
| Venda, South Africa | 945 (20.1) | 212 (4.5) | 346 (7.4) | 194 (4.2) | 14 (0.3) | 337 (7.2) | 226 (4.9) | 704 (16.2) |
| Total positive | 13,502 (23.8) | 8147 (14.3) | 9025 (15.9) | 8215 (14.5) | 820 (1.4) | 8218 (14.4) | 5226 (9.3) | 13,454 (26.8) |
| Total stools | 56,713 | 56,943 | 56,832 | 56,842 | 57,154 | 56,930 | 56,485 | 50,177 |
| Improved Water Source | Improved Sanitation | Improved Flooring | Caregiver Education | Household Crowding | Total Subjects | |
|---|---|---|---|---|---|---|
| Bamako, Mali | 5872 (87.5) | 127 (1.9) | 5253 (98.5) | 1242 (31.4) | 3119 (58.5) | 6711 |
| Basse, The Gambia | 4087 (86.3) | 82 (1.7) | 2837 (85.0) | 1029 (42.4) | 2987 (89.5) | 4738 |
| Bhaktapur, Nepal | 232 (98.3) | 131 (55.5) | 104 (44.1) | 152 (64.4) | 47 (19.9) | 240 |
| Cajazeiras, Brazil | 172 (86.0) | 197 (98.5) | 198 (99.0) | 137 (68.5) | - | 200 |
| Crato, Brazil | 189 (94.5) | 181 (90.5) | 170 (87.2) | 169 (84.9) | - | 200 |
| Dhaka, Bangladesh | 242 (100.0) | 28 (11.6) | 226 (93.4) | 57 (23.6) | 3 (1.2) | 265 |
| Fortaleza, Brazil | 142 (67.6) | 201 (95.7) | 208 (99.0) | 146 (69.5) | 6 (2.9) | 233 |
| Haydom, Tanzania | 79 (31.6) | 0 (0.0) | 17 (6.8) | 6 (2.4) | 23 (9.2) | 262 |
| Karachi, Pakistan | 3274 (62.6) | 2428 (46.4) | 2881 (75.6) | 1120 (37.8) | 443 (11.6) | 5231 |
| Kolkata, India | 5147 (98.7) | 635 (12.2) | 3877 (95.9) | 1880 (64.2) | 160 (4.0) | 5214 |
| Loreto, Peru | 309 (89.6) | 70 (20.3) | 98 (28.4) | 192 (56.3) | 45 (13.0) | 378 |
| Manhiça, Mozambique | 2745 (85.1) | 219 (6.8) | 1691 (70.1) | 454 (24.7) | 417 (17.4) | 3227 |
| Midlands, Zimbabwe | 611 (61.8) | 619 (61.2) | 547 (55.2) | 844 (82.6) | - | 1046 |
| Mirzapur, Bangladesh | 5907 (99.8) | 2830 (47.8) | 887 (20.8) | 2662 (75.3) | 769 (18.0) | 5916 |
| Naushahro Feroze, Pakistan | 265 (100.0) | 9 (3.4) | 74 (27.9) | 41 (15.5) | 55 (20.8) | 277 |
| Nyanza, Kenya | 2549 (64.5) | 169 (4.3) | 659 (19.5) | 1630 (52.9) | 34 (1.0) | 3951 |
| Ouricuri, Brazil | 193 (96.5) | 195 (97.5) | 195 (98.0) | 142 (71.0) | - | 200 |
| Patos, Brazil | 199 (100.0) | 197 (98.5) | 198 (99.5) | 139 (70.6) | - | 200 |
| Picos, Brazil | 198 (99.5) | 193 (96.5) | 192 (96.5) | 129 (64.5) | - | 200 |
| Souza, Brazil | 200 (100.0) | 181 (90.5) | 198 (99.0) | 125 (62.5) | - | 200 |
| Vellore, India | 235 (100.0) | 12 (5.1) | 220 (93.6) | 123 (52.3) | 1 (0.4) | 251 |
| Venda, South Africa | 216 (85.4) | 3 (1.2) | 233 (92.1) | 207 (81.8) | 62 (24.5) | 314 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Colston, J.M.; Faruque, A.S.G.; Hossain, M.J.; Saha, D.; Kanungo, S.; Mandomando, I.; Nisar, M.I.; Zaidi, A.K.M.; Omore, R.; Breiman, R.F.; et al. Associations between Household-Level Exposures and All-Cause Diarrhea and Pathogen-Specific Enteric Infections in Children Enrolled in Five Sentinel Surveillance Studies. Int. J. Environ. Res. Public Health 2020, 17, 8078. https://doi.org/10.3390/ijerph17218078
Colston JM, Faruque ASG, Hossain MJ, Saha D, Kanungo S, Mandomando I, Nisar MI, Zaidi AKM, Omore R, Breiman RF, et al. Associations between Household-Level Exposures and All-Cause Diarrhea and Pathogen-Specific Enteric Infections in Children Enrolled in Five Sentinel Surveillance Studies. International Journal of Environmental Research and Public Health. 2020; 17(21):8078. https://doi.org/10.3390/ijerph17218078
Chicago/Turabian StyleColston, Josh M., Abu S. G. Faruque, M. Jahangir Hossain, Debasish Saha, Suman Kanungo, Inácio Mandomando, M. Imran Nisar, Anita K. M. Zaidi, Richard Omore, Robert F. Breiman, and et al. 2020. "Associations between Household-Level Exposures and All-Cause Diarrhea and Pathogen-Specific Enteric Infections in Children Enrolled in Five Sentinel Surveillance Studies" International Journal of Environmental Research and Public Health 17, no. 21: 8078. https://doi.org/10.3390/ijerph17218078
APA StyleColston, J. M., Faruque, A. S. G., Hossain, M. J., Saha, D., Kanungo, S., Mandomando, I., Nisar, M. I., Zaidi, A. K. M., Omore, R., Breiman, R. F., Sow, S. O., Roose, A., Levine, M. M., Kotloff, K. L., Ahmed, T., Bessong, P., Bhutta, Z., Mduma, E., Penatero Yori, P., ... Kosek, M. N. (2020). Associations between Household-Level Exposures and All-Cause Diarrhea and Pathogen-Specific Enteric Infections in Children Enrolled in Five Sentinel Surveillance Studies. International Journal of Environmental Research and Public Health, 17(21), 8078. https://doi.org/10.3390/ijerph17218078