Potential Effects on Travelers’ Air Pollution Exposure and Associated Mortality Estimated for a Mode Shift from Car to Bicycle Commuting

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Defining Current and Alternative Modes of Commuting
2.1.1. Current Modes of Travel
2.1.2. Mode-Shift Scenario
2.2. Vehicle Emissions
2.3. Dispersion and Exposure Modeling
2.4. Estimation of Dose among Bicyclists and Motorists
2.5. Health Impact Calculations
3. Results
3.1. Effects on Mode of Commuting
3.2. Effects on NOx and BC (Black Carbon) Concentrations
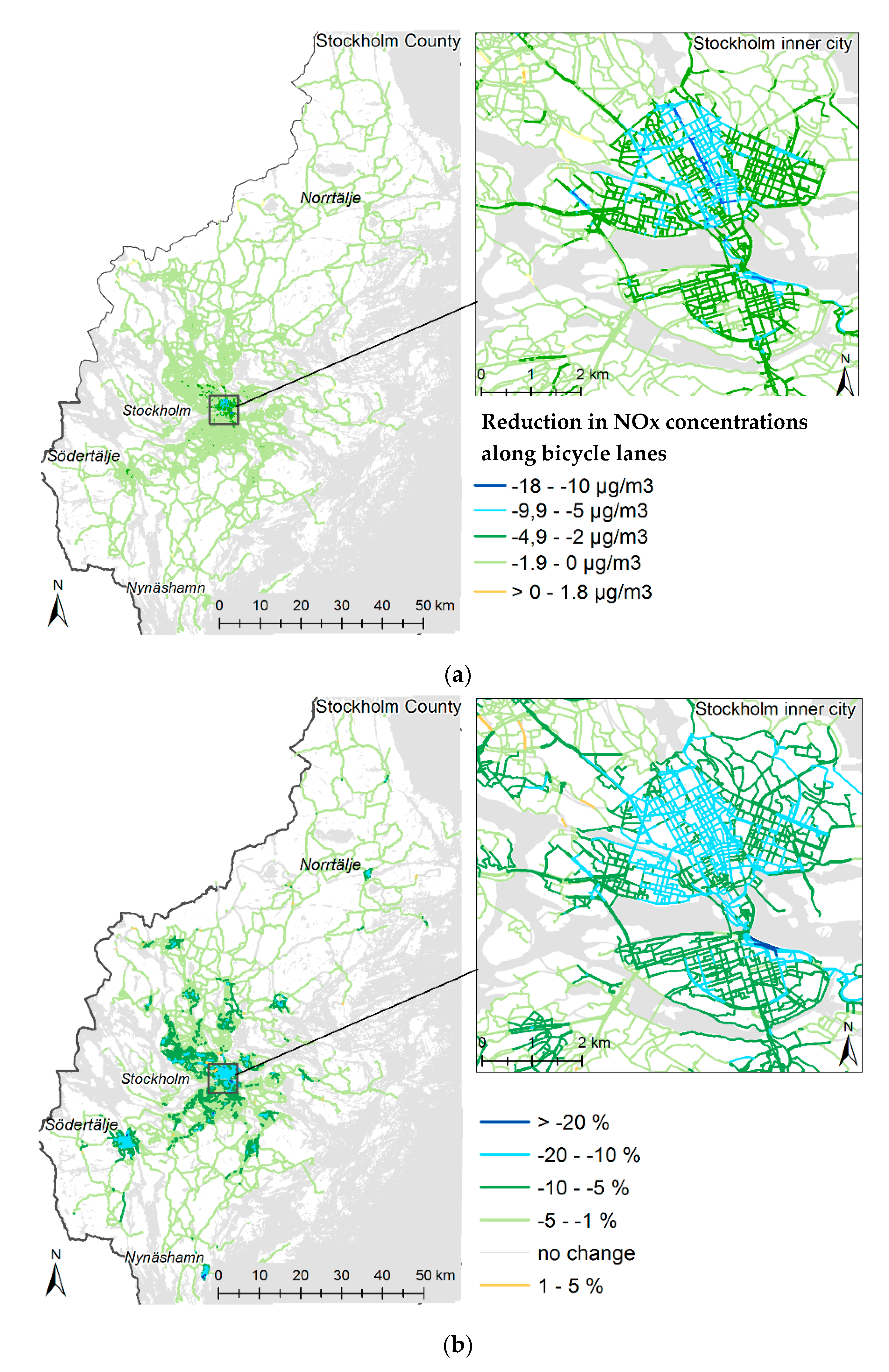
3.2.1. NOx
3.2.2. BC
3.3. Effects on NOx and BC Doses
3.3.1. NOx
3.3.2. BC
3.4. Impact on Mortality Related to Changed NOx and BC Exposure among Bicyclists
3.4.1. NOx
3.4.2. BC
3.5. Counterfactual Exposures
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Dons, E.; Panis, L.I.; Van Poppel, M.; Theunis, J.; Wets, G. Personal exposure to black carbon in transport microenvironments. Atmos. Environ. 2012, 55, 392–398. [Google Scholar] [CrossRef]
- Hanninen, O.O.; Alm, S.; Katsouyanni, K.; Kunzli, N.; Maroni, M.; Nieuwenhuijsen, M.J.; Saarela, K.; Sram, R.J.; Zmirou, D.; Jantunen, M.J. The EXPOLIS study: Implications for exposure research and environmental policy in Europe. J. Expo. Anal. Environ. Epidemiol. 2004, 14, 440–456. [Google Scholar] [CrossRef] [PubMed]
- Engstrom, E.; Forsberg, B. Health impacts of active commuters’ exposure to traffic-related air pollution in Stockholm, Sweden. J. Transp. Health 2019, 14, 100601. [Google Scholar] [CrossRef]
- de Nazelle, A.; Bode, O.; Orjuela, J.P. Comparison of air pollution exposures in active vs. passive travel modes in European cities: A quantitative review. Environ. Int. 2017, 99, 151–160. [Google Scholar] [CrossRef] [PubMed]
- Bigazzi, A.Y.; Figliozzi, M.A. Review of urban bicyclists’ intake and uptake of traffic-related air pollution. Transp. Rev. 2014, 34, 221–245. [Google Scholar] [CrossRef]
- Cepeda, M.; Schoufour, J.; Freak-Poli, R.; Koolhaas, C.M.; Dhana, K.; Bramer, W.M.; Franco, O.H. Levels of ambient air pollution according to mode of transport: A systematic review. Lancet Public Health 2017, 2, E23–E34. [Google Scholar] [CrossRef]
- Daigle, C.C.; Chalupa, D.C.; Gibb, F.R.; Morrow, P.E.; Oberdorster, G.; Utell, M.J.; Frampton, M.W. Ultrafine particle deposition in humans during rest and exercise. Inhal. Toxicol. 2003, 15, 539–552. [Google Scholar] [CrossRef]
- Mueller, N.; Rojas-Rueda, D.; Salmon, M.; Martinez, D.; Ambros, A.; Brand, C.; de Nazelle, A.; Dons, E.; Gaupp-Berghausen, M.; Gerike, R.; et al. Health impact assessment of cycling network expansions in European cities. Prev. Med. 2018, 109, 62–70. [Google Scholar] [CrossRef]
- Rojas-Rueda, D.; de Nazelle, A.; Tainio, M.; Nieuwenhuijsen, M.J. The health risks and benefits of cycling in urban environments compared with car use: Health impact assessment study. BMJ 2011, 343, d4521. [Google Scholar] [CrossRef]
- Woodcock, J.; Tainio, M.; Cheshire, J.; O’Brien, O.; Goodman, A. Health effects of the London bicycle sharing system: Health impact modelling study. BMJ 2014, 348, 425. [Google Scholar] [CrossRef]
- de Hartog, J.J.; Boogaard, H.; Nijland, H.; Hoek, G. Do the health benefits of cycling outweigh the risks? Environ. Health Perspect. 2010, 118, 1109–1116. [Google Scholar] [CrossRef] [PubMed]
- The Swedish National Travel Survey (RVU Sweden). Available online: https://www.trafa.se/en/travel-survey/ (accessed on 14 October 2020).
- Jonsson, D.; Berglund, S.; Almstrom, P.; Algers, S. The usefulness of transport models in Swedish planning practice. Transp. Rev. 2011, 31, 251–265. [Google Scholar] [CrossRef]
- Stjernström, O. The ASTRID database and population geography (only in swedish “databasen ASTRID och befolkningsgeografi—Exemplen integration och barnfamiljernas geografi”). Geogr. Not. 2011, 69, 79–86. [Google Scholar]
- Schantz, P. Distance, duration, and velocity in cycle commuting: Analyses of relations and determinants of velocity. Int. J. Environ. Res. Public Health 2017, 14, 1166. [Google Scholar] [CrossRef]
- Schantz, P.; Stigell, E. A criterion method for measuring route distance in physically active commuting. Med. Sci. Sport Exerc. 2009, 41, 472–478. [Google Scholar] [CrossRef]
- Schantz, P.; Wahlgren, L.; Eriksson, J.S.; Sommar, J.N.; Rosdahl, H. Estimating duration-distance relations in cycle commuting in the general population. PLoS ONE 2018, 13, e0207573. [Google Scholar] [CrossRef]
- Trafikverket. Road Data Overview, Trafikverket, Road and Railway Data. 2015. Available online: http://www.nvdb.se/globalassets/upload/styrande-och-vagledande-dokument/eng/road-data-overview.pdf (accessed on 14 October 2020).
- Johansson, C.; Eneroth, K.; Lövenheim, B.; Silvergren, S.; Burman, L.; Bergström, S.; Norman, M.; Engström Nylén, A.; Hurkmans, J.; Elmgre, M.; et al. Luftkvalitetsberäkningar för Kontroll av Miljökvalitetsnormer: Modeller, Emissionsdata, Osäkerheter och Jämförelser med Mätningar; SLB-analys: Stockholms, Sweeden, 2017; Available online: http://slb.nu/slb/rapporter/pdf8/slb2017_011.pdf (accessed on 14 October 2020).
- Johansson, C.; Hadenius, A.; Johansson, P.Å.; Jonson, T. The Stockholm Study on Health Effects of Air Pollution and Its Economic Consequences. Part 1: NO2 and Particulate Matter in Stockholm; Aqma Report 6:98; Box 38 024, 100 64; Stockholm Environment and Health Protection Administration: Stockholm, Sweden, 1999; Available online: http://slb.nu/slb/rapporter/pdf8/lvf1998_006.pdf (accessed on 1 January 2017).
- The Handbook Emission Factors for Road Transport (HBEFA). Handbook Emission Factors for Road Transport. Version HBEFA 3.2 from July 2014. Available online: http://www.hbefa.net/e/index.html (accessed on 1 January 2017).
- Transphorm. Transport-Related Air Pollution and Health Impacts—Integrated Methodologies for Assessing Particulate Matter. Deliverable D1.1.2: Methodology for the Quantification of Road Transport PM—Emissions, Using Emission Factors or Profiles; Transphorm: Goleta, CA, USA, 2013; Available online: http://www.transphorm.eu/portals/51/documents/deliverables/new%20deliverables/d1.1.2_updated.pdf (accessed on 1 December 2016).
- Johansson, C.; Burman, L.; Forsberg, B. The effects of congestions tax on air quality and health. Atmos. Environ. 2009, 43, 4843–4854. [Google Scholar] [CrossRef]
- Johansson, C.; Norman, M.; Gidhagen, L. Spatial and temporal variations of PM10 and particle number concentrations in urban air. Environ. Monit. Assess. 2007, 127, 477–487. [Google Scholar] [CrossRef]
- Meister, K.; Johansson, C.; Forsberg, B. Estimated short-term effects of coarse particles on daily mortality in Stockholm, Sweden. Environ. Health Perspect. 2012, 120, 431–436. [Google Scholar] [CrossRef]
- Johansson, C.; Lovenheim, B.; Schantz, P.; Wahlgren, L.; Almstrom, P.; Markstedt, A.; Stromgren, M.; Forsberg, B.; Sommar, J.N. Impacts on air pollution and health by changing commuting from car to bicycle. Sci. Total Environ. 2017, 584, 55–63. [Google Scholar] [CrossRef]
- Hystad, P.U.; Setton, E.M.; Allen, R.W.; Keller, P.C.; Brauer, M. Modeling residential fine particulate matter infiltration for exposure assessment. J. Expo. Sci. Environ. Epidemiol. 2009, 19, 570–579. [Google Scholar] [CrossRef] [PubMed]
- Kearney, J.; Wallace, L.; MacNeill, M.; Heroux, M.E.; Kindzierski, W.; Wheeler, A. Residential infiltration of fine and ultrafine particles in Edmonton. Atmos. Environ. 2014, 94, 793–805. [Google Scholar] [CrossRef]
- Bigazzi, A.Y.; Figliozzi, M.A. Impacts of freeway traffic conditions on in-vehicle exposure to ultrafine particulate matter. Atmos. Environ. 2012, 60, 495–503. [Google Scholar] [CrossRef]
- Briggs, D.J.; de Hoogh, K.; Morris, C.; Gulliver, J. Effects of travel mode on exposures to particulate air pollution. Environ. Int. 2008, 34, 12–22. [Google Scholar] [CrossRef] [PubMed]
- Boulter, P.; McCrae, I.S.; Taylor, K. Road Tunnel Air Pollution Monitoring, TRL Limited, Report PR/SE/746/03; Miljöförvaltningen i Stockholm: Stockholm, Sweden, 2004. [Google Scholar]
- Xu, B.; Liu, S.S.; Liu, J.J.; Zhu, Y.F. Effects of vehicle cabin filter efficiency on ultrafine particle concentration ratios measured in-cabin and on-roadway. Aerosol Sci. Technol. 2011, 45, 234–243. [Google Scholar] [CrossRef]
- Hoek, G.; Brunekreef, B.; Goldbohm, S.; Fischer, P.; van den Brandt, P.A. Association between mortality and indicators of traffic-related air pollution in The Netherlands: A cohort study. Lancet 2002, 360, 1203–1209. [Google Scholar] [CrossRef]
- Roemer, W.H.; van Wijnen, J.H. Daily mortality and air pollution along busy streets in Amsterdam, 1987–1998. Epidemiology 2001, 12, 649–653. [Google Scholar] [CrossRef]
- Nafstad, P.; Haheim, L.L.; Wisloff, T.; Gram, F.; Oftedal, B.; Holme, I.; Hjermann, I.; Leren, P. Urban air pollution and mortality in a cohort of Norwegian men. Environ. Health Perspect. 2004, 112, 610–615. [Google Scholar] [CrossRef]
- Hoek, G.; Krishnan, R.M.; Beelen, R.; Peters, A.; Ostro, B.; Brunekreef, B.; Kaufman, J.D. Long-term air pollution exposure and cardio- respiratory mortality: A review. Environ. Health Glob. 2013, 12, 43. [Google Scholar] [CrossRef]
- NBHW. The National Board of Health Andwelfare. Socialstyrelsen SE-106 30, Stockholm, Sweden. 2013. Available online: http://www.socialstyrelsen.se/statistics/statisticaldatabase/causeofdeath (accessed on 1 January 2017).
- Team, R.C. R: A Language and Environment for Statistical Computing. R Foundation for Statistical Computing. Available online: https://www.R-project.org/ (accessed on 14 October 2020).
- Raza, W.; Forsberg, B.; Johansson, C.; Sommar, J.N. Air pollution as a risk factor in health impact assessments of a travel mode shift towards cycling. Glob. Health Action 2018, 11, 1429081. [Google Scholar] [CrossRef]
- Vanwijnen, J.H.; Verhoeff, A.P.; Jans, H.W.A.; Vanbruggen, M. The exposure of cyclists, car drivers and pedestrians to traffic related air-pollutants. Int. Arch. Occup. Environ. Health 1995, 67, 187–193. [Google Scholar] [CrossRef] [PubMed]
- Zuurbier, M.; Hoek, G.; Oldenwening, M.; Lenters, V.; Meliefste, K.; van den Haze, P.; Brunekreef, B. Commuters’ exposure to particulate matter air pollution is affected by mode of transport, fuel type, and route. Environ. Health Perspect. 2010, 118, 783–789. [Google Scholar] [CrossRef] [PubMed]
- Ainsworth, B.E.; Haskell, W.L.; Herrmann, S.D.; Meckes, N.; Bassett, D.R.; Tudor-Locke, C.; Greer, J.L.; Vezina, J.; Whitt-Glover, M.C.; Leon, A.S. 2011 compendium of physical activities: A second update of codes and MET values. Med. Sci. Sports Exerc. 2011, 43, 1575–1581. [Google Scholar] [CrossRef] [PubMed]
- de Nazelle, A.; Fruin, S.; Westerdahl, D.; Martinez, D.; Ripoll, A.; Kubesch, N.; Nieuwenhuijsen, M. A travel mode comparison of commuters’ exposures to air pollutants in Barcelona. Atmos. Environ. 2012, 59, 151–159. [Google Scholar] [CrossRef]
- Mueller, N.; Rojas-Rueda, D.; Cole-Hunter, T.; de Nazelle, A.; Dons, E.; Gerike, R.; Gotschi, T.; Panis, L.I.; Kahlmeier, S.; Nieuwenhuijsen, M. Health impact assessment of active transportation: A systematic review. Prev. Med. 2015, 76, 103–114. [Google Scholar] [CrossRef]
- Woodcock, J.; Givoni, M.; Morgan, A.S. Health impact modelling of active travel visions for England and Wales using an Integrated Transport and Health Impact Modelling Tool (ITHIM). PLoS ONE 2013, 8, e51462. [Google Scholar] [CrossRef]
- Tainio, M.; de Nazelle, A.J.; Gotschi, T.; Kahlmeier, S.; Rojas-Rueda, D.; Nieuwenhuijsen, M.J.; de Sa, T.H.; Kelly, P.; Woodcock, J. Can air pollution negate the health benefits of cycling and walking? Prev. Med. 2016, 87, 233–236. [Google Scholar] [CrossRef]
- Giallouros, G.; Kouis, P.; Papatheodorou, S.I.; Woodcock, J.; Tainio, M. The long-term impact of restricting cycling and walking during high air pollution days on all-cause mortality: Health Impact Assessment study. Environ. Int. 2020, 140, 105679. [Google Scholar] [CrossRef]
- Gidhagen, L.; Johansson, C.; Langner, J.; Olivares, G. Simulation of NOx and ultrafine particles in a street canyon in Stockholm, Sweden. Atmos. Environ. 2004, 38, 2029–2044. [Google Scholar] [CrossRef]
- Gidhagen, L.; Johansson, C.; Omstedt, G.; Langner, J.; Olivares, G. Model simulations of NOx and ultrafine particles close to a Swedish highway. Environ. Sci. Technol. 2004, 38, 6730–6740. [Google Scholar] [CrossRef]
- Faustini, A.; Rapp, R.; Forastiere, F. Nitrogen dioxide and mortality: Review and meta-analysis of long-term studies. Eur. Respir. J. 2014, 44, 744–753. [Google Scholar] [CrossRef] [PubMed]
- Stevens, C.; Williams, R.; Jones, P. Progress on understanding spatial and temporal variability of PM(2.5) and its components in the Detroit exposure and aerosol research study (dears). Environ. Sci. Process. Impacts 2014, 16, 94–105. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Current Situation | Mode-Shift Scenario | Difference and Proportional Change | ||||
|---|---|---|---|---|---|---|
| Mode of Transport | Number of Individuals | Proportion | Number of Individuals | Proportion | Number of Individuals | Proportion |
| Bicycling | 53,206 | 6% | 164,693 | 18% | 111,487 | 210% |
| Walking | 130,441 | 14% | 130,441 | 14% | 0 | 0% |
| Public transport | 352,412 | 38% | 352,412 | 38% | 0 | 0% |
| Car (driver) | 352,614 | 38% | 241,127 | 26% | −111,487 | −32% |
| Car (passenger) | 35,297 | 4% | 35,297 | 4% | 0 | 0% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sommar, J.N.; Johansson, C.; Lövenheim, B.; Markstedt, A.; Strömgren, M.; Forsberg, B. Potential Effects on Travelers’ Air Pollution Exposure and Associated Mortality Estimated for a Mode Shift from Car to Bicycle Commuting. Int. J. Environ. Res. Public Health 2020, 17, 7635. https://doi.org/10.3390/ijerph17207635
Sommar JN, Johansson C, Lövenheim B, Markstedt A, Strömgren M, Forsberg B. Potential Effects on Travelers’ Air Pollution Exposure and Associated Mortality Estimated for a Mode Shift from Car to Bicycle Commuting. International Journal of Environmental Research and Public Health. 2020; 17(20):7635. https://doi.org/10.3390/ijerph17207635
Chicago/Turabian StyleSommar, Johan Nilsson, Christer Johansson, Boel Lövenheim, Anders Markstedt, Magnus Strömgren, and Bertil Forsberg. 2020. "Potential Effects on Travelers’ Air Pollution Exposure and Associated Mortality Estimated for a Mode Shift from Car to Bicycle Commuting" International Journal of Environmental Research and Public Health 17, no. 20: 7635. https://doi.org/10.3390/ijerph17207635
APA StyleSommar, J. N., Johansson, C., Lövenheim, B., Markstedt, A., Strömgren, M., & Forsberg, B. (2020). Potential Effects on Travelers’ Air Pollution Exposure and Associated Mortality Estimated for a Mode Shift from Car to Bicycle Commuting. International Journal of Environmental Research and Public Health, 17(20), 7635. https://doi.org/10.3390/ijerph17207635