Mediating and Moderating Factors of Adherence to Nutrition and Physical Activity Guidelines, Breastfeeding Experience, and Spousal Support on the Relationship between Stress and Quality of Life in Breast Cancer Survivors

 , , ,
, , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Data Collection
2.3. Structured Questionnaires
2.4. Data Analysis
3. Results
3.1. Demographic Characteristics, Stress Level, the Level of HEQoL, Spousal Support, and ACS Guideline Adherence
3.2. Correlation Analysis of Stress Level, Spousal Support, ACS Guideline Adherence, and HRQoL Scores
3.3. Structural Equation Model Analysis Between Stress Level, HRQoL, Spousal Support, ACS Guideline Adherence, and Breastfeeding
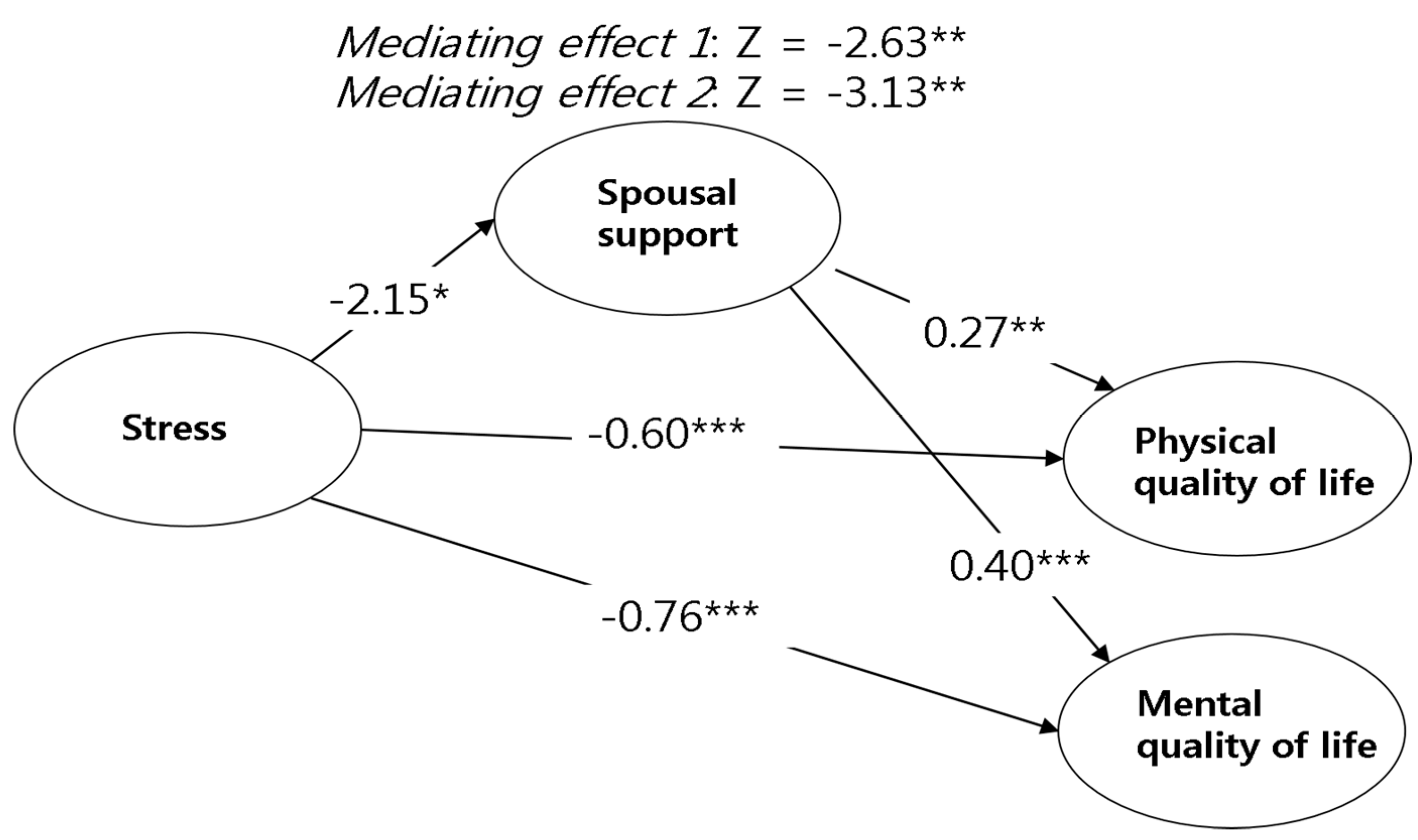
3.3.1. Path Coefficient Analysis of Stress Level, HRQoL, and Spousal Support
3.3.2. Mediating Effect of Spousal Support in the Structural Relationship between Stress and HRQoL
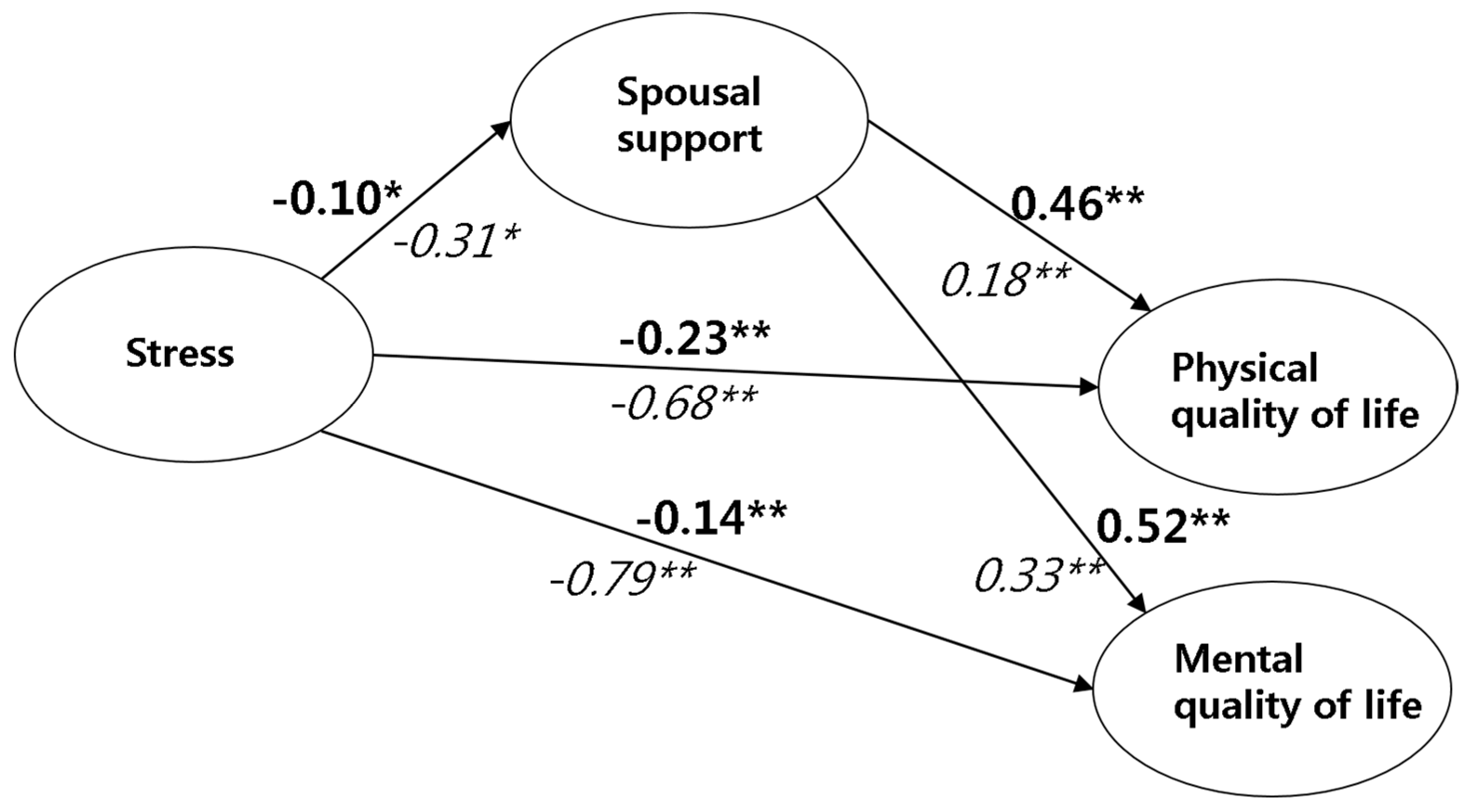
3.3.3. Moderating Effects of ACS Guideline Adherence in the Structural Relationship between Stress, Spousal Support, and HRQoL
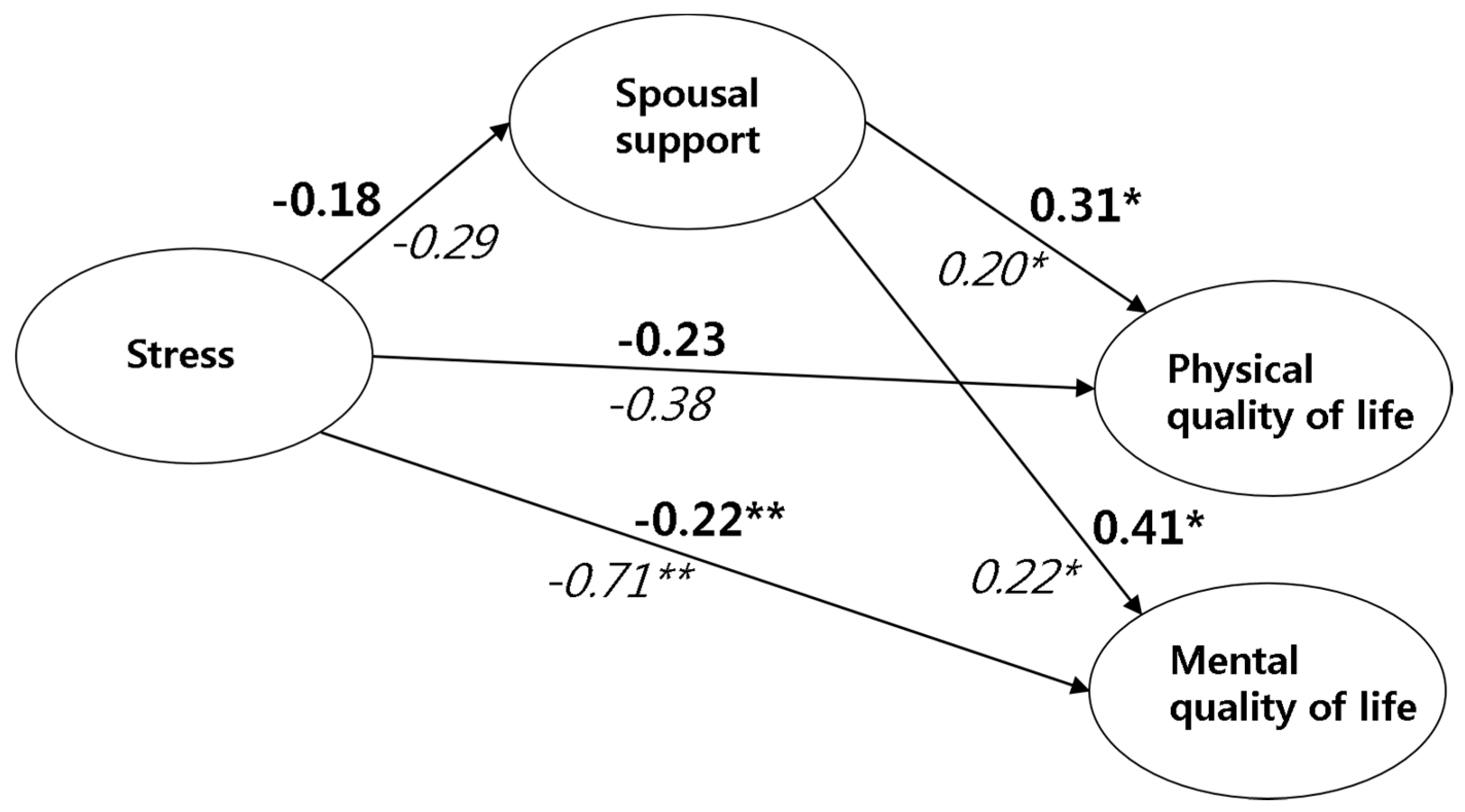
3.3.4. Moderating Effects of Breastfeeding Experience in the Structural Relationship between Stress, Spousal Support, and HRQoL
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Ethical Statement
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed]
- Kang, S.Y.; Kim, Y.S.; Kim, Z.; Kim, H.Y.; Kim, H.J.; Park, S.; Bae, S.Y.; Yoon, K.H.; Lee, S.B.; Lee, S.K.; et al. Breast Cancer Statistics in Korea in 2017: Data from a Breast Cancer Registry. J. Breast Cancer 2020, 23, 115–128. [Google Scholar] [CrossRef] [PubMed]
- Kamalifard, M.; Mirghafourvand, M.; Ranjbar, F.; Gordani, N. Quality of Life Predictors in Breastfeeding Mothers Referred to Health Centers in Iran. Int. J. Women Health Reprod. Sci. 2018, 6, 84–89. [Google Scholar] [CrossRef]
- Ravindran, O.S.; Shankar, A.; Murthy, T. A Comparative Study on Perceived Stress, Coping, Quality of Life, and Hopelessness between Cancer Patients and Survivors. Indian J. Palliat. Care 2019, 25, 414–420. [Google Scholar] [CrossRef]
- Fagerlind, H.; Kettis, Å.; Glimelius, B.; Ring, L. Barriers against psychosocial communication: Oncologists’ perceptions. J. Clin. Oncol. 2013, 31, 3815–3822. [Google Scholar] [CrossRef]
- Rebholz, W.N.; Cash, E.; Zimmaro, L.A.; Bayley-Veloso, R.; Phillips, K.; Siwik, C.; Chagpar, A.B.; Dhabhar, F.S.; Spiegel, D.; Bell, B.S.; et al. Distress and quality of life in an ethnically diverse sample awaiting breast cancer surgery. J. Health Psychol. 2018, 23, 1438–1451. [Google Scholar] [CrossRef]
- Syrowatka, A.; Motulsky, A.; Kurteva, S.; Hanley, J.A.; Dixon, W.G.; Meguerditchian, A.N.; Tamblyn, R. Predictors of distress in female breast cancer survivors: A systematic review. Breast Cancer Res. Treat. 2017, 165, 229–245. [Google Scholar] [CrossRef] [PubMed]
- Cohen, M.; Mabjish, A.A.; Zidan, J. Comparison of Arab breast cancer survivors and healthy controls for spousal relationship, body image, and emotional distress. Qual. Life Res. 2011, 20, 191–198. [Google Scholar] [CrossRef]
- Gremore, T.M.; Baucom, D.H.; Porter, L.S.; Kirby, J.S.; Atkins, D.C.; Keefe, F.J. Stress buffering effects of daily spousal support on women’s daily emotional and physical experiences in the context of breast cancer concerns. Health Psychol. 2011, 30, 20–30. [Google Scholar] [CrossRef]
- Hasson-Ohayon, I.; Goldzweig, G.; Braun, M.; Galinsky, D. Women with advanced breast cancer and their spouses: Diversity of support and psychological distress. Psychooncology 2010, 19, 1195–1204. [Google Scholar] [CrossRef]
- Stulz, A.; Boinon, D.; Dauchy, S.; Delaloge, S.; Bredart, A. Psychological adjustment in couples facing woman’s breast cancer: Perceptions of spousal support. Bull. Cancer 2014, 101, 690–697. [Google Scholar] [CrossRef] [PubMed]
- Alfano, C.M.; Day, J.M.; Katz, M.L.; Herndon, J.E., 2nd; Bittoni, M.A.; Oliveri, J.M.; Donohue, K.; Paskett, E.D. Exercise and dietary change after diagnosis and cancer-related symptoms in long-term survivors of breast cancer: CALGB 79804. Psychooncology 2009, 18, 128–133. [Google Scholar] [CrossRef] [PubMed]
- Koh, D.; Song, S.; Moon, S.E.; Jung, S.Y.; Lee, E.S.; Kim, Z.; Youn, H.J.; Cho, J.; Yoo, Y.B.; Lee, S.K.; et al. Adherence to the American Cancer Society Guidelines for Cancer Survivors and Health-Related Quality of Life among Breast Cancer Survivors. Nutrients 2019, 11, 2924. [Google Scholar] [CrossRef] [PubMed]
- Rock, C.L.; Doyle, C.; Demark-Wahnefried, W.; Meyerhardt, J.; Courneya, K.S.; Schwartz, A.L.; Bandera, E.V.; Hamilton, K.K.; Grant, B.; McCullough, M.; et al. Nutrition and physical activity guidelines for cancer survivors. CA Cancer J. Clin. 2012, 62, 243–274. [Google Scholar] [CrossRef]
- Gonzalez-Jimenez, E.; Garcia, P.A.; Aguilar, M.J.; Padilla, C.A.; Alvarez, J. Breastfeeding and the prevention of breast cancer: A retrospective review of clinical histories. J. Clin. Nurs. 2014, 23, 2397–2403. [Google Scholar] [CrossRef]
- Woodman, I. Breast feeding reduces risk of breast cancer, says study. Br. Med. J. 2002, 325, 184. [Google Scholar] [CrossRef][Green Version]
- Park, J.H.; Chun, M.; Jung, Y.S.; Bae, S.H.; Jung, Y.M. Psychoeducational Approach to Distress Management of Newly Diagnosed Patients with Breast Cancer. J. Korean Acad. Nurs. 2018, 48, 669–678. [Google Scholar] [CrossRef]
- Bail, J.; Meneses, K.; Demark-Wahnefried, W. Nutritional Status and Diet in Cancer Prevention. Semin. Oncol. Nurs. 2016, 32, 206–214. [Google Scholar] [CrossRef] [PubMed]
- Girdano, D.A.; Everly, G.S.J.; Dusek, D.E. Controlling Stress and Tension: A Holistic Approach; Prentice Hall: Englewood Cliffs, NJ, USA, 1979. [Google Scholar]
- Kang, N.M. A study on the stress of nursing students in a university. J. Korean Acad. Soc. Nurs. Educ. 1997, 3, 7–25. [Google Scholar]
- Jenkinson, C.; Wright, L.; Coulter, A. Criterion validity and reliability of the SF-36 in a population sample. Qual. Life Res. 1994, 3, 7–12. [Google Scholar] [CrossRef]
- Lee, B.G.; Lee, T.S.; Kim, S.H. Mediation Effect of Self-Efficacy on the Relationship between Perceived Self-Management Support and Health-Related Quality of Life among Cancer Survivors. J. Korean Acad. Nurs. 2019, 49, 298–306. [Google Scholar] [CrossRef] [PubMed]
- Kang, J.; Suh, E.E. The Influence of Stress, Spousal Support, and Resilience on the Ways of Coping among Women with Breast Cancer. Asian Oncol. Nurs. 2015, 15, 1–8. [Google Scholar] [CrossRef]
- Mols, F.; Vingerhoets, A.J.; Coebergh, J.W.; van de Poll-Franse, L.V. Quality of life among long-term breast cancer survivors: A systematic review. Eur. J. Cancer 2005, 41, 2613–2619. [Google Scholar] [CrossRef] [PubMed]
- Cifu, G.; Arem, H. Adherence to lifestyle-related cancer prevention guidelines and breast cancer incidence and mortality. Ann. Epidemiol. 2018, 28, 767–773. [Google Scholar] [CrossRef] [PubMed]
- Oh, Y.K.; Hwang, S.Y. Impact of Uncertainty on the Quality of Life of Young Breast Cancer Patients: Focusing on Mediating Effect of Marital Intimacy. J. Korean Acad. Nurs. 2018, 48, 50–58. [Google Scholar] [CrossRef]
- Sharif, S.P. Locus of control, quality of life, anxiety, and depression among Malaysian breast cancer patients: The mediating role of uncertainty. Eur. J. Oncol. Nurs. 2017, 27, 28–35. [Google Scholar] [CrossRef]
- Tryggvadottir, L.; Tulinius, H.; Eyfjord, J.E.; Sigurvinsson, T. Breastfeeding and reduced risk of breast cancer in an Icelandic cohort study. Am. J. Epidemiol. 2001, 154, 37–42. [Google Scholar] [CrossRef][Green Version]
- Pérez-Escamilla, R.; Sellen, D. Equity in breastfeeding: Where do we go from here? J. Hum. Lact. 2015, 31, 12–14. [Google Scholar] [CrossRef]
- Del Ciampo, L.A.; Del Ciampo, I.R.L. Breastfeeding and the Benefits of Lactation for Women’s Health. Rev. Bras. Ginecol. Obstet. 2018, 40, 354–359. [Google Scholar] [CrossRef]
- Krol, K.M.; Grossmann, T. Psychological effects of breastfeeding on children and mothers. Bundesgesundheitsbl. Gesundheitsforsch. Gesundheitsschutz 2018, 61, 977–985. [Google Scholar] [CrossRef]
- Chen, Y.C.; Chie, W.C.; Kuo, S.C.; Lin, Y.H.; Lin, S.J.; Chen, P.C. The association between infant feeding pattern and mother’s quality of life in Taiwan. Qual. Life Res. 2007, 16, 1281–1288. [Google Scholar] [CrossRef] [PubMed]
- Alijanpoor, M.; Bahadoran, P. Quality of life of nursing mothers referred to healthcare centers. J. Health Care 2015, 17, 108–115. [Google Scholar]
- Kent, G. Child feeding and human rights. Int. Breastfeed J. 2006, 1, 27. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | Categories | n | ValidPercentage (%) | CumulativePercentage (%) |
|---|---|---|---|---|
| Time since surgery | 1–2 years | 27 | 18.8 | 18.8 |
| 2–3 years | 19 | 13.2 | 32.0 | |
| 3–4 years | 17 | 11.8 | 43.8 | |
| 4–5 years | 19 | 13.2 | 57.0 | |
| >5 years | 62 | 43.0 | 100.0 | |
| Marital status | Married or cohabitation | 109 | 76.5 | 76.5 |
| Not married or divorced or widowed | 35 | 23.5 | 100.0 | |
| Breastfeeding experience | No | 38 | 26.4 | 26.4 |
| Yes | 106 | 73.6 | 100 | |
| Parity | No | 13 | 8.7 | 8.7 |
| Yes | 136 | 91.3 | 100.0 | |
| Education level | Elementary school or below | 25 | 17.4 | 17.4 |
| Middle school | 15 | 10.4 | 27.8 | |
| High school | 71 | 49.3 | 77.1 | |
| College or above | 33 | 22.9 | 100.0 | |
| Cancer stage | I | 73 | 50.7 | 50.7 |
| II | 62 | 43.1 | 93.8 | |
| III | 9 | 6.2 | 100.0 |
| Variables | Mean ± SD | Skewness | Kurtosis | Min-Max | |
|---|---|---|---|---|---|
| Stress level | 20.9 ± 3.41 | 1.24 | 1.40 | 5–25 | |
| HRQoL | |||||
| Physical QoL | PF | 73.45 ± 22.29 | −0.94 | 0.32 | 5–100 |
| RP | 75.21 ± 26.20 | −1.03 | 0.35 | 0–100 | |
| BP | 69.75 ± 24.10 | −0.24 | −0.99 | 21–100 | |
| GH | 60.65 ± 19.99 | −0.54 | −0.12 | 5–100 | |
| Mental QoL | VT | 58.12 ± 20.95 | −0.35 | −0.64 | 0–100 |
| SF | 81.88 ± 21.28 | −1.10 | 0.43 | 25–100 | |
| RE | 77.46 ± 26.36 | −1.04 | 0.15 | 0–100 | |
| MH | 69.31 ± 20.43 | −0.77 | 0.52 | 0–100 | |
| Spousal support | 33.41 ± 13.26 | 0.45 | −0.60 | 13–65 | |
| ACS adherence | 7.91 ± 1.91 | 0.04 | −0.29 | 3–12 |
| Stress | Spousal Support | ACS | Physical Quality of Life | Mental Quality of Life | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| PF | RP | BP | GH | PF | RP | BP | GH | |||||
| Stress | 1.000 | |||||||||||
| Spousal support | 0.151 | 1.000 | ||||||||||
| ACS | 0.031 | 0.057 | 1.000 | |||||||||
| Pysical QoL | PF | −0.415 * | 0.049 | 0.032 | 1.000 | |||||||
| RP | −0.494 * | 0.040 | 0.121 | 0.594 * | 1.000 | |||||||
| BP | −0.506 * | −0.044 | −0.051 | 0.504 * | 0.585 * | 1.000 | ||||||
| GH | −0.460 * | −0.140 | 0.087 | 0.393 * | 0.405 * | 0.448 * | 1.000 | |||||
| Mental QoL | VT | −0.536 * | −0.069 | −0.059 | 0.443 * | 0.433 * | 0.559 * | 0.643 * | 1.000 | |||
| SF | −0.593 * | −0.041 | 0.051 | 0.528 * | 0.684 * | 0.592 * | 0.473 * | 0.549 * | 1.000 | |||
| RE | −0.609 * | −0.026 | 0.075 | 0.607 * | 0.821 * | 0.556 * | 0.417 * | 0.487 * | 0.685 * | 1.000 | ||
| MH | −0.679 * | −0.151 | 0.110 | 0.369 * | 0.491 * | 0.495 * | 0.524 * | 0.654 * | 0.580 * | 0.570 * | 1.000 | |
| β | S.E | Min | Max | t | p | |||
|---|---|---|---|---|---|---|---|---|
| Stress level | → | spousal support | −0.22 | 0.06 | −0.04 | −0.40 | −3.77 | 0.015 * |
| Stress level | → | physical quality of life | −0.60 | 0.06 | −0.72 | −0.51 | −10.68 | <0.001 *** |
| Stress level | → | mental quality of life | −0.76 | 0.04 | −0.83 | −0.68 | −20.15 | <0.001 *** |
| Spousal support | → | physical quality of life | 0.27 | 0.11 | 0.11 | 0.29 | 2.33 | 0.004 ** |
| Spousal support | → | mental quality of life | 0.40 | 0.07 | −0.14 | 0.15 | 5.61 | <0.001 *** |
| ACS Adherence (β) | t | df | p | ||||
|---|---|---|---|---|---|---|---|
| High | Low | ||||||
| Stress | → | spousal support | −0.10 | −0.31 | −2.37 | 105 | 0.014 * |
| Stress | → | physical quality of life | −0.23 | −0.68 | −3.27 | 105 | 0.007 ** |
| Stress | → | mental quality of life | −0.14 | −0.79 | −3.86 | 105 | 0.004 ** |
| Spousal support | → | physical quality of life | 0.46 | 0.18 | 3.28 | 105 | 0.009 ** |
| Spousal support | → | mental quality of life | 0.52 | 0.33 | 1.79 | 105 | 0.062 |
| Breastfeeding (β) | t | df | p | ||||
|---|---|---|---|---|---|---|---|
| Yes | No | ||||||
| Stress | → | spousal support | −0.18 | −0.29 | −1.05 | 105 | 0.153 |
| Stress | → | physical quality of life | −0.23 | −0.38 | −1.41 | 105 | 0.104 |
| Stress | → | mental quality of life | −0.22 | −0.71 | −3.27 | 105 | 0.001 ** |
| Spousal support | → | physical quality of life | 0.31 | 0.20 | 2.02 | 105 | 0.041 * |
| Spousal support | → | mental quality of life | 0.41 | 0.22 | 2.13 | 105 | 0.038 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kang, N.M.; Hahn, W.-H.; Park, S.; Lee, J.E.; Yoo, Y.B.; Ryoo, C.J. Mediating and Moderating Factors of Adherence to Nutrition and Physical Activity Guidelines, Breastfeeding Experience, and Spousal Support on the Relationship between Stress and Quality of Life in Breast Cancer Survivors. Int. J. Environ. Res. Public Health 2020, 17, 7532. https://doi.org/10.3390/ijerph17207532
Kang NM, Hahn W-H, Park S, Lee JE, Yoo YB, Ryoo CJ. Mediating and Moderating Factors of Adherence to Nutrition and Physical Activity Guidelines, Breastfeeding Experience, and Spousal Support on the Relationship between Stress and Quality of Life in Breast Cancer Survivors. International Journal of Environmental Research and Public Health. 2020; 17(20):7532. https://doi.org/10.3390/ijerph17207532
Chicago/Turabian StyleKang, Nam Mi, Won-Ho Hahn, Suyeon Park, Jung Eun Lee, Young Bum Yoo, and Chung Ja Ryoo. 2020. "Mediating and Moderating Factors of Adherence to Nutrition and Physical Activity Guidelines, Breastfeeding Experience, and Spousal Support on the Relationship between Stress and Quality of Life in Breast Cancer Survivors" International Journal of Environmental Research and Public Health 17, no. 20: 7532. https://doi.org/10.3390/ijerph17207532
APA StyleKang, N. M., Hahn, W.-H., Park, S., Lee, J. E., Yoo, Y. B., & Ryoo, C. J. (2020). Mediating and Moderating Factors of Adherence to Nutrition and Physical Activity Guidelines, Breastfeeding Experience, and Spousal Support on the Relationship between Stress and Quality of Life in Breast Cancer Survivors. International Journal of Environmental Research and Public Health, 17(20), 7532. https://doi.org/10.3390/ijerph17207532