Motor Imagery Performance and Tactile Spatial Acuity: Are They Altered in People with Frozen Shoulder?


Abstract
1. Introduction
2. Materials and Methods
2.1. Ethics
2.2. Participants
2.3. Left/Right Judgement Task Procedure
2.4. Two-Point Tactile Discrimination Procedure
2.5. Statistical Analysis
3. Results
3.1. Participant Characteristics
3.2. Left/Right Judgement
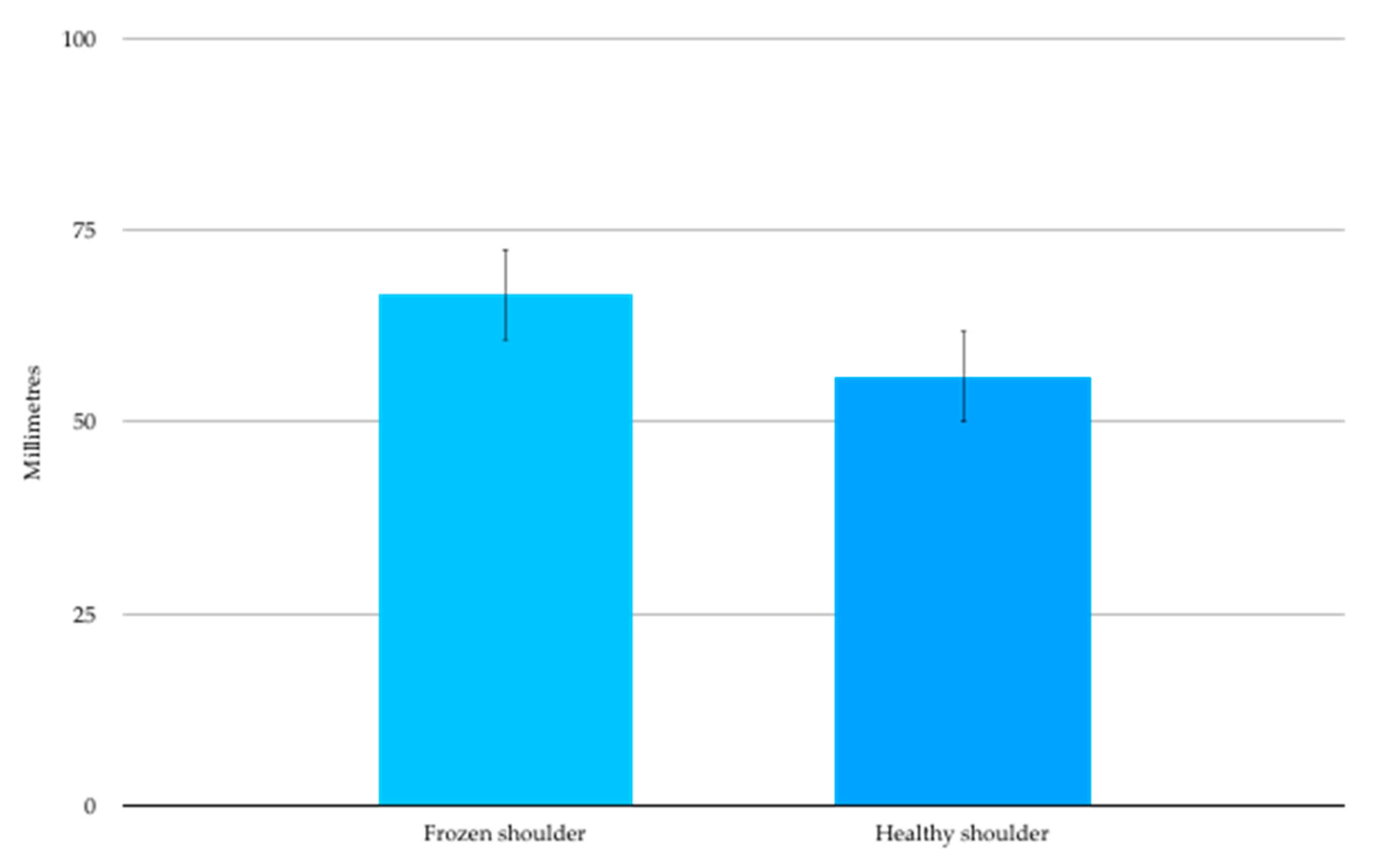
3.3. Two-Point Discrimination
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Lewis, J. Frozen shoulder contracture syndrome–Aetiology, diagnosis and management. Man. Ther. 2015, 20, 2–9. [Google Scholar] [CrossRef]
- Reeves, B. The Natural History of the Frozen Shoulder Syndrome. Scand. J. Rheumatol. 2009, 4, 193–196. [Google Scholar] [CrossRef]
- Wong, C.K.; Levine, W.N.; Deo, K.; Kesting, R.S.; Mercer, E.A.; Schram, G.A.; Strang, B.L. Natural history of frozen shoulder: Fact or fiction? A systematic review. Physiotherapy 2017, 103, 40–47. [Google Scholar] [CrossRef] [PubMed]
- Hanchard, N.C.; Goodchild, L.; Thompson, J.; O′Brien, T.; Davison, D.; Richardson, C. Evidence-based clinical guidelines for the diagnosis, assessment and physiotherapy management of contracted (frozen) shoulder: Quick reference summary. Physiotherapy 2012, 98, 117–120. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.-P.; Fann, C.-Y.; Chiu, Y.-H.; Yen, M.-F.; Chen, L.-S.; Chen, H.-H.; Pan, S.-L. Association of Diabetes Mellitus with the Risk of Developing Adhesive Capsulitis of the Shoulder: A Longitudinal Population-Based Followup Study. Arthritis Care Res. 2013, 65, 1197–1202. [Google Scholar] [CrossRef]
- Huang, S.-W.; Lin, J.-W.; Wang, W.-T.; Wu, C.-W.; Liou, T.-H.; Lin, H.-W. Hyperthyroidism is a Risk Factor for Developing Adhesive Capsulitis of the Shoulder: A Nationwide Longitudinal Population-Based Study. Sci. Rep. 2014, 4. [Google Scholar] [CrossRef]
- Smith, S.P.; Devaraj, V.S.; Bunker, T.D. The association between frozen shoulder and Dupuytren’s disease. J. Shoulder Elb. Surg. 2001, 10, 149–151. [Google Scholar] [CrossRef]
- Müller, L.; Müller, L.; Happ, J.; Kerschbaumer, F. Frozen shoulder: A sympathetic dystrophy? Arch. Orthop. Trauma Surg. 2000, 120, 84–87. [Google Scholar] [CrossRef] [PubMed]
- Ryan, V.; Brown, H.; Minns Lowe, C.J.; Lewis, J.S. The pathophysiology associated with primary (idiopathic) frozen shoulder: A systematic review. BMC Musculoskelet. Disord. 2016, 17, 340. [Google Scholar] [CrossRef] [PubMed]
- Hollmann, L.; Halaki, M.; Haber, M.; Herbert, R.; Dalton, S.; Ginn, K. Determining the contribution of active stiffness to reduced range of motion in frozen shoulder. Physiotherapy 2015, 101. [Google Scholar] [CrossRef]
- Hollmann, L.; Halaki, M.; Kamper, S.J.; Haber, M.; Ginn, K.A. Does muscle guarding play a role in range of motion loss in patients with frozen shoulder? Musculoskelet. Sci. Pr. 2018, 37, 64–68. [Google Scholar] [CrossRef] [PubMed]
- Itoi, E.; Arce, G.; Bain, G.I.; Diercks, R.L.; Guttmann, D.; Imhoff, A.B.; Mazzocca, A.D.; Sugaya, H.; Yoo, Y.S. Shoulder Stiffness: Current Concepts and Concerns. Arthroscopy 2016, 32, 1402–1414. [Google Scholar] [CrossRef]
- Walmsley, S.; Rivett, D.A.; Osmotherly, P.G. Adhesive Capsulitis: Establishing Consensus on Clinical Identifiers for Stage 1 Using the Delphi Technique. Phys. Ther. 2009, 89, 906–917. [Google Scholar] [CrossRef] [PubMed]
- Walmsley, S.; Osmotherly, P.; Rivett, D. Clinical Identifiers for Early-Stage Primary/Idiopathic Adhesive Capsulitis: Are We Seeing the Real Picture? Physiotherapy 2014, 94, 968–976. [Google Scholar] [CrossRef] [PubMed]
- Codman, E. The Shoulder: Rupture of the Supraspinatus Tendon and Other Lesions in and around the Subacromial Bursa; Thomas Todd Company: Boston, MA, USA, 1934. [Google Scholar]
- Diercks, R.L.; Stevens, M. Gentle thawing of the frozen shoulder: A prospective study of supervised neglect versus intensive physical therapy in seventy-seven patients with frozen shoulder syndrome followed up for two years. J. Shoulder Elb. Surg. 2004, 13, 499–502. [Google Scholar] [CrossRef] [PubMed]
- Vermeulen, H.M.; Rozing, P.M.; Obermann, W.R.; le Cessie, S.; Vliet Vlieland, T.P. Comparison of High-Grade and Low-Grade Mobilization Techniques in the Management of Adhesive Capsulitis of the Shoulder: Randomized Controlled Trial. Phys. Ther. 2006, 86, 355–368. [Google Scholar] [CrossRef] [PubMed]
- Carette, S.; Moffet, H.; Tardif, J.; Bessette, L.; Morin, F.; Fremont, P.; Bykerk, V.; Thorne, C.; Bell, M.; Bensen, W.; et al. Intraarticular corticosteroids, supervised physiotherapy, or a combination of the two in the treatment of adhesive capsulitis of the shoulder: A placebo-controlled trial. Arthritis Rheum. 2003, 48, 829–838. [Google Scholar] [CrossRef]
- Moseley, G.L.; Flor, H. Targeting Cortical Representations in the Treatment of Chronic Pain: A Review. Neurorehabilit. Neural Repair 2012, 26, 646–652. [Google Scholar] [CrossRef]
- Chang, W.J.; O’Connell, N.E.; Beckenkamp, P.R.; Alhassani, G.; Liston, M.B.; Schabrun, S.M. Altered Primary Motor Cortex Structure, Organization, and Function in Chronic Pain: A Systematic Review and Meta-Analysis. J. Pain 2018. [Google Scholar] [CrossRef]
- Wand, B.M.; Parkitny, L.; O’Connell, N.E.; Luomajoki, H.; McAuley, J.H.; Thacker, M.; Moseley, G.L. Cortical changes in chronic low back pain: Current state of the art and implications for clinical practice. Man. Ther. 2011, 16, 15–20. [Google Scholar] [CrossRef]
- Di Pietro, F.; McAuley, J.H.; Parkitny, L.; Lotze, M.; Wand, B.M.; Moseley, G.L.; Stanton, T.R. Primary somatosensory cortex function in complex regional pain syndrome: A systematic review and meta-analysis. J. Pain 2013, 14, 1001–1018. [Google Scholar] [CrossRef] [PubMed]
- Shanahan, C.J.; Hodges, P.W.; Wrigley, T.V.; Bennell, K.L.; Farrell, M.J. Organisation of the motor cortex differs between people with and without knee osteoarthritis. Arthritis Res. Ther. 2015, 17, 164. [Google Scholar] [CrossRef] [PubMed]
- Schabrun, S.M.; Hodges, P.W.; Vicenzino, B.; Jones, E.; Chipchase, L.S. Novel Adaptations in Motor Cortical Maps: The Relation to Persistent Elbow Pain. Med. Sci. Sports Exerc. 2015, 47, 681–690. [Google Scholar] [CrossRef] [PubMed]
- Ngomo, S.; Mercier, C.; Bouyer, L.J.; Savoie, A.; Roy, J.S. Alterations in central motor representation increase over time in individuals with rotator cuff tendinopathy. Clin. Neurophysiol. 2015, 126, 365–371. [Google Scholar] [CrossRef] [PubMed]
- Di Pietro, F.; McAuley, J.H.; Parkitny, L.; Lotze, M.; Wand, B.M.; Moseley, G.L.; Stanton, T.R. Primary motor cortex function in complex regional pain syndrome: A systematic review and meta-analysis. J. Pain 2013, 14, 1270–1288. [Google Scholar] [CrossRef]
- Moseley, G.L. I can’t find it! Distorted body image and tactile dysfunction in patients with chronic back pain. Pain 2008, 140, 239–243. [Google Scholar] [CrossRef]
- Brumagne, S.; Cordo, P.; Lysens, R.; Verschueren, S.; Swinnen, S. The role of paraspinal muscle spindles in lumbosacral position sense in individuals with and without low back pain. Spine 2000, 25, 989–994. [Google Scholar] [CrossRef]
- Harvie, D.S.; Hillier, S.; Madden, V.J.; Smith, R.T.; Broecker, M.; Meulders, A.; Moseley, G.L. Neck Pain and Proprioception Revisited Using the Proprioception Incongruence Detection Test. Phys. Ther. 2016, 96, 671–678. [Google Scholar] [CrossRef]
- Stanton, T.R.; Leake, H.B.; Chalmers, K.J.; Moseley, G.L. Evidence of Impaired Proprioception in Chronic, Idiopathic Neck Pain: Systematic Review and Meta-Analysis. Phys. Ther. 2016, 96, 876–887. [Google Scholar] [CrossRef]
- Stanton, T.R.; Leake, H.; Wallwork, S.B.; Moseley, G.L. Disruptions to cortical proprioceptive representation in people with chronic neck pain. Physiotherapy 2015, 101, e1433–e1434. [Google Scholar] [CrossRef]
- Nishigami, T.; Mibu, A.; Tanaka, K.; Yamashita, Y.; Yamada, E.; Wand, B.M.; Catley, M.J.; Stanton, T.R.; Moseley, G.L. Development and psychometric properties of knee-specific body-perception questionnaire in people with knee osteoarthritis: The Fremantle Knee Awareness Questionnaire. PLoS ONE 2017, 12, e0179225. [Google Scholar] [CrossRef]
- Cammarata, M.L.; Dhaher, Y.Y. Associations between frontal plane joint stiffness and proprioceptive acuity in knee osteoarthritis. Arthritis Care Res. 2012, 64, 735–743. [Google Scholar] [CrossRef]
- Chang, A.H.; Lee, S.J.; Zhao, H.; Ren, Y.; Zhang, L.Q. Impaired varus-valgus proprioception and neuromuscular stabilization in medial knee osteoarthritis. J. Biomech. 2014, 47, 360–366. [Google Scholar] [CrossRef] [PubMed]
- Moseley, G.L. Distorted body image in complex regional pain syndrome Neurology.pdf. Neurology 2005, 65, 773. [Google Scholar] [CrossRef] [PubMed]
- Moseley, G.L.; Gallace, A.; Spence, C. Bodily illusions in health and disease: Physiological and clinical perspectives and the concept of a cortical ‘body matrix’. Neurosci. Biobehav. Rev. 2012, 36, 34–46. [Google Scholar] [CrossRef]
- Moseley, G.L.; Gallace, A.; Iannetti, G.D. Spatially defined modulation of skin temperature and hand ownership of both hands in patients with unilateral complex regional pain syndrome. Brain 2012, 135, 3676–3686. [Google Scholar] [CrossRef] [PubMed]
- Ager, A.L.; Borms, D.; Deschepper, L.; Dhooghe, R.; Dijkhuis, J.; Roy, J.S.; Cools, A. Proprioception: How is it affected by shoulder pain? A systematic review. J. Hand Ther. 2019. [Google Scholar] [CrossRef]
- Catley, M.J.; O′Connell, N.E.; Berryman, C.; Ayhan, F.F.; Moseley, G.L. Is tactile acuity altered in people with chronic pain? A systematic review and meta-analysis. J. Pain 2014, 15, 985–1000. [Google Scholar] [CrossRef]
- Parsons, L. Integrating cognitive psychology, neurology and neuroimaging. Acta Psychol. 2001, 107, 155–181. [Google Scholar] [CrossRef]
- Breckenridge, J.D.; Ginn, K.A.; Wallwork, S.B.; McAuley, J.H. Do People with Chronic Musculoskeletal Pain Have Impaired Motor Imagery? A Meta-analytical Systematic Review of the Left/Right Judgment Task. J. Pain 2018. [Google Scholar] [CrossRef]
- Mena-del Horno, S.; Balasch-Bernat, M.; Dueñas, L.; Reis, F.; Louw, A.; Lluch, E. Laterality judgement and tactile acuity in patients with frozen shoulder: A cross-sectional study. Musculoskelet. Sci. Pract. 2020, 47, 102136. [Google Scholar] [CrossRef] [PubMed]
- Heerkens, R.J.; Köke, A.J.; Lötters, F.J.; Smeets, R.J. Motor imagery performance and tactile acuity in patients with complaints of arms, neck and shoulder. Pain Manag. 2018, 8, 277–286. [Google Scholar] [CrossRef]
- Cashin, A.G.; McAuley, J.H. Measuring two-point discrimination threshold with a caliper. J. Physiother. 2017, 63, 186. [Google Scholar] [CrossRef] [PubMed]
- Moseley, G.L. Graded motor imagery is effective for long-standing complex regional pain syndrome: A randomised controlled trial. Pain 2004, 108, 192–198. [Google Scholar] [CrossRef] [PubMed]
- Bowering, K.J.; O′Connell, N.E.; Tabor, A.; Catley, M.J.; Leake, H.B.; Moseley, G.L.; Stanton, T.R. The effects of graded motor imagery and its components on chronic pain: A systematic review and meta-analysis. J. Pain 2013, 14, 3–13. [Google Scholar] [CrossRef]
- Moseley, G.L. Is successful rehabilitation of complex regional pain syndrome due to sustained attention to the affected limb? A randomised clinical trial. Pain 2005, 114, 54–61. [Google Scholar] [CrossRef]
- Moseley, G.L. Graded motor imagery for pathologic pain: A randomized controlled trial. Neurology 2006, 67, 2129–2134. [Google Scholar] [CrossRef]
- Flor, H.; Denke, C.; Schaefer, M.; Grusser, S. Effect of sensory discrimination training on cortical reorganisation and phantom limb pain. Lancet 2001, 357, 1763–1764. [Google Scholar] [CrossRef]
- Moseley, G.L.; Zalucki, N.M.; Wiech, K. Tactile discrimination, but not tactile stimulation alone, reduces chronic limb pain. Pain 2008, 137, 600–608. [Google Scholar] [CrossRef]
- Kalin, S.; Rausch-Osthoff, A.K.; Bauer, C.M. What is the effect of sensory discrimination training on chronic low back pain? A systematic review. BMC Musculoskelet. Disord. 2016, 17, 143. [Google Scholar] [CrossRef]
- Wand, B.; O′Connell, N.; Di Pietro, F.; Bulsara, M. Managing Chronic Nonspecific Low Back Pain with a Sensorimotor Retraining Approach: Exploratory Multiple-Baseline Study of 3 Participants. Phys. Ther. 2011, 91, 535–546. [Google Scholar] [CrossRef] [PubMed]
- Sawyer, E.E.; McDevitt, A.W.; Louw, A.; Puentedura, E.J.; Mintken, P.E. Use of Pain Neuroscience Education, Tactile Discrimination, and Graded Motor Imagery in an Individual With Frozen Shoulder. J. Orthop. Sports Phys. Ther. 2018, 48, 174–184. [Google Scholar] [CrossRef] [PubMed]
- Kamper, S.J. Pain Intensity Ratings. J. Physiother. 2012, 58. [Google Scholar] [CrossRef]
- Roach, K.E.; Budiman-Mak, E.; Songsiridej, N.; Lertratanakul, Y. Development of a Shoulder Pain and Disability Index. Arthritis Care Res. 1991, 4, 143–149. [Google Scholar] [CrossRef]
- Breckenridge, J.D.; McAuley, J.H. Shoulder Pain and Disability Index (SPADI). J. Physiother. 2011, 57, 197. [Google Scholar] [CrossRef]
- Hayes, K.; Walton, J.R.; Szomor, Z.L.; Murrell, G.A.C. Reliability of five methods for assessing shoulder range of motion. Aust. J. Physiother. 2001, 47, 289–294. [Google Scholar] [CrossRef]
- Breckenridge, J.D.; McAuley, J.H.; Butler, D.S.; Stewart, H.; Moseley, G.L.; Ginn, K.A. The development of a shoulder specific left/right judgement task: Validity & reliability. Musculoskelet. Sci. Pr. 2017, 28, 39–45. [Google Scholar] [CrossRef]
- Wallwork, S.B.; Butler, D.S.; Fulton, I.; Stewart, H.; Darmawan, I.; Moseley, G.L. Left/right neck rotation judgments are affected by age, gender, handedness and image rotation. Man. Ther. 2013, 18, 225–230. [Google Scholar] [CrossRef]
- Bowering, K.J.; Butler, D.S.; Fulton, I.J.; Moseley, G.L. Motor imagery in people with a history of back pain, current back pain, both, or neither. Clin. J. Pain 2014, 30, 1070–1075. [Google Scholar] [CrossRef]
- Bray, H.; Moseley, G.L. Disrupted working body schema of the trunk in people with back pain. Br. J. Sports Med. 2011, 45, 168–173. [Google Scholar] [CrossRef]
- Dey, A.; Barnsley, N.; Mohan, R.; McCormick, M.; McAuley, J.H.; Moseley, G.L. Are children who play a sport or a musical instrument better at motor imagery than children who do not? Br. J. Sports Med. 2012, 46, 923–926. [Google Scholar] [CrossRef] [PubMed]
- Cooper, L.A.; Shepard, R.N. Mental transformation in the identification of left and right hands. J. Exp. Psychol. Hum. Percept. Perform. 1975, 1, 48–56. [Google Scholar] [CrossRef]
- Moberg, E. Two point discrimination test. Scand. J. Rehab. Med. 1990, 22, 127–134. [Google Scholar]
- Mancini, F.; Bauleo, A.; Cole, J.; Lui, F.; Porro, C.A.; Haggard, P.; Iannetti, G.D. Whole-body mapping of spatial acuity for pain and touch. Ann. Neurol. 2014, 75, 917–924. [Google Scholar] [CrossRef]
- Wand, B.M.; Di Pietro, F.; George, P.; O′Connell, N.E. Tactile thresholds are preserved yet complex sensory function is impaired over the lumbar spine of chronic non-specific low back pain patients: A preliminary investigation. Physiotherapy 2010, 96, 317–323. [Google Scholar] [CrossRef]
- Scandola, M.; Dodoni, L.; Lazzeri, G.; Arcangeli, C.A.; Avesani, R.; Moro, V.; Ionta, S. Neurocognitive Benefits of Physiotherapy for Spinal Cord Injury. J. Neurotrauma 2018, 36, 2028–2035. [Google Scholar] [CrossRef] [PubMed]
- Brumagne, S.; Cordo, P.; Verschueren, S. Proprioceptive weighting changes in persons with low back pain and elderly persons during upright standing. Neurosci. Lett. 2004, 366, 63–66. [Google Scholar] [CrossRef] [PubMed]
- Breckenridge, J.D.; McAuley, J.H.; Moseley, G.L.; Ginn, K.A. Is motor imagery altered in people with shoulder pain? The shoulder left/right judgement task. Musculoskelet. Sci. Pract. 2020. [Google Scholar] [CrossRef]
- Lewis, J.S.; Kersten, P.; McPherson, K.M.; Taylor, G.J.; Harris, N.; McCabe, C.S.; Blake, D.R. Wherever is my arm? Impaired upper limb position accuracy in Complex Regional Pain Syndrome. Pain 2010, 149, 463–469. [Google Scholar] [CrossRef] [PubMed]
- Lundberg, B. The Frozen Shoulder. Acta Orthop. Scand. 1969, S119, 1–59. [Google Scholar] [CrossRef]
- Perruchoud, D.; Fiorio, M.; Cesari, P.; Ionta, S. Beyond variability: Subjective timing and the neurophysiology of motor cognition. Brain Stimul. Basic Transl. Clin. Res. Neuromodul. 2018, 11, 175–180. [Google Scholar] [CrossRef] [PubMed]
- Pleger, B.; Tegenthoff, M.; Ragert, P.; Forster, A.F.; Dinse, H.R.; Schwenkreis, P.; Nicolas, V.; Maier, C. Sensorimotor retuning [corrected] in complex regional pain syndrome parallels pain reduction. Ann. Neurol. 2005, 57, 425–429. [Google Scholar] [CrossRef] [PubMed]
- Nolan, M.F. Two point discrimination assesssment in the upper limb in young adult men and women. Phys. Ther. 1982, 62, 965–969. [Google Scholar] [CrossRef] [PubMed]
- Davey, N.; Nowicky, A.; Zaman, R. Somatotopy of perceptual threshold to cutaneous electrical stimulaton in man. Experimantal Physiol. 2001, 86, 127–130. [Google Scholar] [CrossRef] [PubMed]
- Botnmark, I.; Tumilty, S.; Mani, R. Tactile acuity, body schema integrity and physical performance of the shoulder: A cross-sectional study. Man. Ther. 2016, 23, 9–16. [Google Scholar] [CrossRef]
- Louis, D.S.; Greene, T.L.; Jacobson, K.E.; Rasmussen, C.; Kolowich, P.; Goldstein, S.A. Evaluation of normal values for stationary and moving two-point discrimination in the hand. J. Hand Surg. 1984, 9, 552–555. [Google Scholar] [CrossRef]
- Shimokata, H.; Kuzuya, F. Two-point discrimination test of the skin as an index of sensory aging. Gerontology 1995, 41, 267–272. [Google Scholar] [CrossRef]
- Melzack, R. Phantom limbs and the concept of a neuromatrix. Trends Neurosci. 1990, 13, 88–92. [Google Scholar] [CrossRef]
- Lundborg, G.; RosÉN, B. The Two-Point Discrimination Test–Time for a Re-Appraisal? J. Hand Surg. 2004, 29, 418–422. [Google Scholar] [CrossRef]
- Tong, J.; Mao, O.; Goldreich, D. Two-point orientation discrimination versus the traditional two-point test for tactile spatial acuity assessment. Front. Hum. Neurosci. 2013, 7, 579. [Google Scholar] [CrossRef]
- Catley, M.J.; Tabor, A.; Wand, B.M.; Moseley, G.L. Assessing tactile acuity in rheumatology and musculoskeletal medicine–How reliable are two-point discrimination tests at the neck, hand, back and foot? Rheumatology 2013, 52, 1454–1461. [Google Scholar] [CrossRef] [PubMed]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |




{kind=link}
{kind=link}
{kind=link}
| Participant | Affected Shoulder | Age Years | Gender | Duration Frozen Shoulder Weeks | Worst Pain NRS /10 | Average Pain NRS /10 | SPADI Score % |
|---|---|---|---|---|---|---|---|
| 1 | Left | 69 | Female | 24 | 8 | 5 | 55 |
| 2 | Right | 48 | Female | 9 | 9 | 5 | 66 |
| 3 | Left | 45 | Male | 13 | 10 | 7 | 67 |
| 4 | Left | 57 | Male | 13 | 9 | 5 | 46 |
| 5 | Left | 45 | Male | 13 | 10 | 5 | 24 |
| 6 | Left | 50 | Female | 32 | 10 | 9 | 88 |
| 7 | Left | 50 | Male | 20 | 10 | 6 | 62 |
| 8 | Left | 52 | Female | 13 | 8 | 5 | 54 |
| 9 | Right | 41 | Female | 36 | 6 | 3 | 35 |
| 10 | Left | 67 | Female | 28 | 0 | 0 | 17 |
| 11 | Right | 58 | Male | 20 | 9 | 8 | 79 |
| 12 | Left | 46 | Female | 20 | 8 | 6 | 68 |
| 13 | Left | 63 | Female | 28 | 10 | 5 | 87 |
| 14 | Left | 57 | Female | 11 | 7 | 2 | 59 |
| 15 | Right | 43 | Female | 26 | 10 | 7 | 74 |
| 16 | Right | 49 | Female | 44 | 9 | 7 | 76 |
| 17 | Right | 59 | Female | 30 | 6 | 3 | 39 |
| 18 | Left | 53 | Female | 16 | 5 | 2 | 70 |
| Mean (SD) | 52.9(8.1) | 22.0(9.7) | 8.0(2.5) | 5.0(2.3) | 59.2(20.4) |
| Passive Range of Motion | ||||||
|---|---|---|---|---|---|---|
| Affected Shoulder | Healthy Shoulder | |||||
| Participant | Flexion | Ext. Rot. | HBB. | Flexion | Ext. Rot. | HBB |
| 1 | 90 | 15 | - | 160 | 55 | - |
| 2 | 85 | -5 | hip | 175 | 75 | T8 |
| 3 | 105 | 5 | butt | 180 | 45 | T6 |
| 4 | 105 | 15 | SIJ | 180 | 60 | T7 |
| 5 | 100 | 55 | L1 | 175 | 70 | T7 |
| 6 | 45 | -10 | butt | 180 | 70 | T6 |
| 7 | 105 | 10 | hip | 170 | 70 | T7 |
| 8 | 100 | 20 | L5 | 180 | 75 | T4 |
| 9 | 115 | 55 | SIJ | 160 | 70 | T10 |
| 10 | 95 | 50 | L5 | 160 | 70 | T10 |
| 11 | 100 | 25 | S1 | 180 | 70 | T10 |
| 12 | 90 | 10 | - | 180 | 90 | - |
| 13 | 90 | 30 | hip | 180 | 80 | T10 |
| 14 | 90 | 15 | butt | 185 | 95 | T6 |
| 15 | 105 | 35 | butt | 160 | 80 | T10 |
| 16 | 90 | 5 | - | 150 | 35 | - |
| 17 | 85 | 10 | - | 175 | 80 | - |
| 18 | 95 | 10 | butt | 180 | 80 | T6 |
| Mean (SD) | 93.9(14.7) | 19.4(19.0) | 172.5(10.0) | 70.6(14.8) | ||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Breckenridge, J.D.; McAuley, J.H.; Ginn, K.A. Motor Imagery Performance and Tactile Spatial Acuity: Are They Altered in People with Frozen Shoulder? Int. J. Environ. Res. Public Health 2020, 17, 7464. https://doi.org/10.3390/ijerph17207464
Breckenridge JD, McAuley JH, Ginn KA. Motor Imagery Performance and Tactile Spatial Acuity: Are They Altered in People with Frozen Shoulder? International Journal of Environmental Research and Public Health. 2020; 17(20):7464. https://doi.org/10.3390/ijerph17207464
Chicago/Turabian StyleBreckenridge, John D., James H. McAuley, and Karen A. Ginn. 2020. "Motor Imagery Performance and Tactile Spatial Acuity: Are They Altered in People with Frozen Shoulder?" International Journal of Environmental Research and Public Health 17, no. 20: 7464. https://doi.org/10.3390/ijerph17207464
APA StyleBreckenridge, J. D., McAuley, J. H., & Ginn, K. A. (2020). Motor Imagery Performance and Tactile Spatial Acuity: Are They Altered in People with Frozen Shoulder? International Journal of Environmental Research and Public Health, 17(20), 7464. https://doi.org/10.3390/ijerph17207464