Trauma and Violence Informed Care Through Decolonising Interagency Partnerships: A Complexity Case Study of Waminda’s Model of Systemic Decolonisation

 , ,
, ,  and
and 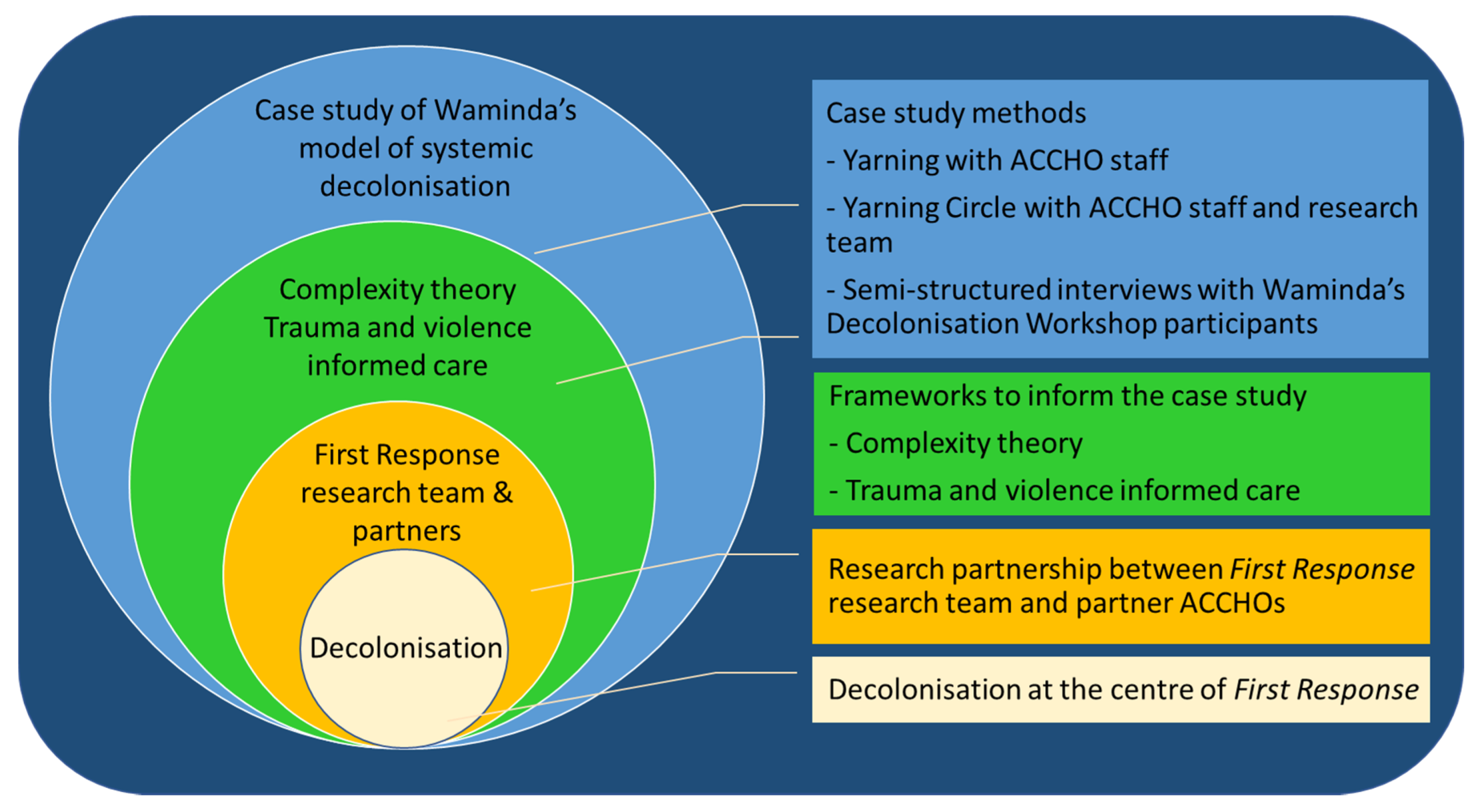{kind=link}
{kind=link}
Abstract
1. Introduction
2. Materials and Methods
2.1. Design and Theory
2.2. Ethics, Participants and Data Collection
2.3. Analysis and Synthesis
3. Results
3.1. Complexity of Interagency Partnerships
3.1.1. Why Advocacy
“And that’s not saying we should be duplicating services, or just doing the work of other services but it’s just making sure that people don’t miss out really”(ACCHO Management/Team leader)
“[I] do a lot of advocating for people to government departments such as Centrelink and Department of Housing; and now with the NDIS (National Disability Insurance Scheme) I assist people with their applications”(ACCHO Team member)
“There’s a lack of information for clients, a big lack of information for clients and I know even since I’ve been down here in 10 years the information that’s supplied by other services, and even government organisations, is very confusing for victims and their children and they don’t understand it so they don’t follow through with it because they don’t have the understanding of what’s going on, that’s the difference I think”(ACCHO Management/Team leader)
“So, it is very different, we do work in that strength-based way, which is very different to pretty well everyone else to be honest. But that’s complex because, you know, the women get a particular experience here. I’m not saying we’re perfect by any means but if you get a particular way of working here and then you’re trying to navigate a whole heap of other systems or people or workers who say, well you know, you were late or you don’t give a shit because you didn’t turn up again. And, you know, how many chances do you need”(ACCHO Management/Team leader)
“I’m really supportive of the police and the hospital system, I understand their jobs are really hard but that’s probably the biggest challenge. So, when crunch comes to crunch and you have quite an acute issue I find the response—especially when it’s repeated from certain clients that ring the police a lot and there’s drug and alcohol issues or whatever—I find the response a bit blasé sometimes from those organisations, or a woman desperate and goes to the emergency department to present with a child and they just turn her away. And then the shelters are full, the housing is limited so I find that really hard. We’re Monday to Friday nine to five so that limits what we can do. We’ve only got the resources we’ve got, we’re not a crisis service so then when we go to use or direct our clients to that crisis service, and they’re turned away they stop going there. They go, ‘What’s the point?’”(ACCHO Management/Team leader)
“Because you refer someone, or you drop someone off to a service and they get a shit service, or they don’t even get past the receptionist. Of course, it comes backs on you because we do have a responsibility to improve access, you know. I mean we can’t do everything, but if they’re not getting a decent service, we need to do something about that”(ACCHO Management/Team leader)
3.1.2. Making Partnerships Work
“I think we could do more in terms of the NGOs, I think a lot of us rely on who we know in services and then people move around. I tend to follow the clinician more than the service because I know who’s going to respond and who’s going to do what so it’s just keeping up to date with that… we just don’t have time to get out or even know where they’re doing what they’re doing. Because stuff changes quickly, funding changes and it’s hard to keep up.”(ACCHO Management/Team leader)
“So, yes, it can be quite complicated, the relationships—and it can be quite time consuming as well because it’s just a constant thing that you’ve got to give attention to. You can’t have an MOU [memorandum of understanding] and put it on the shelf and think ‘oh, well, sweet we’ve got that under control’—because people change, things change and you’ve actually got to have these organic partnerships, that take a huge amount of work, huge amount of work”(ACCHO Management/Team leader)
“Communication is—once again, it’s not rocket science, is it, but we’ve had a really great outcome recently, with incredible communication with Justice Health….They’re just really good outcomes, like incredible communication over what services, and the women are just going, “This is awesome,” because she’s been listened to, she knows what’s happening there’s transparency—transparency’s a big one—letting women know what you’re doing …. And that’s probably benefits of a multidisciplinary team being together and making sure everyone knows what’s happening, that can be really good”(ACCHO Team member)
“And that’s based on the historical context, and we have a very good relationship with Corrective Services here, and the magistrate understands all that, so if there’s a (ACCHO) worker down there at the courthouse, he will look more favourably on (ACCHO) support with this particular family, because children’s court they’re closed sometimes, but he has allowed (ACCHO) people in there to support the family; he’s understanding. Not many courts will do that, but our local court does.”(ACCHO Management/Team leader)
3.1.3. Acts of Resistance
“So, the (NGO), about two years ago they setup a 1300 number for people to ring for food assistance and financial assistance. You can be on hold there for over an hour and then all of a sudden, they’ll say, ‘I’m sorry, we’re unable to assist you today, please ring back tomorrow.’ So that infuriated me, let alone someone that’s starving, poor mental health, whatever. So, I rang and complained to head office and said, ‘This just isn’t acceptable. I haven’t been able to access your service for eight months’ and I said, ‘And I’m leaning on other services and I don’t think that’s fair.’ So, I then got the direct number for the person down here. Now I just ring them—you really have to be a proactive worker to want to go out on a limb and do things like that”(ACCHO Team member)
“There’s some pretty solid work that we’ve done for, probably, for a number of years with certain government departments…. where that’s made a huge impact for community. That’s probably come from pretty bad places to very positive relationships now. So, that’s really important because, again, it’s that first response stuff. But we do have, you know, fractious relationships, too, with some services we believe are not delivering good services. And I suppose we have never been backward in coming forward in saying what we think about that. But always with, you know, through decolonisation lens… and I’m not saying that you need to be arguing with everyone all the time either. Because that often, can be counterproductive but yeah, I think we’re pretty on par in knowing that partnerships are important because we know, if we can influence and have impact on other service providers then that—what’s going to happen is better outcomes for the women”(ACCHO Management/Team leader)
“So, she’s trying to get her finger in all of those pies, to make sure that they’re engaging our women in a culturally appropriate way rather than alienating them. You know, you can’t speak that sort of language to some of our women. Because I wouldn’t understand it. You know, the language and the terminology that they use when they’re referring to—for the impacts of trauma or whatever, you need to say it as it is”(ACCHO Management/Team leader)
“That’s a lot what I do with the government organisations, is to talk about the cultural stuff that’s going on and the intergenerational trauma and things like that. So, a lot of service providers ask me questions because they feel comfortable enough to sort of ask me those types of questions in private”(ACCHO Team member)
3.2. A New Approach to Decolonising the Workforce
3.2.1. A Skilled and Capable Workforce Across Sectors
“So, it is a process that’s actually really helping, and what it is, it’s taking responsibility. So, the white people have to take responsibility for white people here. And you talk to a lot of the Aboriginal senior staff here, and they’re just relieved, that they don’t have to sort us out. Like, it’s our responsibility to confront that”(ACCHO Management/Team leader)
“And so, having these sessions with staff, with the Health District, where we looked at, walking in two worlds and looking at traditional way[s] of people living but reflecting on, well, what’s changed, what has colonisation actually done. So, it’s not all that warm and fuzzy stuff and this is a didg [didgeridoo]… it’s really quite different. But a big part of what happens is that looking at colonisation, transgenerational trauma, very much about white privilege and white fragility and really breaking that down. So that’s had a massive impact”(ACCHO Management/Team leader)
“Until you look at decolonisation and systemic racism and where this has all come from and your white privilege, you can’t do anything else…. I said: ‘If people aren’t up for this discussion, the problem is bigger than you think.’ And I said, ‘We won’t be partnering in community with anybody who doesn’t see this as a major issue or the issue’”(ACCHO Management/Team leader)
“You know, people didn’t know what decolonisation was at all and that wasn’t even a judgement by us, it’s just, like, wow, that’s not even talked about”(ACCHO Management/Team leader)
“We’ve had to think about what we do about that, in a bigger picture. So not just that worker to worker, people experiencing that prejudice or that racist approach, but really trying to look more systemically, I suppose. And so out of that very much, looking at that systemic racism and institutional stuff, we have been really working a lot at that level and having a lot of conversations with high levels of government”(ACCHO Management/Team leader)
3.2.2. Decolonisation: More Than Just ‘Cultural Competency’
“The take home messages are that colonisation is alive and well and everything that we’ve designed in our system is not designed with Aboriginal people in mind, and that is so massive, how do you make a change that’s going to be able to meet the objectives … and be effective and respectful for people on the ground”(Decolonisation workshop participant)
“Oh my God, every single person in Australia needs to attend that training, but they’re not going to, so then how do we do this?”(Decolonisation workshop participant)
“So, I think that it’s the life stories— so having somebody standing up in the room …. sharing their stories is a really, really powerful tool”(Decolonisation workshop participant)
“I think it (the workshop) focused less on Aboriginal cultural practice. I think most cultural awareness training that I’ve been to has a really strong focus and is often very locality based—and it’s often really focused on sharing the local culture and the local history. So, I guess, for me, this one moved away from that. It talked a lot about Aboriginal history, in a much broader context as colonisation, which is something that I studied at uni and had the awareness of, but I guess this workshop really personalised it a bit more for people and the context or the impact on particularly some of the workers (Wamimda staff) who spoke”(Decolonisation workshop participant)
“I particularly enjoyed the sisters (elders) that came from the Illawarra, and they were able to give us some really deep, local knowledge and context. So, in terms of a level of investment in improving our knowledge, understanding and engagement, I thought it was very, very high [quality]”(Decolonisation workshop participant)
3.2.3. Understanding and Reflecting on White Privilege
“I’m really getting a lot out, at the moment, around the whole focus on white privilege. I think there needs to be more of that education, and that’s what I’ve been educating my white friends about. Because they don’t know—or let’s just say—they don’t think there’s any such thing as white privilege”(Decolonisation workshop participant)
“I think because I manage staff, I’ll have it always in the back of my mind that this is a focus area for us, that I need to have my staff’s understanding of those concepts in regard to white fragility as well as white privilege in the back of their mind in regard to whatever they’re doing with their target group of young people”(Decolonisation workshop participant)
3.3. Decolonising Partnerships
3.3.1. Shared Experience and Common Language
“When you think about that group, incredible group of leaders and many leaders for a really long time, we’re all much more used to talking than listening … having the opportunity to have our opinion …but I think this was a real opportunity to spend some time listening and reflecting”(Decolonisation workshop participant)
“So it was very good. I mean, it took me a while to actually get into that headspace. All of us in that room are really, really busy people and there’s so many demands. But once I managed to get over that I really got a lot out of it”(Decolonisation workshop participant)
“You know, a lot of people sitting in that room, I don’t see much at all, but just having that shared knowledge and knowing, okay, this is not just our organisation that’s thinking through these issues, there are others, and we either need to connect more or coordinate effort more strongly …. and just getting that sense that we’ve now got a bit of a shared language in one sense. I know that’s a big phrase because the issue is not a new one, but the fact that we’ve had that shared experience”(Decolonisation workshop participant)
“I’m sure that everybody in that room had a strong commitment to positive outcomes for Aboriginal communities and Aboriginal families. There’s no doubt. I’m absolutely certain that many, many people in that room already worked well with Aboriginal communities, but I just feel like it sort of draws a line in the sand that we all can agree on, and so commonality around language and objective”(Decolonisation workshop participant)
“Having that workshop was something that we could all agree on, was necessary to build a more collaborative focus for that leadership group ….So this, I think, will enable, hopefully, a strategic focus on how the region or the district applies itself and how we can make sure that our programs in that district are doing that work to the best that we can and how we are shaping our services”(Decolonisation workshop participant)
3.3.2. Responsibility and Change
“It’s all of our responsibilities to think about what we can all contribute, and it’s a community issue, that we all need to have a level of ownership of …as well as a personal one—but I thought it was clever how it [the workshop] enforced or emphasised the collective responsibility we all have in our respective positions, to pay attention, to deal with this issue”(Decolonisation workshop participant)
“But recognising that the trauma is with the person and with the family and with the community and stays there and that when you’re working with them you need to work in a way that recognises that”(Decolonisation workshop participant)
“So I’ve kind of really pulled back from the whole launch idea now as well, and just having a think about how we might do that in the teams and have deeper conversations more about structural racism and some of the concepts that we were really getting exposed to in the workshop. And, doing more of that to make the plan more personal for each person, rather than it just being one big event that’s engaging at a fairly superficial level”(Decolonisation workshop participant)
“One of the things I’ve done since the workshop, is we have an Aboriginal staff group that meet with the managers and that’s around …how we strengthen our work with Aboriginal families and also support our Aboriginal staff as well, and I’ve just really noticed our managers in that group are really relying on those Aboriginal people in that group to lead it, as opposed to the other way around”(Decolonisation workshop participant)
“Some of the key things for us to think about is being careful not to overly rely on our Aboriginal staff. Yeah, around our education and really taking responsibility as—we have Aboriginal leaders but as non-Aboriginal leaders within our organisation as well”(Decolonisation workshop participant)
“What I think it will do is continue to build momentum around Aboriginal families being a priority for our district... So, I think it will cement that and because it was so powerful that will stay with people and will give them the incentive to keep planning around this”(Decolonisation workshop participant)
“I think the main benefit of the workshop is that it gets everybody on the same page. So, I think from (Organisation) perspective their work is going to focus more on working with Aboriginal communities and Aboriginal families. And I think as a strategic group leading that direction, I think it’s really important that we all view that from the same standpoint”(Decolonisation workshop participant)
4. Discussion
4.1. Co-Evolution: Language Shapes Responses
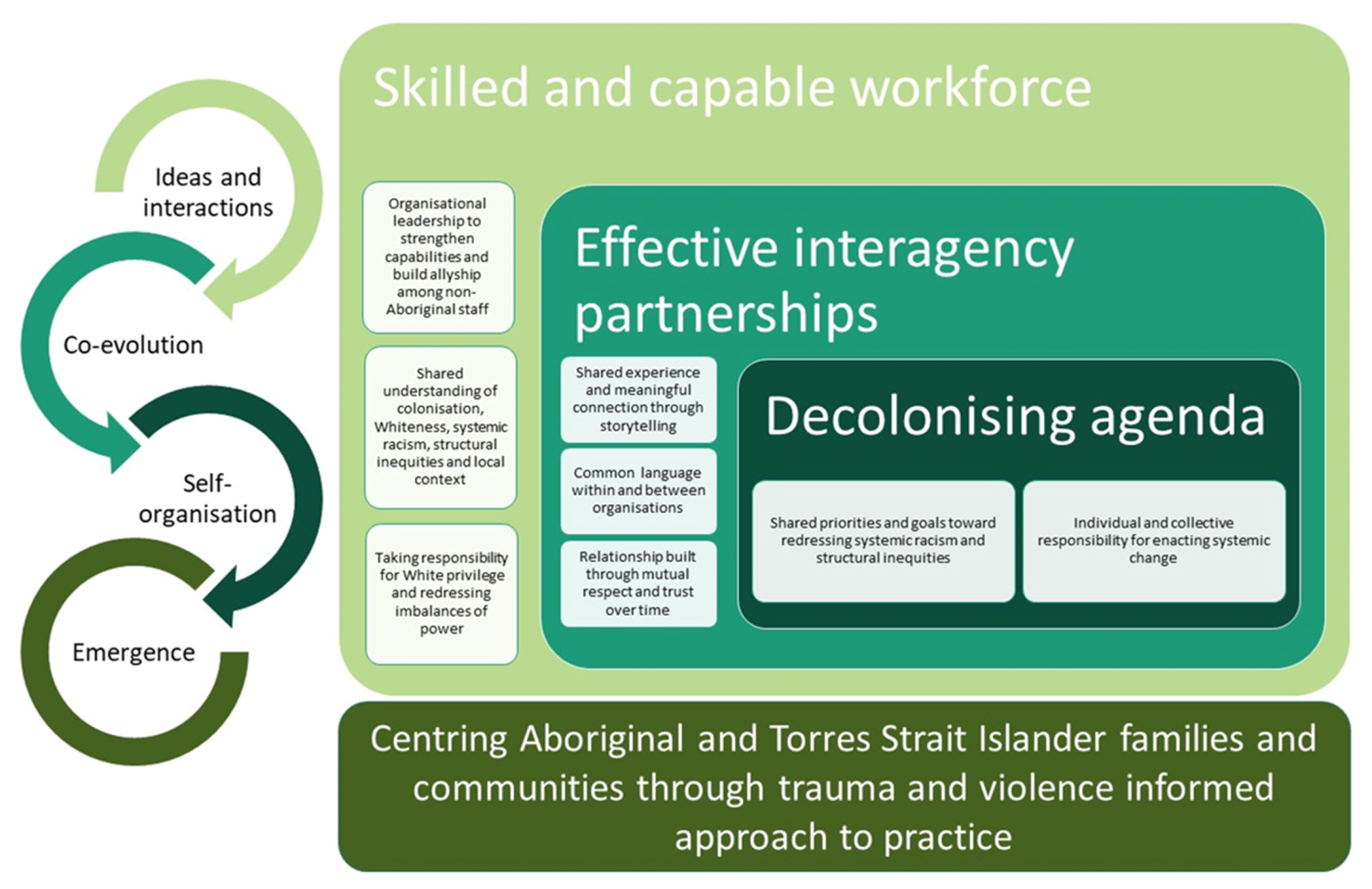
4.2. Self-Organisation: New Ways of Working
4.3. Emergence: The Butterfly Effect
4.4. Implications for Practice, Policy and Future Research
4.5. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- United Nations. Fact Sheet No.9 (Rev.1), The Rights of Indigenous Peoples; United Nations: Geneva, Switzerland, 1997. [Google Scholar]
- Griffiths, K.; Coleman, C.; Lee, V.; Madden, R. How colonisation determines social justice and Indigenous health—A review of the literature. J. Popul. Res. 2016, 33, 9–30. [Google Scholar] [CrossRef]
- Paradies, Y. Colonisation, racism and indigenous health. J. Popul. Res. 2016, 33, 83–96. [Google Scholar] [CrossRef]
- Calma, T.; Dudgeon, P.; Bray, A. Aboriginal and Torres Strait Islander Social and Emotional Wellbeing and Mental Health. Aust. Psychol. 2017, 52, 255–260. [Google Scholar] [CrossRef]
- Dudgeon, P.; Walker, R. Decolonising Australian Psychology: Discourses, Strategies, and Practice. J. Soc. Politi-Psychol. 2015, 3, 276–297. [Google Scholar] [CrossRef]
- Sherwood, J.; Edwards, T. Decolonisation: A critical step for improving Aboriginal health. Contemp. Nurse 2006, 22, 178–190. [Google Scholar] [CrossRef]
- Sherwood, J. Who is Not Coping with Colonization? Laying Out the Map for Decolonization. Australas. Psychiatry 2009, 17, S24–S27. [Google Scholar] [CrossRef]
- Atkinson, J.; Nelson, J.; Atkinson, C. Trauma, transgenerational transfer and effects on community wellbeing. In Working Together: Aboriginal and Torres Strait Islander Mental Health and Wellbeing Principles and Practice; Purdie, N., Dudgeon, P., Walker, R., Eds.; Australian Institute of Health and Welfare: Canberra, Australia, 2010; pp. 135–144. [Google Scholar]
- Fogarty, W.; Bulloch, H.; McDonnell, S.; Davis, M. Deficit Discourse and Indigenous Health: How Narrative Framings of Aboriginal and Torres Strait Islander People Are Reproduced in Policy; The Lowitja Institute: Melbourne, Australia, 2018. [Google Scholar]
- Ziersch, A.; Gallaher, G.; Baum, F.; Bentley, M. Responding to racism: Insights on how racism can damage health from an urban study of Australian Aboriginal people. Soc. Sci. Med. 2011, 73, 1045–1053. [Google Scholar] [CrossRef]
- Durey, A. Reducing racism in Aboriginal health care in Australia: Where does cultural education fit? Aust. N. Z. J. Public Health 2010, 34, S87–S92. [Google Scholar] [CrossRef]
- Larson, A.; Gillies, M.; Howard, P.J.; Coffin, J. It’s enough to make you sick: The impact of racism on the health of Aboriginal Australians. Aust. N. Z. J. Public Health 2007, 31, 322–329. [Google Scholar] [CrossRef]
- Priest, N.C.; Paradies, Y.C.; Gunthorpe, W.; Cairney, S.J.; Sayers, S.M. Racism as a determinant of social and emotional wellbeing for Aboriginal Australian youth. Med. J. Aust. 2011, 194, 546–550. [Google Scholar] [CrossRef]
- Australian Institute of Health and Welfare. The Health and Welfare of Australia’s Aboriginal and Torres Strait Islander Peoples 2015; AIHW: Canberra, Australia, 2015. [Google Scholar]
- Moreton-Robinson, A. Toward a New Research Agenda? Foucault, Whiteness, and Indigenous Sovereignty. Seeing Race Again 2019, 42, 293–306. [Google Scholar]
- Mackean, T.; Fisher, M.; Friel, S.; Baum, F. A framework to assess cultural safety in Australian public policy. Health Promot. Int. 2019, 35, 340–351. [Google Scholar] [CrossRef] [PubMed]
- Browne, A.J.; Varcoe, C.; Lavoie, J.; Smye, V.; Wong, S.T.; Krause, M.; Tu, D.; Godwin, O.; Khan, K.; Fridkin, A. Enhancing health care equity with Indigenous populations: Evidence-based strategies from an ethnographic study. BMC Health Serv. Res. 2016, 16, 544. [Google Scholar] [CrossRef] [PubMed]
- Browne, A.J.; Varcoe, C.; Wong, S.T.; Smye, V.L.; Lavoie, J.; Littlejohn, D.; Tu, D.; Godwin, O.; Krause, M.; Khan, K.B.; et al. Closing the health equity gap: Evidence-based strategies for primary health care organizations. Int. J. Equity Health 2012, 11, 59. [Google Scholar] [CrossRef] [PubMed]
- Aboriginal Affairs Victoria. Strong Culture, Strong Peoples, Strong Families: Towards a Safer Future for Indigenous Families and Communities; Victorian Government: Melbourne, Victoria, Australia, 2008. Available online: https://www.dhhs.vic.gov.au/sites/default/files/documents/201706/Strong-culture-10_Year_plan_Oct08_2nd_edition.pdf (accessed on 8 June 2020).
- Anderson, R.A.; Crabtree, B.F.; Steele, D.J.; McDaniel, R.R. Case study research: The view from complexity science. Qual. Health Res. 2005, 15, 669–685. [Google Scholar] [CrossRef] [PubMed]
- Cohn, S.; Clinch, M.; Bunn, C.; Stronge, P.; Bunn, C. Entangled complexity: Why complex interventions are just not complicated enough. J. Health Serv. Res. Policy 2013, 18, 40–43. [Google Scholar] [CrossRef] [PubMed]
- Braithwaite, J.; Churruca, K.; Ellis, L.A.; Long, J.; Clay-Williams, R.; Damen, N.; Herkes, J.; Pomare, C.; Ludlow, K. Complexity Science in Healthcare–Aspirations, Approaches, Applications and Accomplishments: A White Paper; Macquarie University: Sydney, Australia, 2017; Available online: https://www.mq.edu.au/research/research-centres-groups-and-facilities/healthy-people/centres/australian-institute-of-health-innovation/news-and-events/news/news/complexity-science-in-healthcare-aspirations,-approaches,-applications-and-accomplishments-a-white-paper (accessed on 15 May 2020).
- Braithwaite, J.; Glasziou, P.; I Westbrook, J. The three numbers you need to know about healthcare: The 60-30-10 Challenge. BMC Med. 2020, 18, 102–108. [Google Scholar] [CrossRef]
- Braithwaite, J.; Churruca, K.; Long, J.C.; A Ellis, L.; Herkes, J. When complexity science meets implementation science: A theoretical and empirical analysis of systems change. BMC Med. 2018, 16, 63. [Google Scholar] [CrossRef]
- Gear, C.; Koziol-McLain, J.; Eppel, E. Exploring sustainable primary care responses to intimate partner violence in New Zealand: Qualitative use of complexity theory. BMJ Open 2019, 9, e031827. [Google Scholar] [CrossRef]
- Browne, A.J.; On behalf of the EQUIP Research Team; Varcoe, C.; Ford-Gilboe, M.; Wathen, C.N. EQUIP Healthcare: An overview of a multi-component intervention to enhance equity-oriented care in primary health care settings. Int. J. Equity Health 2015, 14, 1–11. [Google Scholar] [CrossRef]
- Bessarab, D.; Ng’Andu, B. Yarning About Yarning as a Legitimate Method in Indigenous Research. Int. J. Crit. Indig. Stud. 2010, 3, 37–50. [Google Scholar] [CrossRef]
- Laycock, A.; Walker, D.; Harrison, N.; Brands, J. Chapter Three: Indigenous Frameworks and Methods for Research. In Researching Indigenous Health: A Practical Guide for Researchers; The Lowitja Institute: Melbourne, Australia, 2011; pp. 43–64. [Google Scholar]
- Walker, M.; Fredericks, B.; Mills, K.; Anderson, D. “Yarning” as a Method for Community-Based Health Research With Indigenous Women: The Indigenous Women’s Wellness Research Program. Health Care Women Int. 2014, 35, 1216–1226. [Google Scholar] [CrossRef] [PubMed]
- QSR International Pty Ltd. NVivo Qualitative Data Analysis Software (Version 12), 2018.
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V. Reflecting on reflexive thematic analysis. Qual. Res. Sport Exerc. Health 2019, 11, 589–597. [Google Scholar] [CrossRef]
- Gale, N.; Heath, G.; Cameron, E.; Rashid, S.; Redwood, S. Using the framework method for the analysis of qualitative data in multi-disciplinary health research. BMC Med. Res. Methodol. 2013, 13, 117. [Google Scholar] [CrossRef]
- Shepherd, S.M. Cultural awareness workshops: Limitations and practical consequences. BMC Med. Educ. 2019, 19, 14. [Google Scholar] [CrossRef] [PubMed]
- Fisher-Borne, M.; Cain, J.M.; Martin, S.L. From Mastery to Accountability: Cultural Humility as an Alternative to Cultural Competence. Soc. Work. Educ. 2015, 34, 165–181. [Google Scholar] [CrossRef]
- DiAngelo, R. White Fragility. Int. J. Crit. Pedagog. 2011, 3, 54–70. [Google Scholar]
- Herring, S.; Spangaro, J.; Lauw, M.; McNamara, L. The Intersection of Trauma, Racism, and Cultural Competence in Effective Work with Aboriginal People: Waiting for Trust. Aust. Soc. Work. 2013, 66, 104–117. [Google Scholar] [CrossRef]
- Sonn, C.C.; Stevens, G.; Duncan, N. Decolonisation, critical methodologies and why stories matter. In Race, Memory and the Apartheid Archive: Towards a Transformative Psychosocial Praxis; Stevens, G., Duncan, N., Hook, D., Eds.; Palgrave Macmillan: New York, NY, USA, 2013; pp. 295–314. [Google Scholar]
- Walter, M.; Taylor, S.; Habibis, D. How White is Social Work in Australia? Aust. Soc. Work. 2011, 64, 6–19. [Google Scholar] [CrossRef]
- Cabrera, N.L. White Immunity: Working Through Some of the Pedagogical Pitfalls of “Privilege”. JCSCORE 2018, 3, 77–90. [Google Scholar] [CrossRef]
- Tate, S.A.; Page, D. Whiteliness and institutional racism: Hiding behind (un)conscious bias. Ethic Educ. 2018, 13, 141–155. [Google Scholar] [CrossRef]
- Fernando, T.; Bennett, B. Creating a Culturally Safe Space When Teaching Aboriginal Content in Social Work: A Scoping Review. Aust. Soc. Work. 2018, 72, 47–61. [Google Scholar] [CrossRef]
- Green, S.; Bennett, B. Wayanha: A Decolonised Social Work. Aust. Soc. Work. 2018, 71, 261–264. [Google Scholar] [CrossRef]
- Anderson, P.; Tilton, E. Bringing Them Home 20 Years on: An Action Plan for Healing; Aboriginal and Torres Strait Islander Healing Foundation: Canberra, Australia, 2017. [Google Scholar]
- Walker, N.; Mackean, T.; Longbottom, M.; Coombes, J.; Bennett-Brook, K.; Clapham, K.; Ivers, R.; Hackett, M.; Redfern, J.; Cullen, P. Responses to the primary health care needs of Aboriginal and Torres Strait Islander women experiencing violence: A scoping review of policy and practice guidelines. Health Promot. J. Aust. 2020. [Google Scholar] [CrossRef]
- Greenhalgh, T.; Papoutsi, C. Studying complexity in health services research: Desperately seeking an overdue paradigm shift. BMC Med. 2018, 16, 95. [Google Scholar] [CrossRef]


© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cullen, P.; Mackean, T.; Worner, F.; Wellington, C.; Longbottom, H.; Coombes, J.; Bennett-Brook, K.; Clapham, K.; Ivers, R.; Hackett, M.; et al. Trauma and Violence Informed Care Through Decolonising Interagency Partnerships: A Complexity Case Study of Waminda’s Model of Systemic Decolonisation. Int. J. Environ. Res. Public Health 2020, 17, 7363. https://doi.org/10.3390/ijerph17207363
Cullen P, Mackean T, Worner F, Wellington C, Longbottom H, Coombes J, Bennett-Brook K, Clapham K, Ivers R, Hackett M, et al. Trauma and Violence Informed Care Through Decolonising Interagency Partnerships: A Complexity Case Study of Waminda’s Model of Systemic Decolonisation. International Journal of Environmental Research and Public Health. 2020; 17(20):7363. https://doi.org/10.3390/ijerph17207363
Chicago/Turabian StyleCullen, Patricia, Tamara Mackean, Faye Worner, Cleone Wellington, Hayley Longbottom, Julieann Coombes, Keziah Bennett-Brook, Kathleen Clapham, Rebecca Ivers, Maree Hackett, and et al. 2020. "Trauma and Violence Informed Care Through Decolonising Interagency Partnerships: A Complexity Case Study of Waminda’s Model of Systemic Decolonisation" International Journal of Environmental Research and Public Health 17, no. 20: 7363. https://doi.org/10.3390/ijerph17207363
APA StyleCullen, P., Mackean, T., Worner, F., Wellington, C., Longbottom, H., Coombes, J., Bennett-Brook, K., Clapham, K., Ivers, R., Hackett, M., & Longbottom, M. (2020). Trauma and Violence Informed Care Through Decolonising Interagency Partnerships: A Complexity Case Study of Waminda’s Model of Systemic Decolonisation. International Journal of Environmental Research and Public Health, 17(20), 7363. https://doi.org/10.3390/ijerph17207363