Well-Being without a Roof: Examining Well-Being among Unhoused Individuals Using Mixed Methods and Propensity Score Matching

 , , and
, , and 
Abstract
1. Introduction
2. Materials and Methods
3. Results
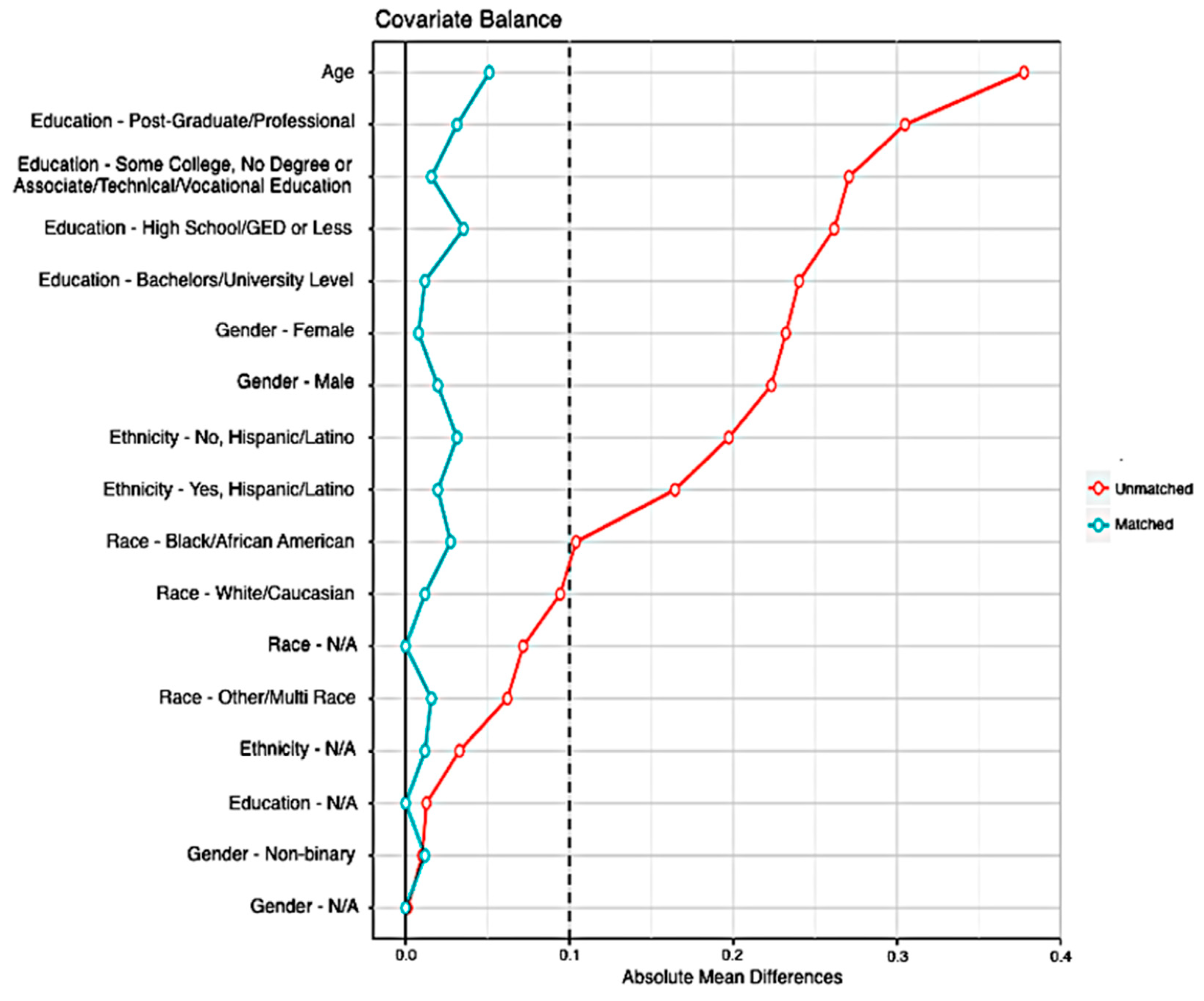
3.1. Demographics of the Matched Samples
3.2. Survey Results Comparing Well-Being Between the Unhoused and Housed
3.3. Qualitative Results
3.3.1. Reliance on Spirituality and Religiosity
3.3.2. Stress Experiences
“Well it’s so expensive to live here, there’s so much traffic. Unless you’re retired and have a bunch of money, costs you three thousand dollars to get a studio [apartment]. It’s ridiculous. You got to work your butt off to get by. There’s a lot of stress there. And your quality of life. You might be working fifteen hours a day to get there.”
3.3.3. Purpose and Meaning Experiences
“The first time that I came here, I sat on my butt for six months, didn’t try to work anything, didn’t try to get into a program. [This time] the second I got here, I told myself ‘I’m getting out of here.’ And I was going to do whatever it took to get the [explicit language] up out of here.”
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Henry, M.; Mahathey, A.; Morrill, T.; Robinson, A.; Shivji, A.; Watt, R. The 2018 Annual Homeless Assessment Report (AHAR) to Congress, Part 1: Point-in-Time Estimates of Homelessness. 2018. Available online: https://socialinnovation.usc.edu/homeless_research/he-2018-annual-homeless-assessment-report-ahar-to-congress-part-1-point-in-time-estimates-of-homelessness/ (accessed on 29 September 2020).
- Sullivan, B. Homelessness Declines in Most Communities of the U.S. With Increases Reported in High-Cost Areas 2017. Available online: https://www.hud.gov/press/press_releases_media_advisories/2017/HUDNo_17-109 (accessed on 8 August 2020).
- Henry, M.; Watt, R.; Rosenthal, L.; Shivji, A.; Associates, A. The 2017 Annual Homeless Assessment Report (AHAR) to Congress. 2017. Available online: https://www.abtassociates.com/insights/publications/report/the-2017-annual-homeless-assessment-report-to-congress-ahar-part-1 (accessed on 29 September 2020).
- Fazel, S.; Geddes, J.R.; Kushel, M. The health of homeless people in high-income countries: Descriptive epidemiology, health consequences, and clinical and policy recommendations. Lancet 2014, 384, 1529–1540. [Google Scholar] [CrossRef]
- National Coalition for the Homeless. Remembering Those Lost to Homelessness. 2018. Available online: https://nationalhomeless.org/category/mortality/ (accessed on 1 July 2020).
- National Center for Health Statistics. 2020. Available online: https://www.cdc.gov/nchs/fastats/life-expectancy.htm (accessed on 1 July 2020).
- Davies, A.; Wood, L.J. Homeless health care: Meeting the challenges of providing primary care. Med. J. Aust. 2018, 209, 230–234. [Google Scholar] [CrossRef] [PubMed]
- Hwang, S.W.; Burns, T. Health interventions for people who are homeless. Lancet 2014, 384, 1541–1547. [Google Scholar] [CrossRef]
- Maslow, A.H. Motivation and Personality; Harper & Row: New York, NY, USA, 1954; p. 395. [Google Scholar]
- Hobfoll, S.E. Conservation of Resources Theory: Its Implication for Stress, Health, and Resilience. In The Oxford Handbook of Stress, Health, and Coping; Oxford University Press: Oxford, UK, 2010; pp. 127–147. [Google Scholar]
- Diener, E.; Lucas, R.E.; Scollon, C.N. Beyond the hedonic treadmill: Revising the adaptation theory of well-being. Am. Psychol. 2006, 61, 305–314. [Google Scholar] [CrossRef]
- Ormel, J.; Lindenberg, S.M.; Steverink, N.; Verbrugge, L.M. Subjective well-being and social production functions. Soc. Indic. Res. 1999, 46, 61–90. [Google Scholar] [CrossRef]
- Biswas-Diener, R.; Diener, E. The Subjective Well-Being of the Homeless, and Lessons for Happiness. Soc. Indic. Res. 2006, 76, 185–205. [Google Scholar] [CrossRef]
- Rutenfrans, M.; Regenmortel, T.V.; Schalk, R. How to enhance social participation and well-being in (formerly) homeless clients: A structural equation modelling approach. Soc. Indic. Res. 2019, 145, 329–348. [Google Scholar] [CrossRef]
- Dunleavy, A.; Kennedy, L.A.; Vaandrager, L. Wellbeing for homeless people: A Salutogenic approach. Health Promot. Int. 2014, 29, 144–154. [Google Scholar] [CrossRef]
- Levasseur, M.; Richard, L.; Gauvin, L.; Raymond, É. Inventory and Analysis of Definitions of Social Participation Found in the Aging Literature: Proposed Taxonomy of Social Activities. Soc. Sci. Med. 2010, 71, 2141–2149. [Google Scholar] [CrossRef]
- Rutenfrans-Stupar, M.; Hanique, N.; Van Regenmortel, T.; Schalk, R. The Importance of Self-Mastery in Enhancing Quality of Life and Social Participation of Individuals Experiencing Homelessness: Results of a Mixed-Method Study. Soc. Indic. Res. 2020, 148, 491–515. [Google Scholar] [CrossRef]
- Stuart, E.A. Matching methods for causal inference: A review and a look forward. Stat. Sci. 2010, 25, 1–21. [Google Scholar] [CrossRef] [PubMed]
- Hansen, B.B.; Klopfer, S.O. Optimal Full Matching and Related Designs via Network Flows. J. Comput. Graph. Stat. 2006, 15, 609–627. [Google Scholar] [CrossRef]
- Hansen, B.B. Full Matching in an Observational Study of Coaching for the SAT. J. Am. Stat. Assoc. 2004, 99, 609–618. [Google Scholar] [CrossRef]
- Rosenbaum, P.R.; Rubin, D.B. The Central Role of the Propensity Score in Observational Studies for Causal Effects. Biometrika 1983, 70, 41–55. [Google Scholar] [CrossRef]
- Greifer, N. Cobalt: Covariate Balance Tables and Plots. R Pacakge Version 3.7.0. 2019. Available online: https://CRAN.R-project.org/package=cobalt (accessed on 29 September 2020).
- WELL for Life. WELL for Life. Available online: http://med.stanford.edu/wellforlife.html (accessed on 24 July 2020).
- Heaney, C.A.; Rich, T.; Avery, E.; Man, Y.; Chrisinger, B.W.; Ahuja, N.J. A qualitative exploration of well-being: What is well-being? How do we know? Why do we care? Unpublished work.
- R Core Team. R: A Language and Environment for Statistical Computing. 2016. Available online: https://www.r-project.org/ (accessed on 10 August 2018).
- Krueger, R.A.; Casey, M.A. Focus Groups: A Practical Guide for Applied Research; SAGE Publications: Thousand Oaks, CA, USA, 2014; p. 477. [Google Scholar]
- NVivo 12. NVivo Qualitative Data Analysis Software | QSR International Pty Ltd. Version 12. 2018. Available online: https://www.qsrinternational.com/nvivo/home (accessed on 7 January 2020).
- Thomas, D.R. A General Inductive Approach for Analyzing Qualitative Evaluation Data. Am. J. Eval. 2006, 27, 237–246. [Google Scholar] [CrossRef]
- Gabriel, I.; Ciudad-Real, V. State of Homelessness in California Fact Sheet. Homelessness Policy Research Institute. 2020, p. 2. Available online: https://socialinnovation.usc.edu/wp-content/uploads/2020/02/Homelessness-in-CA-Fact-Sheet-v3.pdf (accessed on 29 September 2020).
- HUD Exchange. 2019 AHAR: Part 1—PIT Estimates of Homelessness in the U.S. 2020. Available online: https://www.hudexchange.info/resource/5948/2019-ahar-part-1-pit-estimates-of-homelessness-in-the-us/ (accessed on 20 September 2020).
- Fajardo-Bullón, F.; Esnaola, I.; Anderson, I.; Benjaminsen, L. Homelessness and self-rated health: Evidence from a national survey of homeless people in Spain. BMC Public Health 2019, 19, 1081. [Google Scholar] [CrossRef] [PubMed]
- de Vet, R.; Beijersbergen, M.D.; Lako, D.A.M.; van Hemert, A.M.; Herman, D.B.; Wolf, J.R. Differences between homeless women and men before and after the transition from shelter to community living: A longitudinal analysis. Health Soc. Care Community 2019, 27, 1193–1203. [Google Scholar] [CrossRef]
- Jones, M.M. Does Race Matter in Addressing Homelessness? A Review of the Literature. World Med. Health Policy 2016, 8, 139–156. [Google Scholar] [CrossRef] [PubMed]
- van Dongen, S.I.; van Straaten, B.; Wolf, J.R.L.M.; Onwuteaka-Philipsen, B.D.; van der Heide, A.; Rietjens, J.A.C. Self-reported health, healthcare service use and health-related needs: A comparison of older and younger homeless people. Health Soc. Care Community 2019, 27, e379–e388. [Google Scholar] [CrossRef]
- Fazel, S.; Khosla, V.; Doll, H.; Geddes, J. The Prevalence of Mental Disorders among the Homeless in Western Countries: Systematic Review and Meta-Regression Analysis. PLoS Med. 2008, 5, e225. [Google Scholar] [CrossRef]
- Hossain, M.; Sultana, A.; Tasnim, S.; Fan, Q.; Ma, P.; McKyer, E.L.J.; Purohit, N. Prevalence of mental disorders among people who are homeless: An umbrella review. Int. J. Soc. Psychiatry 2020, 66, 528–541. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Constituent Domain of Well-Being | Definition | Example Items |
|---|---|---|
| Social Connectedness | Positive or negative relationships with others and how they influence your well-being | During the last two weeks, how often did you feel… |
| 1. … that you lacked companionship? | ||
| 2. … that there were people you could talk to? | ||
| 3. … that you were a part of a group of friends? | ||
| Lifestyle and Daily Practices | Lifestyle behaviors that can influence your well-being such as: diet; physical activity; sleep; the use of tobacco, alcohol, and marijuana; and other ways people take care of themselves | 1. During the past two weeks, how would you rate your sleep quality overall? |
| Stress and Resilience | Stress: Feelings of overload and an inability to balance or manage tasksResilience: Ability to adapt to change and bounce back after hardship | 1. During the last two weeks, how often have you felt that you were not able to give enough time to the important things in your life? |
| 2. How confident are you that you can bounce back quickly after hard times? | ||
| Experience of Emotions | How often you experience both pleasant and unpleasant emotions | During the last two weeks, how often did you feel… |
| 1. …calm? | ||
| 2. …drained? | ||
| Physical Health | Perception of your own health status, i.e., energy levels, ability to resist illness, physical fitness, and experience of pain. | 1. Compared to others of your own age, how would you rate your health? |
| 2. During the last two weeks, how often did your energy level allow you to do the things you WANT to do, as opposed to only the things you have to do? | ||
| Purpose and Meaning | Having a sense that aspects of your life provide purpose and meaning, i.e., goals, dreams, and being part of something larger than yourself. | How often does your daily life include experiences that give your life… |
| 1. … purpose? | ||
| 2. … meaning? | ||
| Sense of Self | The extent to which you feel you know yourself, can express your true self, have self-confidence, and feel good about who you are. | During the last two weeks, how often did you feel… |
| 1. … accepting of yourself? | ||
| 2. … that you were interested in your daily activities? | ||
| Finances | Your perception of having enough money to meet your needs. | 1. During the last year, how often have you had enough money to meet your needs? |
| Spirituality and Religiosity | The extent to which spiritual and religious beliefs, practices, communities, and traditions are important in your life. | 1. How important are spiritual or religious beliefs in your day to day life? |
| Exploration and Creativity | Having opportunities to grow as a person and to explore new experiences and ways of thinking. | 1. How often do you engage with opportunities to challenge yourself and grow as a person? |
| Housed (N = 255) | Unhoused (N = 51) | ||||
|---|---|---|---|---|---|
| Variable | N | % | N | % | |
| Age (Mean SD) | 46.00 (19.0) | 46.82 (13.0) | |||
| Gender | Female | 127 | 49.8 | 25 | 49.0 |
| Male | 120 | 47.1 | 25 | 49.0 | |
| Non-Binary | 8 | 3.1 | 1 | 2.0 | |
| Education | High School/GED or less | 71 | 27.8 | 16 | 31.4 |
| Associate, Some College, No Degree | 114 | 44.7 | 22 | 43.1 | |
| Bachelors/University Level | 32 | 12.5 | 7 | 13.7 | |
| Post-Graduate/Professional | 33 | 12.9 | 5 | 9.8 | |
| Missing | 5 | 2.0 | 1 | 2.0 | |
| Race | White/Caucasian | 117 | 45.9 | 24 | 47.1 |
| Black/African American | 42 | 16.5 | 7 | 13.7 | |
| Other/Multi Race | 36 | 14.1 | 8 | 15.7 | |
| Missing | 60 | 23.5 | 12 | 23.5 | |
| Ethnicity | Hispanic | 65 | 25.5 | 14 | 27.5 |
| Not Hispanic | 183 | 71.8 | 35 | 68.6 | |
| Missing | 7 | 2.7 | 2 | 3.9 | |
| Domain | Regression Coefficient (SD) 1 |
|---|---|
| Overall Well-being | −5.022 * (1.989) |
| Social Connectedness | −1.086 *** (0.251) |
| Lifestyle and Daily Practices | −1.219 *** (0.188) |
| Diet | −1.169 *** (0.239) |
| Physical Activity | −0.662 (0.452) |
| Sleep | −1.292 *** (0.295) |
| Stress and Resilience | −0.493 * (0.214) |
| Stress | −0.293 (0.260) |
| Resilience | −0.692 ** (0.238) |
| Experience of Emotions | −0.632 ** (0.240) |
| Positive Emotions | −0.521 (0.268) |
| Negative Emotions | −0.742 ** (0.263) |
| Sense of Self | −0.395 (0.290) |
| Purpose and Meaning | 0.149 (0.323) |
| Physical Health | −0.944 *** (0.238) |
| Finances | −3.099 *** (0.457) |
| Spirituality and Religiosity | 2.401 *** (0.507) |
| Exploration and Creativity | 0.038 (0.341) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ahuja, N.J.; Nguyen, A.; Winter, S.J.; Freeman, M.; Shi, R.; Rodriguez Espinosa, P.; Heaney, C.A. Well-Being without a Roof: Examining Well-Being among Unhoused Individuals Using Mixed Methods and Propensity Score Matching. Int. J. Environ. Res. Public Health 2020, 17, 7228. https://doi.org/10.3390/ijerph17197228
Ahuja NJ, Nguyen A, Winter SJ, Freeman M, Shi R, Rodriguez Espinosa P, Heaney CA. Well-Being without a Roof: Examining Well-Being among Unhoused Individuals Using Mixed Methods and Propensity Score Matching. International Journal of Environmental Research and Public Health. 2020; 17(19):7228. https://doi.org/10.3390/ijerph17197228
Chicago/Turabian StyleAhuja, Naina J, Allison Nguyen, Sandra J Winter, Mark Freeman, Robert Shi, Patricia Rodriguez Espinosa, and Catherine A Heaney. 2020. "Well-Being without a Roof: Examining Well-Being among Unhoused Individuals Using Mixed Methods and Propensity Score Matching" International Journal of Environmental Research and Public Health 17, no. 19: 7228. https://doi.org/10.3390/ijerph17197228
APA StyleAhuja, N. J., Nguyen, A., Winter, S. J., Freeman, M., Shi, R., Rodriguez Espinosa, P., & Heaney, C. A. (2020). Well-Being without a Roof: Examining Well-Being among Unhoused Individuals Using Mixed Methods and Propensity Score Matching. International Journal of Environmental Research and Public Health, 17(19), 7228. https://doi.org/10.3390/ijerph17197228